
Abstract
Background
Avoidance of colonoscopy is often associated with fear, embarrassment, and disgust aroused in screening procedures. However, each emotion can be linked to different challenges faced by patients. More research is needed to evaluate and address the causes of these respective emotions.
Aim
The purpose of this study was to develop and assess the scales of three negative emotions (i.e., fear, embarrassment, and disgust) caused by specific issues in colonoscopy screening.
Method
The measurement items were developed based on multiple common barriers in colonoscopy screening procedures. An online sample of 232 adults aged 45-75 was recruited from Amazon Mechanical Turk to test the scales. Explorative and confirmatory factor analyses were conducted to validate the measurement models.
Results
Psychometric evidence demonstrated the factor structures of three negative emotions. Each emotional factor was caused by unique combinations of barriers in the preparation, screening, and recovery stages of colonoscopy. Most of the emotional factors were associated with attitudes and screening intention.
Conclusion
This study showed different dimensions of negative emotions and their underlying causes in colonoscopy. These findings will help assess specific causes of negative emotions in colonoscopy and develop effective interventions to improve screening uptake.
Colorectal cancer (CRC) is the second leading cause of cancer-related deaths in the United States that affect both men and women (Siegel et al., 2021). Evidence indicates that CRC preventive screenings can significantly reduce incidence and mortality (U.S. Preventive Services Task Force et al., 2016). Compared with other screening modalities, colonoscopy is the most commonly used and efficacious one because it does not need supplemental tests to validate the screening results (Rees et al., 2016; Shapiro et al., 2012).
However, adherence to CRC screening recommendations remains low (Cyhaniuk & Coombes, 2016). Identifying and addressing the barriers to colonoscopy can improve screening rates and decrease mortality (Basch et al., 2016). Recent attention has been paid to the unique role of emotions in colonoscopy avoidance (Reynolds et al., 2013). Negative emotions, including fear, embarrassment, and disgust, can be simultaneously evoked by multiple issues throughout the colonoscopy procedures, such as handling stool or exposing private body parts (Bynum et al., 2012; Klasko-Foster et al., 2020). Assessing various causes of each negative emotion that are associated with different issues in the screening procedures can better predict screening behaviors and develop more effective interventions (Reynolds et al., 2018).
Fear
Fear evolves from the evolutionary need to protect oneself from threats of safety, wellness (Lazarus, 1991; Öhman, 2008). In the context of CRC, fear can be elicited by various issues that may threaten an individual’s health and self-esteem (McLachlan et al., 2012; Vrinten et al., 2017). For example, fear may be aroused by a potential cancer diagnosis resulting from colonoscopy (Hay et al., 2005). Patients can also experience fear of the adverse side effects or the violation of a person’s privacy during colonoscopy (McLachlan et al., 2012; Winterich et al., 2009).
The causes of fear are associated with different aspects of colonoscopy, bringing uncertainty to predicting how fear influences screening behaviors. Past research suggests that fear arising from different barriers can act as either a catalyst or a deterrent to colonoscopy uptake (Vrinten et al., 2015). For example, people fearing cancer could accept colonoscopy screenings to rule out the possibility of cancer. Fear of side effects, however, may trigger screening avoidance (Vrinten et al., 2015). Thus, it is important to assess the factors in colonoscopy as different causes of fear.
Embarrassment
Embarrassment is characterized as feelings of awkwardness and foolishness (Miller, 1996; Tangney et al., 1996). Embarrassment stems from a social need to prevent being ostracized by a community for violation of shared social standards (Keltner & Anderson, 2000). People often feel embarrassed in different medical examination situations, such as losing control of themselves or presentations of physical incompetence (Consedine et al., 2007; Miller, 1996). Embarrassment can also arise from one’s behaviors or appearances that are not consistent with personal expectations (Mitchell et al., 2012).
The role of embarrassment in colonoscopy is not sufficiently understood. First, colonoscopy-related embarrassment has been examined using single-term scales (Codori et al., 2001; Harewood et al., 2002), which is not adequate to measure this multidimensional construct. Qualitative findings suggest that potential triggers of embarrassment occur at multiple points in the screening process, including difficulties of privacy regulation, and loss of modesty (Oh et al., 2021; Von Wagner et al., 2009). Second, distinct elicitors of embarrassment may suggest different screening behaviors. Embarrassment could cause avoidance and also increase engagement in colonoscopy (Consedine et al., 2007; Consedine, Reddig, et al., 2011).
Consedine, Ladwig, et al. (2011) identified feces and rectal examination as well as provider-patient intimacy as two factors of colonoscopy-related embarrassment but overlooked some other elicitors (Mitchell et al., 2012). Thus, more inquiries are needed to assess different causes of embarrassment in the context of colonoscopy.
Disgust
Disgust is an emotional response to contamination and degradation (Haidt et al., 1997; Rozin et al., 1999). As an adaptive mechanism, disgust safeguards individuals from pathogens and microbial pollutants that can bring harmful consequences to health (Curtis et al., 2011). Disgust can also be triggered by a breach of social and moral codes set up to delineate humans from animals (e.g., deviant sexual acts) (Berle & Phillips, 2006; Haidt et al., 1997). Disgust results in withdrawal and avoidant responses that distance oneself from offensive stimuli (Berle & Phillips, 2006; Curtis et al., 2011).
Colonoscopy presents many elements of disgust. First, handling body products was commonly reported by patients as a main reason for disgust (Chapple et al., 2008; Reynolds et al., 2013). Second, disgust is elicited by invasive procedures, including surgical access to internal organs that break into the integrity of one’s body (Klasko-Foster et al., 2020). Third, colonoscopy exposes patients to symptoms and diagnoses of cancer that signals mortality (Reynolds et al., 2013). Disgust is a natural reaction of patients that helps distance themselves from the reminders of death (Haidt et al., 1997).
Several elicitors of disgust related to colonoscopy have been identified in qualitative studies and have yet to be quantified (Reynolds et al., 2013). While these studies have recognized that core disgust resulted from prototypical elicitors, such as body waste, disgust associated with other elicitors is not fully understood (Klasko-Foster et al., 2020; Reynolds et al., 2013). As a result, suitable measurement tools for different disgust elicitors are not available (Reynolds et al., 2013), limiting the understanding of the effects on screening uptake.
The Present Study
Colonoscopy presents critical challenges that could elicit fear, embarrassment, and disgust, leading to screening avoidance. However, past research often focused on a single issue in colonoscopy as the cause of a negative emotion (e.g., feces as an elicitor of disgust) (McLachlan et al., 2012; Reynolds et al., 2018). The literature reveals three important problems. First, there is not a one-to-one relationship between an emotion and a causal factor in colonoscopy. Throughout screening procedures, one issue can arouse several discrete emotions. Also, each emotion can be caused by many different issues (Reynolds et al., 2018). Thus, a patient’s exact feelings and underlying causes cannot be clearly determined without examining their responses to various related issues in screening. Second, each emotion could influence screening behaviors differently, depending on eliciting reasons (Consedine, Ladwig, et al., 2011; Reynolds et al., 2018). For example, disgust of death could motivate screening, but disgust of body waste could increase avoidance (Reynolds et al., 2013). Third, the lack of valid measurement tools further impedes the theoretical understanding of emotions in colonoscopy (Klasko-Foster et al., 2020; Reynolds et al., 2013).
Therefore, we propose the measurement of an individual’s simultaneous responses to a set of issues in colonoscopy as a way to evaluate the shared, underlying reasons for a discrete emotion. In other words, responses to another set of issues indicate a different cause of the same emotion. Accordingly, the present study will develop and assess the measurement models that can systematically account for different causes of fear, embarrassment, and disgust associated with a variety of issues in colonoscopy. Using psychometric analyses, the study answers the following Research Question (RQ): What are the respective causes of (a) fear, (b) embarrassment, and (c) disgust related to colonoscopy screening?
Method
Measures
The measurement instruments for three negative emotions (i.e., fear, embarrassment, disgust) were developed in two steps. First, two co-authors conducted a systematic literature search for publications on PubMed and Google Scholar that were published after 2010 using (a) emotion-related search terms (“emotion*” or “fear” or “embarrass*” or “disgust”) and (b) colonoscopy-related terms (“colonoscopy” OR “colorectal cancer screening”). Then, we reviewed each publication from the search results and recorded unique issues or elements of colonoscopy that had been found as causes of emotions. The results, coded by two co-authors, were cross-checked and synthesized to ensure all causes were recorded. The process concluded when no new causes of emotions emerged from further sampling (Saunders et al., 2018). In total, we identified 19 issues throughout colonoscopy procedures as potential causes of three emotions (e.g., Basch et al., 2016; McLachlan et al., 2012; Mitchell et al., 2012). Five were related to pre-screening preparation, nine related to peri-screening procedures, and five related to post-screening recovery.
Second, we developed each measurement item by breaking it into three phrases. Part 1 of an item mentioned the stage of colonoscopy screening (i.e., before/during/after a colonoscopy screening). Part 2 included a stem statement about an emotional feeling (i.e., I would feel fearful/embarrassed/disgusted) plus a preposition word (. . . of/by). Part 3 indicated one of the 19 barriers. For example, “During a colonoscopy exam, I would feel embarrassed by passing gas” was an item for embarrassment.
We developed a total of three models, each of which included 19 items for one emotion (see Tables 2–5). Each item was rated from “very unlikely” (coded as 1) to “very likely” (5). The items for a colonoscopy stage (i.e., pre-, peri-, post-screening) of each emotion were randomized to reduce fatigue and potential order effects.
In addition, this study measured attitudes and screening intention as index outcomes. Attitudes were measured by a 5-point semantic-differential scale (Dillard et al., 2007), which used the phrase stem “I think colonoscopy is . . .” followed by six adjective pairs: good/bad, favorable/unfavorable, positive/negative, desirable/undesirable, necessary/unnecessary, and beneficial/detrimental. Screening intention was measured by a four-item scale (Peng et al., 2022). The items assessed how much participants intended to get a colonoscopy, talk to their doctor, look for information online, and talk to their family about colonoscopy.
Participants and Procedure
The Institutional Review Board reviewed the study protocol and provided exemption certification before data collection. Informed consent was obtained from all participants in the final sample. Participants were recruited from Amazon Mechanical Turk (MTurk). This crowdsourcing platform allowed us to recruit a large, diverse sample of participants without a significant cost during COVID-19 when conventional methods of data collection were less feasible (Hlatshwako et al., 2021). The data quality of MTurk has been better than alternative online sampling services (Buhrmester et al., 2011; Kees et al., 2017; Moss et al., 2020).
We recruited a total of 247 U.S. residents aged between 45 and 75 years. The selection criteria were determined by the U.S. Preventive Services Task Force’s (2016) colorectal cancer screening recommendations. Participants completed a brief questionnaire in exchange for 50 cents (USD) as an incentive. After providing informed consent and then completing demographic questions, all participants read a general introduction about colonoscopy from National Institute of Diabetes and Digestive and Kidney Diseases (2017). Afterward, all participants completed the measures listed above.
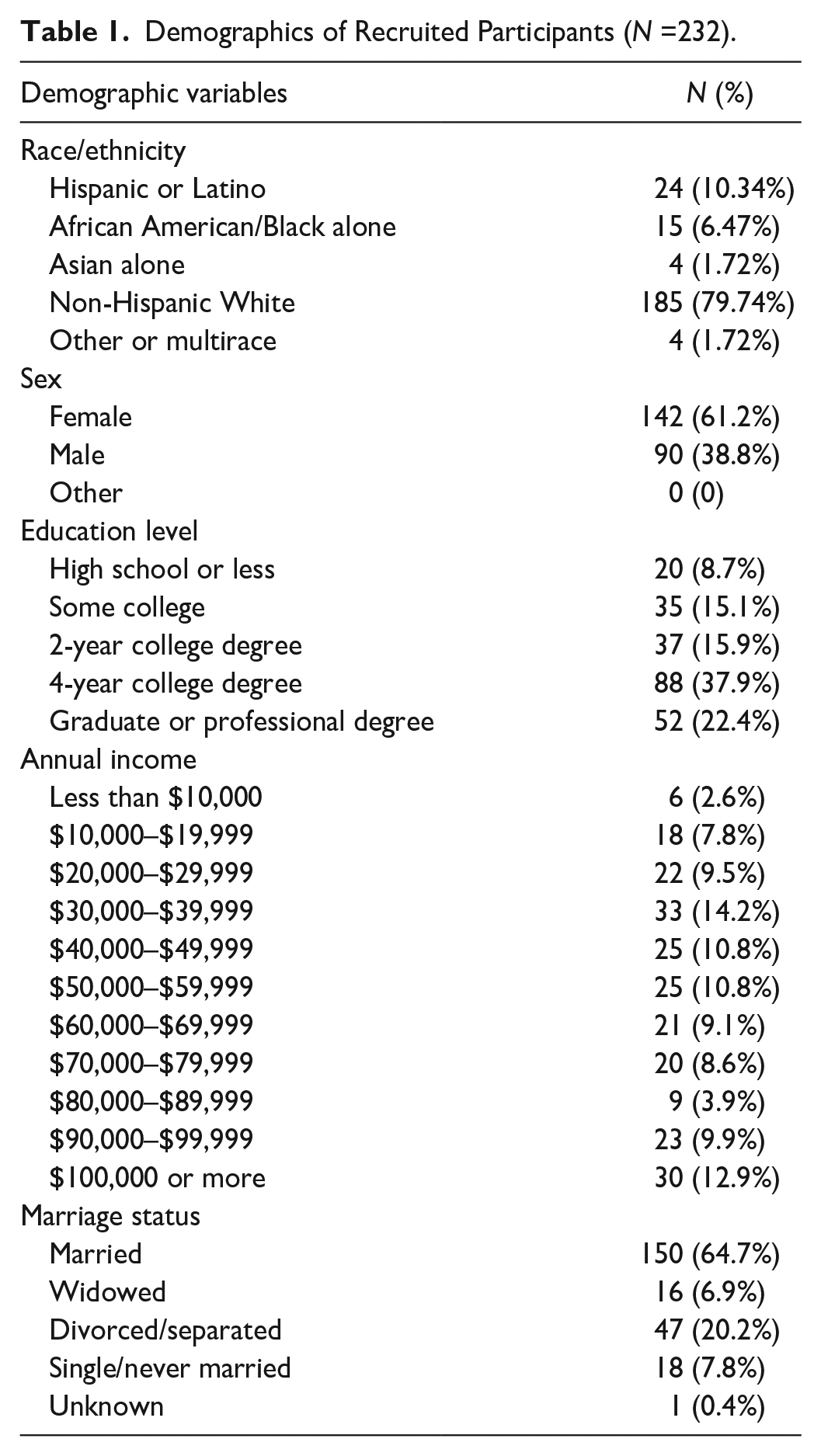
We used the rIP R package (Waggoner et al., 2019) through ProxyCheck IP verification services to detect bot or fraudulent data. The detection process led to the removal of 15 suspicious cases, yielding a final sample (N) size of 232. The average age was 61.89 (SD = 7.22; see other demographic details in Table 1).
Demographics of Recruited Participants (N =232).
Analysis
Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted to assess the factor structure of the measurement items for each emotion. The total sample was randomly split into two subsets, one for EFA (n = 116) and one for CFA (n = 116). For each subset, we computed the Mahalanobis Distance (M-D) of 19 observed variables for each emotion to flag multivariate normality outliers. As suggested by Tabachnick and Fidell (2007), we removed 10 outliers from the EFA subset and eight from the CFA subset that had a probability less than .001 on a chi-square distribution (df = 19) of M-D values of any one of three emotions. The final sample sizes of EFA and CFA subsets were 106 and 108, respectively. Critical indicators for validity assessment were computed based on CFA.
Results
EFA
EFAs used principal axis factoring to identify the factor structure of 19 items for each emotion. Considering possible correlations between emotion factors (Reynolds et al., 2018), direct oblimin rotation was used. The results of EFAs for all three emotions rejected the null hypothesis of Barlett’s test of sphericity (ps < .001). The Kaiser–Meyer–Olkin (KMO) measures of sampling adequacy of three EFAs were sufficient (KMOs > .90).
Factors
Fear
EFA returned a two-factor solution for fear. The first factor included various items related to preparation and screening procedures (Table 2). Most items clustered on the first factor had very high loadings above or close to .80. However, two items, “inserting diagnostic equipment . . .” and “removing body tissue . . .,” had relatively lower loadings (around .60 or below). The effects of these two procedures were less consistent because they occur after patients are sedated—as sedation reduces fear and pain (National Cancer Institute, 2021). Thus, these two items were dropped from the first factor. The second factor included the items concerning adverse outcomes in post-screening recoveries, such as puncture and bleeding. According to a systematic review (McLachlan et al., 2012), colonoscopy procedures and potential post-procedure complications are common causes of fear. Thus, two factors were labeled as “fear of colonoscopy procedures” and “fear of medical complications.”
Summary of Exploratory Factor Analysis (EFA; n = 106) and Confirmatory Factor Analysis (CFA; n = 108) of Items for Fear of Colonoscopy.
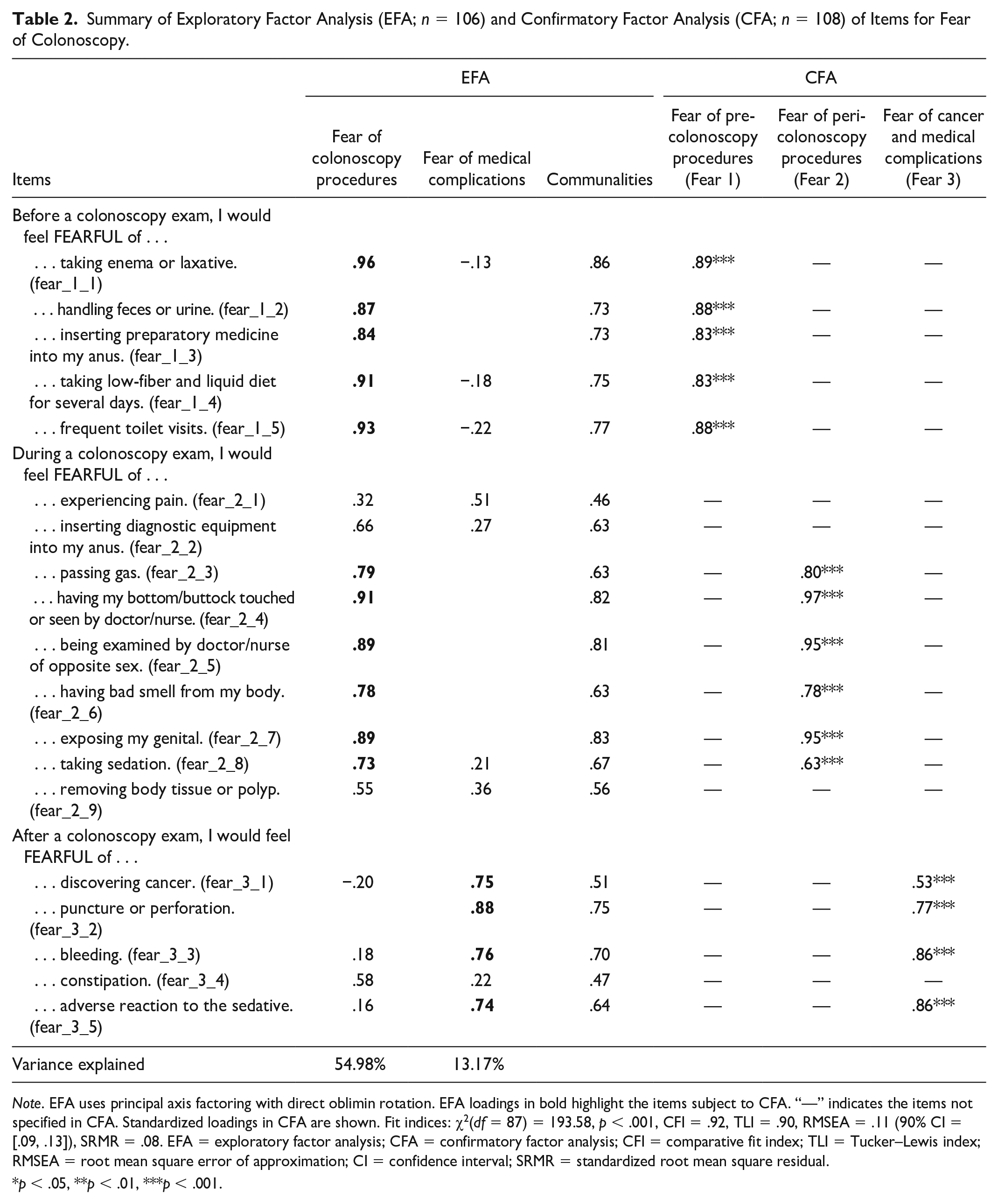
Note. EFA uses principal axis factoring with direct oblimin rotation. EFA loadings in bold highlight the items subject to CFA. “—” indicates the items not specified in CFA. Standardized loadings in CFA are shown. Fit indices: χ2(df = 87) = 193.58, p < .001, CFI = .92, TLI = .90, RMSEA = .11 (90% CI = [.09, .13]), SRMR = .08. EFA = exploratory factor analysis; CFA = confirmatory factor analysis; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual.
p < .05, **p < .01, ***p < .001.
Embarrassment
EFA returned three factors of embarrassment (Table 3). Three items for peri-screening and all five items for post-screening loaded onto the first factor at a level of .60 or higher. These items were associated with negative impacts of colonoscopy that decreased individuals’ control of their bodies. Based on Miller’s (1996) classification of embarrassment, we labeled the first factor as “embarrassment of losing bodily control.”
Summary of Exploratory Factor Analysis (EFA; n = 108) and Confirmatory Factor Analysis (CFA; n = 108) of Items for Embarrassment of Colonoscopy.
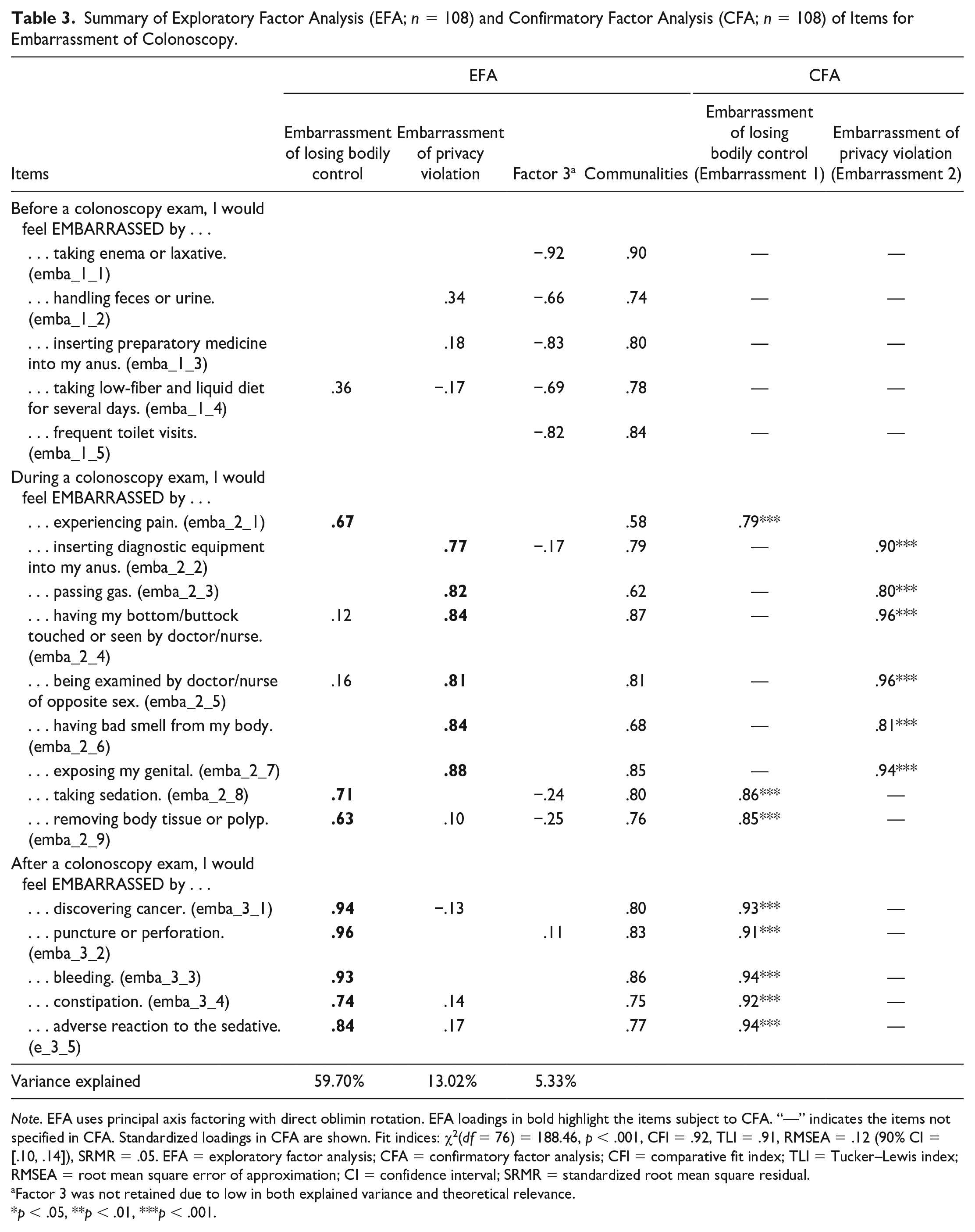
Note. EFA uses principal axis factoring with direct oblimin rotation. EFA loadings in bold highlight the items subject to CFA. “—” indicates the items not specified in CFA. Standardized loadings in CFA are shown. Fit indices: χ2(df = 76) = 188.46, p < .001, CFI = .92, TLI = .91, RMSEA = .12 (90% CI = [.10, .14]), SRMR = .05. EFA = exploratory factor analysis; CFA = confirmatory factor analysis; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual.
Factor 3 was not retained due to low in both explained variance and theoretical relevance.
p < .05, **p < .01, ***p < .001.
Another six items for peri-colonoscopy procedures clustered on the second factor at the level of .70 or higher. The second factor was specific to the privacy issues of colonoscopy procedures in hospital settings. In contrast, the aspect of colonoscopy related to at-home preparation did not respond to this factor. Evidently, this embarrassment component reflected the difficulty in regulating one’s privacy which causes awkward interactions (Consedine, Ladwig, et al., 2011). Thus, the second component was labeled as “embarrassment of privacy violation.”
Five items for pre-colonoscopy had negative loadings on the third factor. Because the third factor explained only 5.33% of the variance and negative loadings were not theoretically relevant, we did not retain this third factor.
Disgust
A three-factor solution for disgust emerged from EFA (Table 4). The first factor included items related to physical symptoms and discomfort in both peri- and post-colonoscopy parts. Notably, two items clustered on the first factor with below .60 loadings. Because disgust can be elicited by reminders of death, such as signs of mortality, diseases, and medical complications (Curtis & Biran, 2001; Rozin & Fallon, 1987), we kept the item “removing body tissue or polyp” as an important indicator of cancer but dropped the one about “taking sedation.” The first factor was hence named “disgust of cancer and death.”
Summary of Exploratory Factor Analysis (EFA; n = 108) and Confirmatory Factor Analysis (CFA; n = 108) of Items for Disgust of Colonoscopy.
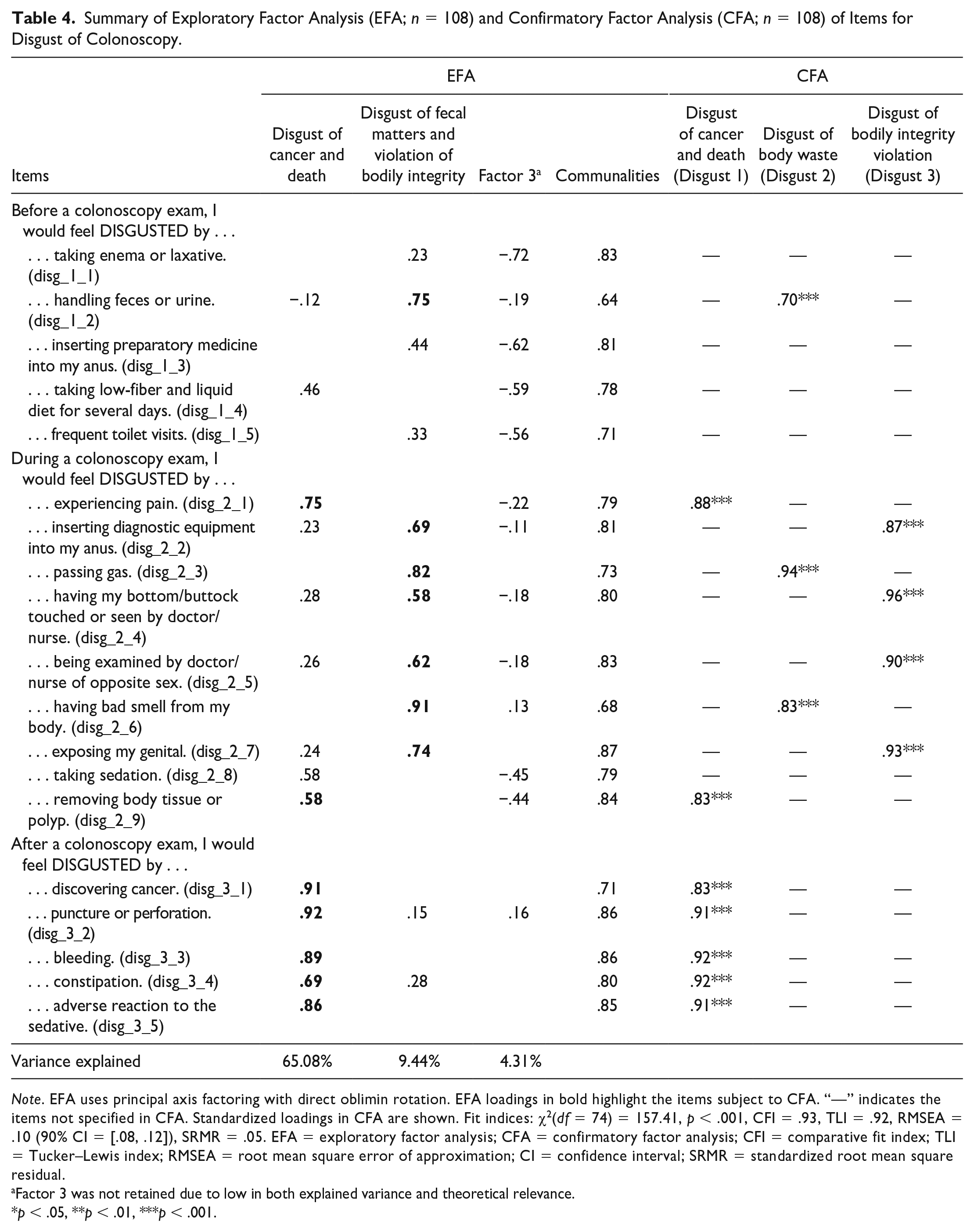
Note. EFA uses principal axis factoring with direct oblimin rotation. EFA loadings in bold highlight the items subject to CFA. “—” indicates the items not specified in CFA. Standardized loadings in CFA are shown. Fit indices: χ2(df = 74) = 157.41, p < .001, CFI = .93, TLI = .92, RMSEA = .10 (90% CI = [.08, .12]), SRMR = .05. EFA = exploratory factor analysis; CFA = confirmatory factor analysis; CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean square residual.
Factor 3 was not retained due to low in both explained variance and theoretical relevance.
p < .05, **p < .01, ***p < .001.
The second factor included three items related to both handling body waste and another four concerning violations of the body envelope. Thus, the second factor was labeled “disgust of body waste and violated bodily integrity.”
The third factor, which was negatively loaded by items throughout colonoscopy procedures, indicated no clear theoretical implications. Thus, this factor was not further assessed.
CFA
The measurement items for each affective experience were subject to CFAs. A total of three CFA models were specified, one for each emotion (see supplemental material for model specification). The Maximum Likelihood with Robust Standard Errors estimator in Mplus was used because of its robustness to potential non-normality of data (Kline, 2015; Muthén & Muthén, 2017; Zhong & Yuan, 2011). Also, previous literature has widely documented (Chen et al., 2008; Kenny et al., 2015; Taasoobshirazi & Wang, 2016) that root mean square error of approximation (RMSEA) could be inflated due to a small sample size, which may wrongfully reject a valid model. Given the small sample size of the CFA dataset, we allowed a slightly higher threshold of RMSEA (<.13) than Hu and Bentler’s (1999) suggestion to determine the goodness of fit.
Fear
The two-factor model from EFA did not fit the data sufficiently, χ2(df = 89) = 327.78, p < .001, comparative fit index (CFI) = .81, Tucker–Lewis index (TLI) = .78, root mean square error of approximation (RMSEA) = .16 (90% confidence interval [CI] = [.14, .18]), standardized root mean square residual (SRMR) = .09. A close examination shows that the first factor, “fear of colonoscopy procedure,” consisted of items related to both pre- and peri-colonoscopy procedures, which were respectively conducted at home in private and in a clinical setting with providers. We re-specified the model by loading the items for pre- and peri-screening on separate factors. The re-specified three-factor model showed a reasonable fit (see Table 2 and supplemental material).
Embarrassment
CFA supported the two-factor model identified in EFA, which fit data sufficiently (Table 3 and supplemental material).
Disgust
The original two-factor solution showed suboptimal fit, χ2(df = 76) = 205.32, p < .001, CFI = .90, TLI = .88, RMSEA = .13 (90% CI = [.11, .15]), SRMR = .05. Because handling body waste and violation of body envelope were two distinct causes of disgust (Klasko-Foster et al., 2020; Reynolds et al., 2013), we decided to load the items for these two causes on separate factors. The re-specified three-factor CFA model fitted the data sufficiently (Table 4 and supplemental material).
Convergent Validity
The convergent validity of each scale was assessed and satisfied based on four indicators (Almén et al., 2018; Fornell & Larcker, 1981; Hair et al., 2005). First, the standardized loadings of all items in four CFA models (Tables 2–4) exceed the minimum value of 0.50 set by Hair et al. (2005). Second, the composite reliability (CR) value of a factor was greater than 0.70 and its corresponding average variance extracted (AVE) (Table 5). Third, the AVEs of all factors were greater than 0.50, suggesting higher variance explained by each factor in relation to the variance due to measurement errors (dos Santos & Cirillo, 2021). Fourth, Cronbach’s alpha values of all factors exceeded .80.
Descriptive Statistics, Correlation, and Validity Results of Confirmatory Factor Analyses (N = 108).
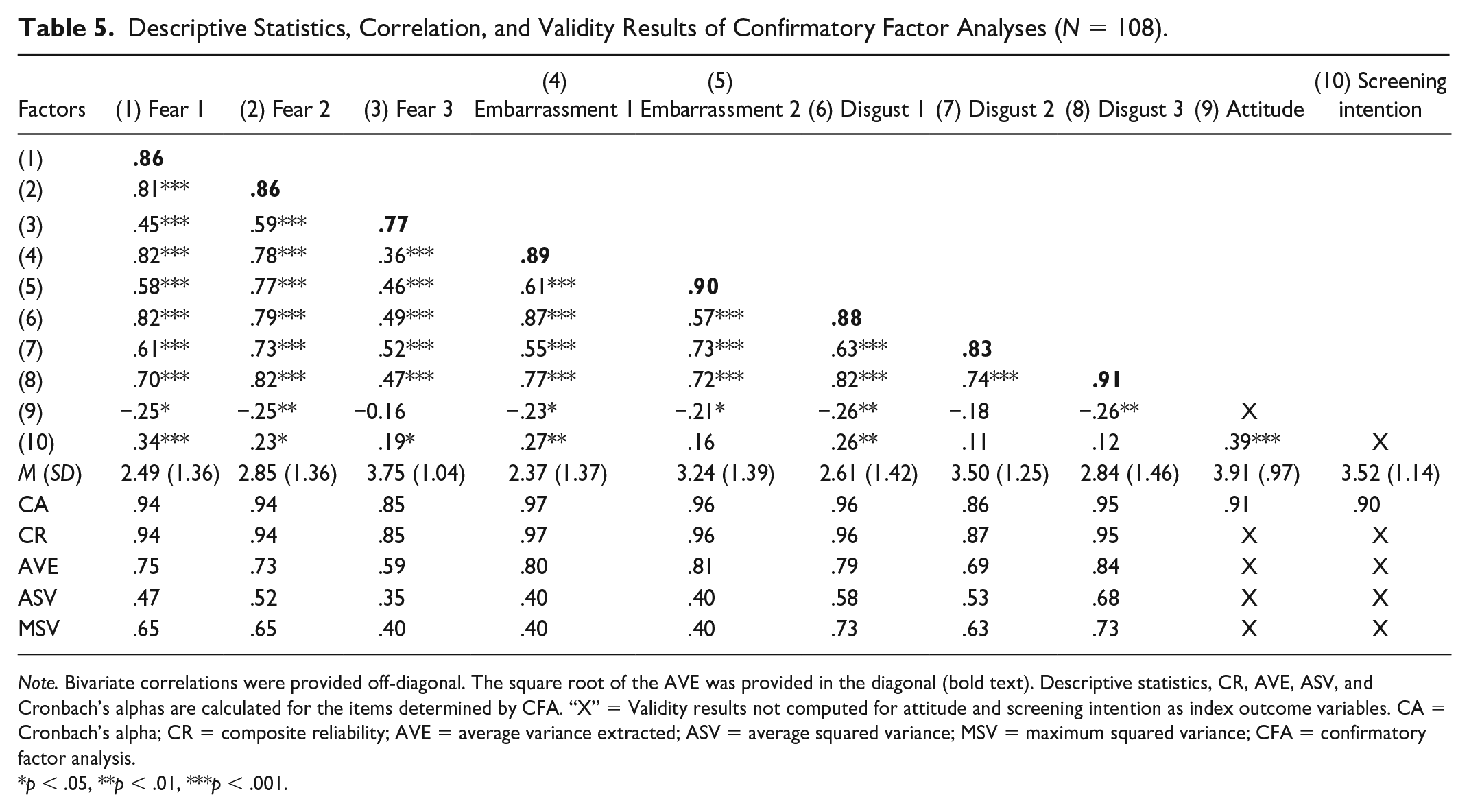
Note. Bivariate correlations were provided off-diagonal. The square root of the AVE was provided in the diagonal (bold text). Descriptive statistics, CR, AVE, ASV, and Cronbach’s alphas are calculated for the items determined by CFA. “X” = Validity results not computed for attitude and screening intention as index outcome variables. CA = Cronbach’s alpha; CR = composite reliability; AVE = average variance extracted; ASV = average squared variance; MSV = maximum squared variance; CFA = confirmatory factor analysis.
p < .05, **p < .01, ***p < .001.
Discriminant Validity
Discriminant validity was established based on Fornell and Larcker’s (1981) criterion (see also Hair et al., 2005). We found that the AVE of each factor was greater than its corresponding average shared squared variance (ASV) and maximum squared variance (MSV). Alternatively, the square root of each factor’s AVE was higher than its correlation with another construct. All factors met the criterion (Table 5).
Predictive Validity
Predictive validity was assessed by correlational analyses between the mean of emotional factors and either attitude or screening intention as an index outcome. The mean values of emotion factors were computed based on the indicator items confirmed by factor analyses. Table 5 shows that most of the emotional factors were either negatively correlated with attitudes or positively correlated with screening intention. The only exception was disgust of body waste, which was marginally correlated with attitudes and not significantly with screening intention. The results not only supported the predictive validity of the measures for most emotional factors but also suggested the possibility of different index measures in future research.
Discussion
The present study developed and assessed the measurement models for fear, embarrassment, and disgust linked to colonoscopy. The psychometric analysis identified multiple causes of each emotion associated with different elicitors throughout the screening process. Each cause indicated a salient psychological and practical barrier, bringing different impacts to colonoscopy screening (Consedine & Moskowitz, 2007). Given the lack of valid instrumentation for emotions in colonoscopy (Klasko-Foster et al., 2020; Reynolds et al., 2013), the present study provides a useful tool to clarify different possible roles of each emotion in colonoscopy screening and informs future interventions to improve colonoscopy uptake.
We identified three factors of fear specific to colonoscopy screening and their influences at different stages of the decision-making process. The first two factors for fear centered on the preparation and test procedures at home and in the hospital, respectively. In line with earlier studies (Basch et al., 2016; McLachlan et al., 2012), we found preparation and test procedures emerged as the two primary causes of fear that negatively lowered screening attitudes. Thus, the priority of health education should be on helping patients cope with fear before and during screening. Patients experiencing fear associated with at-home bowel preparation need support to improve the practical skills that reduce discomfort and inconvenience (McLachlan et al., 2012). To control the fear of clinical procedures, information to address challenges associated with common barriers, such as pain and privacy, should be provided in hospitals (McLachlan et al., 2012).
Responding to cancer and medical complications, the third factor increased screening intention but did not lower attitude toward screening. This result might be explained by previous findings (Basch et al., 2016; Vrinten et al., 2015) that people who feared cancerous consequences accepted screening recommendations in attempts to seek assurance. Nonetheless, such fear might not easily subside even with a consultation with health care providers. Thus, this factor also highlights the role of providers in educating patients about the medical benefits and low risks of colonoscopy in early decision-making (Basch et al., 2016; Reumkens et al., 2016).
Second, while privacy challenges have been frequently cited in previous studies as a common reason for embarrassment (Consedine, Ladwig, et al., 2011; Wang et al., 2019), our study showed that losing bodily control could be a more important cause of embarrassment. This finding suggests that compared with privacy issues, people were more concerned about negative social judgment if they became physically sick and feeble after colonoscopy screening (Keltner & Buswell, 1997; McLachlan et al., 2012). This is further evidenced by correlational results. Although both factors of embarrassment were linked to negative attitudes, embarrassment of losing bodily control further motivated individuals to undergo screening so they could detect cancer earlier and avoid embarrassing illness or symptoms (Consedine et al., 2007).
Therefore, to tackle the embarrassment of losing bodily control, information about the safety, comfort, and benefit of colonoscopy is potentially helpful (McLachlan et al., 2012). Increasing self-efficacy (Friedman et al., 2014) and delivering messages about treatment effectiveness could also reduce concerns about social judgment. For non-adherents due to privacy violations, health care providers can proactively discuss the issues involving private matters to destigmatize colonoscopy procedures (Consedine, Ladwig, et al., 2011).
Third, drawing on and expanding extant literature (Klasko-Foster et al., 2020; Reynolds et al., 2013), the present study provided critical instrumentation to assess multiple dimensions of disgust. Three causes of disgust—cancer and death, body waste, and violated bodily integrity—suggest different psychological reasons and behavioral impacts on colonoscopy. As a more pronounced factor in our model, disgust of cancer and death indicated strong distress and denial of mortality (Rozin, 2008). Disgust could increase negative attitudes as people distanced themselves from physical reminders of death, such as blood or pain in colonoscopy (Reynolds et al., 2013; Rozin, 2008). However, this type of disgust could also promote screening behaviors to eliminate the possibility of cancer (Reynolds et al., 2013), as evidenced by a positive correlation with intention.
We also identified two other elicitors of core disgust, including body products and body envelope violations, in line with qualitative findings (Wangmar et al., 2021). Core disgust is considered an instinctual reaction, leading to avoidance (Rozin, 2008). However, both disgust elicitors were not related to screening intentions. This was probably because personal trait differences in disgust sensitivity might influence the intensity of disgust and its effects on screening (Klasko-Foster et al., 2020; Scaglioni et al., 2021). Some researchers advocated for targeted exposure therapy to weaken core disgust (Klasko-Foster et al., 2020; Reynolds et al., 2013), but more studies are needed to confirm the effects.
We point out two limitations of the study. First, the study recruited an online sample with an overrepresentation of White, females, and those with high educational attainment. Retesting the measurement scales with a representative sample and in health care settings can further improve the validity. Second, most of the emotional factors were positively associated with screening intention. We argued that negative emotions could still cause avoidance, which was suggested by their negative association with attitude. Also, positive correlations between screening intention and several negative emotions might suggest some individuals’ interest in following up with their providers or online sources. Other factors, such as perceived benefits or normative beliefs (Ajzen, 1985), could also influence their screening intention. Given the infancy of this research area, future research should test different outcomes to further improve the predictive validity of the present models.
Supplemental Material
sj-docx-1-heb-10.1177_10901981231177075 – Supplemental material for Assessing Fear, Embarrassment, and Disgust in Colonoscopy: The Development of Measurement Instruments and Psychometric Evidence
Supplemental material, sj-docx-1-heb-10.1177_10901981231177075 for Assessing Fear, Embarrassment, and Disgust in Colonoscopy: The Development of Measurement Instruments and Psychometric Evidence by Wei Peng, Jocelyn McKinnon-Crowley, Qian Huang and Bingjing Mao in Health Education & Behavior
Footnotes
Acknowledgements
The findings reported in this manuscript have not been previously published and that the manuscript was not being simultaneously submitted elsewhere. The Institutional Review Board at Washington State University reviewed the study protocol and provided exemption certification prior to data collection. Informed consent was obtained from all participants included in the final sample. All procedures adhered to ethical standards for research involving human participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.