
Abstract
The Food and Drug Administration proposed “patient medication information” inserts for all medications, including the abortion drug Mifepristone. It is unclear how abortion attitudes or state policies affect how people evaluate such communications. Participants (n = 311) were randomized to view variants of the Mifepristone insert. Linear regression was used to assess abortion attitudes’ and policies’ relationships with comprehension and perceived evidence strength, safety, and effectiveness. Interaction terms were constructed to assess moderation of those relationships. Abortion policies were unrelated to comprehension, perceived evidence strength, or perceived effectiveness, but abortion bans at or before 6 weeks were associated with lower perceived safety. Attitudes were not associated with comprehension, but participants with positive attitudes rated the evidence as stronger and the drug as safer. Abortion attitudes moderated the effect of randomized group on perceived safety. The informational inserts communicate well across abortion policy environments (except perceived safety where abortion is banned at or before 6 weeks), yet negative abortion attitudes affected perceptions of evidence strength and drug safety.
Keywords
Introduction
Medication abortion is highly common, constituting 63% of all abortions in the United States, where approximately one in four women have an abortion in their lifetime (Jones, 2024; Jones & Friedrich-Karnik, 2024). Mifepristone, one of the two drugs used in medication abortion, is currently approved by the U.S. Food and Drug Administration (FDA) for pregnancy termination up to 10 weeks’ gestation (FDA, 2021). While medication abortion is highly effective and safe (Gatter et al., 2015), it was historically regulated by the Risk Evaluation and Mitigation Strategy (REMS), FDA requirements traditionally intended for certain medications with serious safety concerns (Cleland et al., 2021). The Mifepristone REMS included in-person dispensing, prescriber certification, prohibition against pharmacy dispensing, and a Patient Agreement Form (Grossman & Chung, 2025). The Patient Agreement Form (see Supplemental Appendix A) requires patients to sign a document indicating they understand the risks of Mifepristone, and studies have documented the form is confusing to potential users (Grossman & Chung, 2025). In 2023, the REMS were amended to eliminate in-person dispensing requirement and add a pharmacy certification option for retail pharmacies. Yet access has severely declined after the June 2022 Supreme Court decision in Dobbs v. Jackson Women’s Health overturned federal abortion protections enacted under Roe v. Wade (Guttmacher Institute, 2024). At the time of this study, 22 U.S. states had completely outlawed or severely restricted abortion (Guttmacher Institute, 2024). Stigma-related misinformation and disinformation about abortion were common even before Dobbs (Pagoto et al., 2023), but now are even more pervasive, including federal leaders who question Mifepristone’s safety (Smith-Schoenwalder, 2025).
To facilitate informed patient decision-making about prescription drugs, including Mifepristone (Federal Register, 2023), the FDA has proposed changing drug label regulation to include the provision of a 1-page summary of “patient medication information” (PMI) at the point of drug dispensing. Current drug labels include handouts created by pharmaceutical vendors (see Supplemental Appendix A), without intentional stakeholder engagement or consideration of decision science principles. The new FDA PMI template is a 1-page document with warnings about safety, common side effects, and directions for use. It was developed through extensive research and stakeholder engagement with consumers and consumer groups, industry, health care professional groups, physicians, pharmacists, and pharmacy organizations (Center for Drug Evaluation and Research, 2024). Given the rising use of medication abortion through telemedicine and substantial misinformation surrounding the drug’s safety, we chose Mifepristone as a case study. We compared the current vendor handout with the proposed FDA PMI template (see Supplemental Appendix A) and a variant of the FDA PMI we created (see Supplemental Appendix A) based on critical decision science principles that included information about benefits, risks, and mechanism of action (“Decision Critical Handout”; Krishnamurti et al., 2025). A recent systematic review of evidence-based design for PMI found that patient beliefs about the medication (i.e., perceived risk and perceived drug effectiveness) are optimized by providing details about side effects, addressing patient concerns, and explaining medication benefits (Russell et al., 2025). Our “Decision Critical Handout” was based on the new FDA PMI then revised by a small group of decision scientists, abortion researchers, and psychologists. Unlike the REMS-required Patient Agreement Form, the “Decision Critical Handout” includes information about effectiveness, safety, mechanism of action, and benefits of Mifepristone and does not require attestation from patients.
In the randomized controlled trial with 311 participants, we found the “Decision Critical Handout” was associated with better comprehension, greater perceived strength of the scientific evidence, greater perceived safety of Mifepristone, and greater perceived effectiveness of Mifepristone compared with the current vendor handout and the proposed FDA PMI template (Krishnamurti et al., 2025). Here, we conducted secondary data analyses, asking, “Do people comprehend and judge the strength of the evidence on Mifepristone as a function of their personal abortion attitude and their state’s abortion policy?”
Method
Randomized Controlled Trial Conditions
Data were collected in March 2024 as part of a prospective, three-arm randomized controlled trial testing three versions of the PMI for Mifepristone (see Krishnamurti et al., 2025). Participants assigned female at birth (n = 331) were recruited using the Prolific online research survey service. They were randomized to view (a) the current drug insert (“Default”), (b) the new “FDA PMI,” or (c) our “Decision Critical Handout.”
Outcomes: Comprehension and Perceived Strength of the Evidence
Primary outcomes (see Supplemental Appendix B) were comprehension of the information (number of correct answers, 0–7) as well as perceived strength of the evidence, perceived drug effectiveness, and perceived safety (all on 1–5 Likert-type scales).
Predictors: Abortion Attitudes and State-Level Abortion Policy
Abortion attitudes were measured by asking: “Which of the following best describes your feeling about the Supreme Court’s overturning of Roe v. Wade?” This measure was developed de novo by the research team to capture contemporary abortion attitudes with a single item in the post-Roe environment. Response choices were the following:
o 1—It is taking our country very much in the right direction
o 2—It is taking our country somewhat in the right direction
o 3—I feel neutral/I don’t know
o 4—It is taking our country somewhat in the wrong direction
o 5—It is taking our country very much in the wrong direction
In bivariate and multivariate analyses, this was dichotomized as positive attitudes (4, 5) vs. conservative attitudes (1, 2). Respondents who were neutral or unsure (3) were excluded, because this study was intended to compare people with established attitudes.
The abortion policies on gestational age limits in participants’ state were identified using their ZIP code and the Guttmacher Institute’s data on state abortion policies (Guttmacher Institute, 2024) as of March 3, 2024. Categories were “abortion severely restricted” (total ban, restricted to 18 weeks or less) or “abortion legal” (restrictions after 18 weeks, no restrictions). One state, Wisconsin, was still in legal flux (excluded from bivariate and multivariate analyses). We also conducted a sensitivity analysis using a modified variable of states with a “near total or total ban” (restricted at or before 6 weeks’ gestation) compared with other states.
Covariate
Given the potential for reading comprehension to influence understanding of the information presented in the Mifepristone handouts and the association between education and abortion attitudes, all multivariate models controlled for level of education. This was measured as a high school degree or less, technical school/some college, undergraduate college degree, or postgraduate degree.
Analyses
Using Stata v.18, we examined whether abortion attitudes and state abortion policies were related to participants’ comprehension or perceived evidence strength, drug safety, and drug effectiveness. We calculated descriptive statistics for age (mean, SD), gender (n, %), race/ethnicity (n, %), education level (n, %), distribution by geographical region (n, %), and distribution by state abortion policy (n, %). We calculated univariate statistics for predictors and outcomes. We then constructed linear regression models predicting comprehension and perceived evidence strength, safety, and effectiveness from abortion attitudes and state policies, controlling for randomized group and education:




To test whether those effects of randomized group differed across personal abortion attitudes or state abortion policy contexts, we constructed two interaction terms: one between study arm and abortion attitudes and one between study arm and state abortion policies. These terms were added separately to the linear regression models. Overall interaction significance was assessed using a postestimation Wald test:


Results
Sample Descriptives
Three hundred and eleven participants completed the surveys. Their mean age was 31.7 years (SD = 7.07; range = 18–45); 94% identified as female, while 4% identified as nonbinary, 1% as gender queer, and 1% preferred not to share their gender identity. The sample was diverse across race/ethnicity, socioeconomic status, and region of the country: 31% had a high school degree, 40% completed undergraduate, and 16% had a postgraduate degree; 65% identified as White, 20% as Black, 13% as Hispanic, 11% as Asian, and 13% as multiracial; and 40% lived in the South, 24% in the West, 21% in the Midwest, and 16% in the Northeast. The sample was well-distributed across states where abortion is banned or restricted to/before 18 weeks (40%) and states where abortion is still legal after 18 weeks (59%), with 1% of the sample in Wisconsin. 84% of participants stated that the Dobbs decision was very much or somewhat taking the country in a wrong direction (positive abortion attitudes), and 7% felt it was moving the country in very much or somewhat the right direction (conservative abortion attitudes). The remaining 9% felt neutrally or did not know.
State-Level Abortion Policies
In bivariate analyses, comprehension was similar in states with liberal and restrictive abortion policies (X̄ = 5.80 vs. 5.70, p = .412), as were ratings of evidence strength (X̄ = 3.94 vs. 3.94, p = .966) and drug effectiveness (X̄ = 4.33 vs. 4.30, p = .724). Perceived safety was higher where abortion is legal (X̄ = 3.97 vs. 3.70, p = .008). Controlling for education, study arm, and abortion attitudes in multivariate regression, state-level abortion policy was not associated with comprehension (b = 0.02, p = .836), perceived strength of the evidence (b = –0.03, p = .792), perceived safety (b = 0.19, p = .065), or perceived effectiveness (b = –0.04, p = .617; see Table 1). Sensitivity analyses using the alternative measure of abortion policy (states where abortion was banned at or before 6 weeks vs. other states) showed very similar results, except in the multivariate regression model (controlling for education, study arm, and abortion attitudes), where perceived safety was significantly higher in states where abortion was not banned at or before 6 weeks (b = 1.02, p < .001).
Regression Models of Mifepristone Comprehension and Perceived Strength of the Evidence, Safety, and Effectiveness by Personal Abortion Attitudes and State-Level Abortion Policy With Interaction Terms (Group and Abortion Attitudes, Group and State-Level Policy).
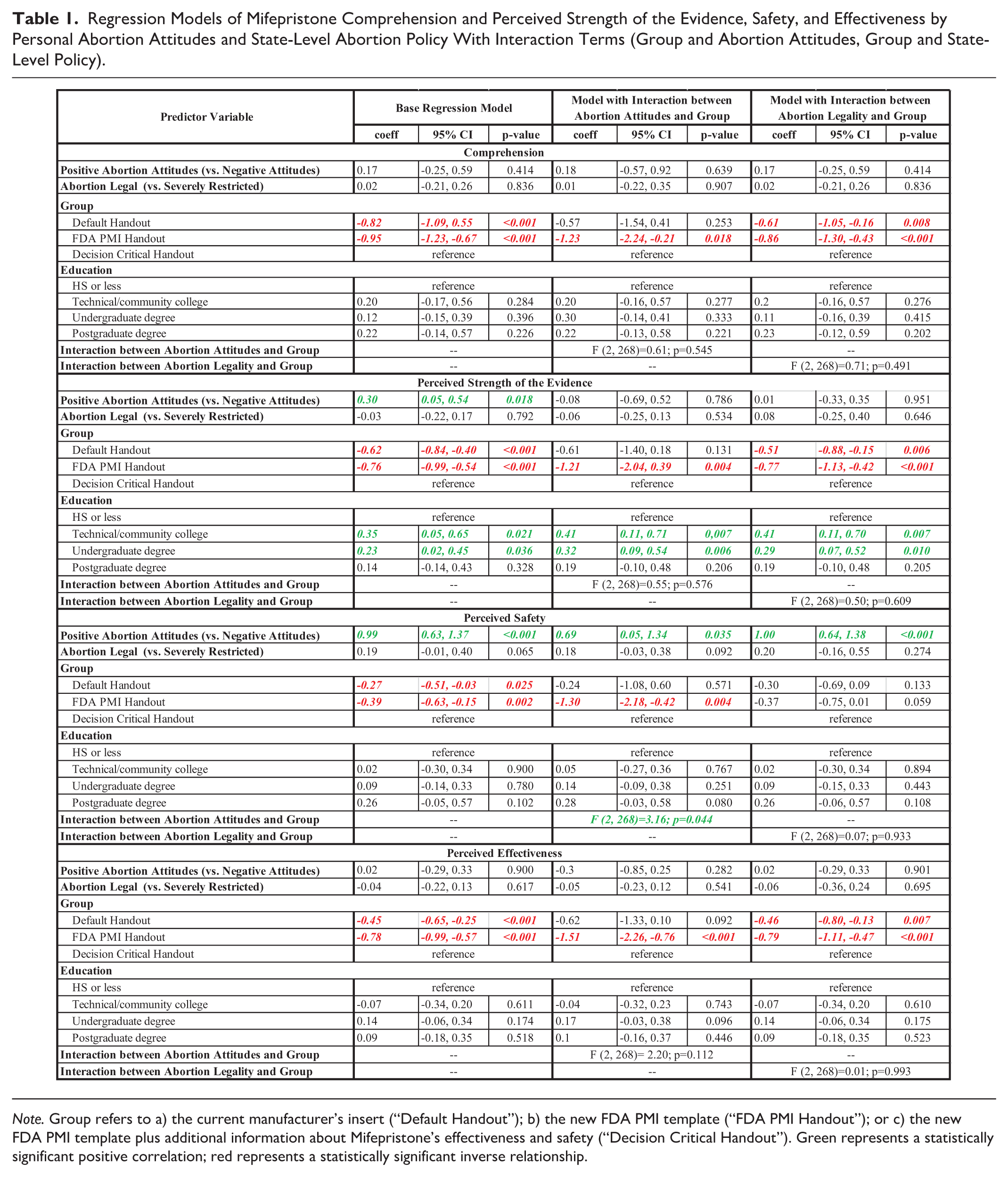
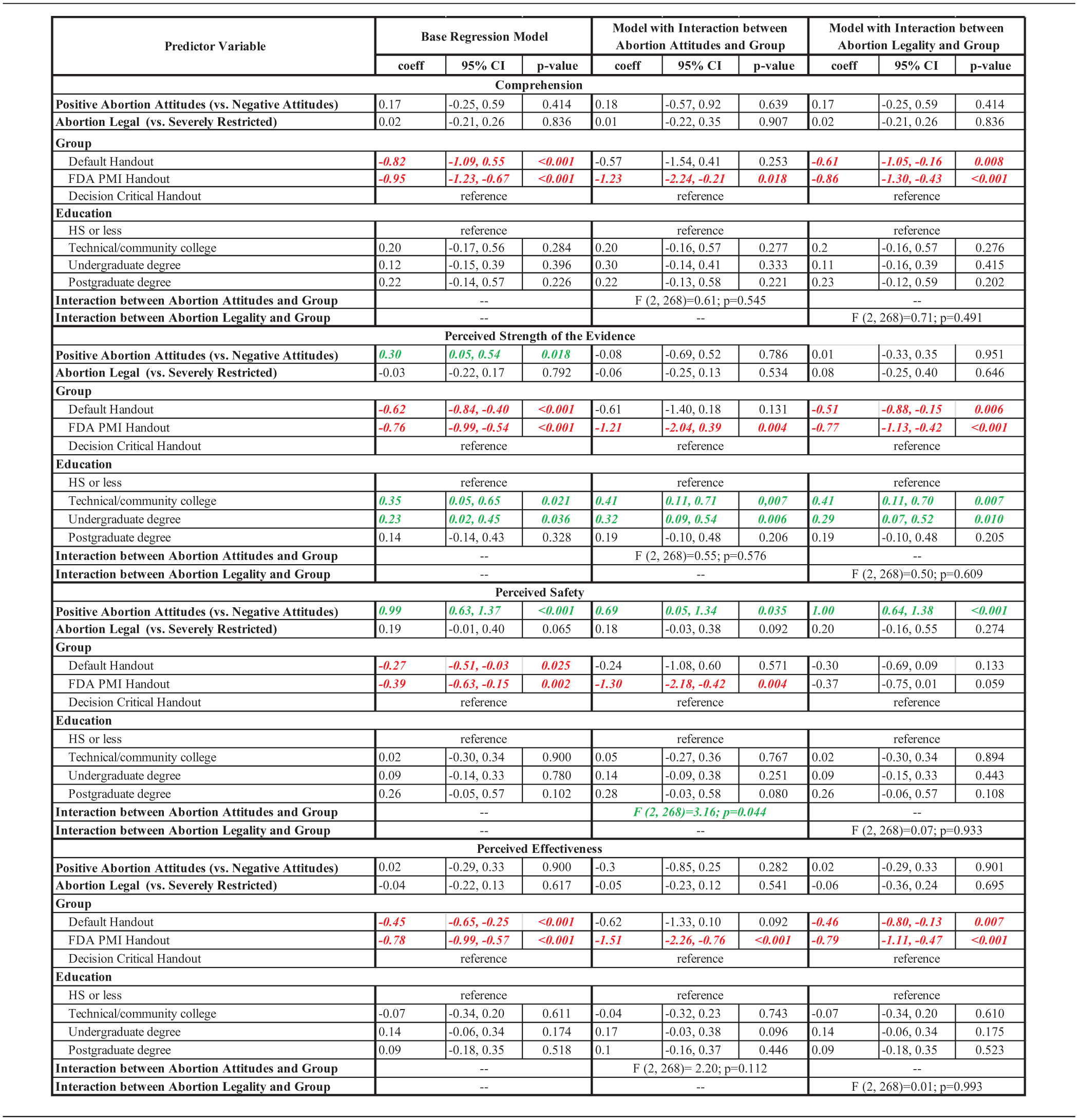
Note. Group refers to a) the current manufacturer’s insert (“Default Handout”); b) the new FDA PMI template (“FDA PMI Handout”); or c) the new FDA PMI template plus additional information about Mifepristone’s effectiveness and safety (“Decision Critical Handout”). Green represents a statistically significant positive correlation; red represents a statistically significant inverse relationship.
Abortion Attitudes
In bivariate analyses, abortion attitudes were unrelated to comprehension (X̄ = 5.81 vs. 5.59, p = .339) or perceived evidence of strength (X̄ = 4.00 vs. 3.91, p = .608). Participants with more positive abortion attitudes rated the drug as safer (X̄ = 3.98 vs. 2.95, p < .001) and more effective (X̄ = 4.37 vs. 4.08, p = .021). Controlling for education, study arm, and state abortion policy in multivariate regression, abortion attitudes were unrelated to comprehension (b = 0.17, p = .414) or perceived effectiveness (b = 0.02, p = .900; see Table 1). However, positive abortion attitudes were associated with an average of 0.30 points (p = .018) higher perceived strength of the evidence and an average of 1.0 points (p < .001) higher perceived safety.
Interactions Between Study Arm, Abortion Attitudes, and State Abortion Policy
Only one interaction effect was statistically significant (see Table 1): the effects of Mifepristone information received (randomized group) on perceived safety differed by abortion attitudes (F = 3.16, p = .044). When stratifying the regression models by abortion attitudes (see Table 2), there were no differences between randomized group for people with negative abortion attitudes (“Decision Critical”= ref; bDefault = –0.16, p = .767; bFDA PMI = –0.80, p = .232). Only among people with positive abortion attitudes, the “Decision Critical Handout” was associated with greater perceived safety compared with both the current drug insert (b = –0.28, p = .024) and the proposed FDA PMI (b = –0.32, p = .012).
Regression Models of Mifepristone Perceived Safety Stratified by Personal Abortion Attitudes and Predicted by State-Level Abortion Policy and Level of Education.
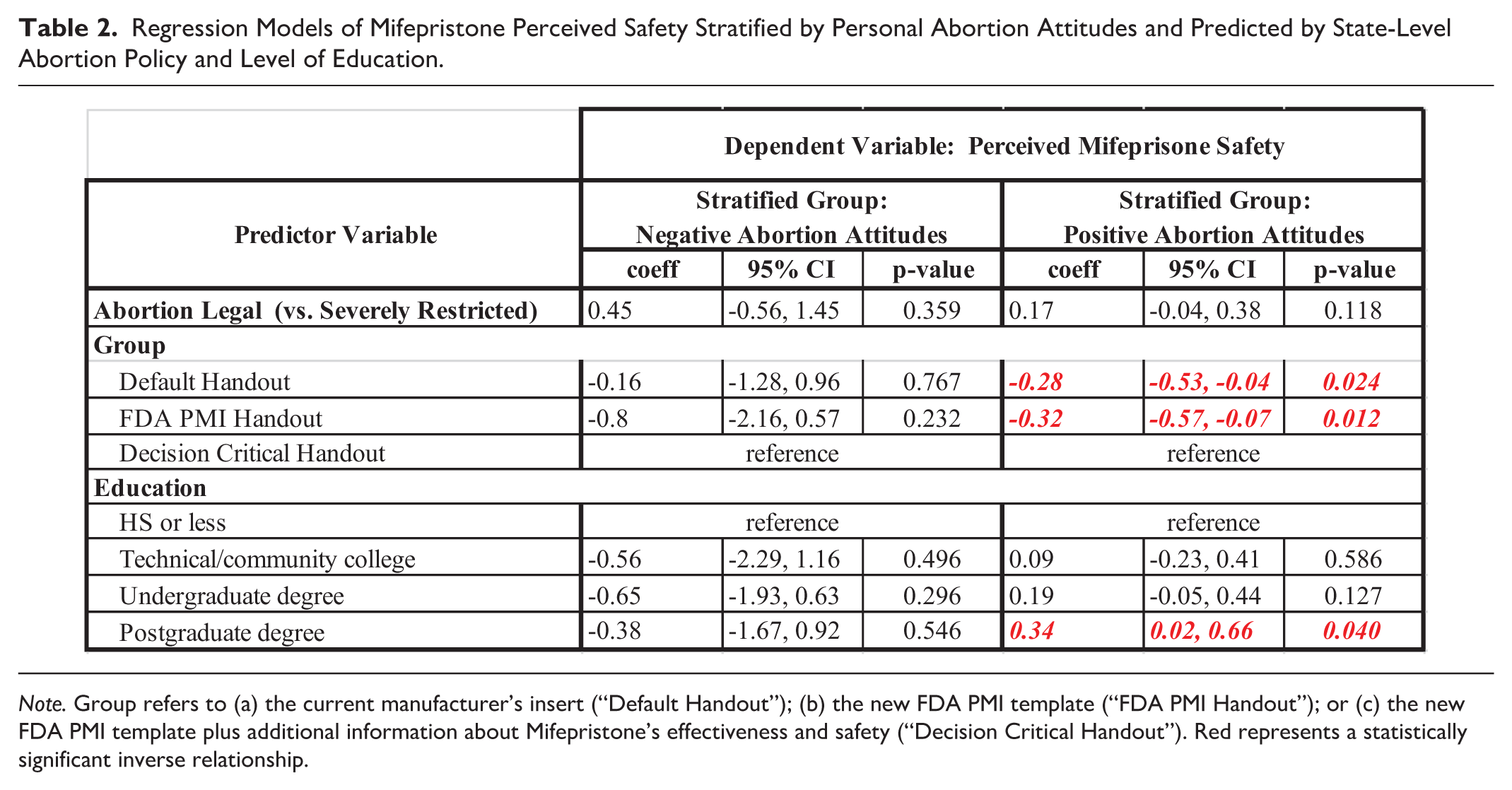
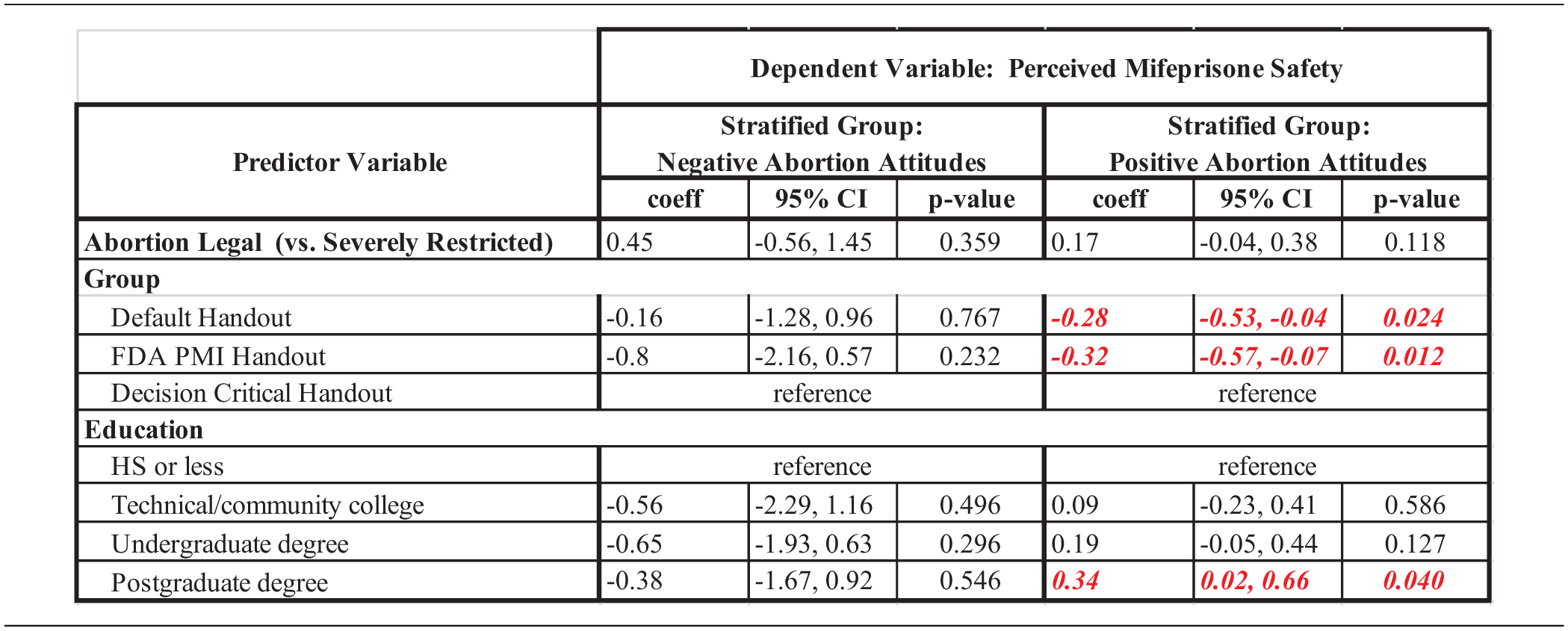
Note. Group refers to (a) the current manufacturer’s insert (“Default Handout”); (b) the new FDA PMI template (“FDA PMI Handout”); or (c) the new FDA PMI template plus additional information about Mifepristone’s effectiveness and safety (“Decision Critical Handout”). Red represents a statistically significant inverse relationship.
Discussion
While negative abortion attitudes were not associated with lower comprehension of the educational materials or perceived Mifepristone effectiveness, they were associated with lower perceived evidence strength and perceived safety. Comprehension and perceived evidence strength, safety, and effectiveness did not vary across state-level abortion policy contexts, except in states that banned abortion at or before 6 weeks’ gestation, where perceived safety was significantly lower. Previous research similarly demonstrates that people’s personal attitudes and emotional involvement toward a given topic can influence how they receive and interpret information about that topic (Fortner & Henk, 1990), including abortion. Less is known about the role of state-level abortion policy context on patients’ ability to comprehend and accurately perceive abortion-related information.
As previously demonstrated (Krishnamurti et al., 2025), our “Decision Critical Handout” (containing information about Mifepristone benefits, risks, and mechanism of action) better educates potential users and better conveys the strength of scientific evidence as compared with the current manufacturer pamphlet and proposed FDA PMI. This remained true regardless of the individual’s state-level abortion policy, except for perceived safety which was lower in states that banned abortion at or before 6 weeks’ gestation. However, the effects of randomized group differed between people with positive versus negative abortion attitudes. The “Decision Critical Handout” was associated with significantly greater perceived safety among people with positive abortion attitudes, but not among people with negative abortion attitudes. While designing patient medication information to clearly communicate risks and benefits allowed for universal improvements in comprehension, it appears that abortion attitudes (which some consider a sacred value) may affect individual thresholds on what constitutes an acceptable level of risk. In the face of any upcoming changes in the regulation and availability of Mifepristone in the coming months and years, it will be necessary to examine how the role of personal attitudes and values might affect the interpretation of established regulatory standards of safety and efficacy while simultaneously considering the additional resources and support that patients may need to make informed decisions.
Limitations and Strengths
The most significant study limitation was the use of secondary data from the original randomized controlled trial to address questions about abortion attitudes and state-level abortion policies. The data were not collected for this purpose but do provide exploratory results that can inform future research. The Prolific pool of respondents is not representative of the entire U.S. female population of reproductive age; however, our sample is heterogeneous and roughly representative of that target population. Notably, 84% of participants stated that the Dobbs decision was very much or somewhat taking the country in a wrong direction (positive abortion attitudes). This underrepresentation of negative views on abortion could have diminished our statistical power to detect meaningful differences. Respondents were being asked about Mifepristone, a medication they were not likely considering at the time of this study. It is possible that actual pregnant patients considering Mifepristone would have answered differently. There is possible historical confounding given that this study was being conducted as abortion was being outlawed in many states and while the Supreme Court was debating legality of Mifepristone. Regardless, that is also a strength because data were collected at an important time when information was highly politicized, visible, and rapidly changing.
Implications for Theory, Policy, and Practice
This study informs abortion policy research by demonstrating educational materials with information about drug risks, benefits, and mechanism of action are most effective for comprehension and assessing scientific evidence, regardless of abortion policy context. Our findings also support health education and behavior theories—including the Integrated Behavioral Model (Montano & Kasprzyk, 2015)—by demonstrating that individual-level abortion attitudes influence perceptions of the scientific evidence and perceived drug safety. Our results also inform health education practices by counselors and regulatory bodies including the FDA. The handout designed using decision science principles was the most effective for comprehension and evaluation of the scientific evidence across state-level abortion policy contexts. However, it is notable that patients with negative abortion attitudes had different interpretations of the degree of safety and strength of evidence than those with positive attitudes; suggesting that abortion attitudes may not be affected by the unbiased presentation of scientific information or that thresholds for risk may differ by personal attitudes toward abortion.
Supplemental Material
sj-docx-1-heb-10.1177_10901981251377723 – Supplemental material for Evaluating Information on Medication Abortion: Do Attitudes and State Policies Matter?
Supplemental material, sj-docx-1-heb-10.1177_10901981251377723 for Evaluating Information on Medication Abortion: Do Attitudes and State Policies Matter? by Elizabeth A. Mosley, Gianna White, Barry Dewitt and Tamar Krishnamurti in Health Education & Behavior
Supplemental Material
sj-docx-2-heb-10.1177_10901981251377723 – Supplemental material for Evaluating Information on Medication Abortion: Do Attitudes and State Policies Matter?
Supplemental material, sj-docx-2-heb-10.1177_10901981251377723 for Evaluating Information on Medication Abortion: Do Attitudes and State Policies Matter? by Elizabeth A. Mosley, Gianna White, Barry Dewitt and Tamar Krishnamurti in Health Education & Behavior
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.