
Abstract
Despite advancements in screening technologies, gynecologic cancers remain among the deadliest and most overlooked cancers. Early detection is crucial, but many women are reluctant to undergo screening due to various barriers and misconceptions. This study explores the motivations and barriers influencing women’s decisions regarding early gynecologic cancer screening in Malaysia. In-depth interviews were conducted with 20 professional women from diverse backgrounds using a qualitative approach. Data were analyzed through open and axial coding to identify key themes. An empathy map and user journey map captured the psychological and behavioral aspects of decision-making. The study identified themes such as lack of knowledge, reliance on social media and health care professionals, financial and time constraints, fear of results, and cultural stigmas. Participants with higher awareness were more likely to undergo screening, while those with personal or family cancer experiences showed greater vigilance. The findings emphasize the importance of culturally sensitive communication and health care professionals’ role in reducing stigma and promoting early screening. The study’s insights contribute to developing strategies to encourage early detection and improve health outcomes for women. These strategies align with the United Nations’ Sustainable Development Goals (SDGs), particularly SDG 3 (Good Health and Well-being) and SDG 5 (Gender Equality), promoting health equity and empowering women. As emphasized by SDG 17 (Partnerships for the Goals), achieving these goals requires strong partnerships and collaborative efforts to create a supportive environment for early cancer screening initiatives. Policymakers can use these insights to foster health equity and empower women through supportive screening environments.
Keywords
Gynecological cancers, among the deadliest forms, remain significantly overlooked. In 2022, approximately 1,500,000 women worldwide were diagnosed with gynecological cancers (World Cancer Research Fund, 2024). Symptoms of these cancers are frequently mistaken for menstrual irregularities, delaying early intervention. However, global studies underscore the critical role of early prevention and detection in reducing mortality rates, with a fairly high survival rate when detected at an early stage of advancement (Ferrari & Giannini, 2024; Trinidad et al., 2020).
Given these facts, social science scholars are increasingly exploring methods to raise awareness, particularly through social marketing, a concept introduced by Kotler and Zaltman in the 1970s to influence behavior change. Social marketing applies conventional marketing approaches to positively impact social behavior, such as stopping drinking and driving, undergoing vaccination, and quitting smoking (Lee & Kotler, 2011). The approach primarily uses the “4 Ps” framework; Product, Price, Place, and Promotion, to design impactful health campaigns:
Product: In social marketing, the product is the adoption of new behaviors, such as early screening or discontinuing habitual behaviors like smoking.
Price: Behavioral changes often involve perceived tangible (financial) and intangible (time, effort, embarrassment, and societal stigma) costs.
Place: Accessibility to screening services and information channels significantly influences behavior adoption.
Promotion: Crafting culturally sensitive, relatable messages is crucial for resonance.
Even though social marketing in public health has a decades-long history, many initiatives fail due to a lack of a comprehensive approach that considers cultural and other environmental factors (e.g., economy, infrastructure). This often results in mismatched messaging that fails to resonate with public perceptions (Akbar et al., 2022; Wymer, 2015). To explore the main reasons influencing women to undergo early screening, it is necessary to understand their motives and, in some cases, the mental obstacles and hurdles they face. One theory that explains this phenomenon is Social Cognitive Theory (SCT), which identifies three key concepts: Self-Efficacy, Observational Learning, and Reciprocal Determinism (Luszczynska & Schwarzer, 2020; Schunk & DiBenedetto, 2020).
Self-efficacy refers to one’s belief in their ability to successfully overcome challenges and obstacles related to a decision or action. Financial and time constraints, for instance, may reduce the likelihood of undergoing screenings (Zhang et al., 2024). Generally, individuals who perceive they cannot afford the associated costs or allocate time for screening may experience lower self-efficacy, reducing their motivation to pursue early screening (Cavers et al., 2022; Guilford et al., 2017).
Observational learning plays a significant role in early cancer screening behavior, especially when individuals observe societal stigma. For women, these stigmas can range from discussions about reproductive health to situations where their private areas need to be examined by health professionals (Akoto & Allsop, 2023; Iragorri & Spackman, 2018).
Furthermore, cultural misconceptions that gynecologic cancers primarily affect older women or that only those with a family history are at risk may discourage women from seeking necessary screenings and medical attention (Akoto & Allsop, 2023; Iragorri & Spackman, 2018). Generally, stigma and misconceptions surrounding screening often arise from negative societal perceptions and beliefs about gynecologic cancers, leading to avoidance and fear of the screening process (Iragorri & Spackman, 2018).
The Health Belief Model (HBM) is another widely used framework to explain individual behavior in health-related contexts (Le et al., 2024). HBM effectively predicts health behaviors by explaining the relationship between perceived severity, susceptibility, benefits, barriers, and cues to action (Chin & Mansori, 2019; Joseph & Fleary, 2024). It suggests that individuals who perceive the severity of a health issue, such as cancer, and recognize their susceptibility or risk of developing it are more likely to take preventive actions (Chin & Mansori, 2019). Understanding the benefits of an intervention and perceiving fewer barriers to its implementation further increases the likelihood of behavior change (Grant-Alfieri et al., 2022).
In addition, individuals are influenced by cues to action, which can be internal, such as pain, discomfort, or disease symptoms (Feng et al., 2021; Yeung & Lu, 2022), or external, such as media, significant life events (having a family history), motivations from society or peers, and persuasive guidance from health professionals (Feng et al., 2021; Tavakoli et al., 2024). When public health communication through social marketing campaigns effectively supports these cues, individuals may demonstrate higher levels of engagement in preventive (proactive) behaviors to reduce the risk of disease (Chin & Mansori, 2019; McDonald et al., 2023; Olubodun et al., 2022).
By examining the viewpoints of various stakeholders, this study aims to identify the complex motivations and obstacles that affect women’s decisions regarding gynecologic cancer screening and prevention. Using a qualitative, exploratory approach, the research investigates the factors that either encourage or discourage women from participating in screening and preventive measures.
The findings will help develop more effective strategies to promote early detection and enhance overall health outcomes for women. This effort supports the United Nations’ Sustainable Development Goals (SDGs), specifically SDG 3 (Good Health and Well-being) and SDG 5 (Gender Equality), by fostering health equity and empowering women to take proactive steps in managing their health. In addition, achieving these goals necessitates strong partnerships and collaborative efforts, as highlighted by SDG 17 (Partnerships for the Goals), to create a supportive environment for early cancer screening initiatives.
Methodology
This study adopts a qualitative exploratory approach to investigate factors that may influence females to undergo early screening for endometrial cancer. In-depth interviews serve as the primary data collection method, utilizing a semi-structured format guided by a set of predeveloped questions (see Appendix). A team of three trained female interviewers conducted the interviews to minimize communication barriers related to social stigmas. Each interview was recorded and transcribed using MS Teams, with all transcripts double-checked by the interviewers to ensure accuracy and clarity.
Participants for this study were selected in public places, specifically transportation hubs such as long-distance bus terminals, train stations, and airports in Malaysia. Each participant was thoroughly briefed on the interview process and the management of their data in accordance with the approved ethical guidelines. Participation in the study was entirely voluntary, and participants were informed of their right to withdraw at any point without obligation. A total of 20 professional female participants from diverse backgrounds were interviewed. The data collection process concluded with the 20th participant as theoretical saturation was reached by the 17th interview, with no new insights identified by the research team.
The initial data analysis was done after receiving each sample for open coding. However, after completing the data collection process, to ensure consistency in analysis, the whole 20 samples were uploaded to tools (OpenAI—Chat GPT-4.0 and Microsoft Copilot). The second level of collective analysis was applied to avoid overlooking some codes that might have been missed in the first step. In the second step, axial coding was performed using two additional artificial intelligence (AI) tools (Cloud.ai and Gemini) to explore possible associations among the identified themes. The final outputs from each step were discussed and verified by the research team and an independent scholar to ensure the accuracy and reliability of the results (Hamilton et al., 2023; Li et al., 2024; Sun et al., 2025).
In the next step, an empathy map, a well-used tool in design thinking, was developed to discover individuals’ feelings, thoughts, environmental exposure, pain points, and gains they are looking for. The empathy map assists in identifying individuals’ feelings, behaviors, environmental exposure, main pain points, frustrations, and potential gains. Generally, using an empathy map can enhance the exploration of user attitudes and behaviors within the domain of interest, with a deeper understanding, and reveal any gaps in existing user data (Siricharoen, 2021). After finalizing the empathy map, the user journey map was developed to demonstrate the actions, emotions, pain points, insights, and opportunities at different stages of decision-making: Awareness, Consideration, Engagement, After Experience, and Postexperience.
Results
The study involved a diverse group of 20 participants spanning a wide age range. Nearly half (45%) were in their 20s, while the remaining 55% were above 30 years old (40% in their 30s and 15% aged 41 and above). Educationally, the participants were well-qualified, with 40% holding a degree, 40% a master’s degree, and 20% a PhD. This high level of education was reflected in their professional roles. Nearly half (50%) held junior and senior executive positions, while the other half were managers and senior managers. The participants were evenly divided in terms of marital status, with half married and half unmarried (Table 1).
Characteristics of the Participants (N = 20).

In the first step, the open coding approach was used to identify emerging themes from the provided answers to each question. In this step, coding was done based on the emergence of words and the meaning of each word in their context. The below findings are based on open coding of data, which focuses on the level of knowledge and awareness, source of the knowledge and information, issues related to stigmas and cultural taboos, and concerns about hurdles and obstacles.
Awareness and Knowledge
Based on the responses provided by the participants, the three main themes regarding knowledge awareness of gynecologic cancers are as follows:
Lack of Specific Knowledge: Several participants expressed a lack of awareness specifically about gynecologic cancers. They either had never heard of it before, confused it with other types of cancer, or struggled to understand the term “gynecologic.” Some participants mentioned they only had a general awareness of cancer but were not familiar with gynecological cancers specifically.
Basic Awareness or Professional Background: Generally, participants in this study showed a basic knowledge of gynecological cancers. However, when asked about more specific details, they mentioned that their knowledge is limited. A few participants demonstrated more extensive knowledge, mainly through reading or having a professional background related to science (e.g., psychology).
Personal Experience or Family History: Another recurring theme regarding the awareness was due to personal experiences or family history with cancer. The experiences ranged from having ovarian cysts to having a family member diagnosed with any of the gynecologic cancers.
Overall, these results reveal that the awareness level of participants is general and ranges from complete unawareness to basic knowledge through personal experiences.
Source of Information and Knowledge
Based on the responses provided by the participants, the three main themes regarding the sources of information are as follows:
Social Media and Digital Platforms: Social media such as Instagram, TikTok, Twitter, and Facebook are some of the primary sources of information for participants. Almost all participants noted that there is very limited content available on social media that has been developed by health authorities or verified professional medical doctors.
Health Care Professionals, Institutions, and Official Media: Participants mentioned that they consider health care professionals, such as medical officers and specialists, as their main and most reliable source of information. They also noted that the primary mediums to access this level of information are TV news, talk shows on TV, or static communication channels such as posters and brochures.
Personal and Family Experiences: The results show that having personal experience, either for themselves or with a close family member, had a significant impact on some participants’ level of awareness. This happens mainly due to the natural curiosity of individuals when they face an unknown phenomenon with a high impact on their personal life, which can be a main motive to search and explore further regarding that matter.
These results indicate while many mentioned social media as a primary and effective source of information, they also noted that this information is often unreliable or difficult to verify. The findings further suggest that participants still regard more conventional channels, such as posters, brochures, and TV shows, as more reliable sources for health-related information.
Hurdles and Obstacles
Based on the responses provided by the participants, the main themes regarding their concerns toward hurdles and obstacles to undergoing early cancer screening are as follows:
Associated Costs and Expenses: Cost and financial impact emerged as the main factors that can influence participants’ decisions to proceed with any sort of cancer screening, especially with private health providers. Although cost is considered the main factor for undergoing early screening, it has never been the sole contributor to the lack of intention by females.
Time Off and Lengthy Process: Time constraints and the perception that screening is time-consuming or associated with long waiting times in public health centers are other factors that women have highlighted. Although this may be due to very busy schedules or misperceptions, this factor is more significant among females who consider public health providers as the only affordable option.
Fear of Unbearable Results: Fear or anxiety about receiving potentially concerning positive results is another factor that almost all participants mentioned during interviews. This primarily occurs because much of the public still harbors a deep fear of cancer treatment, and there is still a strong misconception that cancer is incurable and there is almost zero chance of survival regardless of the stage of cancer progression. Generally, a lack of awareness about the screening procedure or fear of unknown or unexpected results contributed to reluctance among some participants.
Overall, while many participants acknowledge that early screening might be useful, concerns about costs, time constraints, and fear or anxiety about the process or results were significant factors influencing their intentions and decisions regarding screening.
Stigmas and Taboos
Based on the responses provided by the participants, the three main themes regarding stigma and taboos associated with gynecological cancer screening are as follows:
Doctor’s Gender Preference: The majority of participants mentioned that the gender of the health care practitioner is important for them when it comes to screening processes related to gynecological cancers. Generally, females are more comfortable and less embarrassed to undergo screening if the medical practitioner is female.
Language Barriers: The language barrier is another factor that some participants mentioned as one of the barriers. In multilingual societies where individuals can speak a few languages, including their mother tongue, having the conversation in their mother tongue seems to make individuals more comfortable when it comes to issues considered private.
Hymen Rupture Anxiety: A few participants also expressed concerns about hymen-related stigma and its importance for unmarried women in their community and society. The main question they had in mind was whether undergoing screening might lead to hymen rupture, which can be a big taboo in some more traditional societies.
These themes collectively highlight the varied perspectives and experiences of participants regarding the stigma and taboos associated with screening. While many participants expressed specific preferences related to the gender of the doctor and language or concerns over hymen rupture, few participants did not perceive cultural factors as significant barriers to undergoing the screening process (Table 2).
Summary of Thematic Analysis of Data.

After identifying the core concepts during open coding, the next step was axial coding. This stage focused on exploring how different factors, such as stigma and taboos, might interact with other identified elements. The aim was to understand how these interactions can shape participants’ intentions toward early screening.
Exploring the Association Between Stigma, Taboos, and Information Sources
Upon analyzing the participants’ responses regarding their sources of information and their perceptions toward stigma and taboos, several associations can be observed:
Medical Professionals as a Source of Information and Reduced Stigma: The results revealed an obvious association between the source of information and the level of stigma. Participants who mentioned professional or official health care provider channels as their source often showed lower levels of stigma or used words less associated with stigma.
Social Media and Perceptions of Stigma and Taboos: The group that mentioned social media (e.g., TikTok and Instagram) as the main channel for health information, especially about cancer, through unverified content usually produced by influencers, mainly used words related to higher stigma and skepticism.
Language Barriers in Relation to Stigma: Participants who highlighted language as one of their concerns throughout the screening also shared higher levels of stigma and taboos. This can happen due to several factors, such as having access to information that they can fully comprehend and are comfortable with.
Personal Experiences and Family History: Having firsthand exposure to cancer treatment, either as an individual or through a close family member’s experience, can significantly reduce the stigma and taboos toward the cancer screening process. This may happen due to the higher chance of survival or regret that screening could or should have happened earlier, which would have led to a higher chance of survival. These individuals are often highly motivated to advocate for promoting early screening.
Overall, while the results show that sources of information may influence perceptions of stigma and taboos, various other factors such as societal and cultural norms, and personal experiences may also play a role.
Factors Associated With Early Cancer Screening Intentions
Based on the participants’ responses, several associations between their knowledge and awareness of gynecologic cancers and their intention to undergo early cancer screening can be observed:
Awareness and Willingness to Undergo Screening: There is a strong association between the level of knowledge and awareness of gynecological cancers and the individual’s intention to undergo early screening. Generally, participants with a higher level of awareness have shown a greater intention to accept the process and go for tests. In contrast, individuals who mentioned that they did not have much experience or knowledge were more conservative about undergoing the early screening process, as they felt more anxious and fearful about the possible unfavorable outcomes.
Personal Experiences and Family History: Having firsthand experience is the most influential factor for individuals who have a family member or close associate diagnosed with any sort of gynecologic cancer. This group mainly expresses their vigilance and becomes receptive when it comes to any cancer test.
Cost Considerations: Perceived high costs associated with early screening are another factor that might create a mental hurdle for females and reduce their intention to undergo tests. Some with tight budgets often hesitate as they perceive that they cannot afford it. However, when the research team shared information regarding government-funded services that are fully or partially subsidized, this group tried to find other reasons (e.g., time, distance) not to go for tests.
Overall, while awareness and knowledge regarding gynecologic cancers play an essential role in shaping intentions toward early screening, other factors such as personal experiences, financial concerns, and access to health care resources also significantly influence decision-making. These findings suggest that the public health system should adopt a holistic approach to promoting early screening services rather than focusing on individual factors in isolation. To gain a better understanding of how individuals navigate the decision-making process for early screening, an empathy map (see Figure 1) was developed. The primary purpose of this map is to capture the target group’s psychological engagement and mental interaction with the process through various societal lenses, including self-perceptions, media exposures, interactions with family and peers, and the challenges they face along with potential solutions they seek.
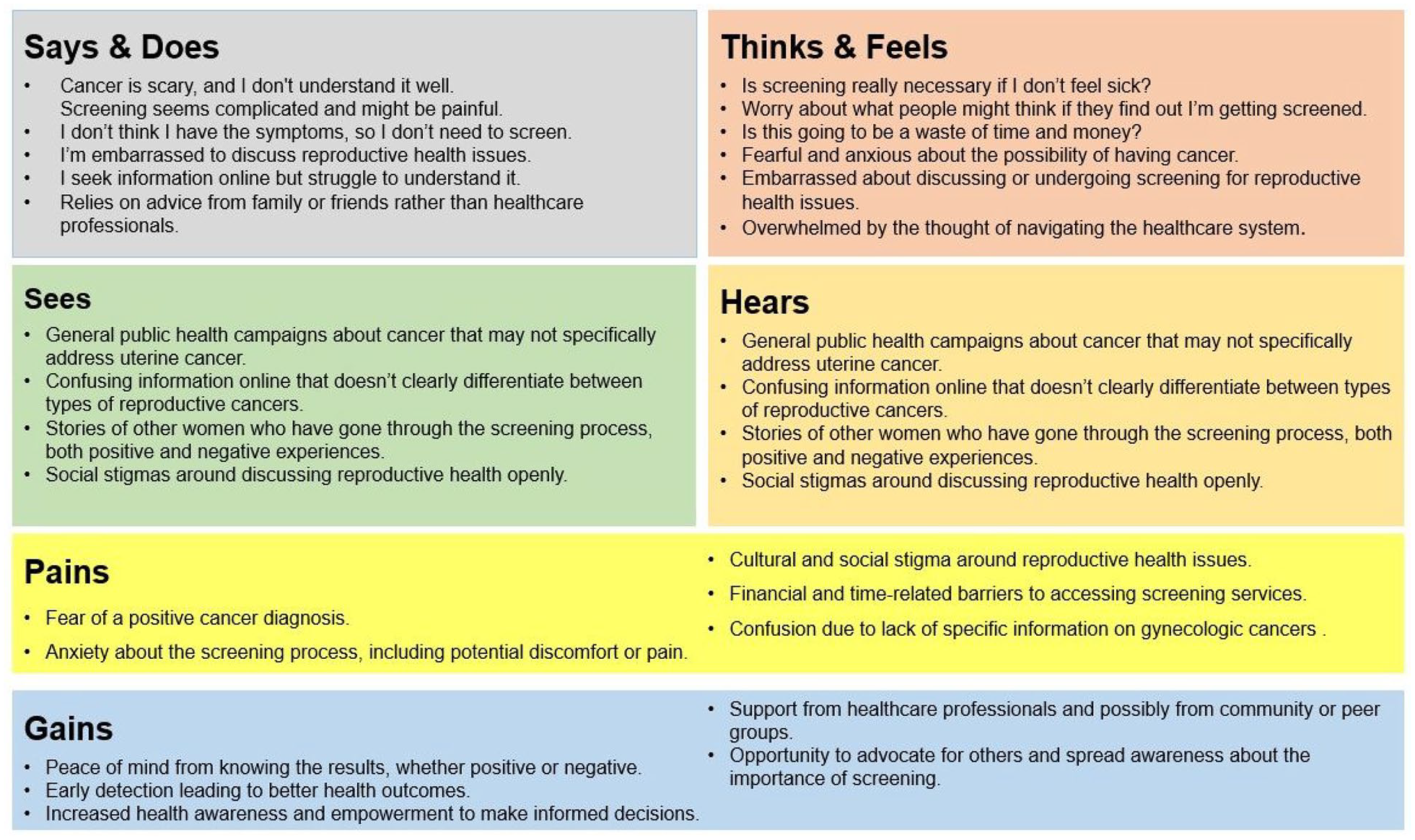
Empathy Map.
By considering the findings from open coding and axial coding and also incorporating the findings from the empathy map developed, the following user journey map was developed to better understand the individual journey throughout the entire experience, starting from Discovery, Evaluation, Engagement, Adoption, and Postengagement. In each stage of the user experience journey, actions, emotions, pain points, and insights were included to create the matrix.
Discussion
The summary of the analysis presented in the empathy map and user journey map revealed that women perceive several difficulties (pain points) while considering undergoing the screening process. They primarily focus on the following pain points:
Confusion due to lack of specific information on gynecologic cancers (Ferrari & Giannini, 2024; Trinidad et al., 2020).
Anxiety about the screening process, including potential discomfort or pain (Maheu et al., 2021).
Cultural and social stigma around reproductive health issues (Akoto & Allsop, 2023; Iragorri & Spackman, 2018).
Financial and time-related barriers to accessing screening services (Cavers et al., 2022; Zhang et al., 2024).
Fear of a positive cancer diagnosis (Chin & Mansori, 2019; Iragorri & Spackman, 2018).
Primarily, the results revealed a strong positive association between the level of awareness and other factors such as perceived obstacles and stigmas. Particularly, when an individual is fully aware of the effectiveness and importance of regular screening, the likelihood that they decide to go through the process is higher (Ferrari & Giannini, 2024; Trinidad et al., 2020). In addition, a higher level of awareness leads to acceptance of the cost and time required. Furthermore, having more accurate knowledge can be associated with the level of cultural stigma. It is always more comfortable to discuss reproductive organ diseases with health care professionals (nurses and doctors) when the individual is aware of the effectiveness of tests and the seriousness of delaying cancer detection at an early stage, making it easier to overcome this stigma (Akoto & Allsop, 2023; Iragorri & Spackman, 2018).
Although language is not the main barrier for educated individuals who can speak English, this study shows that women are more comfortable discussing their reproductive health issues with doctors and nurses who can speak their mother tongue. This may be due to having more confidence in understanding the terms and avoiding the need for a third-party translation during consultations.
In addition, having access to the right channels that provide accurate information can reduce misconceptions and stigmas. This can also reduce women’s anxieties. These insights serve as a foundation for health interventions aimed at increasing early detection through targeted awareness and screening behavior shifts, underscoring the promise of social marketing as a tool for meaningful change (Lee & Kotler, 2011; Wymer, 2015).
The findings show that only a multifaceted approach can address the women’s lack of interest in undergoing prescreening. Although each of the above findings is important to consider, like an orchestra, all parties involved in the decision-making process for women need to work seamlessly. Table 3 provides a fairly comprehensive view of the female journey in this process, from the discovery stage to postengagement. Emphasizing the importance of collaboration between several stakeholders, including health care providers, policy support, and even corporations, is crucial in overcoming barriers to gynecologic cancer screening.
User Journey Map.

While messaging and providing information to create awareness, using advice from health care professionals is crucial. However, businesses, as part of their ESG (Environmental, Social, Governance) initiatives, can also allocate part of their CSR (Corporate Social Responsibility) budget to promote the right message from health care professionals. This aligns with the 17 SDGs initiated by the United Nations in 2015. Participating in campaigns related to gynecologic cancer awareness can be mapped to SDG 3 (Health and Well-being) and SDG 5 (Gender Equality), as it can give women the chance to have better health and subsequently a more equal chance in the workplace and society.
This sort of partnership among different stakeholders not only can create a better corporate image in the market but also assist companies in enhancing their ESG rating index, which in return can give them access to a wider range of fund management as well as better market performance. Although partnerships with corporations can create a platform to have a wider reach of messages, communicating the right messages is still crucial.
At the discovery stage, the findings show that women’s concerns are more related to stigma, cultural taboos, and fear of the screening process or diagnosis. At this stage, partnerships with health professionals can give more credibility to awareness campaigns and make them more convincing from the audience’s point of view (see Table 4 for more details). The reach of this communication and campaign should not be limited to the general public, but it can be highly impactful if the campaign is channeled to schools, universities, and even workplaces through the human resource departments of companies. Essentially, the main insight of this research is that the level of awareness is low even among educated and professional women, which can shed light on the possibly very low awareness in smaller cities and even rural areas of developing countries.
List of Proposed Strategies to Promote Early Screening.

In addition, social media platforms, including Instagram, TikTok, and Twitter, have surfaced as significant information sources. With their expansive reach, these platforms offer health care organizations an effective communication channel. Collaborating with responsible influencers and producing engaging, accessible content could extend the reach of accurate information, helping to counter misinformation and foster open conversations about uterine cancer. This approach builds awareness and can also reduce stigma, making discussions around reproductive health more normalized.
Equally, the role of public policies in influencing screening perceptions stands out. Based on the findings, at the engagement stage, the main concerns are accessibility issues (location), cost, time, and lack of support during screening. Providing subsidized screening packages, facilities to shorten waiting times (e.g., online booking, mobile applications), and the use of technology such as AI chatbots can make the female experience easier and remove their major highlighted hurdles and obstacles (cost, time, stigma of discussing with others to gain information). In addition, public–private partnerships to facilitate mobile screening units to reach rural and underserved areas can be another effective channel to make screening services accessible to women. Table 4 provides a summary of insights on possible practical considerations.
Limitation of Study
While this study offers valuable insights into the barriers to undergoing gynecological cancer screening, the results should be interpreted considering the potential limitations associated with the methods and sampling. First, the findings are based on interviews where participants share their ideas, perceptions, experiences, and levels of awareness. This approach may introduce self-reporting biases, such as social desirability bias or recall bias, potentially leading to over- or under-reporting.
In addition, the findings should be generalized with caution due to the sample size and the study’s geographical focus on metropolitan areas in Malaysia. The perspectives gathered may not fully capture variations in awareness and attitudes across different demographic or rural populations.
Implications for Future Research
To address the limitations of this research, it is recommended that future studies explore similar topics in diverse cultural, societal, and economic contexts to identify context-specific challenges and best practices. Studies may use other qualitative approaches, such as focus groups and the Delphi method, to study this phenomenon from the perspective of professional health practitioners as well. In addition, longitudinal studies involving control and experimental groups with a larger number of participants can provide deeper insights into how individual behavior may evolve over time.
Furthermore, exploring multidisciplinary approaches integrating behavioral science, health communication, and digital engagement strategies may offer innovative solutions for improving gynecologic cancer screening rates. Future research can also focus on evaluating the effectiveness of the proposed solutions through empirical testing. Specifically, experimental approaches such as A/B testing could assess the impact of different communication strategies on awareness and screening behaviors.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.