
Abstract
Health behaviors such as physical activity (PA) are socially influenced, such that individuals from shared social networks or living environments may exhibit similar habits. This cross-sectional study examined associations of social support, social control, and family member stage of change with moderate-to-vigorous self-reported and objective PA in dyads of adult Hispanic family members. We used the Godin Leisure-Time Physical Activity Questionnaire to assess self-reported PA and accelerometry for objective PA. Validated scales assessed social support, social control, and stage of change. We performed multivariable multilevel analysis using generalized estimating equations (GEE) to account for within-dyad correlations. We conducted multivariable negative binomial regression for Metabolic Equivalent Task minutes (MET-minutes) (self-reported; N = 429) and accelerometer data (N = 356) and logistic regression for meeting PA guidelines (self-reported; N = 429). Most dyads were spouses (41%) or parents and adult children (32%). Individuals with high family support had 81% higher odds of meeting PA guidelines (1.81 adjusted odds ratio (aOR); 95% confidence interval [CI] = [1.06, 3.09]; p = .030) and 58% higher leisure-time MET-minutes of PA per week (1.58 adjusted incidence rate ratio [aIRR], 95% CI = [1.30, 1.91]; p < .0001) than those with low levels of support. Participants reporting medium-to-high family punishment were 98% higher in odds of meeting PA guidelines (1.98 aOR; 95% CI = [1.09, 3.61]; p = .025) and had 70% higher leisure-time MET-minutes of PA (1.7 aIRR; 95% CI = [1.36, 2.13]; p<.0001) compared with those with low scores. Participants with study partners in action or maintenance stages had significantly higher leisure-time MET-minutes of PA per week (aIRR = 1.45, 95% CI = [1.10, 1.91], p = .009 and aIRR = 1.33, 95% CI = [1.01, 1.76], p = .041, respectively) compared with those with partners in other stages. No statistically significant associations were observed for social control with any measure of PA or between psychosocial measures and accelerometer-assessed PA. Our findings demonstrated that interventions should engage social networks and multimodal forms of PA assessment to optimize behavior change in similar populations.
Keywords
Physical inactivity is strongly associated with premature death, various cancers, and a range of chronic disease morbidities, including obesity, cardiovascular disease, hypertension, and diabetes (Moore et al., 2016; Paffenbarger et al., 1978; Winzer et al., 2011; World Cancer Research Fund International, 2018). Despite its importance in modifying disease risk, most adults in the United States do not meet physical activity (PA) guidelines that recommend at least 150 minutes of moderate-intensity activity or 75 minutes of vigorous-intensity activity per week, or an equivalent combination (U.S. Department of Health and Human Services, 2018). National estimates suggest that Hispanic/Latino adults (heretofore just Hispanic) are less likely to meet PA guidelines compared with non-Hispanic Whites (Whitfield et al., 2021), although more recent findings are mixed as accelerometer-based data suggest higher levels of PA among Hispanics (Arredondo et al., 2016; Carlson et al., 2010; Marquez et al., 2010). Given the significant health benefits of PA, it is critical that we explore ways to optimize PA engagement and maintenance in this population.
Lifestyle behaviors such as PA, alcohol consumption, diet, smoking, and sedentary behaviors are often socially influenced, such that individuals in shared social environments are likely to exhibit similar health behaviors (Eyler et al., 1998; Hartweg et al., 2012; Homish & Leonard, 2008). For Hispanic families, the cultural value of familism (where the family’s needs and family cohesiveness are prioritized over individual needs) may play a role in shaping health behaviors, such as PA (Perez & Cruess, 2014; Sabogal et al., 1987). As such, tapping into the family unit as an agent for behavior modification may hold promise in promoting positive PA attitudes and behaviors among Hispanic populations (Emmons, 2000). By examining dyads, we can gain valuable insights into how key psychosocial factors such as social support, social control, and readiness for behavior change, influence PA engagement. For social support in particular, multiple racially and socioeconomic diverse studies provide strong evidence that social support -family support in particular- is positively associated with PA engagement (Carron et al., 1996; Eyler et al., 1999; Filomena-Scarapicchia et al., 2017; Kim et al., 2008; Treiber et al., 1991). In addition to social support, social control may also influence health by regulating the health behaviors of others (Fekete et al., 2006; Khan et al., 2013; Lewis & Rook, 1999; Stephens et al., 2010). Social control is expressed through positive reinforcement (persuasion), which includes instrumental support and motivational approaches, or negative reinforcement (pressure), which relies on prodding, nagging, and inducement of guilt (Khan et al., 2013; Stephens et al., 2010). Prior studies indicate that pressure tends to be ineffective or even counterproductive; participants describe hiding unhealthy behaviors, exhibiting less motivation to change, and reporting psychological distress. In comparison, persuasion has been associated with positive behavior change –including adherance- and less psychological distress (Fekete et al., 2006; Lewis et al., 2006; Stephens et al., 2010). Studies also indicate that one person’s stage of change (readiness to modify existing behavior) may influence the PA behaviors of a close friend or family member, and vice versa. Within couples, studies suggest that one’s confidence to change PA habits was shaped by their partner’s stage of change and personal attitudes toward that given behavior (Falba & Sindelar, 2008; Franks et al., 2012). Based on research by Prochaska and collaborators, individuals in the action and maintenance stages of change are more likely to meet PA guidelines, whereas those in the pre-contemplation, contemplation, and preparation stages are less likely to participate or even consider engaging in PA (Prochaska et al., 2008; Prochaska & Velicer, 1997).
These studies, along with others (Ashida et al., 2012; Congello et al., 2020; Emmons, 2000; Eyler et al., 1999; John et al., 2022; Lindsay Smith et al., 2017; Marquez et al., 2016), underscore the value of social interactions within the family in supporting positive PA behaviors. While most research on the associations of psychosocial factors (social control, family social support, and partner’s stage of change) with PA (self-reported and objective) has focused on individuals, our study provides a unique opportunity to examine these associations specifically within Hispanic families. In this study, we aimed to explore the social environment via the lens of social support, social control, and partner’s stage of change in relation to PA outcomes. We hypothesized that family support and positive social control would be positively associated with self-reported and objective (device-assessed) moderate-to-vigorous intensity PA (MVPA) and that individuals with study partners at a higher stage of change would engage in more MVPA than those with partners at a lower stage of change for PA. This study will enhance our understanding of how the family social context affects PA within this rapidly growing, yet still relatively understudied population.
Method and Analysis
Study Design
This cross-sectional analysis uses baseline data from a randomized controlled trial (RCT) that was designed to test the effectiveness of a family-based healthy lifestyle intervention delivered by community health workers (“Tu Salud, ¡Sí Cuenta!”/ “Your Health Matters!”) to increase PA and fruit and vegetable intake among Hispanic adult family dyads, which included spousal/partner, sibling, parent–adult child, and other family relationships. In this article, we examine self-reported PA collected using the Godin Leisure-time Physical Activity Questionnaire and objective accelerometer data.
Recruitment and Sampling
Bilingual and bicultural research staff, along with trained community health workers, recruited participants between June 2018 and March 2020 through community outreach efforts at churches, community organizations, clinics, community events (e.g., health fairs), and schools. In-person assessments were conducted at baseline and 6-month and 12-month follow-ups. Eligibility criteria included residence in specific Houston neighborhoods where the study took place, English or Spanish speaker, possession of a working mobile phone, Hispanic, between the ages of 18 and 70 years old, not meeting PA guidelines (self-reported PA < 150 minutes/week of leisure MVPA) or insufficient fruit and vegetable intake (<5 cups/day), physically able to engage in PA based on the Physical Activity Readiness Questionnaire (PAR-Q) (Thomas et al., 1992) or with medical authorization, and able to enroll with an eligible family member as their study partner. Women who were pregnant or planning to become pregnant during the study period were not eligible to participate given that pregnancy is associated with changes in activity and weight gain, and PA can be contraindicated for certain pregnancy-related complications. Study visits took place in community settings (e.g., community organizations, churches). Both members of the dyad were required to attend the baseline visit together. The research staff explained the study procedures and obtained written consent. The survey was administered using REDCap on a laptop with touchscreen capabilities. Research staff first administered the demographic and PA questions and then the participants completed the remaining questions on their own unless they desired assistance. All study procedures were approved by The University of Texas MD Anderson Cancer Center’s institutional review board and ethics review committee.
Measures
PA —Dependent Variables
Godin Leisure-Time Physical Activity Questionnaire (Self-Reported PA)
Using the modified version of the Godin Leisure-time Physical Activity Questionnaire, we obtained data on the frequency and duration of strenuous, moderate, and light PA (lasting ≥10 minutes) performed during leisure time in a typical week, as reported by participants (Godin & Shephard, 1985). We created weighted scores by multiplying the Metabolic Equivalent Task (MET) values to convert minutes of PA into weekly MET-minutes of PA (Godin, 2011). Self-reported PA outcomes included the following: (a) total weekly MET-minutes of PA and (b) a binary variable indicating whether PA guidelines were met, with 600 MET-minutes as the cutoff (Jette et al., 1990).
Accelerometer (Objective PA)
We also measured MVPA using the Actigraph wGT3X+ accelerometer (Actigraph LLC, Pensacola, FL, USA). Participants were instructed to wear the device on their hip for 7 days during all waking hours except when bathing or swimming. We classified wear and non-wear times using validated methods established by authors, (Choi et al., 2011). Although 4 days of 10-hour wear is preferred, we selected 3 days as the minimum to allow additional participant data to be included as a similar approach has been used in other studies, including the Study of Latinos (Arredondo et al., 2016; Evenson et al., 2015). Cut-points for estimating moderate and vigorous PA were used based on established thresholds (moderate PA: 1952-5724 counts/min) and (vigorous PA: ≥5725 counts/minutes) (Freedson et al., 1998). The objective PA outcome included mean daily minutes that participants were engaged in MVPA.
Psychosocial Variables —Independent Variables
Social support for PA from family members (i.e., not limited to the study partner) was assessed using two subscales: Family Participation (10 items) and Family Punishment—criticizing or complaining (2 items) of the Social Support for Exercise Scale. Questions inquired about how often family members provided words of encouragement, participated in PA with the participant, or complained about the participant’s activity. Responses ranged from “none” (1) to “very often” (5) (Sallis et al., 1987). Social control assessed the extent to which participants perceived their study partners as using positive (persuasion, 3 items) and negative (pressure, 3 items) strategies (Lewis & Rook, 1999; Sorkin et al., 2014). Participants were also asked to indicate the frequency with which their study partner sought to exercise health-related social control in the past month using a 6-point scale from “0—not at all” to “5—everyday.” For example, participants were asked to think about the past3 months and respond to prompts including, “how often did your partner do things to help you eat better or exercise more,” “how often did your partner criticize you for what you eat or for not exercising,” or “how often did your partner try to convince you to eat better or exercise more.” Questions assessing the stage of change for PA inquired about current activity levels and plans for meeting national PA guidelines of 150 minutes of leisure MVPA per week to categorize participants into the various stages of engagement, including precontemplation not (no intentions of meeting PA guidelines) contemplation (intending to meet guidelines within 6 months), preparation (intending to meet guidelines within 30 days), action (has met PA guideline for less than 6 months), and maintenance (has met PA guidelines for at least 6 months (Prochaska et al., 2008; Prochaska & Velicer, 1997; Robinson et al., 2008).
Demographic Characteristics—Covariates
Demographic data on age, sex, marital status, type of dyad relationship, country of birth, body mass index (BMI), education, annual household income, insurance status, employment, and whether study partners resided in the same household were collected using a detailed demographics questionnaire with survey items adapted from Behavioral Risk Factor Surveillance System (Centers for Disease Control and Prevention [CDC], 2017). Anthropometric data on height and weight were collected by trained research staff using a Tanita calibrated digital scale and stadiometer to calculate BMI (kg/m²). Using CDC cutoff guidelines, the following weight categories were established: underweight (BMI<18.5 kg/m²), normal weight (18.5–24.9 kg/m²), overweight (25–29.9 kg/m²), and obese/morbid obesity (30 kg/m² or above).
Statistical Analysis
Initially, we analyzed the distributions of variables of interest, considering the presence of missing data and outliers. We summarized descriptive statistics for all demographic variables of interest using frequency (%) for all categorical variables and mean and standard deviations (SD) for continuous variables.
We conducted multilevel analysis using the generalized estimating equations (GEE) method, which accounts for the correlations of individual observations within a dyad, to assess the associations of independent psychosocial variables (social support, social control, and partner’s stage of change) with PA minutes (self-reported Godin moderate-vigorous MET-minutes per week) and logistic regression models for binary data, such as meeting PA guidelines (yes/no). Analyses adjusted for potential confounding effects from variables, including age, BMI category, sex, marital status, birth country, education, insurance, and accelerometer wear time (hours per day). These variables were selected for the final models based on their significance in the univariable analysis, consistency with the literature, data completeness, and lack of collinearity with other variables. Next, we conducted multilevel analysis using the GEE method to also assess the associations of independent psychosocial variables (social support, social control, and partner’s stage of change) with accelerometer-measured moderate-vigorous PA minutes per day and self-reported Godin moderate-vigorous MET-minutes per week as rate outcomes. Specifically, we applied multivariable negative binomial regression models for MET-minutes and accelerometer data and logistic regression models for binary data, for example, meeting PA guidelines (yes/no) after adjusting for potential confounding effects as noted above. We examined underlying assumptions, including the linearity of the association between continuous independent variables (social support, social control, and stage of change) and the outcome (PA), while building the multivariable models. If the linearity assumption was not satisfied, we categorized the continuous independent variables using widely used cutoffs or quantile-based categories, ensuring that each category had a sufficient frequency of observations. In addition, since we found multicollinearity issues among the subscales of the main independent variables (social support, social control), we conducted analysis for each variable separately. Finally, while not a primary aim of the study, we tested interactions during the model-building process to identify any significant terms that could have influenced the outcome. Statistical significance was evaluated at the level of 0.05. All analyses for this study were conducted using Stata statistical software (Version 16.1.; StataCorp, College Station, TX, USA).
Results
Demographic Characteristics
A total of 1,338 individuals were screened for the study, 908 were eligible, and 450 participants enrolled in the RCT as 225 family dyads. For analysis of self-reported activity data, 21 participants had missing or implausible values for Godin variables and were excluded. Table 1 displays the characteristics of study participants. The average age was 40.5 (SD 12.7) years, 76.5% were women, 85.8% were in the overweight or obese category, 87.6% were born outside the United States, 72.6% of participants were married or living with a partner, 75.5% reported an annual household income less than $40,000, and 50.4% did not complete high school. More than half (55.7%) of the participants had health insurance, and 37.3% reported being employed.
Study Demographics (N = 429).
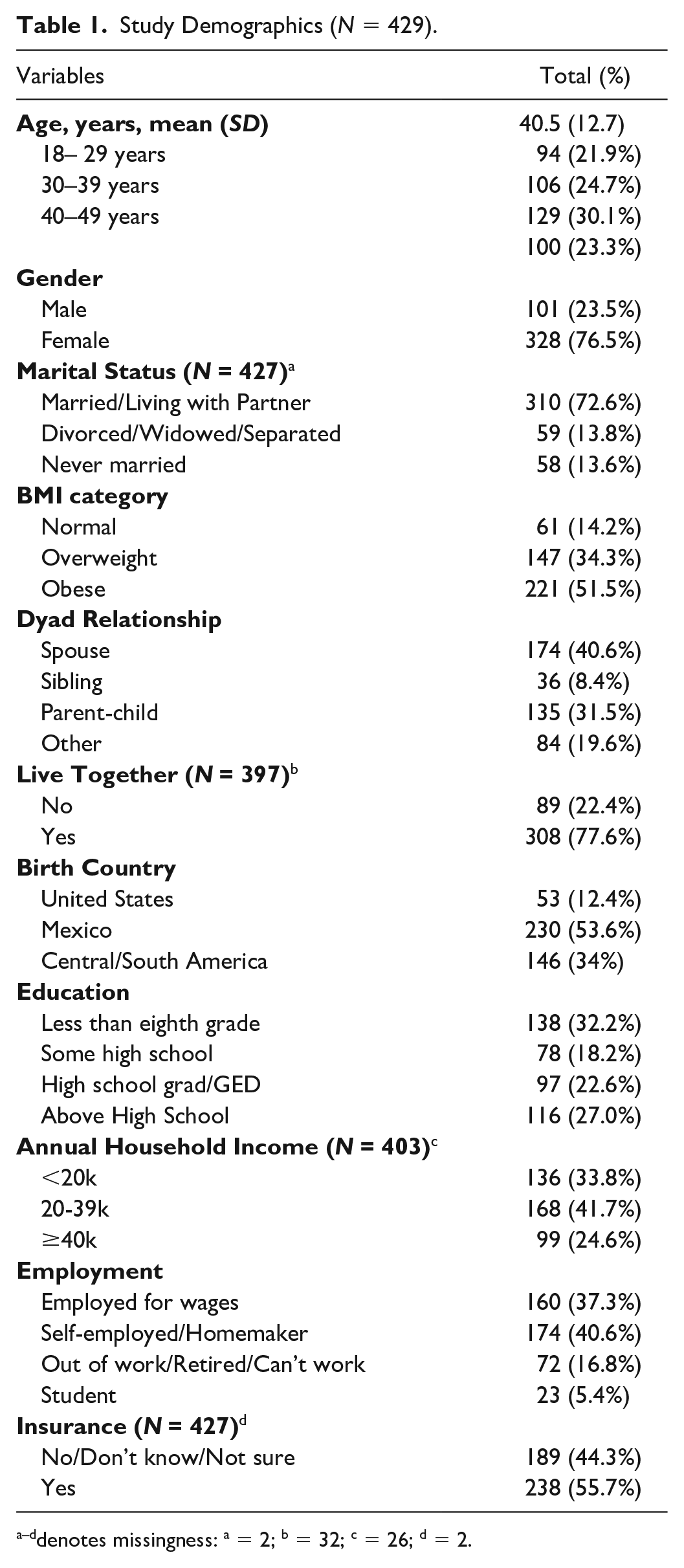
denotes missingness: a = 2; b = 32; c = 26; d = 2.
Association of Social Support, Social Control, and Partner’s Stage of Change With PA Outcomes
Based on self-reported Godin-Leisure PA, 73.4% did not meet PA guidelines. The overall estimated mean of Godin-leisure PA was 449.5 MET-minutes per week and the overall estimated mean of accelerometer-measured MVPA was 38.2 minutes per day.
Godin Leisure-Time MET-Minutes
Our analysis revealed that social support, family participation, and family punishment were significantly associated with higher odds of meeting PA guidelines based on Godin leisure-time MET-minutes in univariable models. Moreover, these associations persisted even after controlling for age, BMI, gender, marital status, birth country, education, and health insurance in multivariable models (Table 2). Specifically, participants who received high levels of family support were nearly twice as likely to meet PA guidelines as those who received low levels of family support (adjusted odds ratio [OR] = 1.81; 95% confidence interval [CI] = [1.06, 3.09]; p = .0304). In addition, participants who reported medium to high scores of family punishment were nearly twice as likely to meet PA guidelines as those who reported low scores (adjusted OR = 1.98; 95% CI = [1.09, 3.61]; p = .0253). Neither social control nor partner’s stage of change was significantly associated with the odds of meeting PA guidelines.
Logistic Regression Models for Psychosocial Variables and Meeting PA Guidelines Using Godin-Leisure Time (Based on MET Minutes).
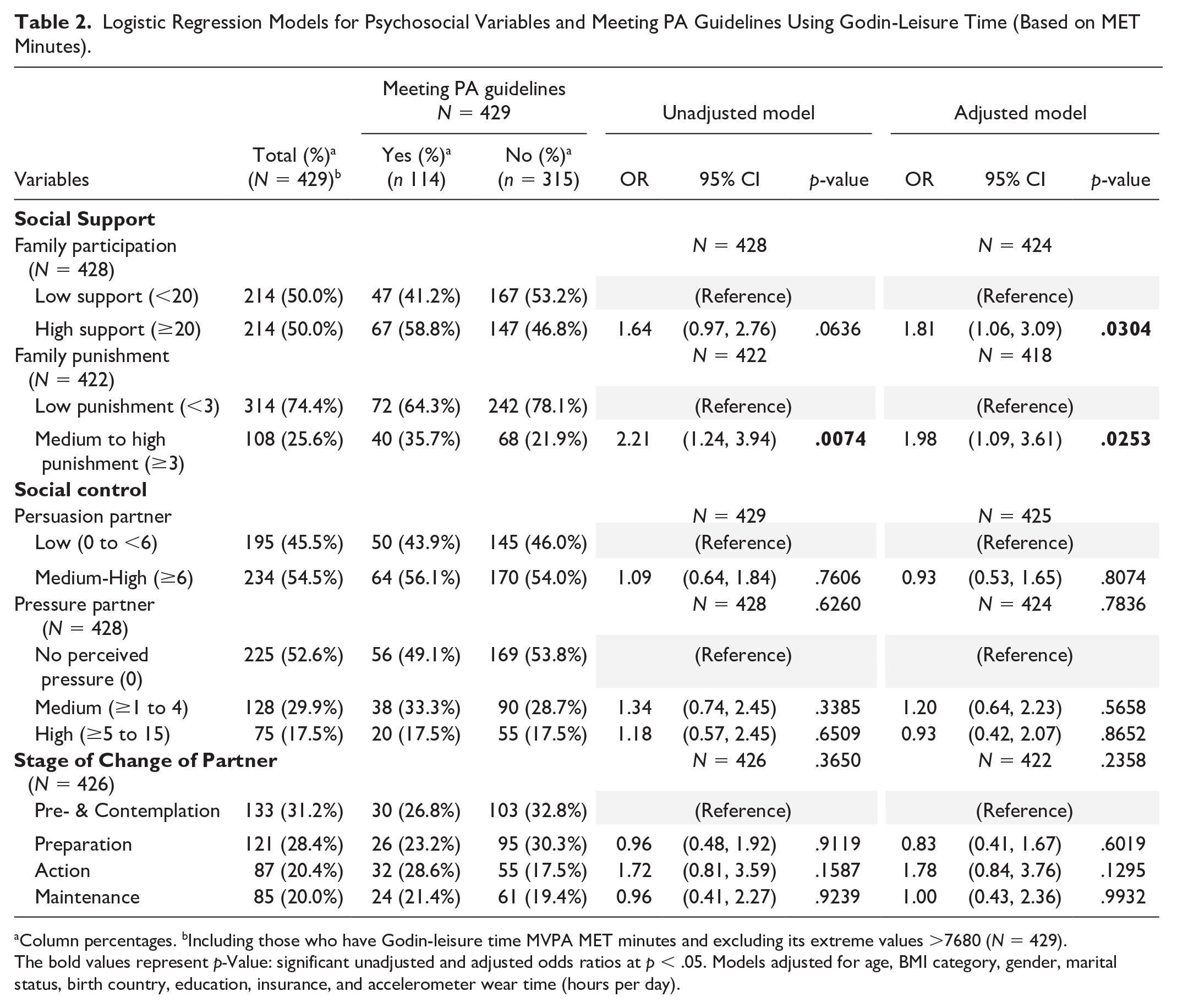
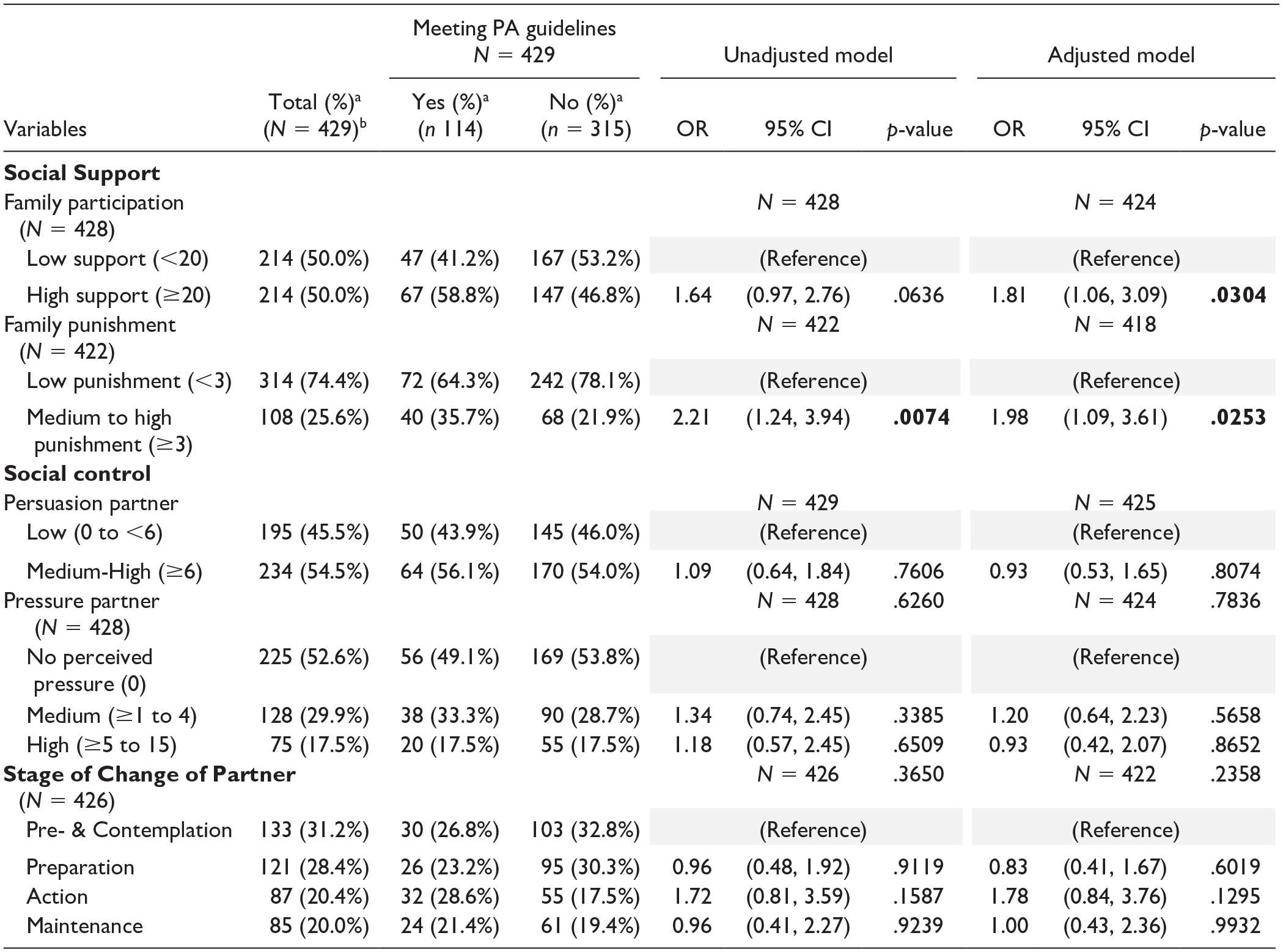
Column percentages. bIncluding those who have Godin-leisure time MVPA MET minutes and excluding its extreme values >7680 (N = 429).
The bold values represent p-Value: significant unadjusted and adjusted odds ratios at p < .05. Models adjusted for age, BMI category, gender, marital status, birth country, education, insurance, and accelerometer wear time (hours per day).
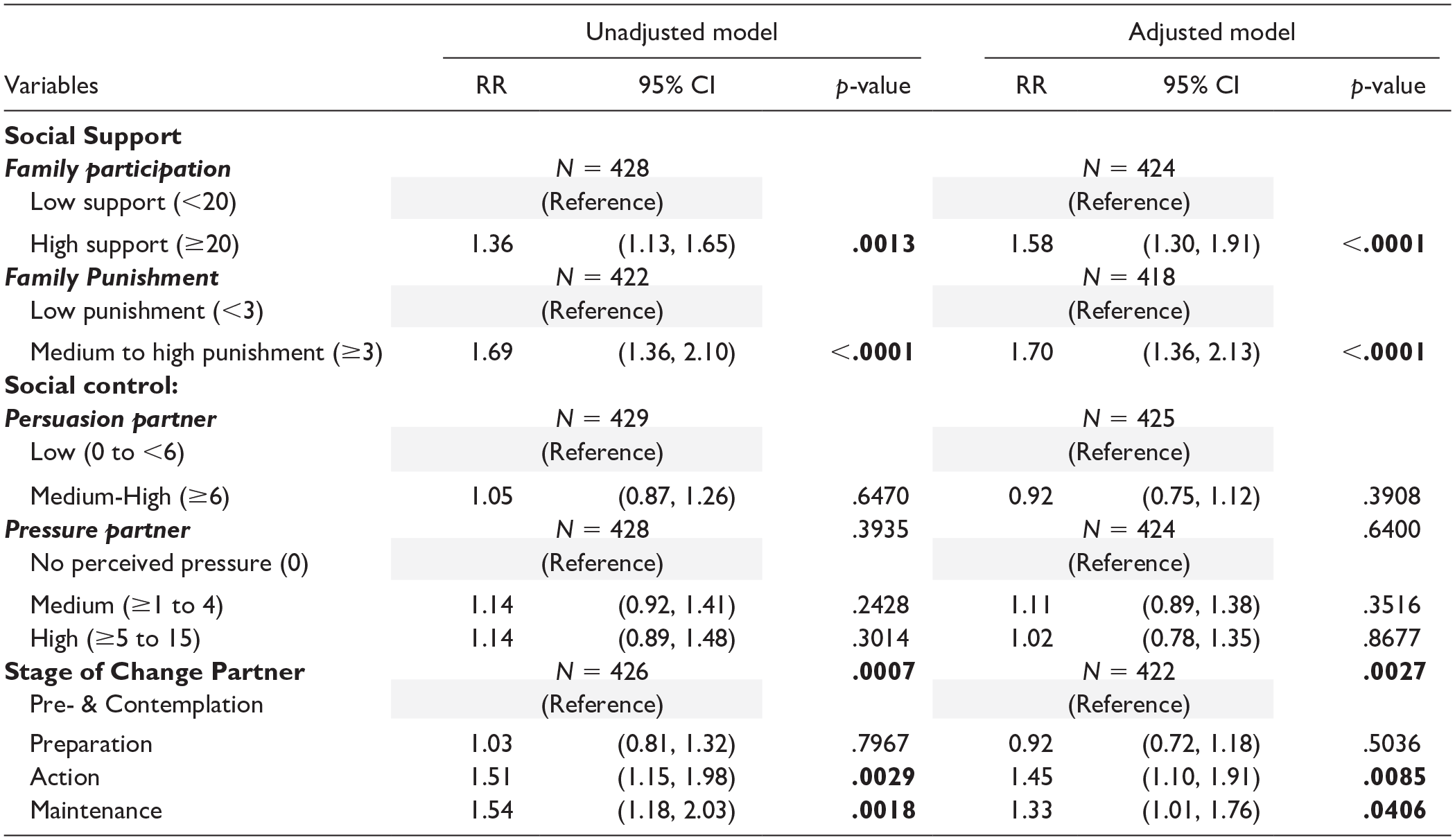
Social support factors were significantly associated with higher rates of Godin leisure-time MET-minutes of PA per week based on both univariable and multivariable modeling (Table 3). Participants who received high levels of family support were estimated to have, on average, 1.58 times greater leisure-time MET-minutes of PA per week than those who received low family support (adjusted rate ratio [RR] = 1.58; 95% CI = [1.30, 1.91]; p < .0001). Participants who experienced medium to high levels of family punishment reported engaging in 0.70 more leisure-time MET-minutes of PA per week than those who experienced low levels of family punishment (adjusted RR = 1.70; 95% CI = [1.36, 2.13]; p < .0001). Partner’s stage of change was also significantly associated with the Godin leisure-time MET-minutes of PA per week. Compared with those whose partners were in the pre-contemplation or contemplation stage, those whose partners were in either the action or maintenance stage had a higher rate of MET-minutes of PA per week (adjusted RR = 1.45; 95% CI = [1.10, 1.91]; p = .00850, and adjusted RR = 1.33; 95% CI = [1.01, 1.76]; p = .0406, respectively). Social control variables, on the other hand, did not show any significant association.
Negative Binomial Models Using GEE for Psychosocial Variables and Physical Activity (Based on MET-Minutes, N = 429).
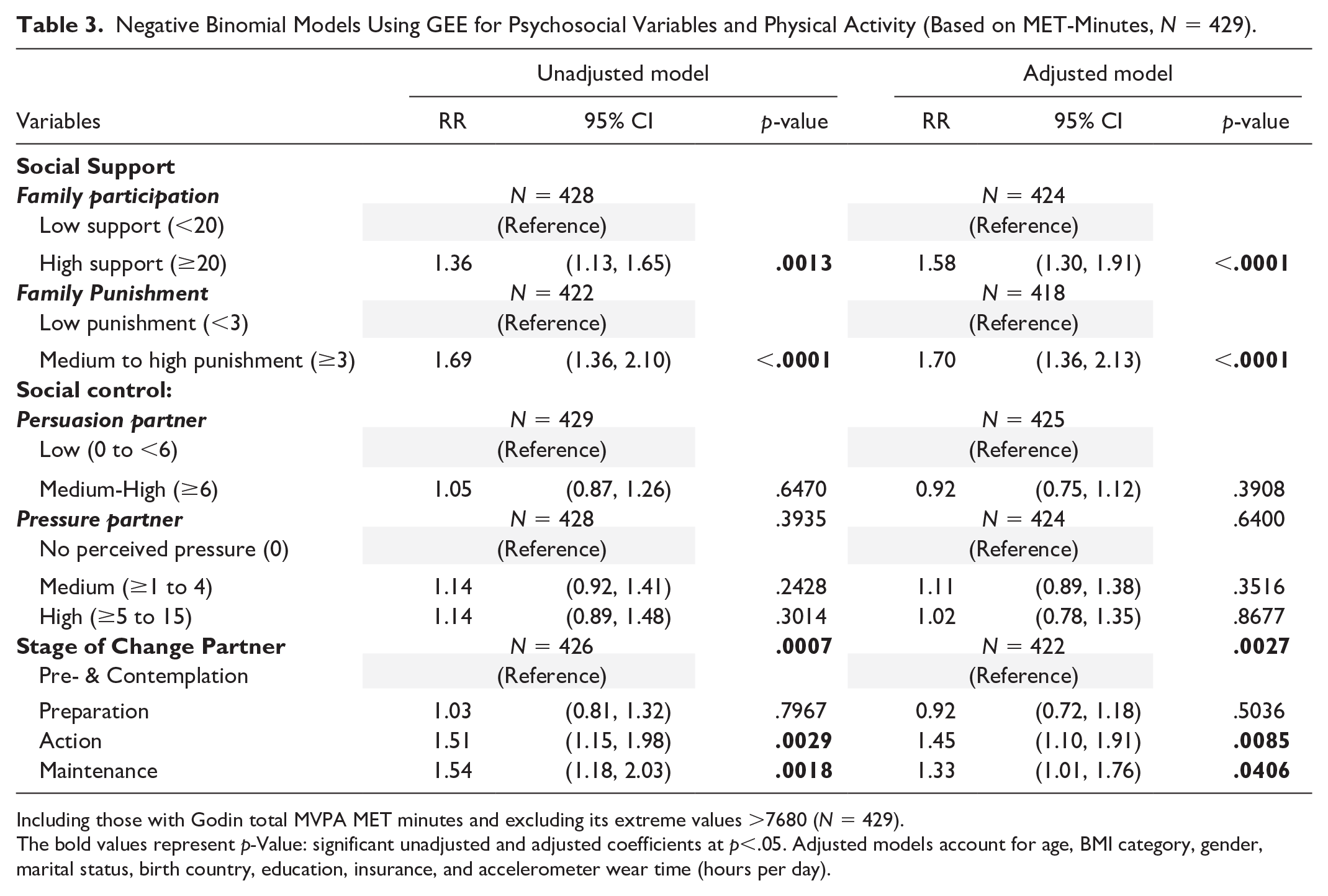
Including those with Godin total MVPA MET minutes and excluding its extreme values >7680 (N = 429).
The bold values represent p-Value: significant unadjusted and adjusted coefficients at p<.05. Adjusted models account for age, BMI category, gender, marital status, birth country, education, insurance, and accelerometer wear time (hours per day).
Accelerometer-Measured MVPA
Finally, for the analysis of accelerometer data, 94 participants did not have sufficient valid wear time and were excluded, bringing the sample size for this analysis to 356 (79%). We did not observe significant associations between accelerometer-measured MVPA minutes per day and any of the social support, social control, and partner’s stage of change variables (Table 4).
Negative Binomial Models Using GEE for Psychosocial Variables and Physical Activity (Based on Accelerometer-Actigraph Data, N = 356).
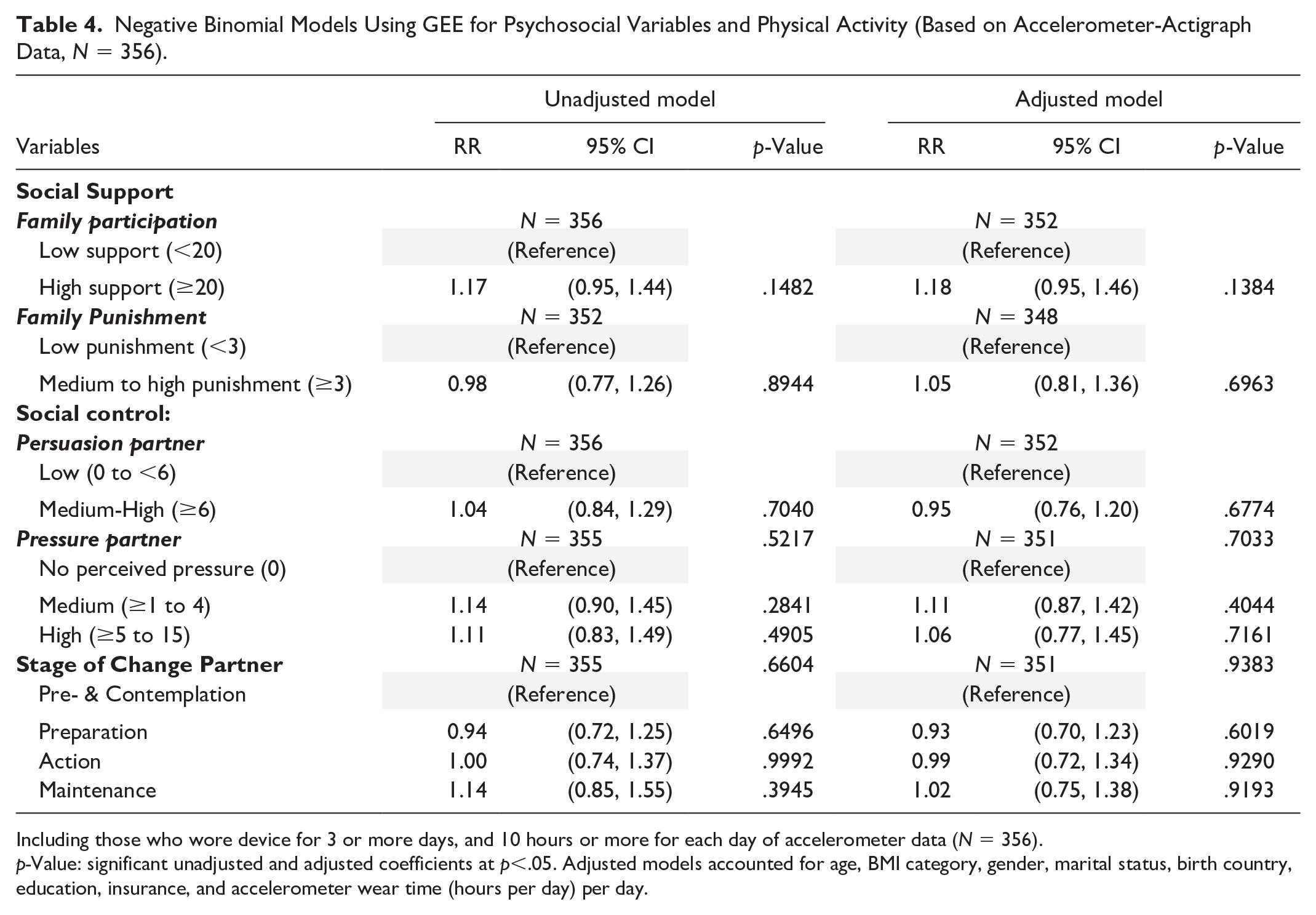
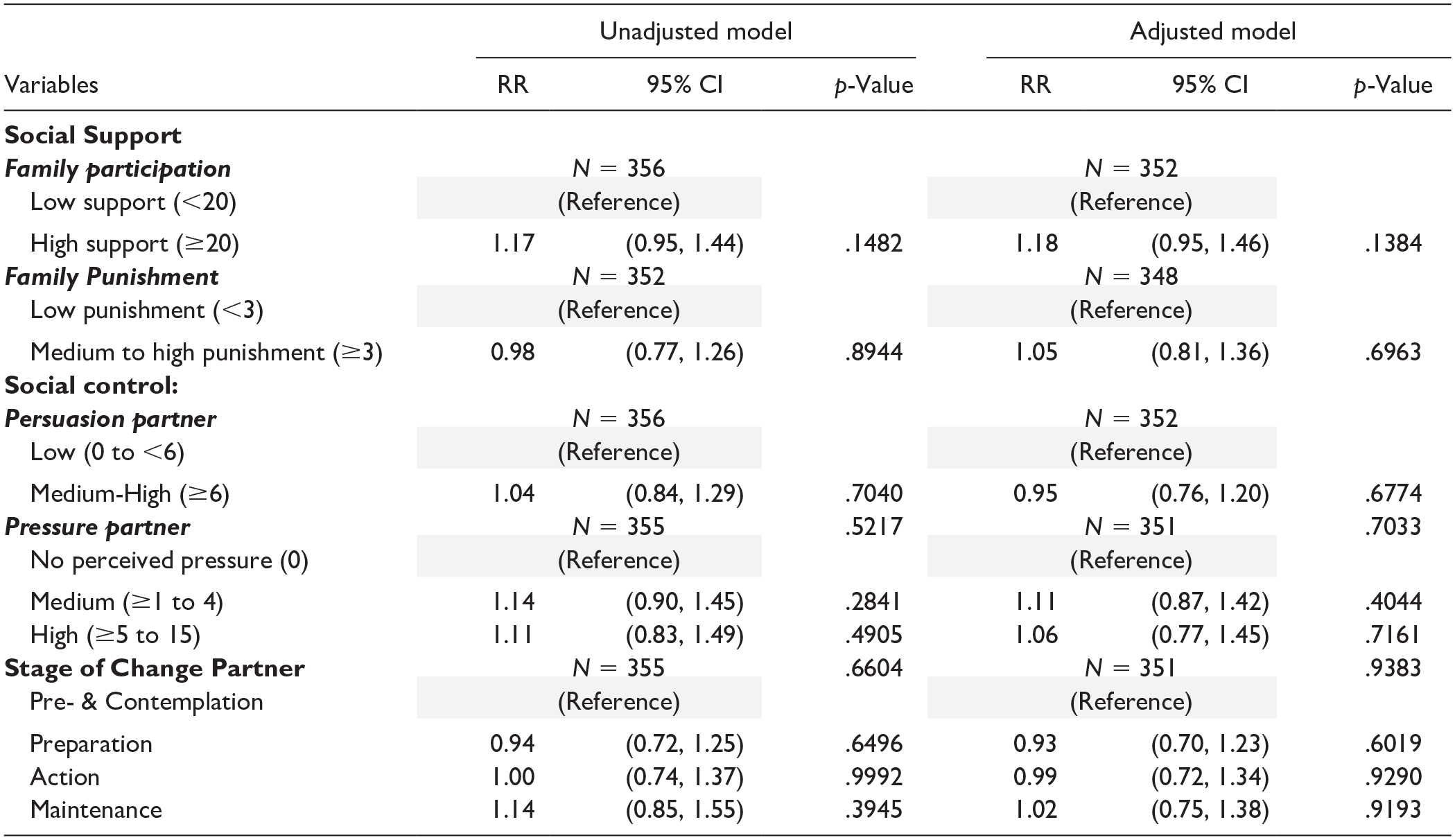
Including those who wore device for 3 or more days, and 10 hours or more for each day of accelerometer data (N = 356).
p-Value: significant unadjusted and adjusted coefficients at p<.05. Adjusted models accounted for age, BMI category, gender, marital status, birth country, education, insurance, and accelerometer wear time (hours per day) per day.
Discussion
In this study, we determined the associations between psychosocial factors (family social support, social control, and partner’s stage of change) and PA. The PA data were collected and analyzed as binary and continuous measures using the Godin Leisure-Time Physical Activity Questionnaire (self-reported) and accelerometer data (objectively measured) in a large sample of Hispanic family dyads. Logistic mixed-effect models demonstrated that high family social support and medium to high family punishment were positively associated with meeting PA guidelines compared with low social support—family participation and low social support—family punishment. Our negative binomial models showed similar findings with greater social support being linked to higher average leisure-time MET-minutes of MVPA per week compared with those who had low social support—family participation and low social support—family punishment. Our social support findings are consistent with existing studies that strongly support the associations between high family support and positive PA behavior (Carron et al., 1996; Eyler et al., 1999; Filomena-Scarapicchia et al., 2017; Treiber et al., 1991). These findings also align with existing studies that emphasize the significant role of Hispanic family values in supporting socially aligned behaviors such as PA (Eyler et al., 1999; Larsen et al., 2013; Marquez et al., 2016). Indeed, the likelihood of individuals engaging in PA increases when they receive support via encouragement and affirmation, physical accompaniment during exercise activities, and reminders to exercise. Marquez and coauthors showed that an intervention to increase social support led to higher levels of PA, due in part to increased family support (p < .05) (Marquez et al., 2016). These findings suggest that integrating family-centric strategies (e.g., friend- and family-focused, group-based, and promotora-led initiatives) to promote PA in Hispanic households may translate positively in real-world settings (Larsen et al., 2013).
Interestingly, our regression analyses showed that medium to high family punishment was significantly associated with both binary and continuous PA outcomes. This means that participants were more likely to indicate higher levels of MVPA per week if they reported that their family “criticized or made fun of them for exercising” or “complained about time spent exercising” (Sallis et al., 1987). This association is somewhat surprising as disapproving of exercise has been associated with lower levels of PA engagement. The research on family punishment and PA is relatively sparse. One study found that higher family punishment was associated with greater odds of being overweight and obese but was not associated with PA (Craven et al., 2018). A longitudinal study found that the impact of family punishment (where family complained about PA) was mitigated when support from friends was factored in (Heredia et al., 2019). In addition, prior qualitative research has shown that Hispanic women have described being discouraged from exercising by others, including their husbands, which may reflect gender and cultural beliefs toward PA (John et al., 2022; Larsen et al., 2013).
We also observed that for the relationship between partner’s stage of change and PA as a continuous variable, study participants with partners in either action or maintenance stages had higher self-reported MET-minutes of MVPA per week compared with those with study partners in pre- and contemplation stages. This finding is consistent with existing literature, which has shown an increased likelihood of positive behavior adoption when partners were at a similar stage and jointly interested in making healthy adjustments (Falba & Sindelar, 2008; Franks et al., 2012; Lewis et al., 2006). With this concordance, it is conceivable that motivation and greater accountability for behavior change are present (Franks et al., 2012). A previous study observed that spouses’ stage of change was positively associated with PA in women but not men (Franks et al., 2012), which is in line with research that has highlighted the importance of social support for women (Marquez et al., 2016). Further research in this area would help to inform the design of effective interventions that address the needs of both men and women.
Our study allowed for a thorough examination of the relationships between social support, social control, and stage of change and self-reported and objective PA in adult Hispanic family dyads. As noted above, the observed associations between the psychosocial measures and self-reported MVPA were not significant when we examined objective PA. This finding is not entirely unexpected as self-reported leisure-time PA and PA measured with accelerometry are not equivalent constructs; accelerometers capture movement, whereas self-report questionnaires assess behavior and behavioral context (Troiano et al., 2014; Welk et al., 2023). Moreover, here we assessed self-reported purposeful MVPA with a duration of at least 10 minutes in a typical week, whereas the accelerometer-derived PA represented total cumulative daily MVPA. Indeed, the objective PA suggests a higher level of activity than that captured by self-report. The psychosocial measures examined here would be expected to be more strongly associated with purposeful MVPA performed during leisure time than to activity occurring within other domains that also contribute to total cumulative MVPA. Importantly, self-report measures and accelerometry both have their respective strengths and limitations. Self-reported PA is subject to recall and social desirability bias and may under- or overestimate PA engagement (Prince et al., 2008; Sallis & Saelens, 2000). Accelerometers provide objective and precise assessments of most types of activities; however, they are costly, may be burdensome to participants, and may not capture all activities (e.g., cycling, swimming). As such, it is important to collect and report data from both types of assessments, recognizing that they are not interchangeable (Troiano et al., 2014; Welk et al., 2023). Collecting both types of data may provide relevant insights on behavior and movement that can altogether enhance understanding of PA correlates and guide intervention design and evaluation.
Several limitations of this study should be noted. First, participants were recruited via nonprobability sampling methods as recruitment strategies focused on community-based approaches. In addition, Hispanic individuals who were unable to find a family member to participate with them were excluded from this study. Thus, findings may not generalize more broadly within the Hispanic population or to other racial/ethnic populations. Second, the Godin questionnaire focuses exclusively on PA performed within leisure time and does not capture PA that occurs within other domains. In addition, the Godin questionnaire focused only on activity occurring within bouts of at least 10 minutes, which is no longer consistent with the updated Physical Activity Guidelines for Americans (2nd edition) (U.S. Department of HHS, 2018). However, a recent study suggests that whether self-reported MVPA is assessed within bouts or in aggregate has minimal impact on PA estimates (Ussery et al., 2020). Third, the social support scale was for exercise only and does not include diet. However, the social control question addressed both diet and exercise, which could explain in part why we did not see significant associations for this variable. Finally, a smaller proportion of participants had valid actigraph data (79%) compared with self-reported PA (95%), which may have created bias and/or limited power to detect significant associations. However, this study also included noticeable strengths. This study is one of few to examine associations between psychosocial factors (social control, family social support, and partner’s stage of change) with both self-reported PA (binary vs. continuous) and objective PA in a sample of adult Hispanic dyads. This research is important as it suggests the need for comprehensive and holistic approaches to examine variations in PA levels and associations of interest using different measurement strategies. Moreover, given the underrepresentation of Hispanics in research, relative to their proportion in the general population, this research is important to better understand the descriptive epidemiology of this population’s PA and ways in which interventions and public health programs can be better adapted to support optimal PA behaviors.
Conclusion
In conclusion, our study found statistically significant associations between self-reported PA data and variables, including social support and stage of change among adult Hispanic family dyads. Despite the lack of a statistically significant association between objectively measured PA and these variables, our significant findings on self-reported PA contribute to the body of literature that highlights the important role of the interpersonal environment to PA, particularly leisure-time and purposeful activity. Collectively, this research underscores the need for studies and public health practice to develop and evaluate interventions that leverage social networks as sources of social support for changing and maintaining PA behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Heart, Lung, and Blood Institute (1R56HL128705), the American Cancer Society (MRSG-13-145-01), and the National Cancer Institute through a Cancer Center Support Grant (CA016672)