
Abstract
This study assessed Chinese cancer patients’ willingness to participate in phase III clinical trials of new anti-cancer drugs and examined influencing factors using the Health Belief Model (HBM) and social support. A cross-sectional survey recruited 480 patients from an online community through convenience sampling. Data included demographics, disease and treatment status, HBM constructs (including perceived severity, perceived benefit, perceived barrier, cue to action, self-efficacy), social support (including family’s, friends’, and others’ support), and willingness to participate. Statistical analyses involved factor analysis, reliability testing, correlations, and hierarchical regression. The mean willingness score was 2.883 (range = 1–5). Willingness varied significantly by living arrangements, employment, income, and treatments. Demographics explained 9.8% of the variance, disease and treatment status 12%, and social support 22.4%, with family support as a significant predictor (β = 0.202, p < .001). Incorporating HBM constructs raised the explained variance to 48.2%. Key positive predictors included cues to action (β = 0.251), self-efficacy (β = 0.281), and perceived severity (β = 0.151), while perceived barriers reduced willingness (β = −0.114). Findings suggest Chinese cancer patients show limited willingness to join phase III trials, although it should be generalized cautiously, considering the non-representative nature of the online sample. Enhancing family support and targeting self-efficacy and external motivators may improve engagement, supporting the utility of the HBM framework.
Introduction
Cancer is an important social, public health, and economic problem facing the 21st century. At present, the best strategy to continuously reduce the global cancer burden in addition to the promotion of primary and secondary prevention is to extensively implement personalized and precision medicine and increase investment in advancing cancer drug research (Liu et al., 2024).
The development of new anticancer drugs faces challenges like high costs, long timelines, and low success rates, requiring phase I, II, and III clinical trials for approval. Phase III trials involve large-scale randomized controlled studies where participants are usually cancer patients with locally advanced or metastatic disease who do not receive systemic therapy or have radiographical progression after prior treatment (Nielsen & Berthelsen, 2019). Evidence from the United States indicates that participation in clinical trials is generally low, with fewer than 5% of eligible adult patients enrolling in clinical research (Saphner et al., 2021). According to the Epistemic AI database, 18% of all phase II/III trials that terminate do so primarily for “enrollment issues,” making it the third-most common stop reason after efficacy/safety signals from 2013 to 2023 (Bowling et al., 2026). As of January 2022, approximately 1.3% of the clinical trials on the China Drug Clinical Trial Registration and Information Disclosure Platform were voluntarily terminated, with phase III trials accounting for 26.3% and 10.1% were terminated due to difficulties in patient enrollment (Li et al., 2019; Su et al., 2021). Slow patient recruitment increases development costs, hinders market approval, and limits drug availability (M. S. Chen et al., 2014; Saphner et al., 2021). Although participation in cancer clinical trials has been widely discussed, existing evidence on phase III trial willingness from the perspective of health beliefs and social support remains limited, particularly in the Chinese context.
Most participants in anti-cancer drug trials are recruited through clinicians from outpatients and inpatients, with some volunteering via invitations or advertisements. However, recruitment faces two main barriers: objective factors such as time and financial burdens, strict eligibility criteria, and lengthy screening processes and subjective barriers including dissatisfaction with randomization, concerns about disruptions to daily life, fear of side effects, doubts about drug efficacy, distrust of researchers, low family support, and low self-efficacy (J. Chen et al., 2023; Fitzer et al., 2022; Mahon et al., 2016). Importantly, while prior studies have often focused on actual enrollment behavior or general attitudes toward clinical trials, relatively less attention has been given to patients’ willingness to participate as a distinct and critical antecedent of enrollment.
Some studies have examined barriers to participation in clinical trials of cancer from health behavior theory (Byrne et al., 2014; Mobley et al., 2020). The Health Belief Model (HBM) is one of the most commonly used frameworks in health-related research that explains and predicts health behavior (Carpenter, 2010), focusing on individual beliefs about health and disease and emphasizing the key role of subjective perception in shaping behavior. In clinical trials, HBM is commonly used to understand patient motivation (Rollins et al., 2018), suggesting that the decision to adopt health behaviors depends on perceived disease threats (susceptibility and severity) and the balance between perceived benefits and barriers. Furthermore, “cues to action,” such as external advice, also influence decision-making, and self-efficacy determines the confidence to take such action. Patients who perceive greater health threats and fewer barriers are more likely to participate, while those satisfied with current treatments or distrustful of physicians and researchers may be less willing (Asher et al., 2022). In addition, HBM constructs do not operate in isolation; rather, they are theorized to interact in complex ways. These interactions may include sequential pathways, where a change in one construct (e.g., a reduction in perceived barriers) subsequently influences another (e.g., an increase in perceived benefits). Furthermore, moderating relationships are plausible, such as self-efficacy conditioning the influence of other constructs like perceived threat or barriers on behavior (Jones et al., 2015). Nevertheless, empirical studies often examine HBM constructs independently and rarely integrate them with broader social-contextual factors, such as social support, when investigating participation in cancer clinical trials. This limits a comprehensive understanding of how individual beliefs and social influences jointly shape decision-making.
Perceived social support refers to an individual’s beliefs about the level of support from their social network and is often measured subjectively, making it a common and easily assessed indicator (Dour et al., 2014; Singstad et al., 2021; Wang et al., 2018). A previous study has revealed that patients who were willing to participate in clinical trials tended to report higher perceived social support than those who refused to participate (Pariera et al., 2017). This suggests that higher perceived social support may play a significant role in motivating patients to consider participating in clinical trials, highlighting the potential importance of social networks in health care decision-making.
In China, awareness and acceptance of new anti-cancer drug clinical trials among cancer patients remain relatively low (Huang et al., 2020). However, empirical evidence examining the psychological and social determinants of clinical trial participation among Chinese cancer patients is still limited, particularly within theory-driven and integrative analytical frameworks. Existing studies have largely been conducted in Western populations, despite substantial differences between Western and Chinese contexts in health care systems, cultural norms, family involvement, and medical decision-making processes.
Therefore, the primary objective of this study was to identify the independent predictors of Chinese cancer patients’ willingness to participate in phase III clinical trials of new anti-cancer drugs based on HBM, and social support was added as an independent construct. Our findings aim to provide insights for developing effective strategies to enhance cancer patient recruitment for phase III clinical trials.
Method
Study Population and Eligible Criteria
This was a cross-sectional study conducted in cancer patients. Participants were selected by convenience sampling from 12 online communities consisting of oncology experts, medical science bloggers, and about 500 cancer patients from various provinces in China. The data collections were completed in May 2024. Participants who met the following criteria were included in the study: (a) diagnosed with cancer by histopathology; (b) radiological disease progression during or after the most recent treatment regimen; (c) were 18 years of age or older; and (d) were able to complete the questionnaires independently and sign the informed consent.
Sample Size and Data Collection Procedure
The minimum sample size was determined by referencing the requirements of explanatory factor analysis (EFA) based on the rule of thumb of a subject-to-item ratio of 10:1 (Osborne & Costello, 2005); by adding a 20% non-response rate, the final sample size was calculated as 288.
After obtaining the cooperation and consent of the community administrators, we disseminated the recruitment information and shared the questionnaire link in the communities. The questionnaire included four quality control questions, and those who failed to answer all four questions correctly were excluded. Prior to the main survey, a pilot test with 20 cancer patients showed a minimum completion time of approximately 4 min, with no reported burden related to questionnaire length or time. Based on these results, a conservative 3-min minimum completion time was used in the main survey for data quality control, and questionnaires completed in less than 3 min were excluded as potentially inattentive responses, and can only be completed once per user.
This study was approved by the Medical Research Ethics Committee of the School of Public Health, Fudan University (the international registry no. IRB00002408 & FWA00002399). All participants provided informed consent, and data were anonymized to ensure confidentiality. Eventually, a total of 494 questionnaires were received, of which 480 were valid, with a response rate of 97.17%.
Measurements
Patient Characteristics
This included questions on sociodemographic characteristics (sex, age, body mass index [BMI], marital status, current living arrangements, education level, current employment status, health insurance, personal monthly income), pre-existing conditions, and treatments received (surgical treatment, chemotherapy, radiation therapy, other treatments [e.g., Traditional Chinese Medicine, TCM]).
HBM
The HBM scale for cancer patients was adopted from previous research (Verheggen et al., 1998) and modified for this study. It contains five dimensions: (a) perceived severity (five items; e.g., I have felt my current cancer condition is severe), (b) perceived benefit (four items; e.g., participation in the trial will help me understand my condition), (c) perceived barriers (five items; e.g., I am concerned that the trial drug may have greater side effects), (d) self-efficacy (four items; e.g., I am confident that I can identify which trials are suitable for me), and (e) cues to action (five items; e.g., if a specialist from a general hospital recommends participation, I will participate in the trial). Each item was rated on a 5-point Likert-type scale ranging from strongly disagree (1 score) to strongly agree (5 score), with a higher score indicating greater belief.
Perceived Social Support
The perceived social support level of cancer patients was measured using the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988). This scale is a self-report questionnaire consisting of three subscales: family (four items), friends (four items), and significant others (four items), which are used to measure the social support perceived by the subjects from different sources. Items are rated on a 7-point Likert-type scale, ranging from strongly disagree (1 score) to strongly agree (7 score). The total score is calculated by summing all item scores and dividing by the number of items, with final scores ranging from 1 to 7. Higher scores indicate greater perceived social support. After obtaining permission from the scale’s author, the existing Chinese version of the MSPSS was used in this study. The Cronbach’s alpha coefficients for the three dimensions were 0.908, 0.917, and 0.936, respectively. The MSPSS has been demonstrated to have good reliability, validity, and effectiveness in measuring perceived social support levels among cancer patients.
Patient’s Willingness to Participate in Cancer Clinical Trials
Cancer patients’ willingness to participate in clinical trials was assessed using the following question: “To what extent are you willing to participate in a phase III clinical trial of new anti-cancer drugs?” Responses were measured using a five-point Likert-type scale, ranging from unwilling (1 score) to very willing (5 scores; Verheggen et al., 1998); a higher score indicates a more positive attitude and greater willingness to participate.
The Chinese version of the questionnaire is provided in the Supplemental File.
Statistical Analysis
Continuous variables are reported as means and standard deviations (SDs), while categorical variables are reported as frequencies and percentages. Exploratory factor analysis (EFA) with principal component analysis (PCA) and varimax rotation was conducted to extract and assess the factor structures of the HBM scale. The Kaiser–Meyer–Olkin (KMO) measurement of sampling adequacy (> 0.6) and Barlett’s test of sphericity (p < .001) were considered for acceptable factor analysis (Cerny & Kaiser, 1977). The internal consistency of each factor was analyzed with Cronbach’s α, where a value above 0.7 indicates good reliability of the scale (Ursachi et al., 2015). Associations between the participants’ characteristics and willingness to participate in a clinical trial were assessed using independent sample t-tests and analysis of variance (ANOVA). Pearson’s correlation coefficients were calculated to define the correlation among health beliefs, perceived social support, and willingness to participate. Finally, we developed a hierarchical multiple regression model to identify independent predictors of willingness to participate. Model 1 included only sociodemographic factors as predictors, while Model 2 incorporated variables related to pre-existing conditions and treatments received. Model 3 further added the three dimensions of perceived social support. The final Model 4 included the five dimensions of the HBM. To assess multicollinearity among the model variables, we calculated the variance inflation factor (VIF), with values below 5 indicating no significant multicollinearity. All analyses were performed using R software, version 4.4.1 (The R Foundation). The p-values less than .05 were considered statistically significant.
Results
Descriptive Analysis and EFA of the HBM
EFA was conducted on the 23 items, with the structure constrained to five factors as proposed by the HBM scale. Criteria for item extraction: (a) low factor loadings (<0.4) or cross-loadings (>0.3); (b) eigenvalues >1; or (c) improperly classified items. Based on the criteria, two items were excluded: “I feel cancer affects my family life” (Perceived severity), due to cross-loadings on multiple factors; and “I do not want to be randomly assigned” (Perceived barriers), which was misclassified as perceived benefit. In the final scale, 21 items were retained from the initial 23 with a cumulative variance contribution of 71.25%, with factor loadings ranging from 0.601 to 0.842. Bartlett’s test of sphericity, χ² (210) = 6,056.659, p < .001 and the KMO index (0.87) indicated an adequate sample size and suitability of the data for EFA. The Cronbach’s alpha coefficients of perceived severity, perceived benefit, perceived barriers, self-efficacy, and cues to action were 0.822, 0.897, 0.743, 0.913, and 0.891, respectively, indicating good internal consistency (Table 1).
Exploratory Factor Analysis and Descriptive Analysis of the HBM Variables.
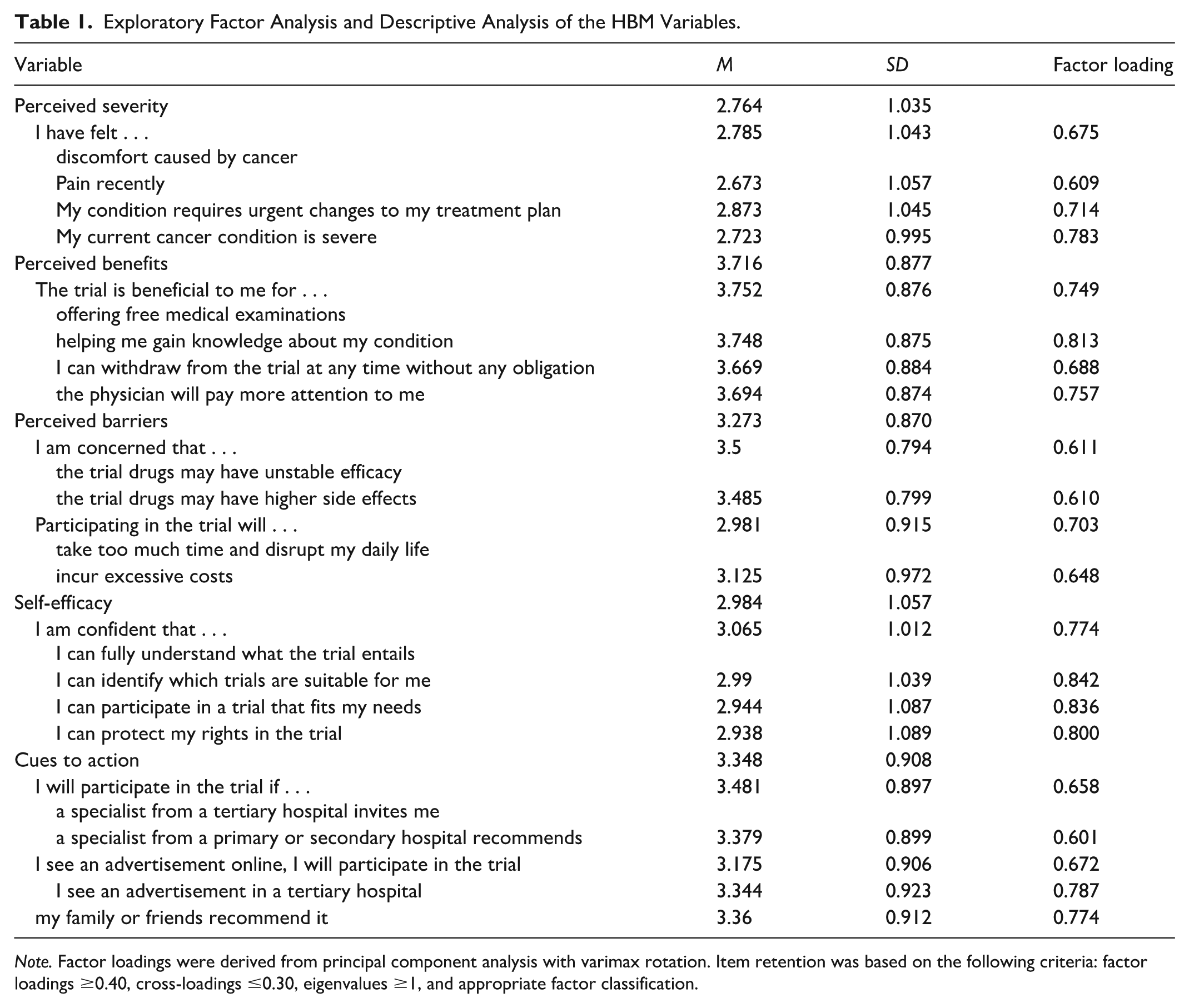
Note. Factor loadings were derived from principal component analysis with varimax rotation. Item retention was based on the following criteria: factor loadings ≥0.40, cross-loadings ≤0.30, eigenvalues ≥1, and appropriate factor classification.
Descriptive Statistics
The demographic information was described in Table 2. Among the 480 participants, 45.83% were male and 54.17% were female, with a mean age of 39.31 years (SD = 12.04). Patients living with spouses or family members reported higher mean willingness scores than those living alone. Differences in willingness were also observed across employment status, with part-time workers showing higher mean willingness scores. In contrast, higher personal income and having received treatments such as TCM were associated with lower mean willingness scores.
Sociodemographic, Disease-Related Characteristics, and Their Associations With Willingness to Participate in Phase III Clinical Trials (n = 480).
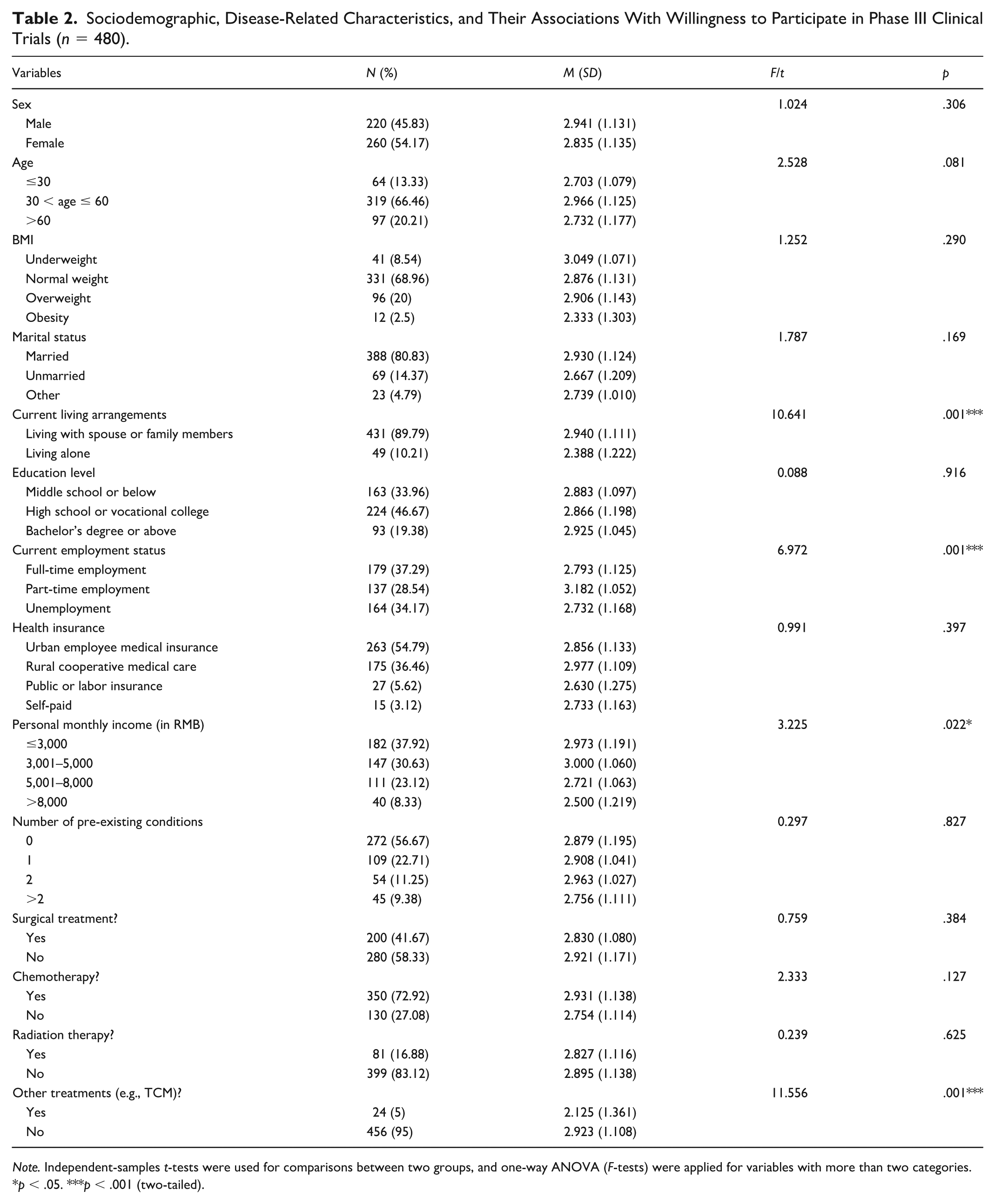
Note. Independent-samples t-tests were used for comparisons between two groups, and one-way ANOVA (F-tests) were applied for variables with more than two categories.
p < .05. ***p < .001 (two-tailed).
Correlation
As shown in Table 3, the willingness to participate in phase III clinical trials of new anti-cancer drugs was significantly and positively correlated with perceived social support and several dimensions of the HBM, including perceived severity, perceived benefits, self-efficacy, and cues to action, while perceived barriers were negatively correlated and were not statistically significant.
Descriptive Statistics, Reliability of HBM and Social Support Variables, and Correlations Between the Variables.
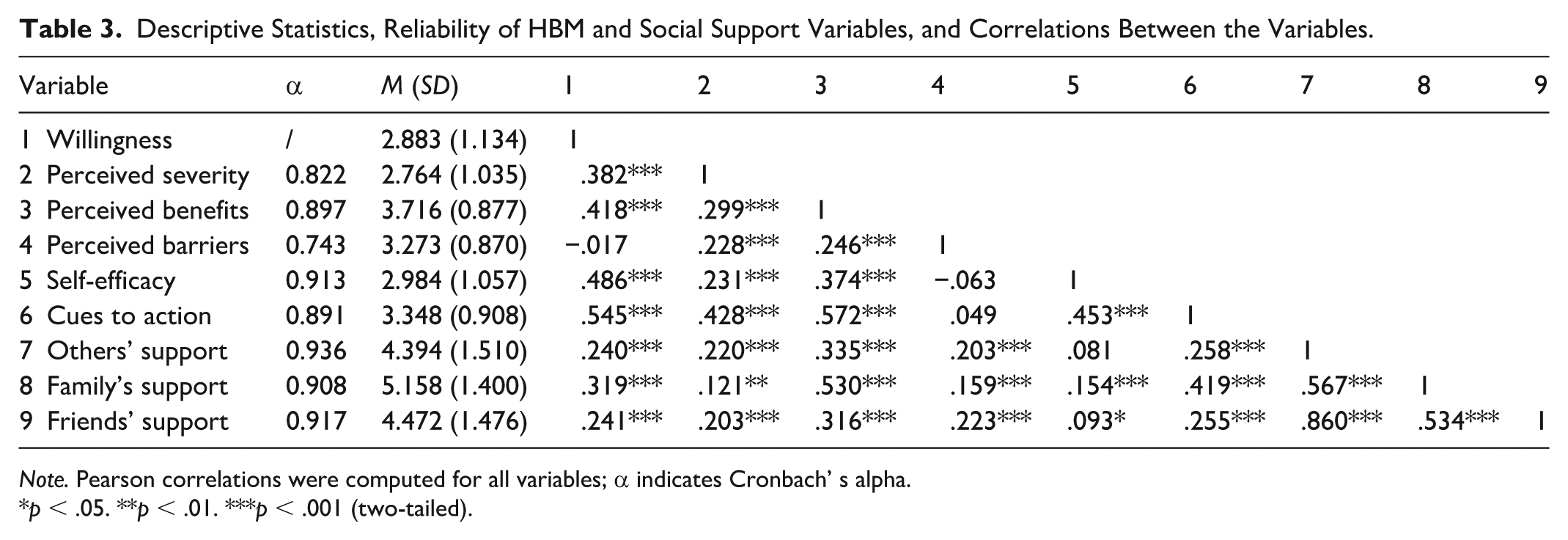
Note. Pearson correlations were computed for all variables; α indicates Cronbach’ s alpha.
p < .05. **p < .01. ***p < .001 (two-tailed).
Hierarchical Multiple Regression
Hierarchical multiple regression was performed to examine the relationship between the HBM scale, perceived social support, participant characteristics, and the willingness to participate in phase III clinical trials of new anti-cancer drugs (see Table 4). The VIFs of all variables were below 5, indicating that there was no significant multicollinearity among the independent variables. In Model 1, patients’ sociodemographic characteristics only explained 6.1% of the variance (F = 2.637, p < .001). In Model 2, a number of pre-existing conditions and treatments received were entered, and the amount of the total variance explained increased to 7.2% (F = 2.486, p <.001). Model 3 added three dimensions of perceived social support, and the variance explained increased by 10.4% (F =4.651, p < .001), in which only support from family members was the significant predictor (β = 0.202, p < .001). In the final Model 4, the entry of HBM predictors explained an additional 26.8% of the variance (F = 12.596, p < .001). Cues to action (β = 0.251, p < .001), self-efficacy (β = 0.281, p < .001), and perceived severity (β = 0.151, p < .001) were positive predictors of willingness to participate, while perceived barriers (β = −0.114, p = .027) were a negative predictor. The statistically significant p-values observed alongside relatively small standardized coefficients may reflect the increased statistical power afforded by the large sample size, suggesting modest but reliable effects.
Hierarchical Multiple Regression of HBM Variables, Social Support, and Cancer Patients’ Willingness to Participate in Phase III Clinical Trials for New Anti-Cancer Drugs.
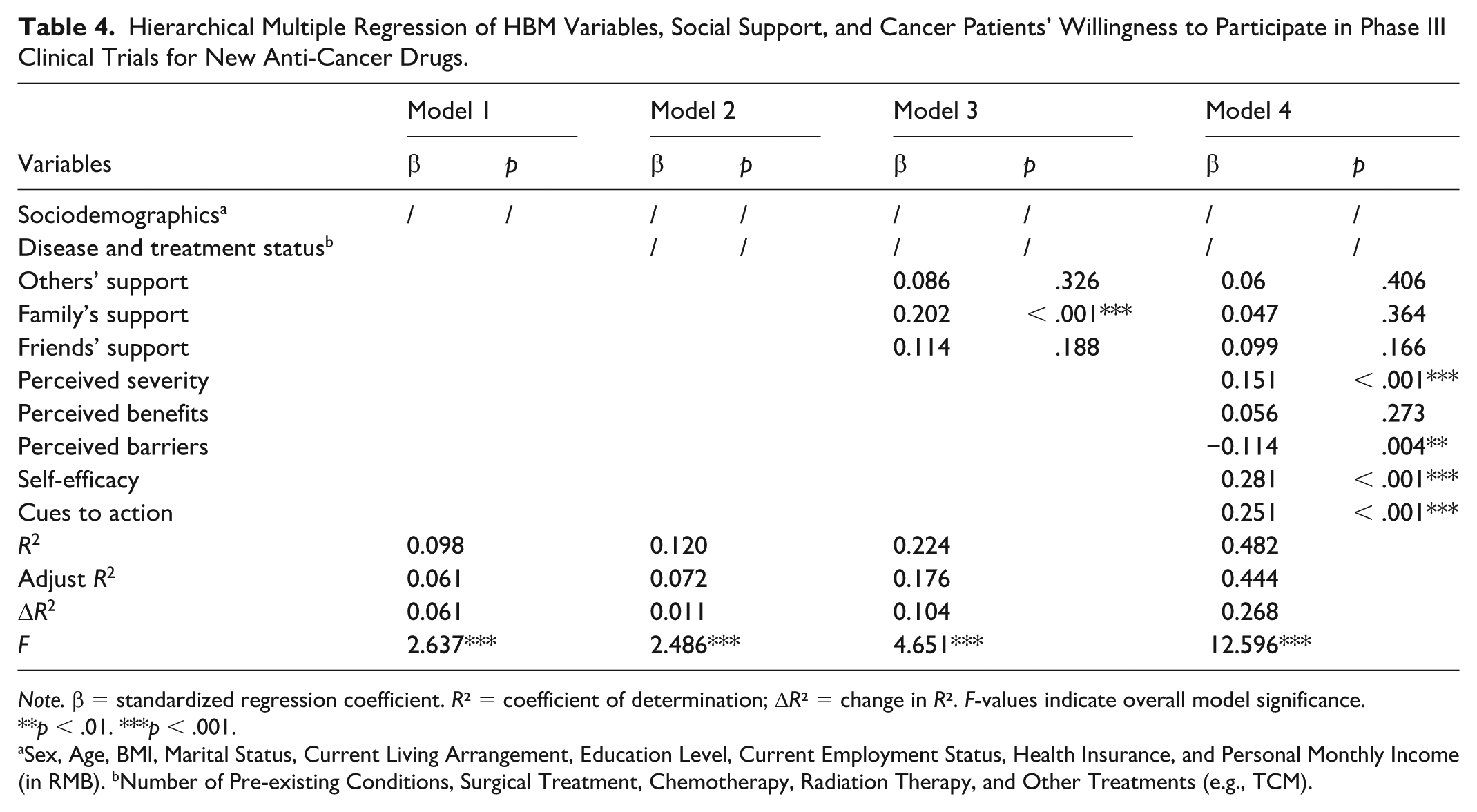
Note. β = standardized regression coefficient. R² = coefficient of determination; ΔR² = change in R². F-values indicate overall model significance.
p < .01. ***p < .001.
Sex, Age, BMI, Marital Status, Current Living Arrangement, Education Level, Current Employment Status, Health Insurance, and Personal Monthly Income (in RMB). bNumber of Pre-existing Conditions, Surgical Treatment, Chemotherapy, Radiation Therapy, and Other Treatments (e.g., TCM).
Discussion
Overall, participants exhibited a relatively low willingness to participate in clinical trials. Hierarchical multiple regression analysis revealed that, after controlling for sociodemographic factors and disease and treatment status, social support exerted an indirect influence, while perceived severity, perceived barriers, self-efficacy, and cues to action emerged as direct predictors of willingness to participate.
In this study, an analysis of the differences in patient’s willingness to participate under different sociodemographic factors found that there were significant differences in willingness to participate based on different living arrangements, with patients living with family or spouse having a higher willingness to participate. Living with family or spouse improves patients’ awareness of their conditions and boosts their sense of self-efficacy (Brito et al., 2021; Park et al., 2018). Employment status was associated with willingness to participate. While previous studies found that individuals who were employed part-time, not employed, or retired were less interested in participating in clinical trials than those employed full-time (Kim et al., 2024; Saphner, 2021), this study observed the opposite, with part-time workers demonstrating highest participation willingness. This may be due to greater flexibility in scheduling, fewer work-related constraints, or different risk-benefit perceptions compared to other groups. Economic factors were also significantly associated with patient’s willingness to participate in clinical trials. Contrary to earlier findings, patients with lower income were less likely to participate in a clinical trial for financial concerns (Unger et al., 2016). The results of this study differed, as the analysis revealed relatively high willingness among low-income patients, whereas high-income patients demonstrated significantly lower willingness. This difference may stem from variations in patients’ psychological expectations regarding treatment options. Low-income patients lack alternative treatment options and may view clinical trials as a critical opportunity to improve their health status. It is necessary to consider the plight of people living alone and on low incomes and how to overcome these barriers, for example, by providing transportation subsidies, arranging flexible trial times, strengthening community collaboration, simplifying the participation process, and disseminating trial information through multiple channels.
Patients who had never received other treatment such as TCM showed a higher willingness to participate than those who had. Previous treatment experience has been found to influence willingness to participate in clinical research, suggesting that patients with differing treatment backgrounds may weigh the benefits and risks of clinical trials differently (Thomas et al., 2022). Meanwhile, research on TCM acceptance indicates that willingness to choose TCM is strongly driven by personal experience, cultural norms, and beliefs rather than solely by evidence from randomized controlled trials (Y. X. Chen et al., 2025). These findings are consistent with this study, suggesting that patients who have received other treatments may be skeptical or resistant to drug clinical trials. Recruitment strategies should focus on targeted communication and support to alleviate these concerns and encourage trial participation.
Family and friends play a crucial role in influencing patients’ decisions to participate in clinical trials. Psychological interventions involving significant others can enhance patients’ perceived social support, increasing their willingness to participate in drug clinical trials (Gouveia et al., 2022). In this study, social support variables significantly improved the model’s explanatory power. Family support emerged as the only key predictor of willingness to participate in clinical trials, with a significant positive influence, while support from friends and others had no significant effect. This also explains why patients living with family members or spouse showed higher willingness to participate. Family members not only provide emotional encouragement but also offer practical assistance, such as accompanying patients to medical appointments, managing treatment-related logistics, and alleviating concerns about trial participation. In contrast, support from friends and others may be less impactful due to their limited role in medical decision-making and daily caregiving. However, in Model 4, social support was no longer significant, suggesting that its influence may be exerted indirectly through other dimensions of HBM. For example, social support can enhance self-efficacy and perceived benefits by providing verbal encouragement, modeling healthy behaviors, and facilitating mastery experiences (Kwok et al., 2025). Practical interventions could include family-inclusive counseling sessions to actively engage relatives in decision-making, targeted digital campaigns delivering tailored information and reminders, and peer support programs where experienced patients share participation experiences.
The HBM variables in the final model explained the largest portion of the variance in willingness to participate. Significant variables included cues to action, self-efficacy, perceived severity, and perceived barriers. Previous research showed a higher willingness to participate in clinical trials in cancer patients with higher perceived severity (King et al., 2025). Consistently, perceived severity was a positive predictor of willingness to participate in this study, and we found that patients with an urgent need for new treatment options had higher levels of perceived severity. Perceived benefits were not a positive predictor, however. Perceived barriers were a significant negative predictor of willingness to participate. A previous study reported that distrust of drug efficacy and concerns about adverse effects were the primary perceived barriers (Amin et al., 2020), which is consistent with the main barriers identified in this study. Indicating that transparent communication can help alleviate concerns about drug efficacy and side effects while providing simple, easy-to-understand guidance materials to enhance patient confidence. Willingness to participate in a clinical trial was influenced by an individual’s perceived self-efficacy beliefs. Patients with higher self-efficacy tend to feel more confident in their ability to manage the trial’s demands, including understanding the trial process and coping with potential side effects (Gouveia et al., 2022). Surveys of cancer patients who have already enrolled in clinical trials emphasize the critical role of the physician in recruitment (King et al., 2025; Moorcraft et al., 2016; You et al., 2025). Consistently, this study found that patients prefer receiving trial information from their physicians or hospitals rather than online advertisements. However, in some cases, surgical oncologists are reluctant to refer patients to drug trials due to limited knowledge of trial details or believe that treatment should not stray from protocol (Kumar et al., 2022; Monreal et al., 2025), which may create a barrier for cancer patients in accessing cues to action. Therefore, how physicians present, explain, and encourage patient enrollment in clinical trials plays a critical role in improving participation rates.
Prior studies have shown that HBM constructs—particularly perceived susceptibility, perceived benefits, and self-efficacy—predict engagement in cancer screening and preventive behaviors (Dewi et al., 2019; Jadgal et al., 2024; Saghafi-Asl et al., 2020). However, the strong influence of cues to action observed in our study may reflect the culturally embedded trust in medical authority within Chinese health care systems. This suggests that, while core HBM constructs remain robust across cultures, their relative salience and behavioral implications can vary depending on sociocultural norms and health care communication patterns. Future studies could further compare how cultural variations in patient–physician relationships or collective decision-making shape the motivational mechanisms predicted by HBM.
This study has several limitations. First, the sample did not differentiate between specific tumor types or stages, and the severity of cancer may influence willingness to participate, which could introduce bias and affect the results. Second, the use of online questionnaires may have led to some respondents having an incomplete understanding of the study, thus affecting the accuracy of their responses. Third, convenience sampling from online cancer communities introduces substantial selection bias—participants are likely more health-literate and internet-savvy than the general cancer population. Consequently, the generalizability of the findings is limited, and caution should be exercised when extending these results to all Chinese cancer patients. And the use of participation incentive might have introduced incentive-related bias by encouraging participation primarily for compensation or by eliciting more favorable responses toward clinical trial participation, thereby potentially affecting data validity. Finally, as a cross-sectional study, this study did not establish causal relationships between variables, suggesting that future experimental studies are needed to further clarify these associations.
Conclusion
This study utilizes the HBM framework and social support theory to identify the predictors of cancer patients’ willingness to participate in clinical trials of new anti-cancer drugs. The findings indicate that key HBM constructs, including cues to action, self-efficacy, perceived severity, and perceived barriers, are significantly associated with participation willingness, while family support plays an important contextual role. Targeting the key factors influencing participation, particularly cues to action and self-efficacy along with emphasizing the importance of family support, may contribute to significant improvement in patient participation rates in clinical trials. However, the findings are exploratory and not generalizable to all Chinese cancer patients.
Supplemental Material
sj-docx-1-heb-10.1177_10901981261450599 – Supplemental material for Chinese Cancer Patients’ Willingness for Phase III Trials: Health Belief Model and Social Support
Supplemental material, sj-docx-1-heb-10.1177_10901981261450599 for Chinese Cancer Patients’ Willingness for Phase III Trials: Health Belief Model and Social Support by Tantan Cheng, Hanlin Zhang, Shuruo Zhang, Bingqi Han, Yuxin Hao, Xinrui Shi, Jiwei Wang and Li Liu in Health Education & Behavior
Footnotes
Ethical Considerations
This study was approved by the Medical Research Ethics Committee of the School of Public Health, Fudan University (the international registry no. IRB00002408 & FWA00002399).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.