
Abstract
The Food and Drug Administration (FDA) proposed to reduce nicotine in cigarettes to minimally addictive levels. To understand how individuals process messages about this policy, we conducted a content analysis of open-ended thought-listing responses to messages about very low nicotine cigarettes (VLNCs). Data were from a 2022 to 2023 randomized clinical trial with a probability sample of 1,901 U.S. adults. Participants viewed messages explaining that under a reduced nicotine policy, all cigarettes will have less nicotine but the same harmful chemicals as regular cigarettes. Afterward, participants were prompted to type in their thoughts. Responses were coded for cognitive reactions (pro-arguing, counter-arguing, message acceptance, message rejection) and emotional reactions (positive, negative). We assessed association between these coded reactions and message-related outcomes. In the sample of 944 coded responses, pro-arguing was most common (42.4%), followed by message acceptance (31.9%), message rejection (19.3%), negative emotions (15.8%), counter-arguing (12.4%), and positive emotions (1.2%). Among people who smoke, message acceptance was associated with higher quit intentions. Overall, pro-arguing and message acceptance were associated with higher support for nicotine reduction policy; counter-arguing and message rejection were associated with lower support (all ps < .01). Two weeks after exposure, participants who expressed negative emotions (OR = 2.58, 95% CI = 1.56, 4.26) were more likely to report having spoken with others about quitting smoking and people who expressed message acceptance were more likely to have made a quit attempt since exposure (OR = 1.98, 95% CI = 1.12, 3.27). Spontaneous cognitive and emotional reactions can indicate message effectiveness and predict behavior, suggesting they should be considered when designing tobacco-related messages.
Keywords
Background
The Food and Drug Administration (FDA) proposed a policy to reduce the nicotine content of cigarettes and other combusted tobacco products to minimally addictive levels (Benowitz & Henningfield, 2018; The Federal Register, 2025; Perkins, 2019). The policy aims to reduce cigarette addictiveness to help people who smoke cut back or quit tobacco use (Berman & Glasser, 2019; Levy et al., 2021; Tidey et al., 2022). Earlier studies have shown that significantly lowering the nicotine content of cigarettes reduces the number of cigarettes smoked and increases quit attempts (Dermody et al., 2015; Livingstone-Banks et al., 2024). Over time, the policy is expected to significantly reduce smoking and smoking-related diseases by preventing initiation and supporting successful quitting (Livingstone-Banks et al., 2024). This policy enjoys a high level of support across the populations (Kim et al., 2025).
While evidence has shown that very low nicotine cigarettes (VLNCs) would be beneficial (Cassidy et al., 2023; Tidey et al., 2022), misunderstandings about the policy persist (Byron et al., 2018; Henderson et al., 2022; Ranney et al., 2022). For instance, many people who smoke believe VLNCs are safer than regular cigarettes (Byron et al., 2018). This misunderstanding likely stems from a belief that nicotine is one of the main causes of tobacco-related harms (Villanti, Byron, et al., 2019); thus, if nicotine is reduced, harm also decreases. It should be noted that some people correctly reason that reduced harm results from reduced addictiveness (Gendall et al., 2025), which may help people smoke fewer cigarettes or quit altogether, thereby lowering overall exposure to harmful substances (Hatsukami et al., 2024). However, VLNCs are not less harmful than conventional cigarettes in terms of toxicant exposure per cigarette; they deliver the same harmful chemicals that cause cancer, cardiovascular disease, and other smoking-related illnesses. Misperceptions that VLNCs are inherently “safer” products may undermine the policy’s success by encouraging smoking initiation among people who never smoked or triggering relapse among those who formerly smoked and could believe that VLNCs are a safer option (Duong et al., 2022).
Public health messaging is an effective tool for influencing consumer perceptions and behavior to improve individual and population health (Albarracin et al., 2024; Myrick, 2015). Studies have demonstrated that messages can address misperceptions that nicotine is the main cause of cancer (Villanti, West, et al., 2019). However, if messaging about VLNCs is unclear or ineffective, it may be counterproductive. Messaging that fails to clearly distinguish reduced nicotine content from reduced harm could reinforce misperceptions about VLNCs. Such misperceptions may obscure the policy’s primary goal of reducing nicotine addiction to support cessation, while also complicating how individuals interpret the role of alternative nicotine products, which are less harmful than combustible cigarettes but not risk-free.
Examining people’s responses to messages about VLNCs, both cognitive and emotional, may be especially important in determining message persuasiveness (Duong et al., 2022; Yang, Liu, et al., 2019). These responses can be examined in light of the elaboration likelihood model (ELM) (Petty, 2018; Petty & Cacioppo, 2012; Petty et al., 2014) and the heuristic–systematic model (HSM) (Chaiken, 1980; Todorov et al., 2002), which emphasize how people process persuasive messages through central and peripheral (or systematic and heuristic) routes along the way toward attitudinal and behavioral change. Central processing of information involves effortful, cognitive consideration of arguments in messages, leading to relatively enduring and stable attitude changes. By contrast, peripheral processing relies on more superficial message cues, such as emotional responses and attractiveness of message features, which may result in attitude changes, albeit less enduring changes (Chaiken, 1980; Petty et al., 2014). Notably, the ELM and HSM argue that central processing (cognitive elaboration) is the primary determinant of message effectiveness, while emotional cues are more likely to operate within the peripheral or heuristic routes of processing, which may be effective in certain contexts but are generally less likely to lead to long-lasting attitude changes. However, other theories, including extended parallel process model (EPPM; Witte, 1992) and the affect heuristic (Slovic et al., 2007), highlight the importance of emotional responses to messages as the driving force of persuasion.
Cognitive evaluations of message content can range from supporting or elaborating on the content of the message (referred here as pro-arguing) to actively disagreeing with or disputing the message (referred here as counter-arguing) (Petty et al., 2014). Similarly, message acceptance (agreeing with the message’s validity or believability) and message rejection are both important cognitive outcomes indicating how well message content is received (Witte, 1996). Expressions of these cognitive processes can serve as indicators of in-depth message processing (Petty & Cacioppo, 2012; Petty et al., 2014), which, in turn, can lead to changes in beliefs and behavior.
Emotional responses, both positive (e.g., happiness, relief, and hope) and negative (e.g., sadness, fear, anger, and guilt), can determine how persuasive a health message is. Positive emotions can enhance message acceptance by fostering a sense of optimism or receptivity (Peters et al., 2006; Slovic et al., 2007). Also, when individuals feel hopeful, inspired, or confident after exposure to a health message, they are more likely to feel increased self-efficacy (Nabi & Myrick, 2019). In contrast, negative emotions may facilitate message encoding into memory and subsequent recall, motivating protective actions that are even stronger indicators of message effectiveness (Yoo et al., 2014). Negative emotions in response to messages, such as fear, can promote desired behavioral change (Cho et al., 2018; Gerend & Maner, 2011; Hall et al., 2019), but when excessive, can bring about defensive reactions (e.g., message derogation, reactance, and avoidance), potentially reducing desired message effects (Van ‘T Riet & Ruiter, 2013), though not always (Cho et al., 2016; Thrasher, Abad-Vivero, et al., 2016).
While previous research has examined the public misperceptions, attitudes, and behavioral intentions around VLNCs, few studies investigated messaging about VLNCs, and they mostly used quantitative experiments or qualitative focus group approaches to study responses to VLNC messages (Denlinger-Apte et al., 2023; Henderson et al., 2022; Reynolds et al., 2024; Yang, Owusu, et al., 2019; Yoo et al., 2014). Earlier studies revealed that while some individuals support the policy, concerns about government motives, policy feasibility, and unintended consequences (e.g., increased smoking or black-market use) were reported (Denlinger-Apte et al., 2023; Henderson et al., 2022). Also, experimental and discrete choice studies demonstrated that including messages about harms of VLNCs can increase policy support and influence behavioral intentions (Ntansah et al., 2025; Reynolds, Popova, et al., 2024; Yang, Owusu, et al., 2019). This study complements earlier research by systematically analyzing spontaneous cognitive and emotional responses to VLNC messages and examining their associations with quit intentions, policy support, talking to others about quitting smoking, and making a quit attempt in the past 2 weeks following messages exposure.
Methods
The data come from a randomized clinical trial (Pei et al., 2024), conducted in 2022 to 2023 among a probability-based sample of noninstitutionalized U.S. adults aged 18 years and above (n = 1,901). The English-language survey was administered through KnowledgePanel, the largest online panel in the United States (KnowledgePanel—Ipsos, 2024). Participants were preidentified from internal data and sampled based on age and smoking status, targeting three groups: (1) people who exclusively smoked cigarettes (n = 941), representing individuals who had smoked 100 or more cigarettes in their lifetime, currently smoked cigarettes either some days or every day, and had never used e-cigarettes or did not use them regularly (either every day or some days); (2) people who currently dual used cigarettes and e-cigarettes (n = 472), representing people who smoked both cigarettes and e-cigarettes either every day or on some days; as this was a low-incidence subgroup, some were recruited from an opt-in sample (n = 232); and (3) young adults who never smoked (18–29 years), representing those who had not smoked 100 or more cigarettes in their lifetime as of the time of the survey (n = 458).
Procedure and Design
Participants were randomized to one of the four message conditions: (1) VLNC messages, (2) e-cigarettes messages, (3) combined VLNC and e-cigarette messages, or (4) control group who viewed water advertisements. Participants in the VLNC, e-cigarette, and control message conditions were shown two randomly selected messages from a set of five messages specific to their assigned group. In the combined condition, participants were first shown one message drawn at random from the VLNC set and then another from the e-cigarette set. Participants were told to read the messages for as long as they wanted. Afterward, they were asked to list the thoughts they had; these open-ended responses provided the message reaction data that we assessed. To ensure that all participants understood the VLNCs policy, it was explained as a hypothetical scenario following message exposure. Then they completed various outcome measures. Two weeks later, participants from the KnowledgePanel were recontacted for a follow-up survey.
This article reports on participants (n = 944) from the two conditions that involved VLNC message exposure followed by the thought-listing task: VLNC messages only and the combined messages. The messages were brief, picture and text-based informational messages stating that all cigarettes would contain much less nicotine; they would still be as harmful as regular cigarettes but will make it easier to quit (Figure 1). They were developed based on prior formative research and message testing that identified effective ways to communicate nicotine reduction (Duong et al., 2022; Reynolds, Popova, et al., 2024).
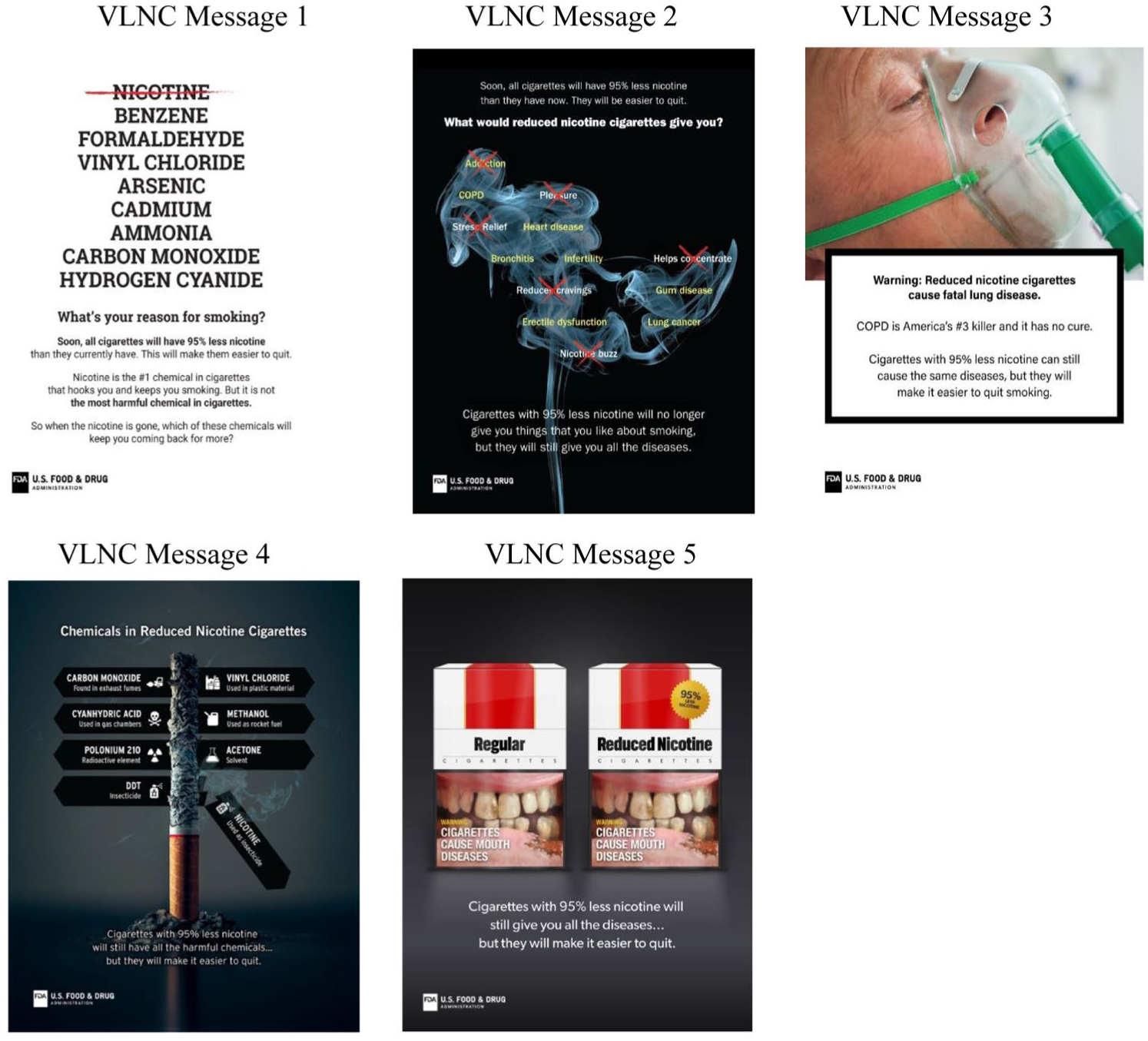
Messages About Very Low Nicotine Cigarettes (VLNCs).
The analytic sample comprised people who exclusively smoked cigarettes (18+, n = 491), people who dual used cigarettes and e-cigarettes (18+, n = 232), and young adults who never smoked (18–29, n = 221). We did not exclude participants who provided no open-ended response (n = 107, 11.33%); instead, all participants were retained in the analytic sample to avoid biasing analyses by excluding individuals based on their level of engagement or expressiveness.
Open-Ended Response Coding and Content Analysis
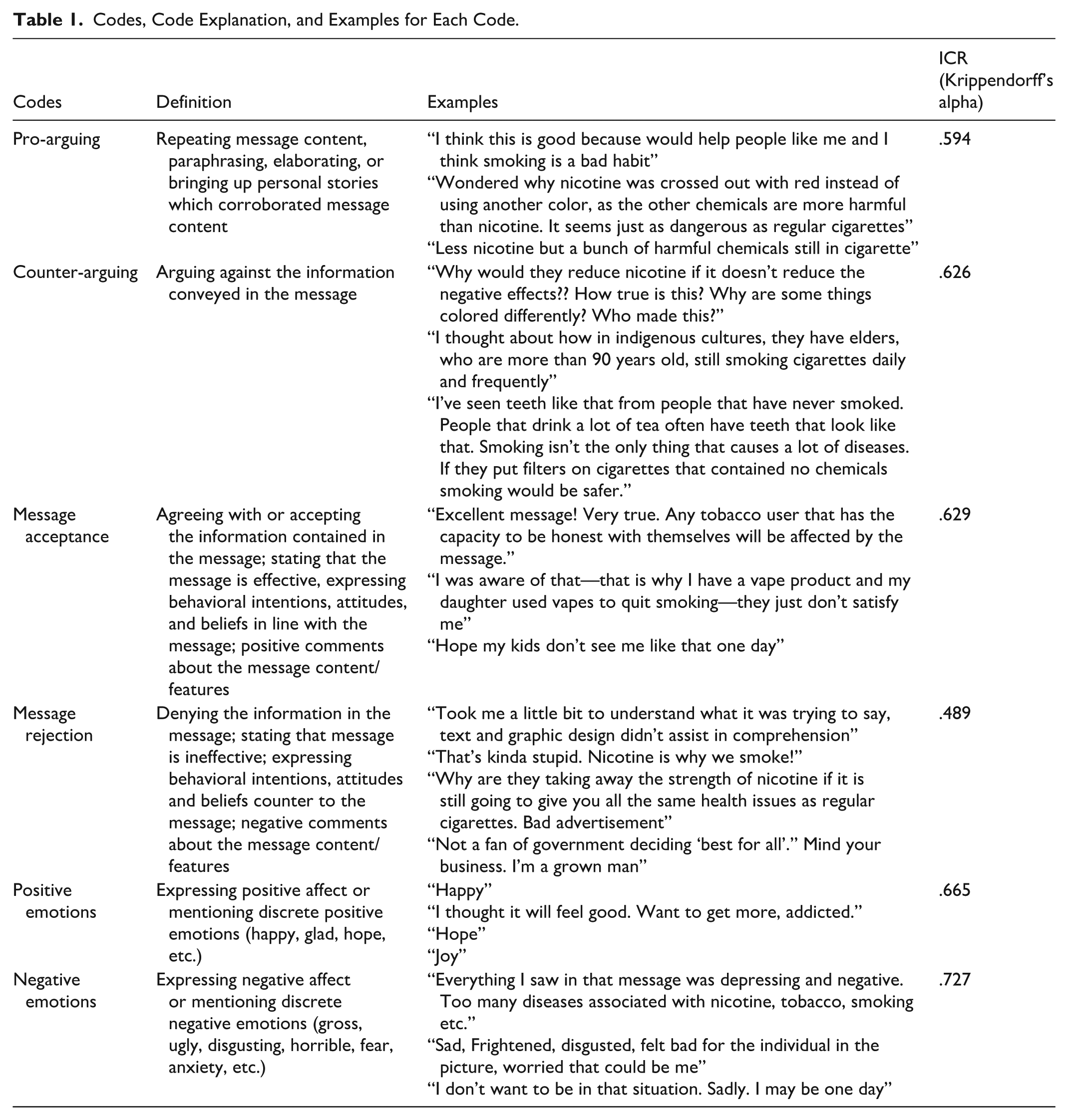
A codebook was deductively developed based on the ELM and HSM theories, focusing on cognitive and emotional processing of messages (Chaiken, 1980; Petty & Cacioppo, 2012). Table 1 presents the coding framework, including code descriptions, examples, and intercoder reliability (ICR) values computed using Krippendorff’s alpha. Each participant’s response was coded as 1 or 0 (present or absent) for cognitive reactions (pro-arguing, counter-arguing, message acceptance, or message rejection) and emotional reactions (positive or negative emotions). Codes were not mutually exclusive, meaning that a response can be coded as 1 for several codes. The coding process involved three rounds of double coding by two coauthors, followed by a final reconciliation stage. A random 10% of responses were double coded in each round and the coded responses were combined to compute a single ICR value for each code. Afterward, the remaining responses were divided between the coders, who switched data sets to cross-check the assigned codes. All outstanding discrepancies were resolved through consensus among authors. These procedures ensured a fully reconciled data set.
Codes, Code Explanation, and Examples for Each Code.
Primary Outcomes
Following message exposure, participants reported their support for VLNC policy and those who smoke were asked about intentions to quit smoking. Two weeks later, participants reported on behavioral outcomes (talking to others about quitting and making a quit attempt for those who smoke). All participants were asked to consider the policy of reducing nicotine by 95% in all cigarettes and indicate their level of support or opposition on a 5-point scale. The response options included (1) strongly oppose, (2) oppose, (3) neither support nor oppose, (4) support, and (5) strongly support. Responses for policy support were recoded into a dichotomous variable, with “strongly support” and “support” combined into a single “support” category, and all other responses grouped into a “do not support” category. Intention to quit smoking was assessed using three questions: (1) How interested are you in quitting smoking in the next 6 months? (2) How much do you plan to quit smoking in the next 6 months? and (3) How likely are you to quit smoking in the next 6 months? Responses to each question were scored on a 1 to 7 scale, with higher scores indicating stronger intentions to quit, and were averaged into a composite scale (Cronbach’s alpha = .92). Talking to others about quitting smoking was measured on a 5-point scale, with options, including: (1) not at all, (2) once, (3) a few times, (4) often, and (5) very often, an outcome that mediates message effects on cessation behaviors (Thrasher, Abad-Vivero, et al., 2016). This variable was dichotomized (i.e., “not at all” vs. all other responses). Finally, making a quit attempt in the last 2 weeks postexposure was measured using a “Yes” or “No” response.
Covariates
Participants reported their sociodemographic characteristics, including sex, age, smoking status, and ethnic background. In addition, the specific VLNC message viewed by participants as well as assigned conditions were included among covariate adjustment variables.
Statistical Analyses
Descriptive statistics were summarized and reported using frequencies and percentages. Cognitive and emotional responses were compared across messages, demographic groups and smoking status groups. Statistically significant differences for categorical variables were assessed by chi-square analyses. Linear regression analyses were used to assess association between quit intentions and open-ended codes while logistic regression analyses examined association between open-ended codes and VLNCs policy support for the entire sample and for people who smoke cigarettes, talking to others about quitting smoking and making a quit attempt in the 2 weeks following message exposure. We first ran univariate models (Model 1) where a single open-ended code predicted each outcome. Then, we ran multivariable models (Model 2) where all open-ended codes were entered into the model simultaneously, including the covariates. All analyses were conducted using unweighted data in SAS 9.4 (M8) via SAS OnDemand for Academics.
Results
A total of 944 participants completed Session 1, including 491 people who exclusively smoke cigarettes, 232 who dual use cigarettes and e-cigarettes, and 221 young adults (aged 18–29) who had never smoked. Two weeks later, 753 completed Session 2 resulting in approximately 80% retention rate. Among Session 1 participants, 55.4% were female, 43.3% were working full-time, 34.3%, had some college education, and 71.6% were non-Hispanic White. Supplemental Table 1 shows demographic characteristics for participants overall and for people who smoke separately.
Cognitive and Emotional Reactions Across VLNC Messages
Overall, pro-arguing was most common (42.4%), followed by message acceptance (31.9%), message rejection (19.3%), negative emotions (15.8%), counter-arguing (12.4%), and positive emotions (1.2%). Table 2 presents the frequency of codes overall and by VLNC message. Pro-arguing differed significantly by message (p = .01); message 4 had the highest percentage of pro-arguing (56.8% of responses) and message 5 the lowest (37.91%). In addition, message rejection (p = .01); and negative emotions (p < .0001) were significantly different across messages; message 2 generated the highest rate of message rejection (23.29%), while message 5 generated the most negative emotions among participants (29.41%).
Cognitive and Emotional Reactions Across VLNC Messages.
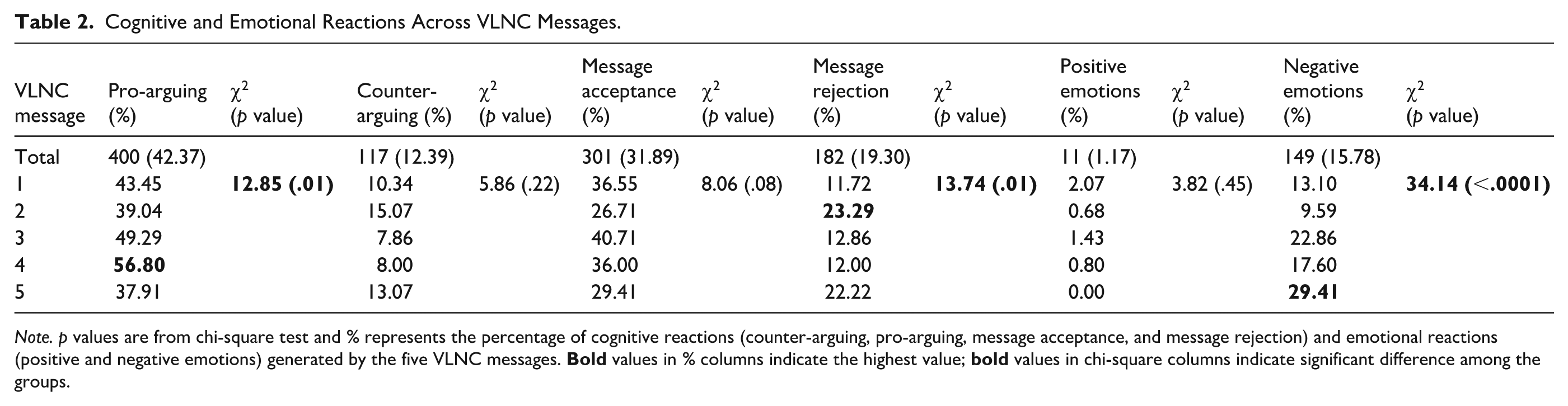
Note. p values are from chi-square test and % represents the percentage of cognitive reactions (counter-arguing, pro-arguing, message acceptance, and message rejection) and emotional reactions (positive and negative emotions) generated by the five VLNC messages.
Cognitive and Emotional Reactions by Demographic and Smoking Status
Table 3 reports cognitive and emotional reactions by demographic and smoking status. Overall, negative emotions were more frequently expressed by females than males (19.26% vs. 11.63%), but otherwise no differences by sex were found. Smoking groups differed significantly for all cognitive reactions, but not for emotional reactions. Counter-arguing (15.68%) and message rejection (24.03%) were more common among people who exclusively smoked regular cigarettes compared with people who dual use cigarettes and e-cigarettes (9.48% and 13.79%, respectively) and young adults who never smoked (8.14% and 14.55%, respectively). In contrast, young adults who never smoked and people who dual use cigarettes and e-cigarettes demonstrated higher levels of pro-arguing (48.42% and 48.28%, respectively) compared with people who exclusively smoked regular cigarettes (36.86%). In addition, people who dual use cigarettes and e-cigarettes had the highest rate of message acceptance (43.1%) compared with young adults who never smoked (37.1%) and people who exclusively smoke cigarettes (24.24%).
Cognitive and Emotional Reactions by Demographic and Smoking Status.
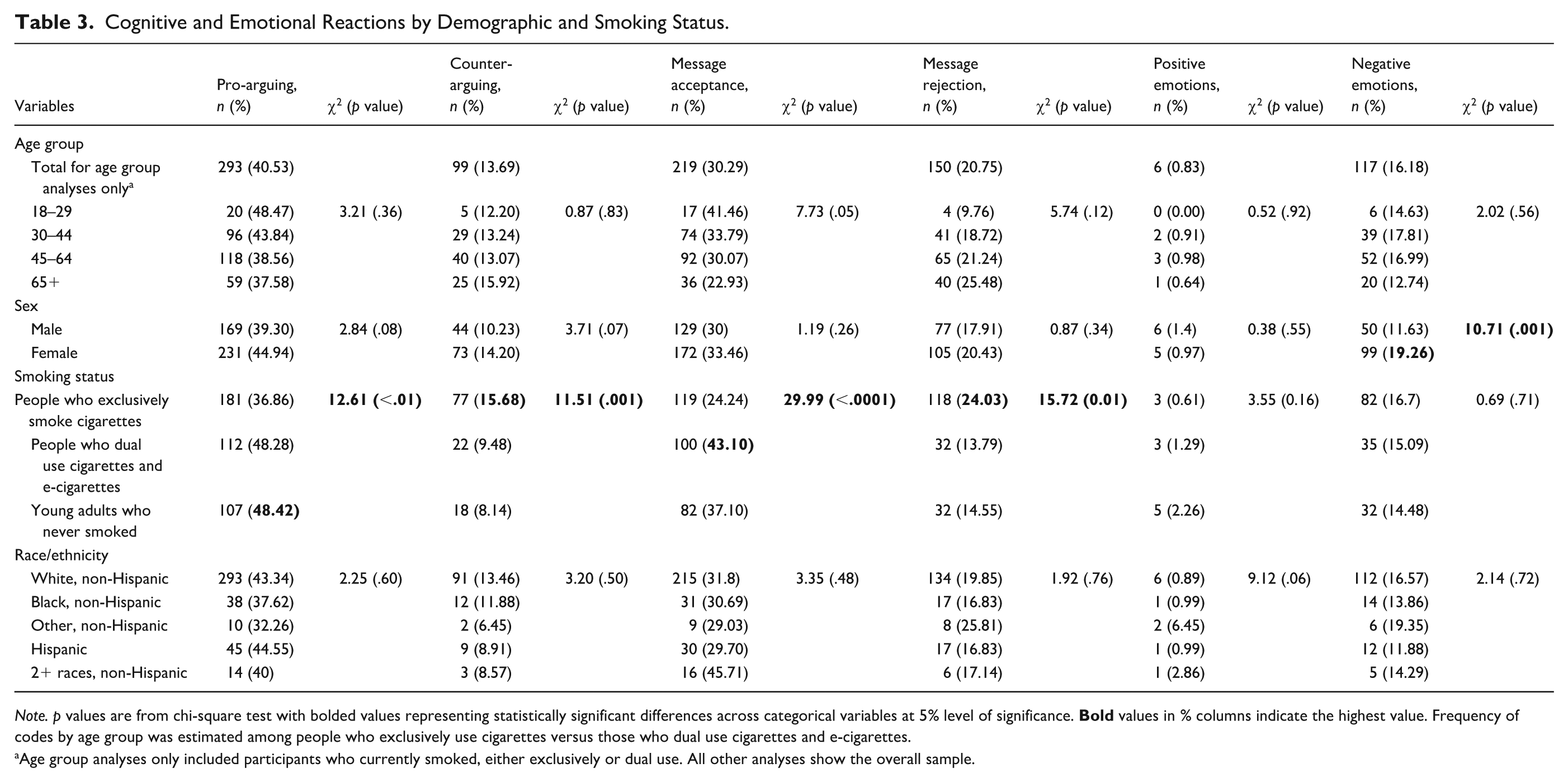
Note. p values are from chi-square test with bolded values representing statistically significant differences across categorical variables at 5% level of significance.
Age group analyses only included participants who currently smoked, either exclusively or dual use. All other analyses show the overall sample.
VLNC Policy Support
Table 4 shows association between open-ended codes and outcomes, including support for nicotine reduction policy and quit intentions immediately following message exposure, as well as talking to others about quitting smoking and making a quit attempt in the 2 weeks after message exposure. In the bivariate model, participants who counter-argued (OR = 0.52, 95% CI = 0.34, 0.80) and those who rejected VLNC messages (OR = 0.48, 95% CI = 0.33, 0.68) were less likely to support nicotine reduction policy. However, pro-arguing (OR = 1.67, 95% CI = 1.28, 2.18) and message acceptance (OR = 1.99, 95% CI = 1.51, 2.63) were positively associated with nicotine reduction policy support. In the multivariable model, only pro-arguing and message acceptance remained significant positive predictors of policy support.
Association Between Open-Ended Codes and Support for the Policy, Quit Intensions, Talking to Others About Quitting, and Quitting Attempts.
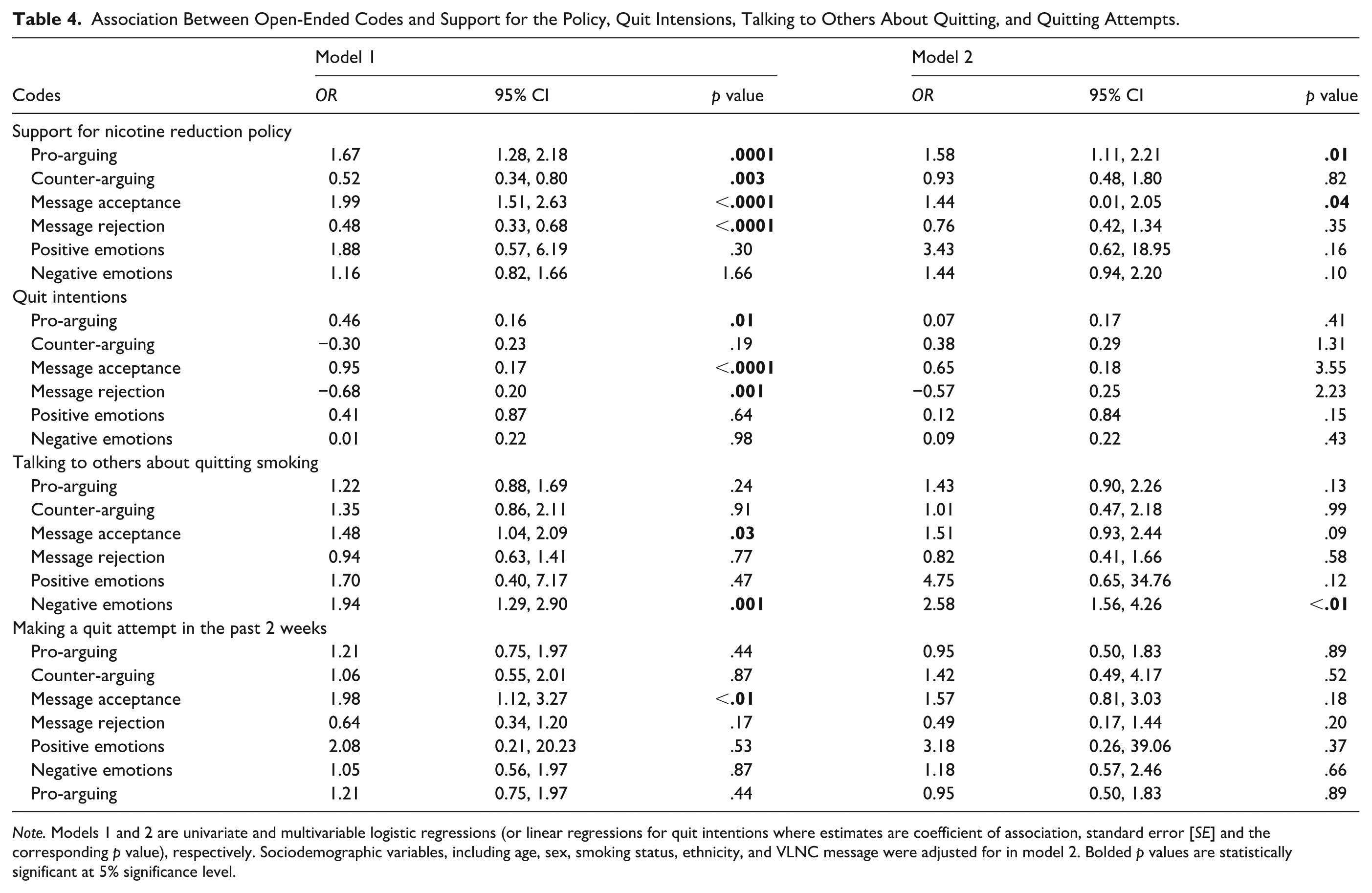
Note. Models 1 and 2 are univariate and multivariable logistic regressions (or linear regressions for quit intentions where estimates are coefficient of association, standard error [SE] and the corresponding p value), respectively. Sociodemographic variables, including age, sex, smoking status, ethnicity, and VLNC message were adjusted for in model 2. Bolded p values are statistically significant at 5% significance level.
Quit Intentions
In Model 1, pro-arguing (β = 0.46, p = .005) and message acceptance (β = 0.95, p < .0001) were associated with increased quit intentions, while message rejection (β = –0.68, p = .0005) was linked to decreased quit intentions. In Model 2, both message acceptance (β = 0.65, p < .0001) and message rejection (β = –0.57, p = .03) remained statistically significant predictors of quit intentions (Table 4).
Talking to Others About Quitting Smoking and Making a Quit Attempt in the 2 Weeks After Message Exposure
Overall, in this sample among adults who smoked who completed the 2-week follow-up (n = 569), 32.3% reported talking to others about quitting smoking and 13.9% made a quit attempt in the 2 weeks following the message exposure. In Model 1, message acceptance (OR = 1.48, 95% CI = 1.04, 2.09) and negative emotions (OR = 1.94, 95% CI = 1.29, 2.90) were significant predictors of talking to others about quitting smoking. In Model 2, participants who expressed negative emotions (OR = 2.58, 95% CI = 1.56, 4.26) in response to VLNC messages were more than twice as likely to talk to others about quitting smoking. Participants who expressed message acceptance were more likely to make a quit attempt within 2 weeks after the exposure (OR = 1.98, 95% CI = 1.21, 3.27), but this was only significant in the univariate model (Table 4).
Discussion
This study systematically examined spontaneous cognitive and emotional responses to messages about VLNCs. Our findings reveal distinct patterns in cognitive responses across different smoking groups. Participants who engaged in pro-arguing or expressed message acceptance were more likely to support the nicotine reduction policy. In addition, participants who expressed message acceptance exhibited greater intentions to quit, and, 2 weeks after message exposure, higher likelihood of talking to others about quitting and making a quit attempt.
Variations in Reaction to VLNC Messages Based on Participant Characteristics
Findings revealed some variation in cognitive and emotional responses to VLNC messages by participant sociodemographics. Female participants more frequently expressed negative emotions, possibly reflecting broader gender differences in emotional expression, especially in response to health information (Kring & Gordon, 1998). Higher expression of negative emotions among females may also indicate that females may feel or express a greater concern about health risks of smoking behavior (Li et al., 2023). Previous studies have also found that, compared with males, females report higher levels of negative emotional responses to health messages (Levkovich & Shinan-Altman, 2021; Wray et al., 2015).
Smoking status was associated with cognitive responses. People who exclusively smoke demonstrated higher levels of counter-arguing and message rejection, possibly due to long-standing beliefs about smoking or resistance to change (Ozarka et al., 2024), whereas people who dual use cigarettes and e-cigarettes and young adults who never smoked exhibited more pro-arguing. This suggests that these latter groups may be more receptive to messages about VLNC policy for cigarettes because they either already have an alternative source of nicotine or they do not use any nicotine at all. In addition, young adults who never smoked, simply due to their age, might be more accepting of new information (Kimber et al., 2020). Furthermore, higher message acceptance among people who dual use cigarettes and e-cigarettes may indicate a willingness to transition to healthier behaviors (since they might be using e-cigarettes because they believe they are less harmful or might help them quit) (Harlow et al., 2022; Tran et al., 2024). Thus, they might be also more open to another smoking modification, in this case, VLNCs. Their receptiveness suggests a greater readiness to change their tobacco use behavior, whether through switching to e-cigarettes or considering health messages that advocate for VLNCs as a step toward addressing addiction and achieving cessation.
Cognitive and Emotional Responses, Nicotine Reduction Policy Support, and Behavior Change
Pro-arguing was a common cognitive response to VLNC messages and was positively associated with key outcomes, including greater policy support and stronger quit intentions among people who smoked. Message acceptance was also frequently expressed and similarly linked to higher policy support, greater quit intentions, and increased likelihood of talking to others about quitting. These patterns align with persuasion through central route processing (ELM) or systematic processing (HSM) (Johnson et al., 2005; Maio & Haddock, 2007). While findings suggest a potential link between pro-arguing or message acceptance and favorable outcomes, it is also possible that individuals already inclined to quit or support nicotine reduction policies were more likely to agree with the messages. The direction of causality requires further investigation. Nonetheless, pro-arguing and message acceptance may reflect perceived message effectiveness, which is a useful indicator of actual message impact (Noar et al., 2018, 2020).
A small proportion of participants engaged in counter-arguing, which was associated only with lower support for the nicotine reduction policy. Prior research has suggested mixed effects of counter-arguing on behavior (Petty et al., 2004; Tormala et al., 2006). Petty et al. (2004) noted that counter-arguing can either strengthen preexisting attitudes that oppose the message, resulting in no change in behavior, or in some cases, lead to attitude shifts that favor the message. Similarly, Tormala et al. (2006) theorized that resisting persuasion may reduce confidence in one’s initial attitudes, which can result in positive behavior change. In this study, counter-arguing was not associated with quit intentions or other behavioral outcomes among people who smoke, suggesting it may not necessarily lead to negative behavioral consequences. Message rejection is a cognitive response that can undermine the effectiveness of health messages. In this study, participants who rejected VLNC messages showed lower support for nicotine reduction policy and lower quit intentions among people who smoke. This may reflect perceptions of the policy as unjustified, ineffective, or lacking credibility, which can reduce the likelihood of behavior change. However, reverse causation is also possible, as those already opposed to nicotine reduction may be more likely to reject related messages. These findings align with prior research showing that message rejection can diminish message effectiveness (Lewis et al., 2010; Tannenbaum et al., 2015), highlighting the importance of crafting messages that reduce messages opposition while increasing messages acceptance (Reynolds-Tylus, 2019).
Expression of positive emotions was low in this study, but this is understandable since our messages were not designed to elicit positive emotions. On the contrary, a sizable number of respondents expressed negative emotions (15.78%), such as fear, guilt, or sadness. These emotional responses have been shown to be linked to the persuasiveness of messages, especially in context of health communication (Baumeister et al., 2007; Becheur & Valette-Florence, 2014). For example, emotions, such as fear, sadness, or guilt can enhance individuals’ recall of health messages and motivate them to resolve these emotions by taking the necessary actions to facilitate behavioral change (Nabi, 1999; Witte, 1992).
Similarly, we found that negative emotions were associated with talking to others. While we did not find link between emotions and quitting behavior, talking is a precursor to behavioral change (Thrasher, Swayampakala, et al., 2016). Earlier studies also found that negative emotions can inspire meaningful interpersonal discussions, which may lead to favorable behavioral changes (Myrick, 2015; Nabi, 1999; Witte, 1992). For example, after interacting with health messages, people who feel fear or sadness might be inclined to express their feelings to others. This sharing could involve encouraging others to quit smoking, raising awareness among the public, or looking for help to stop smoking themselves. Furthermore, talking to others may relieve negative emotions and this may naturally encourage people to have meaningful conversations about their feelings (Ma et al., 2024). Expressing negative feelings can also motivate people to push for or advocate for change by telling others not to engage in harmful behaviors. Previous studies documented this correlation, highlighting the fact that health messages that evoke negative emotions can intensify interpersonal conversations, and how having these conversations can increase message’s impact (Dunlop et al., 2008; Hendriks et al., 2014), including how conversations about anti-smoking messages predict subsequent smoking cessation attempts (Arillo-Santillán et al., 2024; Lambert et al., 2020; Thrasher, Swayampakala, et al., 2016).
Limitations
The design of this study does not allow us to make causal inferences about the role of spontaneous reactions to the messages in subsequent outcomes. While our study was longitudinal, it is still possible that the associations we found were due to confounding factors, such as preexisting individual differences. The study only used a 2-week follow-up period, which might not be enough to ascertain whether the associations found persist over time or result in long-term behavioral changes. Only five messages about VLNCs limit the generalizability of findings.
Implications for Policy and Practice
This study shows how cognitive and emotional reactions to VLNC messages relate to policy support and quit behaviors. Tailoring messages to evoke specific reactions can enhance public support for VLNC policies and encourage quitting. The link between emotional responses and discussions about quitting also highlights the value of incorporating social and community-based approaches in tobacco control campaigns. Policymakers and health communicators can leverage these insights to design messages that drive both policy acceptance and cessation.
Conclusion
Spontaneous cognitive and emotional reactions can be valuable indicators of message effectiveness, offering insights into how individuals process and respond to messages. In addition to reflecting individuals’ immediate response to messages, these responses may predict behavioral outcomes like quit intentions, support for policy, and talking to others about quitting smoking. Designing messages with these reactions in mind can help ensure their effectiveness across diverse smoking populations.
Supplemental Material
sj-docx-1-heb-10.1177_10901981251414630 – Supplemental material for Examining Spontaneous Cognitive and Emotional Reactions to Messages About Very Low Nicotine Cigarettes (VLNCs)
Supplemental material, sj-docx-1-heb-10.1177_10901981251414630 for Examining Spontaneous Cognitive and Emotional Reactions to Messages About Very Low Nicotine Cigarettes (VLNCs) by Folashayo P. Adeniji, Vanessa Mallory, Di Pei, James F. Thrasher and Lucy Popova in Health Education & Behavior
Footnotes
Funding
This study was funded by the National Cancer Institute and the Food and Drug Administration Center for Tobacco Products (R01CA239308). The authors are solely responsible for the content of this manuscript, and reported findings do not reflect the official views of the National Institutes of Health or the Food and Drug Administration. The funders played no role in the study design, data collection, analysis, decision to publish, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.