
Abstract
Increasing colorectal cancer (CRC) screening requires delivery and adaptation of evidence-based and theory-guided interventions. The Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science (ACCSIS) consortium is funded by the National Cancer Institute, with a primary goal of increasing the availability and use of approaches to CRC prevention and control, from screening through follow-up testing, diagnosis, and referral to care. In this article, we present a framework for improving CRC, follow-up, and referral to care among populations that have low CRC screening rates. We used a multistep, consensus- and data-driven approach to develop the ACCSIS framework. Eight collaborating Research Projects of the ACCSIS consortium evaluated the draft; they provided feedback in relation to their study designs, settings, populations, and methods. They also used evaluation results to refine the framework until they reached consensus. The current framework reflects common elements, expected intervention and screening outcomes, and is intended to contribute to future ACCSIS analyses and others’ intervention and research plans. The framework recognizes the iterative nature of CRC screening programs and emphasizes multiple levels of influence—from baseline factors affecting selection of intervention components through measurement of process, screening, and implementation outcomes. Future researchers and practitioners can adapt the ACCSIS framework to advance CRC screening and to improve other cancer prevention and control research and practices that have created and perpetuated health disparities.
Colorectal cancer (CRC) screening is unevenly implemented in the United States, despite the availability of effective screening tests and strong evidence that screening saves lives (Islami et al., 2021; Joseph et al., 2020). Bringing CRC screening, including stool-based tests and colonoscopies, with appropriate follow-up and referral to care, to people who have historically been medically underserved, is essential to addressing health disparities. Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science (ACCSIS) is an initiative of the National Cancer Institute (NCI). ACCSIS researchers developed a unique conceptual framework for advancing delivery and testing of CRC screening. The framework can be used to assist CRC and other cancer screening researchers and program developers to design, deliver, and evaluate interventions to improve screening, follow-up, and referral to care among eligible populations.
Overall, at the population level, screening for CRC is associated with lower mortality from CRC (Lin et al., 2021). The estimated overall screening rate in the United States was 72% in 2020. However, uptake for many racial and ethnic groups was 70% or less, while uptake for people without insurance was 39% (Lin et al., 2021) and people served by federally qualified health centers was 40% (American Cancer Society National Colorectal Cancer Roundtable, n.d.). The COVID-19 pandemic also negatively affected uptake of CRC screening—during the pandemic, fewer people were screened, which will impact incidence and prevalence in the coming years (Alkatout et al., 2021; Mazidimoradi et al., 2022; Teglia et al., 2022). These stark differences in CRC screening and the impact of COVID-19 highlight the need to increase screening, particularly among populations experiencing health care disparities in cancer screening and mortality. Delivery and testing of evidence-based, multilevel interventions are required to increase screening among populations who are disproportionately impacted by CRC (Damschroder et al., 2009; Gupta et al., 2020; Proctor et al., 2011).
As part of its initial collaborative activities, the ACCSIS consortium developed a conceptual framework (“framework”) to formalize the preimplementation, implementation, and postimplementation processes over time and across levels. The aim is to enable a continuous learning cycle to optimize CRC screening uptake in populations experiencing a high burden from CRC. The framework will support the planned trans-ACCSIS comparative analyses, identify areas for improvement within the Research Projects, and provide guidance for researchers and practitioners to design, evaluate, implement, and maintain future efforts to study and improve CRC screening, follow-up, and referral to care.
In this article, we present the ACCSIS framework for improving CRC screening for all.
Method
About ACCSIS
This study was conducted as part of the NCI-funded ACCSIS consortium. The overall aim of ACCSIS is to conduct multisite, coordinated, transdisciplinary research to evaluate and improve CRC screening processes. By design, the ACCSIS Research Projects (Research Projects) focus exclusively on populations in their respective regions who had historically lower screening rates than national averages. These populations include urban, rural, and frontier participants; American Indian tribal members; and Black and Hispanic participants. Each Research Project is working with local clinical and community collaborators to understand what local features have been keeping screening rates low and what local resources can be engaged to increase screening, follow-up, and referral to care. New and existing community–academic partnerships are working in primary care settings to promote and implement CRC screening, with a focus on identifying elements that can be sustained and scaled up to benefit those in the region who are not a part of ACCSIS Research Projects. Results from ACCSIS Research Projects will provide new evidence regarding how multilevel interventions can reduce CRC disparities in the United States. Multilevel interventions include, for example, patient reminders at the individual level, provider assessment and feedback at the provider level, and outreach at health fairs at the community level.
The ACCSIS consortium consists of eight Research Projects; scientific collaborators from NCI; and a Coordinating Center to support trans-ACCSIS collaboration and comparative assessments. Five ACCSIS Research Projects have conducted interventions, such as those described in The Community Guide (Community Preventive Services Task Force, 2016), aimed at different levels of influence (e.g., patient, provider, or clinic staff). These interventions focus on populations with low CRC screening rates in areas of North Carolina; Appalachian Kentucky and Ohio; Chicago; Oregon; San Diego; and American Indian populations in New Mexico, Arizona, and Oklahoma. All ACCSIS Research Projects address multiple stages in the CRC continuum of care, from initial screening to follow-up diagnostic testing, as well as referral for cancer treatment. Consistent with the aim of expanding real-world practice-based evidence, the ACCSIS Research Projects are designed to be pragmatic.
Framework Approach
The framework was designed to achieve four goals: (1) to describe how interventions would address the needs of populations facing disparities; (2) to reflect the adaptive and iterative phases used in the ACCSIS program; (3) to identify and describe the interplay across multilevel interventions; and (4) to reflect that cancer screening is more than a single test. That is, “screening” is a process including many steps, both before and after the test itself. Screening can only affect mortality when the entire process is routinely completed.
Members of the ACCSIS consortium formed a work group to develop the ACCSIS framework. The work group members reviewed published health equity and implementation science models (Aarons et al., 2011; Chambers et al., 2013; Eslava-Schmalbach et al., 2019; Shelton et al., 2020; Singer et al., 2022; Stanton et al., 2022; Wallerstein et al., 2017; Woodward et al., 2019; Yousefi Nooraie et al., 2020), and determined that there were no prior frameworks that contained all the elements of the ACCSIS projects or that fully incorporated health equity. The work group developed the first draft of the framework by incorporating constructs from existing models and incorporating components based on the four ACCSIS conceptual model goals. The work group conducted a review of each of the eight Research Projects’ designs and data collection plans to assess the applicability of the framework.
The work group reviewed the next draft of the framework and provided feedback on missing constructs. To further evaluate the fit and face validity of the framework, the work group requested the ACCSIS Research Projects’ Principal Investigators (PIs) and staff from their teams to apply the framework to their own projects. The work group drafted a series of questions about the fit and face validity of the framework and asked the Research Projects PI and staff from their teams to respond (a copy of the questions is included in Appendices A and B). This process was intended to determine whether the framework was practical; to identify omissions and unnecessary components; and to ensure utility and generalizability of the framework for future projects. Each Research Project provided feedback on additional elements that should be considered for inclusion, as well as the overall applicability of the framework. A result of this feedback step was an added focus on community and partner engagement in the intervention selection process. The work group identified processes that fit well and processes that need tailoring, such as incorporating the iterative steps required for adapting and conducting interventions, as well as distinguishing between intervention elements with existing evidence and ad hoc support provided when preparing for implementation. Finally, we identified gaps in the constructs and added in cost and cost-effectiveness measures, and outcomes.
After incorporating feedback from the work group’s subsequent review of the framework, the final version was created. The framework has since been used to guide trans-ACCSIS analyses of patient navigation (Coronado et al., 2023), mailed approaches to screening with fecal immunochemical tests (FIT; Gupta et al., 2020), and ongoing discussions of how to document intervention adaptations.
Results
The ACCSIS framework (Figure 1) describes three phases of an iterative and continual process: preimplementation, implementation, and postimplementation. The preimplementation phase is the time in which evidence-based interventions are selected and steps are planned to deliver, or implement, the interventions. The implementation phase includes all the time when the intervention is ongoing in practice. Postimplementation is the time after the conclusion of the intervention (or sometimes the passage of a prespecified amount of time). After moving through each phase, projects can return to the preimplementation phase so that modifications can be made, as needed, to adapt the interventions to the context. Timeframes are not prescribed within each phase; rather, they are dependent on the complexity of the processes. As such, projects move through these phases at various speeds, based on their objectives, intervention requirements, study design, and outcomes of focus. This approach is designed to optimize the effectiveness of interventions in increasing CRC screening uptake. In some cases, rapid transitions can occur between the phases.
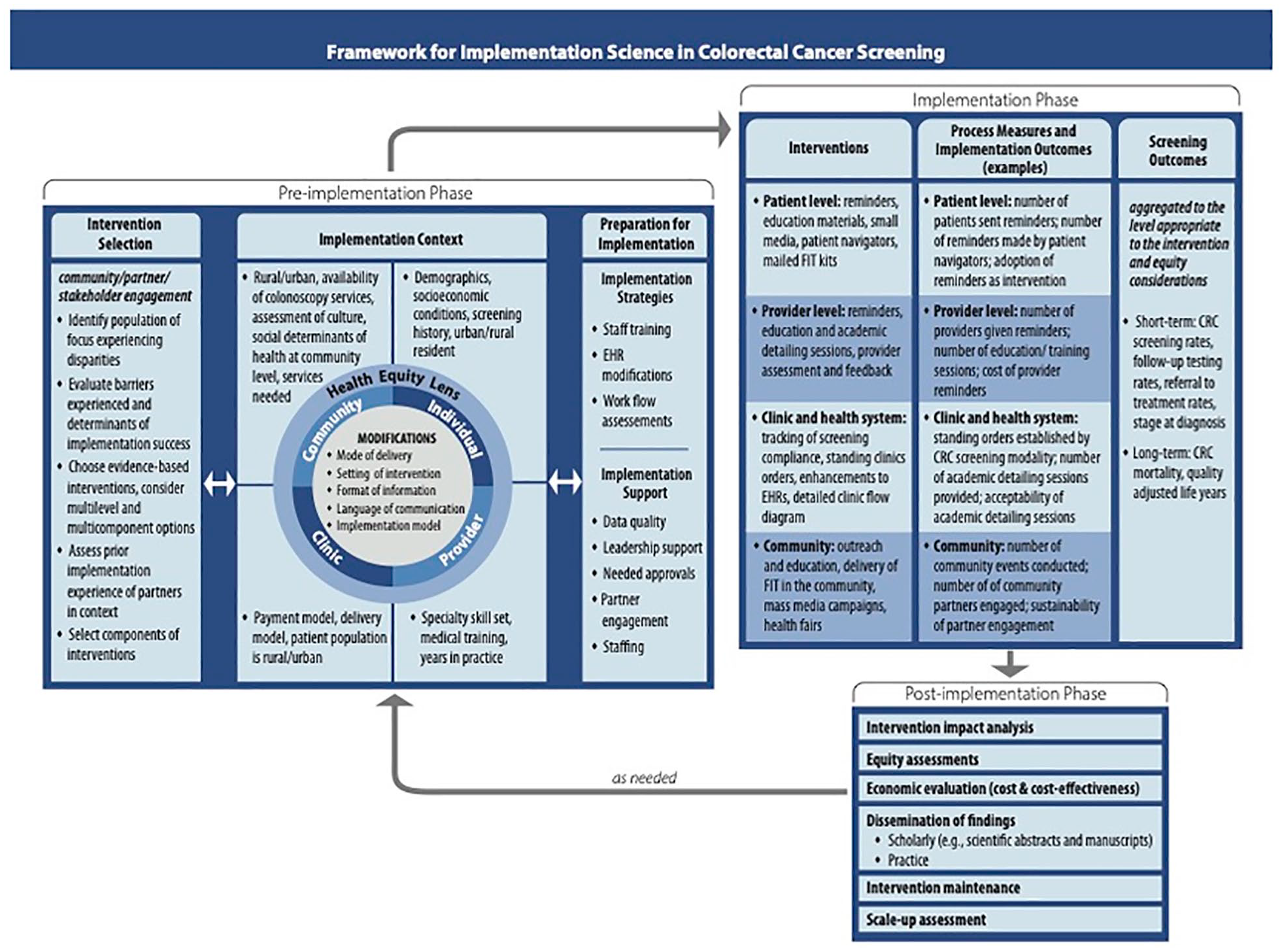
ACCSIS Framework.
The preimplementation phase begins with intervention selection, which should be made in conjunction with community and other partners. Community partner engagement is essential to ensure cultural sensitivity and appropriateness of the intervention to promote screening for all. The steps to choosing an intervention include identifying the population of focus; considering interventions that are evidence-based and often are multilevel and multicomponent; assessing prior experience with the intervention(s); and selecting which components to test. The ACCSIS Research Projects could choose evidence-based interventions from The Community Guide to Preventive Services (https://www.thecommunityguide.org/; Community Preventive Services Task Force, 2016) or NCI’s Evidence-Based Cancer Control Programs evidence-based interventions (https://ebccp.cancercontrol.cancer.gov/index.do). For example, clinic partners of one Research Project tested the following interventions after discussions with their clinic partners: patient and provider education; improvements to electronic health systems; and inclusion of CRC awareness at community events. As indicated by the double-headed arrow in Figure 1, intervention selection is influenced by the context and vice versa.
Once an intervention(s) is selected, modifications may occur at various levels (e.g., individual, provider, clinic, and community). Four distinct quadrants indicate opportunities for intervention adaptations. Contextual factors at the individual level may include socioeconomic factors and screening history; factors at the clinic level may include payment or delivery models. Examples of modifications that help guide intervention development (shown in Figure 1’s inner circle of implementation context) include mode of screening delivery, the setting of the interventions, and the format of the information. Factors within the implementation context and preparation for implementation are expected to affect each other, as shown by the double-headed arrow between the two elements. For example, a Research Project, having observed how a community health center promotes CRC screening, may decide to include colonoscopy as a screening mode after beginning the intervention with just stool-based tests. Furthermore, uninsured people often face cost barriers in obtaining colonoscopies and to ensure access, Research Projects may partner with endoscopy providers to offer free colonoscopies. Modifications such as these should be measured, to the extent possible, to understand their impact on process and screening outcomes.
Projects then continue to move through the framework toward preparation for implementation, considering which intervention elements require additional support. Interventions include staff training and capacity building, electronic health record modifications, and workflow assessments. Supports for implementing the interventions may include evaluation of data quality, engagement of leadership support, needed approvals (e.g., institutional review boards [IRBs], Tribal councils), partner engagements, and staffing. Arrows within the preimplementation phase, between intervention selection and implementation context, and between implementation context and preparation for implementation, are double-headed, indicating the iterative nature of this phase of the framework.
The implementation phase follows the preimplementation phase and is composed of interventions, process measures, and implementation and screening outcomes. The framework provides constructs and measures at each level and for each outcome. These constructs are not exhaustive; preferred interventions undertaken by the ACCSIS Research Projects are highlighted. Examples within the framework distinguish differences across the studies. Projects are expected to select multilevel and multicomponent interventions that occur at the patient, provider, clinic, health system, or community levels. Reminders and small media are examples of patient-level interventions; provider-level interventions include assessment and feedback and academic detailing sessions. Process measures and implementation outcomes can be measured at each of the four levels. For example, at the clinic and health system levels, process measures could include whether primary care providers’ standing orders were established for CRC screening and the number of academic detailing sessions provided. Implementation outcomes could include providers’ acceptance of academic detailing, feasibility of implementing academic detailing, and how well these sessions are attended. The reach of the interventions can be assessed based on population subgroup analysis to measure fair distribution.
Screening outcomes are the third element of the implementation phase. The framework describes short- and long-term screening outcomes. Short-term outcomes encompass CRC screening rates, follow-up testing rates, dates of referral to treatment, and stage at diagnosis; long-term outcomes include CRC mortality and quality-adjusted life years. Projects can report the short-term outcomes at the levels at which interventions occurred. For example, patient-level screening rates can be aggregated by provider to determine provider-level screening rates; all CRC follow-up testing rates for patients at a community health center can be aggregated to report that community health center’s follow-up testing rate. These outcomes can also be reported across the populations served, to assess who does and does not benefit from CRC screening.
The third phase of the framework is postimplementation. Transitioning to the postimplementation phase warrants an understanding of how to maintain progress, disseminate information, and consider scaling up successful components. This phase includes elements such as intervention impact analysis (e.g., changes in CRC screening due to the interventions) and moderation assessments (e.g., variation in CRC screening uptake due to the interventions for different communities and patient groups). Projects may also conduct economic evaluations during this phase and disseminate findings through local and national conferences and publications. In addition, local collaborators can maintain interventions during this phase and assess intervention (or program) scalability. As needed, projects can complete all phases of the framework and restart at the preimplementation phase.
Discussion
The ACCSIS framework, describing three phases of an iterative and continual process of improving cancer screening, with influences throughout and across levels, is intended to guide researchers and practitioners as they plan, test, and implement CRC screening projects. Members of the ACCSIS consortium led the development of the framework, with input from prior published models, literature on Community-based Participatory Research, and frequent feedback on feasibility and fit to the eight NCI-funded ACCSIS Research Projects. Members of the consortium also used their experiences in selecting and implementing interventions to guide the framework. On completion, the ACCSIS projects will offer evidence describing how multilevel interventions can be scaled up to reduce CRC disparities in the United States. The framework can help guide future trans-ACCSIS analyses and has implications for researchers and practitioners who design, conduct, and evaluate future initiatives.
This framework is innovative in several ways — perhaps most importantly in its explicit focus on the preparatory work needed to collaborate effectively with community and clinic partners, which is rarely tested as part of developing evidence-based interventions. Elevating this “pre-work” to a fully recognized intervention component supported with resources in the project budget and timeline is likely to increase the success of local collaborations. A second innovation is the extension of the multilevel focus beyond intervention targets to rigorous consideration at every step. From the foundational work all the way through to outcomes, constructs at each level can affect success; this framework highlights opportunities to consider those effects. Both of these innovations are seen as essential to achieving the goal of increasing CRC screening access for all. And both innovations suggest the framework can be used to address the larger goal of reducing inequities in the implementation of other cancer care beyond CRC and beyond screening.
Like the framework, the development process was iterative; data were brought into the process several times. These data ranged from a matrix of all planned consortium measures to feedback following each project’s test application of the framework and—later—feedback from two ongoing trans-ACCSIS analyses. Writing teams used this framework to guide development of trans-ACCSIS comparisons of patient navigation (Coronado et al., 2023) and mailed FIT programs; both projects used this framework to guide data collection and writing. The two writing projects benefited from the breadth and depth of the framework and produced two real-world pilot tests, which led to small changes to the framework. The framework is currently being used to conceptualize trans-ACCSIS comparisons related to intervention selection, adaptations, and implementation.
This process has produced a framework that can be adapted to future research and practice settings. Commonly, a Research Project is designed to test a static approach, during which opportunities for adaptation may be identified a priori and built into the analysis plan. In contrast, quality improvement programs and public health programs to improve health may expect and welcome change throughout program delivery. This framework aims to provide further guidance for research, practice, and practice-based research, and to advance prior work highlighting the important interfaces among quality improvement, testing interventions, and implementation processes. It intentionally allows for flexibility to enable intervention elements to be modified and adapted as new learning emerges from the field.
Using two dimensions to describe processes that occur at many levels—sometimes simultaneously—is a perpetual challenge with conceptual frameworks. This framework uses arrows to describe feedback loops, but the authors recognize that feedback can happen not only between phases, but within them. Similarly, the framework describes modifications happening only prior to the start of implementation, but the authors recognize that modifications may occur at other times, especially in practice rather than research settings. These limitations are accepted to avoid the confusion created by many overlapping arrows and to emphasize the importance of the phases, levels, and processes included here.
The framework that grew from the ACCSIS consortium describes a goal—for future CRC screening projects to be part of a continuous learning cycle, optimizing interventions and facilitating implementation, to increase CRC screening in populations experiencing a high burden from CRC. In the future, researchers and practitioners can use the ACCSIS framework to advance fairness in all modalities of CRC screening, including blood tests, and to improve other health conditions that have disparities in screening, diagnosis, and mortality.
Footnotes
Appendix A
Appendix B
Acknowledgements
The authors acknowledge the contributions of all collaborators in the ACCSIS consortium, including the many clinics, providers, and people who have and will participate.
Gloria D. Coronado, PhD
Mel and Enid Zuckerman College of Public Health
University of Arizona
Roy P. Drachman Hall
1295 N. Martin Avenue
Tucson, AZ 85719
Jesse Nodora, DrPH
University of California, San Diego
Moores UC San Diego Cancer Center
3855 Health Sciences Dr. #0901
La Jolla, CA 92093
Jessica Blanchard, PhD
Center for Applied Social Research
University of Oklahoma
5 PP, 201 Stephenson Pkwy, Suite 4100
Norman, OK 73019
Karen Kim, MD, MS
Penn State University College of Medicine
Hershey, PA 17033
Mark Dignan, PhD, MPH
University of Kentucky
Department of Internal Medicine
Healthy Kentucky Research Building
760 Press Avenue, Room 343
Lexington, KY 40536-0679
Melinda M. Davis, PhD, MCR
Oregon Rural Practice-based Research Network
Department of Family Medicine & School of Public Health
Oregon Health & Science University
3181 SW Sam Jackson Park Road, Mail Code L222
Portland, OR 97239
Peter Lance, MD, FRCP
University of Arizona
University of Arizona Cancer Center
1515 N. Campbell Avenue
Tucson, AZ 85724
Prajakta Adsul, MBBS, MPH, PhD
University of New Mexico Comprehensive Cancer Center and
Department of Internal Medicine
University of New Mexico Health Sciences Center
Albuquerque, NM 87131
List of abbreviations
ACCSIS Accelerating Colorectal Cancer Screening and Follow-up through Implementation Science
CBPR Community Based Participatory Research
CRC Colorectal cancer screening
FIT Fecal immunochemical tests
IRB Institutional review board
NCI National Cancer Institute
RP Research Project
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: From 2020 to 2023, Coronado has served as a Scientific Advisor to Exact Sciences, through a contract with Kaiser Permanente Center for Health Research (KP-CHR). Coronado also served as the PI (2022–2023) through a contact with KP-CHR on a study funded by Guardant Health that is testing the adherence to a blood test for CRC screening.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers UG3/UH3CA244298 (Oregon), UG3/UH3-CA233251 (North Carolina); UG3/ UH3CA233314 (San Diego); P30CA118100-16S4 (New Mexico); U24CA233218 (RTI); UH3CA233282 (Appalachia); P30CA225520-03S4 (Oklahoma), Chicago (UG3/UH3CA233229), Arizona (P30CA023074). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.