
Abstract
The COVID-19 pandemic uncovered important patterns of structural inequities and their impact on health outcomes for racial and ethnic minorities in the United States. Native Americans, Latinxs, and African Americans are more likely to contract COVID-19 and be hospitalized and die, but are less likely to be tested and vaccinated. Environmental and social vulnerabilities partially explain these disparate impacts while an underfunded and fragmented public health infrastructure accounts for the lag in the distribution of needed resources, including vaccines, at the national, tribal, state and local levels. To further understand the disparities of COVID-19 vaccine uptakes across diverse racial, ethnic and geographic populations, we draw from a socio-ecological model of community resilience and use a mixed-method community engagement approach that includes: digital community stories (N = 34), interviews with health providers (N = 14) and a multimodal quantitative survey (N = 1,194). Our results show that trust in one’s own community being resilient, community stories of cultural resilience and health provider use of resilience techniques increase vaccine uptake and supported self- and community care amid complex grief, traumatic events and personal and professional losses. Looking ahead, cultural, personal, and community resiliencies are key strategies for alleviating the stressors and losses experienced by racial and ethnic populations during pandemics.
Introduction
The COVID-19 pandemic uncovered important patterns of structural inequities and their impact on health outcomes for racial and ethnic minorities in the United States. Native Americans, Latinxs, and African Americans are more likely to contract COVID-19 and be hospitalized and die, but are less likely to be tested and vaccinated (Biel & Hamrah, 2021; KFF 2022; Kakol et al., 2021). Environmental and social vulnerabilities partially explain these disparate impacts (Nayak et al, 2020). Beyond this, however, is the crisis of a fragmented and underfunded public health infrastructure (Maani & Galea, 2020) that created a lag in the distribution of needed resources, including vaccines, at the national, tribal, state and local levels.
Research by grantees of the Community Engagement Alliance for Vaccine Equity (CEAL) initiative, funded by the National Institutes of Health (NIH), reveal that while racial and ethnic disparities influenced the individual decision to get vaccinated, larger structural factors like vaccine supply chain, access to vaccine clinics in underserved geographic areas (Cacari-Stone et al., 2021; Fehr, 2020), digital inequalities and the “infodemic” created by a lack of language and health literacy (Njoku et al., 2021; Webb Hooper et al., 2021), are the more likely reasons for lack of vaccine uptake. The public health system was further weakened by burnout and turnover of health care workers who provided emergency and critical health services to millions of affected Americans during the pandemic (Stone et al., 2021).
To address these public health challenges, an academic–community research partnership WEAVE New Mexico (Wide Engagement for Assessing Vaccine Equity) in collaboration with the Transdisciplinary Research, Equity and Engagement Center, Center for Native American Health, Center for Participatory Research and Clinical and Translational Science Center, examined the community and systems resiliencies and structural challenges of the pandemic among racial, ethnic and geographically under-resourced populations across the state. The key populations in this study reside in New Mexico: Latinxs living in rural and urban border areas; rural and other American Indians; African Americans; and those living unsheltered in Albuquerque. Using a community-based participatory research (CBPR) approach, we employed a mixed-methods study to assess dimensions of community resilience that may explain COVID-19 vaccine uptake across diverse racial, ethnic, and geographic populations in New Mexico.
Conceptual Model: Social Ecology of Community Resilience
The conceptual framework informing our research draws from a social-ecological model that examines multiple and interconnected influences of personal and interpersonal systems and environmental resilience (or “community resilience”) that influence vaccine equity. Community resilience refers to a community’s capacity to withstand, adapt to, and recover from adversity, while maintaining and improving population health and well-being (Plough et al., 2013). This concept encompasses the social, economic, environmental, and cultural systems that enable communities to respond to crises such as natural disasters, pandemics, and systemic inequities. A widely accepted definition emphasizes the ability of a community to use its resources to respond to, withstand, and recover from adverse situations, particularly by strengthening social networks, ensuring access to health services, and addressing the social determinants of health (Norris et al., 2008). Community resilience also includes equity, participation, and empowerment as central elements, recognizing that historically marginalized groups often face disproportionate impacts and must be centered in resilience-building efforts (Patel et al., 2017).
Community resilience has important implications for public health COVID-19 responses, vaccine equity and long-term systems change and population recovery efforts. Resilience is a useful concept for drawing our attention to the ability of Black, Indigenous, and Latinx communities and the health care workers serving them adapt to the stressors of pre-existing structural inequities coupled with the impact of the COVID-19 pandemic.
For our study, we consider critiques by social scientists who question the unidimensional notion of resilience that emphasizes an individual’s ability trel cope with structural racism and other grave inequities (Sims-Schouten & Gilbert, 2022). We also recognize the lack of uniformity in defining community resilience and the debates on whether a unidimensional concept imposes more burden on already taxed minority populations. Thus, we draw from the extant literature that considers resilience as the outcome of dynamic interconnected systems, relationships and processes (Fleming & Ledogar, 2008).
From a socio-ecologic perspective, the cultivation of community resilience at the individual, organizational, and national levels calls for engaging in health protective behaviors, emotional resilience, enhanced organizational support and community social capital while enhancing solidarity and building trust and leadership (Masten, 2015; Saghin et al., 2022; Zhang et al., 2022). A systematic literature review of community resilience during public health emergencies and natural disasters identified nine core elements across resilient communities: (a) local knowledge; (b) community networks and relationships; (c) communication; (d) health; (e) governance and leadership; (f) resources; (g) economic investment; (h) preparedness; and (i) mental outlook (Patel et al., 2017).
Drawing from this literature, we developed a model, Social Ecology of Community Resilience as it relates to COVID-19 Vaccine Equity (Figure 1). Although not conclusive or extensive, this model offers a holistic approach to community resilience (Haldane et al., 2021; Rela et al., 2022). Stress and adversity can be resisted or mitigated, and it may also elicit restorative responses. These occur at interconnected levels of individual, family, community and larger social systems. In Figure 1, resilience as it relates to vaccine equity begins with one’s personal confidence in the safety and efficacy of the COVID-19 vaccine, and then is reflected in the strength of family relationships and social networks. Next, communication and knowledge about COVID-19 and vaccines help determine how communities respond. Then, access to social and health resources facilitates resilience or exacerbates vulnerabilities. Finally, trust in government and confidence in leadership influences decision-making and actions regarding COVID-19 vaccines.
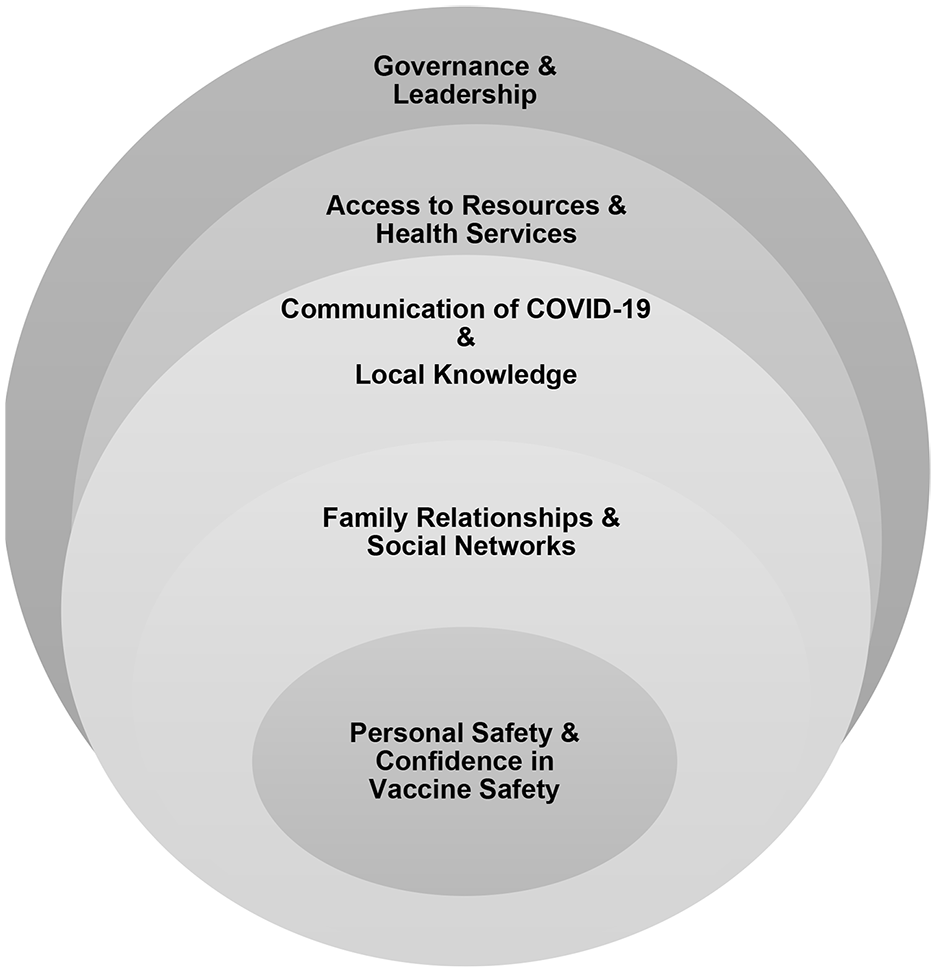
Social Ecology of Community Resilience as It Relates to COVID-19 Vaccine Equity.
Methods
The WEAVE NM academic and community partners, who have decades-long relationships, employed a CBPR approach to assess the social ecology of vaccine equity across diverse racial, ethnic, and geographic populations in New Mexico CBPR has established itself as a valued research approach that has proven effective in reducing inequities through multilevel interventions, systems change, and policy solutions (Cacari-Stone et al., 2014; Israel et al., 2012; Minkler et al., 2012; Wallerstein et al., 2018). Our core research team included community and academic partners. Four centers at the University of New Mexico collaborated to provide scientific institutional infrastructure and team science (Transdisciplinary Research, Equity and Engagement Center, Center for Native American Health, Center for Participatory Research and the Clinical Translational Science Center). Community partners included First Nations Community HealthSource, Cultivating Communities, the National Latino Behavioral Health Association, the Diné Centered Evaluation and Engagement Collaborative, the New Mexico Black Leadership Council, and the Pacific Institute for Research and Evaluation. This study was reviewed and approved by the UNM Human Research Review Committee (HRRC# 21-371).
Design
We employed a convergent parallel mixed-methods study design (Edmonds & Kennedy, 2017) that involves the simultaneous collection of qualitative and quantitative data, followed by combining and comparing these multiple data sources. We used data triangulation involving surveys, qualitative interviews and digital stories to analyze community resilience and its potential to increase COVID-19 vaccine uptake across diverse communities. Triangulation in research refers to the use of multiple methods, data sources, investigators, or theoretical perspectives to study a single phenomenon. The purpose of triangulation is to enhance the credibility, validity, and depth of understanding by cross-verifying findings from different angles. It is commonly used in both qualitative and mixed-methods research to reduce bias and ensure a more comprehensive view of the research question (Denzin, 1978).
Data Collection
The WEAVE NM academic and community partners partnered to develop data collection methods and instruments.
Recruitment and Consent
From 2021 to 2022, participant recruitment was conducted through the expansive networks of the TREE Center 2.0 team, leveraging long-standing relationships with community-based organizations and leaders. These connections were particularly vital during the COVID-19 pandemic when social distancing protocols limited in-person interaction. Recruitment efforts were led by trusted community partners who were not only collaborators but also co-investigators on the study. Their established credibility and cultural alignment with target populations were essential in fostering trust and encouraging participation among diverse and often underrepresented communities.
Potential participants were approached through multiple communication channels tailored to each community’s preferences and accessibility. These included face-to-face conversations (when safe and permitted), phone calls, email outreach, and virtual meetings via platforms like Zoom. This multimodal approach ensured inclusivity and minimized technological or logistical barriers to participation.
Informed consent was a cornerstone of the ethical framework guiding the study. All participants provided consent in accordance with the preferred method of data collection and in formats appropriate to their community context (e.g., oral or written). Consent materials were reviewed in plain language and often translated into the participant’s primary language to ensure full understanding. Community partners played an active role in explaining study procedures and answering questions to reinforce clarity and transparency.
Participants were compensated for their time and contributions with merchandise gift cards. Compensation varied based on the activity—such as completing surveys, participating in interviews, or contributing to the creation of digital stories—and was calibrated to reflect the time and effort required by each engagement method. This approach not only recognized the value of participants’ input but also promoted equitable participation across diverse socio-economic backgrounds.
Survey
We compiled an 80-item Core Survey using the robust methodology developed by scientist with the NIH CEAL (2021). The research team, including community partners, selected and adapted questions to include cultural and linguistic relevance for statewide and site-specific use. The WEAVE NM research team, including community partners, selected, and adapted NIH’s questions to include cultural and linguistic relevance for statewide and site-specific use. As part of our broader community engagement strategy, the survey research team included place-based partners from McKinley County, the US/México borderlands, the Albuquerque metro area (First Nations Community HealthSource and the New Mexico Black Leadership Council), and the Navajo Nation, deploying the survey, successively, in paper-based, online, and oral interview forms from November 8, 2021 to June 28, 2022. All survey modalities were available in both English and Spanish and oral surveys were also conducted in Diné. New Mexico residents were eligible to participate if they were at least 18 years of age and did not live in the same household as a previous survey participant. Participants received a monetary incentive via electronic cards for taking the survey. COVID-19-related survey items included measures of trust, misinformation-related vaccine hesitancy, vaccination motivations, experiences of major challenges in health care and resource availability and vaccination status (NIH CEAL, 2021). Group-level measures from political science surveys (Frasure et al., 2016, 2020) included collective community efficacy (people like me can have positive local impact) and group consciousness specific to primary identified racial or ethnic group (importance of group to identity and feelings of closeness to group) as well as an adaptation of the “triumph in the face of adversity” subscale (e.g., even when my people face challenges, they get up and try again) of racial resilience (Slaughter, 2021). In addition, as shown, in part, in Table 1, we in-cluded multiple socio-demographic items.
Selected Demographics of Survey Participants, NM, 2021–2022.
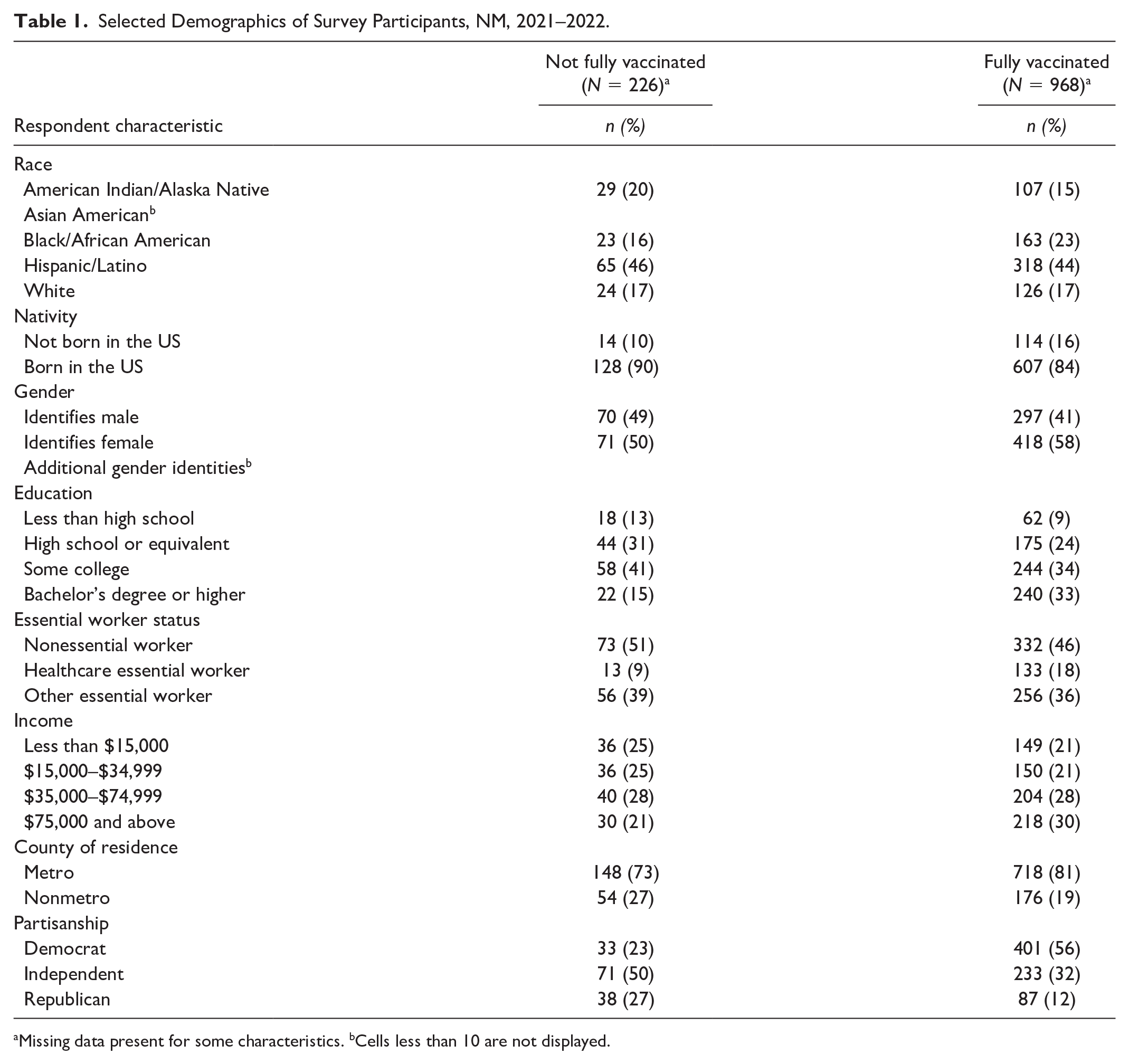
Missing data present for some characteristics. bCells less than 10 are not displayed.
Qualitative Interviews
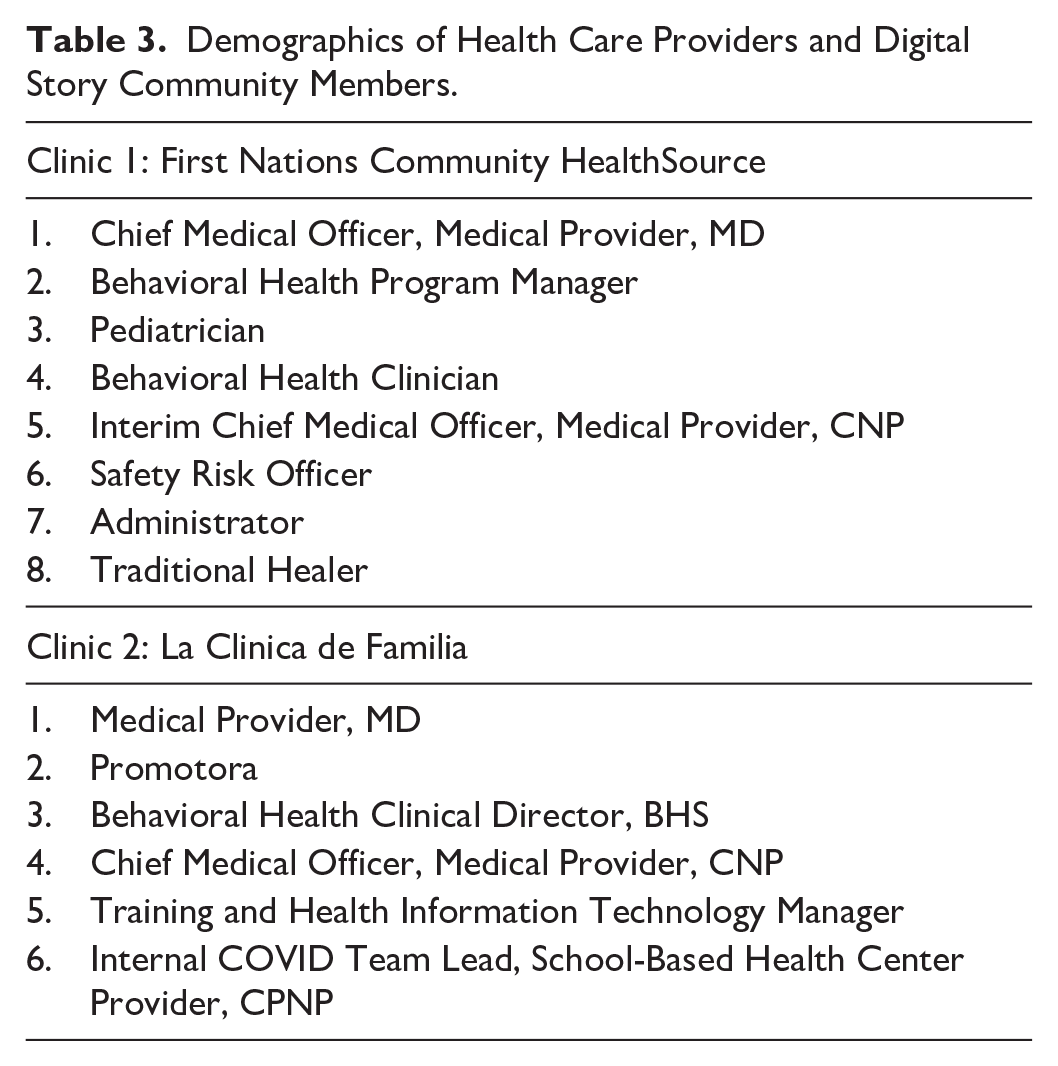
Individual interviews occurred through partnerships with two Federally Qualified Health Centers (FQHC). First Nations Community HealthSource serves American Indian/Alaskan Native families and underserved populations in and around Albuquerque area. La Clinica de Familia is based in southern New Mexico and serves patients throughout the southern and rural borderlands, including Hispanic/Latinx migrants. Leadership at each FQHC invited providers and clinical staff to participate, with the goal of achieving maximum variation across provider and staff role types. Each site could recruit up to eight participants. Interviews lasted between 15 and 60 minutes, conducted via Zoom by a primary interviewer who asked questions and a secondary interviewer who took notes and asked follow-up questions at the end. Participants received $50 compensation.
We developed the interview guide with community advisory input. It started with a narrative question,
This conversation is to tell your story of the pandemic; in particular, thinking about your work in the clinic and how the pandemic has affected you. To start, I’d like to hear your whole story in your own words and in whatever order feels most comfortable for you.
This was followed by semistructured questions that inquired about how their clinic worked to provide vaccine access and adapted to new protocols or ways of operating. They were also asked how trust influenced vaccination in their community and who they trusted for vaccine information. Finally, they were asked what helped their community get through the pandemic, and—looking to the future—what recommendations they had about responding to similar situations in the future. We did not collect demographics for this sample of participants, as our goal was to obtain maximum variation of health care profession within each clinic.
Digital Stories
We conducted a 3-day digital storytelling training for community members, with ongoing technical assistance provided by a team from Healthy Native Communities Partnership, Inc. Each participant created a 5-minute film that reflected personal accounts of their and their communities’ experiences during the COVID-19 pandemic (Lambert et al., 2018). Participants also completed a simple demographic questionnaire that asked for gender, race, ethnicity, and living situation [rural/urban/unhoused].
The digital storytelling workshop participants included American Indian/Alaskan Native, Latinx, African American, and LGBTQ populations living in rural and urban settings. The digital storytelling workshops were open to all genders and adults 18 years and older. The digital storytelling workshops were held virtually and in-person. We worked with the Consortium partners in the Tri-Chapter, Albuquerque, Las Cruces and New Mexico-Mexico border regions to assist with recruitment for the digital story workshops. Consortium partners participated in community human research protection training and were approved by our institutional Review Board (IRB) as co-investigators. They then assisted with recruitment via community flyers that were culturally aligned with each of the diverse communities and were co-developed with the Consortium partners once dates and locations for the workshops were organized. Consortium partner leads also reached out to individuals by email, phone, or in-person to describe the study and invite them to join.
The informed consent process includes reviewing the informed consent cover letter and time for the potential participant to ask questions. If the individual agreed to join the study, the UNM team member helped them prepare for the workshop by providing directions to the workshop location, assessing the participant’s comfort and skill level with using a computer and the internet, determining the participant’s technical support and equipment needs, and conducting a hands-on demonstration of the websites and tools to be used for the workshop.
Data Analysis
Quantitative Analysis of Survey Responses
We calculated descriptive statistics for strictly categorical variables and used mean and standard deviation for interval-level variables. Ordinal items with four or more conceptually equivalent spaced response options (e.g., extent and agreement scales) were treated as interval-level for analysis. To highlight contrasts, we dichotomized remaining ordinal predictors of interest as highest response option, versus others. We calculated scale scores as the mean across nonmissing items and linearly rescaled them to range from one to four in increasing sense to ease comparison. Internal consistency of items within scales was assessed using Cronbach’s alpha.
In our survey analysis, we used multiple statistical tests to explore our research question of which included survey measures linked to community resilience (our predictors of interest) would be most strongly associated with vaccine uptake (our outcome of interest), hypothesizing that all included measures would, individually, statistically significantly increase vaccine uptake and, moreover, that “inner” measures directly asking about individual-level constructs would, in bivariate associations, show relatively greater effect size associations with vaccine uptake than more distal measures invoking group-level constructs. Accordingly, characteristics of fully vaccinated survey respondents versus others were compared using independent sample t-tests for interval-level variables and chi-square tests of independence for dichotomous variables. Cohen’s d (“small,” “medium,” “large”: .2, .5, and .8) and Cramér’s V (.1, .3, .5) were used, respectively, as effect size measures with t-tests and chi-square tests, and p < .05 was the predetermined threshold for statistical significance. Stata 17.0 was used for all statistical analyses (StataCorp., 2023).
Qualitative Analysis of Interviews
Interviews were transcribed by a professional transcription company and then imported into NVivo 12 (QSR International Pty Ltd, 2018). Working as a team, two analysts created a preliminary code book based on interview questions and the first transcripts. The codebook was refined through an iterative process with subsequent application to new transcripts. Throughout, the primary analysts met with other members of the coding team for input on coding and further refinement of the codebook. We then used the theoretical framework specific to community resilience to query our existing coding structure and extract representative quotes that exemplified these constructs.
Qualitative Analysis of Digital Stories
We downloaded transcripts of the digital stories, including symbols and visual images, into a Word document to complement the online digital versions for data analysis. Similar to our analysis of the interviews, the qualitative analysis had researchers identify themes, build codebooks, mark texts and apply a mapping of the social ecological model of community resilience (Ryan & Bernard, 2000; Green & Thorogood, 2013). Two team members independently coded all transcripts based on the preliminary codebook. Team members then adopted thematic content analysis in an iterative process (Green & Thorogood, 2023). We discussed and reconciled coding differences. Relevant quotes were grouped together, allowing team members to develop interpretive notes (Saldaña, 2013) for an understanding of the community resilience dimensions and potential new themes or unique outliers. We also queried the codes related to theoretical framework constructs and pulled out representative quotes.
To identify key themes across both the interview data and digital stories, we first conducted a systematic coding process drawing from our Social Ecology of Community Resilience conceptual model described above. We transcribed all data, then independently and collaboratively reviewed the texts to identify recurring concepts. Through iterative coding cycles and memo writing, we developed a codebook, refined categories, and grouped similar codes into overarching themes. Triangulation across both data sources ensured consistency and enhanced the depth and validity of the thematic findings.
Results
Quantitative Community Survey
Across populations, measures linked to community resilience at multiple levels were positive predictors of vaccine uptake. Of the 1,215 survey participants, 1,194 had nonmissing vaccination status data and were included in analysis. As shown in Table 1, a vast majority of participants (81%) reported being fully vaccinated against COVID-19, having received either two doses of a two-dose vaccine or a single dose of a single-dose vaccine. Descriptive statistics indicate higher proportions of survey participants self-reporting as members of racial or ethnic minority groups than in the general New Mexico population, especially from African American communities, consistent with our study design and community-driven sampling strategy. Participants reporting higher levels of education and Democratic party partisanship were more likely to also report being fully vaccinated.
As shown in Table 2, COVID-related measures showed large effect size associations with vaccination status that were statistically significant, with fully vaccinated participants reporting: (a) higher levels of vaccine trust and confidence; (b) lower levels of vaccine hesitancy attributable to misinformation; (c) higher levels of motivation to enhance their personal, family and community safety through vaccination; and (d) lower health care and resource availability challenges than not fully vaccinated participants. At the local level of our adapted socio-ecologic model (Figure 1), perceived collective community efficacy was statistically significantly higher (d = 0.42, p = .002) in fully vaccinated participants than in those who were not fully vaccinated. In addition, perceived commonality with primary racial or ethnic group (d = 0.29, p = .01) and primary racial or ethnic group perceived resilience to adversity (d = 0.23, p = .03) showed a small effect size, with positive associations with full vaccination status. Categorical measures of trust in COVID-19-related information provided at community and government levels also showed a small effect size, with statistically significant and positive associations with vaccine uptake. Notably, despite reporting generally low levels of trust in information, fully vaccinated individuals still reported strong motivations to enhance safety at multiple levels.
Predictors of Vaccine Uptake, NM, 2021–2022.
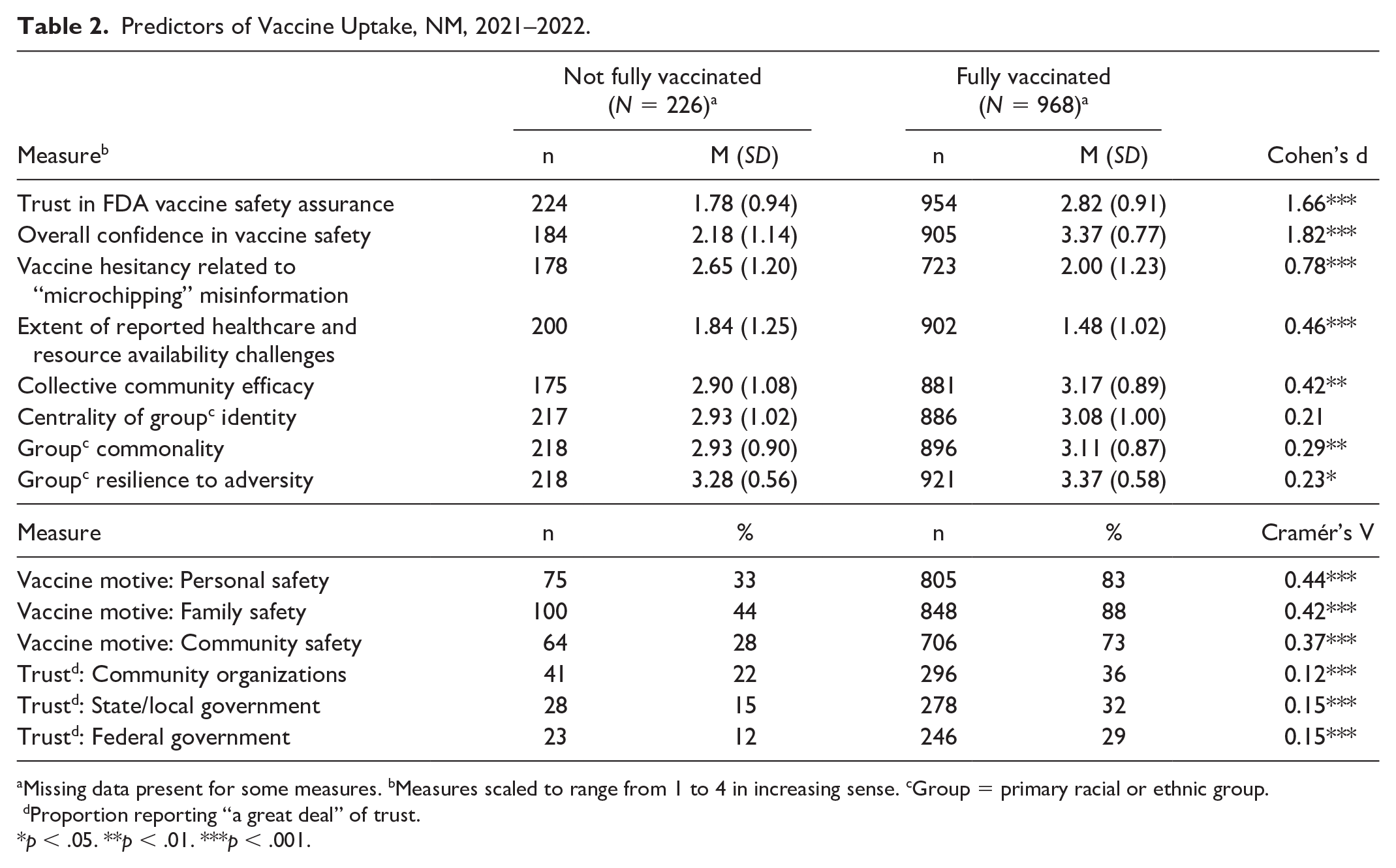
Missing data present for some measures. bMeasures scaled to range from 1 to 4 in increasing sense. cGroup = primary racial or ethnic group. dProportion reporting “a great deal” of trust.
p < .05. **p < .01. ***p < .001.
Qualitative Results
Fourteen health care professionals participated in qualitative interviews. Of these, 8 (57%) were from First Nations Community HealthSource in the central region of the state, and 6 (43%) were from La Clinica de Familia in the southern region of the state. Participants represented a mix of health care providers and clinicians (Table 3).
Demographics of Health Care Providers and Digital Story Community Members.
A total of 34 digital stories were elaborated via consent to be included in the data analysis. A total of 30 participants further consented and agreed to allow their stories to be included into the study and uploaded to the project webpage (weavenm.org). All participants (n = 34, 100%) were adults (>18 years) and equally women (n = 17, 50%) and men (n = 17, 50%). Most were urban dwellers (n = 22, 65%); 8 (24%) were from rural areas and 4 (12%) were unsheltered (experiencing homelessness). All participants were from minoritized groups including Native American (50%), Latinx (29%), and African American (21%) individuals.
Five themes related to community resilience emerged from qualitative analysis of clinician interviews considered alongside digital stories content: (a) Trust in government; (b) Misinformation, communication and local knowledge; (c) Centrality of community and social relationships; (d) Access to resources (health care, social, economic); and (e) Confidence in vaccine and personal safety. Table 4 displays the themes and illustrative quotes from clinical and community perspectives.
Themes and Illustrative Quotes of Clinical and Community Perspectives From Qualitative Interviews and Digital Stories.
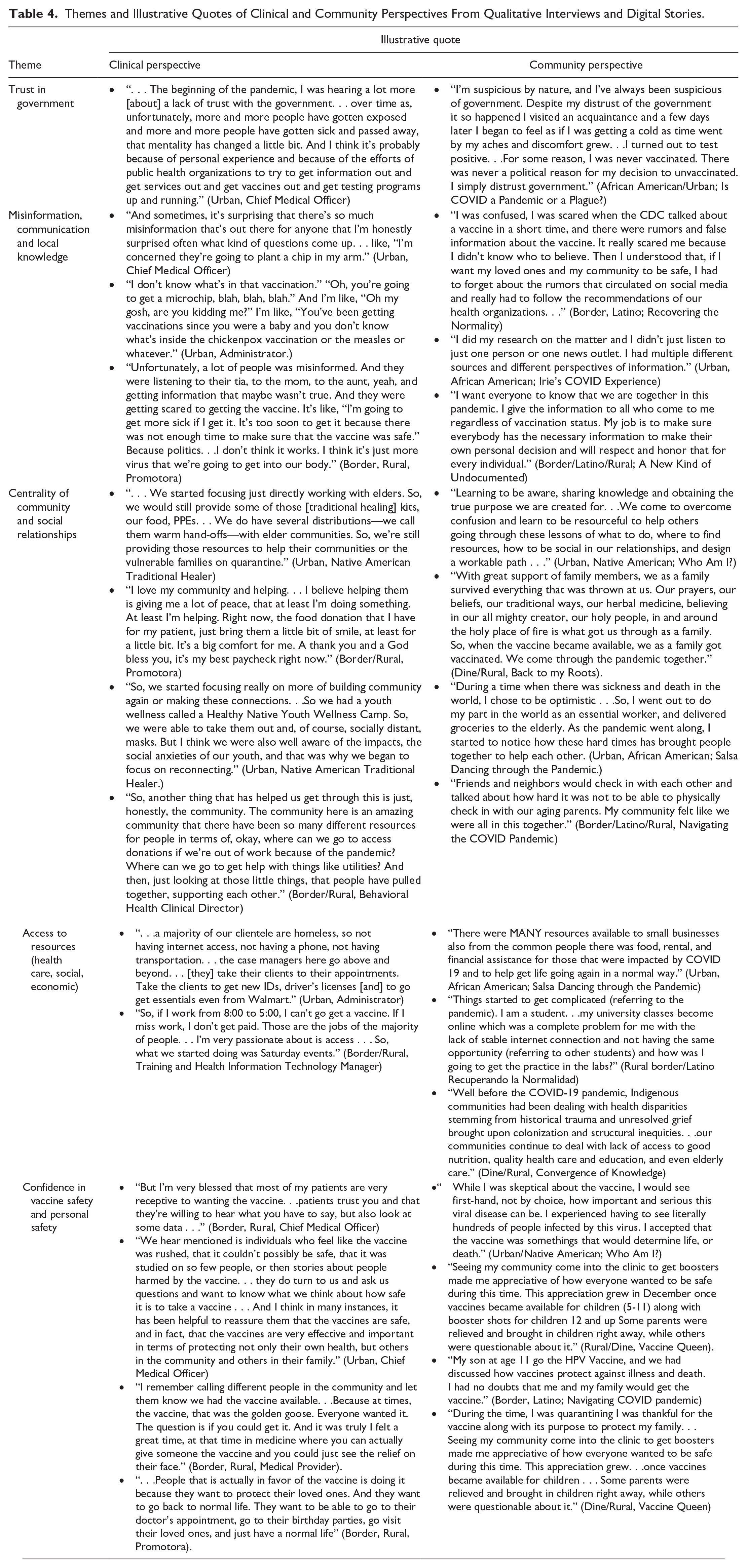
Trust in Government
Health care professionals and staff reported some patients did not trust the government and believed that clinics were government entities. However, some people became more trusting due to public health efforts to disseminate information and the vaccine itself. In the digital stories, a few community members expressed their distrust of government in general as their reason for not getting vaccinated, or shared their disappointment that their tribal government did not act quickly enough to put mandates into place.
Misinformation, Communication and Local Knowledge
Health care professionals were surprised at the amount of misinformation cited by their patients as the reason for their apprehension about the vaccine. Community members indicated they were confused and scared and had to sift through the (mis)information and decide who and what to believe. Health care professionals added that misinformation was often transmitted through family members, leading to heightened fears and suspicions about the vaccine. Some community members took matters in their own hands and said that they felt compelled to get the facts of COVID-19 out to others and in some instances did their own research.
Centrality of Community and Social Relationships
Clinicians and staff spoke about how they enjoyed helping community members (regardless of patient status) and how their clinic made a positive difference in their community. They were proud of the large number of vaccines they administered and how they helped to rebuild a sense of community. They also discussed how community members came together and helped one another by pooling resources like utilities, food and transportation. Across all 34 digital stories, family, community and social relationships were central to coping, finding a sense of belonging during a time of isolation and overcoming stressors during the pandemic. Indigenous community members further expanded from a holistic perspective, on the importance of interconnectedness and relationship.
Access to Resources
Both clinics worked to maintain and improve access to equitable health care for all patients during the pandemic. Because both clinics are FQHCs, they provided care to everyone, regardless of insurance, ability to pay or U.S. documentation. One clinic served many patients experiencing homelessness. It offered various outreach programs to provide patients with vaccines and deliver other health care. The other clinic served a high number of rural patients and migrants near the U.S.–Mexico border. Many of its providers and staff were fluent in Spanish and used a mobile unit to provide vaccines and health care. Similar, yet unique, perspectives were shared by community members, such as being able to access health care services, lack of internet access and trying to meet basic needs like food, clothing and shelter during the pandemic.
Confidence in Vaccine Safety and Personal Safety
Participants spoke about how many patients trusted the vaccine and wanted it to “go back to normal life.” However, some expressed concerns that the vaccine contained microchips. Others asserted that the pandemic was a hoax or voiced worries that the “vaccine was rushed” and not tested on enough people, and that it might make them sick. Among community participants, several related their confidence in the safety of the vaccine and its efficacy for protecting them and their loved ones.
Discussion
As part of our statewide academic–community partnership, we used a mixed-methods study to assess the dimensions of community resilience that might explain COVID-19 vaccine uptake across diverse racial, ethnic and geographic populations in New Mexico. Our survey results are similar to other studies, showing that fully vaccinated adults are more likely to have trust and confidence in the vaccine, their community and government and less likely to be hesitant due to misinformation (AuYoung et al., 2022). Similarly, health care providers and community members emphasized the link between trust in government and attitudes and decisions regarding the vaccine. “Government” is a broad term. It would be better to consider specific layers of government—local, state, tribal, and in some instances, binational—and their respective roles in the pandemic response. For example, the Diné community living on the Navajo Nation, off-reservation (urban) Native Americans, and those residing in border communities are impacted on a daily basis by multiple governments. Thus, they must navigate multiple mandates and sources of information and decide which to trust or listen to.
Transmission of information about the vaccine and COVID-19 through health care providers, online research results and sources like the Centers for Disease Control and Prevention dispelled some confusion caused by misinformation. As in other studies with communities of color (Ignacio et al., 2022), our survey results, interviews and digital stories underscored that personal motivations to get the vaccine were influenced by the desire to enhance safety for self, family and community. In some instances, people sought the guidance of trusted family and community members (i.e., community health workers and traditional knowledge holders). Our study aligns with other research in stressing the need to work with trusted confidants to disseminate public health information and resources about COVID-19 and vaccines, and support community forums to discuss and navigate various conflicting messages between Western and traditional medicine and community ways of knowing (Bastida et al., 2022).
As anticipated, our study found that unvaccinated and not fully vaccinated communities experienced more barriers to accessing health care services and other social resources. FQHCs, such as those in our study, are safety nets for the unhoused, urban Native Americans and African Americans, and border Latinx and undocumented immigrants. Community members expressed the need for basic life-supporting resources like food, housing and internet access.
Finally, our mixed data analysis emphasized the centrality of community, including neighborhood ties, a sense of belonging to one’s racial or ethnic group, valuing social and kinship ties and giving back to community. Health care professionals spoke about how they enjoyed helping community members and how their clinic made a positive difference in their community. Across all 34 digital stories, family, community and social relationships were central to coping, belonging during a time of isolation and overcoming stressors during the pandemic. Other emerging work on community resilience recognizes the interconnected dimensions that come together within cultural-relational networks, as well as the prominence of social capital (Epperson et al., 2022; Portes, 2000; Richardson, 2002).
Strengths and Limitations
Many studies examining the determinants of COVID-19 vaccine equity have employed either quantitative or qualitative data collection methods to determine the barriers to vaccine uptake. However, there are limitations to using only one approach. The strength of our study is that it was conducted with a consortium of academic and community partners who shared long-term, trusting relationships. This was particularly useful during the pandemic, when social distancing measures and closures created conditions where hard-to-reach communities became even more isolated (Harrison et al., 2022; Cacari Stone et al., 2023). While our long-standing academic–community partnership was a strength, it did entail certain study limitations. Convenience sampling allowed us to leverage relationships and continue enrolling diverse populations amid pandemic challenges over an 8-month period. However, our deeper ties in “harder to reach” communities and the overarching goal of NIH CEAL to include high concentrations of underserved minority communities led to a slight over-enrollment of these populations.
Implications for Policy and Practice
The concept of community resilience has important implications for COVID-19 public health responses, vaccine equity and long-term systems change and recovery efforts. First, when considering future actions, public health leaders must focus on the dynamic interconnected factors promoting community resilience for diverse communities. Rather than rely on the ability of communities of color who are heavily burdened by structural inequities, government and private sector investments must be recruited to strengthen the capacities of vulnerable and fragmented public health systems and sustain the health care workforce. This requires an equitable distribution of resources across all public health jurisdictions, including tribal, state and local agencies. CBPR “with” and “by” communities of color rather than “in” cultivates trusted relationships and enables the production of knowledge that reflects the epistemic advantage of those who are most burdened by pandemics and other structural determinants of health. Engagement with public health leaders and practitioners from diverse communities further accelerates the translation and dissemination of public health messages, increases opportunities for engagement in clinical trials and informs systems and policy change.
Footnotes
Acknowledgements
The authors would like to thank Carlos Linares, MD, MPH for his contributions to the literature review and research coordination. This work would not have been possible without the collective effort and collaboration of all the partners. We recognize and honor our community knowledge keepers, advocates, leaders, and researchers who have dedicated their talents to creating a new framework and forging new methods for findings solutions together.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was, in part funded by the National Institute of Minority Health and Health Disparities, the National Heart, Lung, and Blood Institute with the National Institutes of Health CEAL (grant nos. 5U54MD004811-10 and OT2HL158287). The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the NIH, affiliated academic institutions or organizations.
ORCID iDs
Supplement Note
This article is part of the Health Education & Behavior special issue, “Participatory Team Science in Action: The Transdisciplinary Research, Equity and Engagement Center of Excellence at UNM.” The printing and dissemination of the special issue was supported by the National Institute on Minority Health and Health Disparities with the National Institutes of Health (5U54MD004811-10). The views, findings and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the NIH, affiliated academic institutions or organizations. The entire supplement is available free-to-read at: ![]()