
Abstract
Cervical cancer remains a leading cause of mortality among women worldwide, particularly in low- and middle-income countries, yet human papillomavirus (HPV) vaccination—the most effective method of prevention—faces variable uptake and acceptance. This study addresses the problem of suboptimal HPV vaccination by examining the factors associated with parental consent for HPV vaccination of adolescent girls in two distinct Peruvian cities, the capital city of Lima and a large city in the Peruvian Amazon, Iquitos. Cross-sectional survey data were collected in 2017 from 986 women attending public health centers, and the Capability, Opportunity, Motivation, Behavior model was applied to categorize behavioral factors associated with women’s willingness to vaccine their daughters for HPV. Overall, 90.1% of women reported willingness to vaccinate their daughters, with higher support in Iquitos (94.2%) than in Lima (84.7%). Women who were willing to vaccinate tended to be younger and were more likely to believe the vaccine was safe (Capability), know that it was free and be willing to pay for it (Opportunity), and know someone who had been vaccinated (Motivation). This study contributes to the literature on parental willingness to vaccinate daughters against HPV in a Latin American context applying a validated behavioral framework. Findings provide insight into psychosocial and contextual factors associated with self-reported parental willingness to vaccinate daughters against HPV. The results have implications for public health research and practice by identifying modifiable barriers and facilitators that can inform targeted vaccine promotion strategies in Peru and similar settings, particularly in informing future vaccine promotion strategies in contexts where vaccine confidence may have shifted following the COVID-19 pandemic.
Introduction
Vaccination against human papillomavirus (HPV) is the most effective way to prevent cervical cancer, the eighth most common cancer worldwide, and the ninth most lethal (Ferlay et al., 2021; Lei et al., 2020; Pan American Health Organization, 2023). This preventable disease disproportionally affects women in low- and middle-income countries, where 94% of cervical cancer-related deaths occur (Fuady et al., 2024). Mirroring worldwide patterns, cervical cancer in Peru disproportionately impacts low-income women, Indigenous women, and women in remote and rural areas, and remains the leading cause of cancer-related death among Peruvian women (Ministerio de Salud del Perú, 2022a; Singh et al., 2012).
Countries throughout Latin America and other regions of the world have implemented strategies to promote HPV vaccination. In support of eliminating the disease by 2030, the World Health Organization (WHO) launched its 90-70-90 cervical cancer elimination initiative which set ambitious goals for vaccination, screening, and treatment (World Health Organization, n.d.). Despite these goals, vaccination coverage rates in Latin America are uneven and fluctuating, and overall, fall short of the regional target of 90% set by the Pan American Health Organization (Guzman-Holst et al., 2020; WHO, Pan American Health Organization [PAHO], n.d.). In 2020, vaccine coverage in Latin America ranged from 33% coverage in Colombia to 99% in Mexico, with 74% coverage in Peru (Nogueira-Rodrigues et al., 2022).
Peru’s Ministry of Health (MINSA) has promoted the HPV vaccine as a cervical cancer prevention strategy since 2011. As shown in Supplemental File A, the country’s vaccination strategy has evolved over time, beginning with the implementation of a three-dose regimen offered in schools to girls aged 10 to 15. Later in 2015, the strategy evolved to focus on fifth-grade girls aged 10 to 13 at school, at their homes, and in community vaccination facilities (Venegas Rodríguez et al., 2020). More recently, the national policies have expanded to include vaccinations for both girls and boys aged 9 to 18, one-dose regimens, and vaccination for women under 20 years old living with HIV (Ministerio de Salud del Perú, 2022b; Pan American Health Organization, 2023; Venegas Rodríguez et al., 2020). However, the latest available data show that first-dose coverage was only 79.7% in 2023, lower than the goal of 90% (Ministerio de Salud del Perú, 2025).
Despite integration into national policy, HPV vaccine uptake in Peru remains dependent on social and psychological factors. Previous research in Peru found that a lack of knowledge, uncertainty about vaccine efficacy, fear of side effects, misconceptions, discrimination, religion, and cost influence parental consent and HPV vaccination rates (Chaupis-Zevallos et al., 2020; Miles et al., 2021). These largely reflect worldwide barriers to parental consent; namely, the fear of side effects, limitations of written informed consent, misconceptions in mass media, and poor shared decision-making between spouses (Tsu et al., 2014). In contrast, parental willingness to vaccinate in Peru has been found to be positively associated with concepts of disease prevention combined with practical factors of the vaccine (i.e., provided at no cost and at schools) and credibility of the vaccine supported by trusted authority figures such as health care personnel (Bartolini et al., 2012).
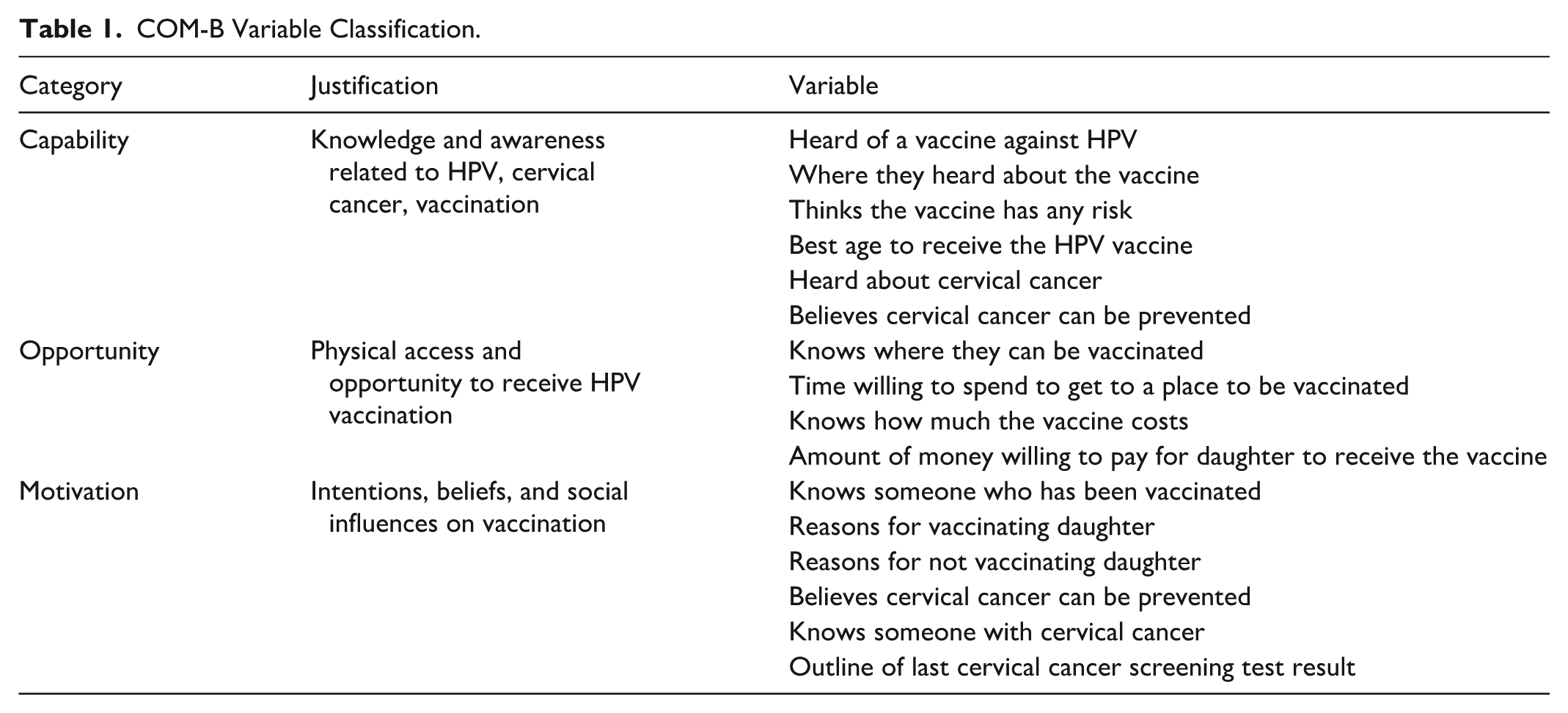
The Capability, Opportunity, Motivation Behavior (COM-B) behavioral model offers a helpful framework for understanding factors associated with parental willingness to vaccinate their children (Flood et al., 2024; Marshall et al., 2023). According to the COM-B model, people must be physically and cognitively able to take action (Capability), have the necessary physical and social means to access the action (Opportunity), and have the necessity or desire to perform that behavior over any other behaviors (Motivation) (Michie et al., 2011; West & Michie, 2020). Together, these components are theorized to interact and influence each other as part of a dynamic system, ultimately leading to the desired behavior (Michie et al., 2011; West & Michie, 2020). Examining variables within the COM-B framework can identify key behavioral factors associated with parental willingness to vaccinate daughters against HPV.
This study uses the COM-B model to understand specific barriers and facilitators of parental willingness to vaccinate their daughters against HPV in two large cities in Peru. Descriptive statistics were used to (a) compare women who were willing to vaccinate their daughters to those who were not and (b) examine differences across two distinct cities. This study aims to inform effective place-based tailored and national implementation strategies in Peru to address HPV vaccination barriers and achieve national cervical cancer prevention goals.
Method
Study Design and Instrument
Cross-sectional survey data collected by Proyecto Precancer (U01 CA190366-A01) were used for this study. Proyecto Precancer is an implementation science project composed of an interdisciplinary team of researchers, health professionals, and health authorities from various Peruvian and U.S. institutions, including U.S. universities, the U.S. National Cancer Institute, a Peruvian nongovernmental health and development organization, and the regional and national Ministries of Health focused on preventing cervical cancer through a new HPV-based screen-and-treat strategy. At the start of the project, the team administered a cross-sectional knowledge, attitudes, and practices (KAP) survey to assess cervical cancer prevention knowledge and practices in the community, focusing on HPV vaccination, and cervical cancer screening, treatment, and follow-up. Most questions were close ended. See Supplemental File B for the survey instrument (in Spanish).
Study Setting
Proyecto Precancer administered the survey in 2017 to women aged 18 to 65 living in Lima, Peru’s capital city (estimated population 11M), and Iquitos, a city in the Peruvian Amazon rainforest (estimated population ~450K). Both populations have vastly different geographical, cultural, and socioeconomic characteristics relevant to cervical cancer (Paz-Soldán et al., 2012), as well as access to health care services.
Study Subjects
A total of 1,227 women participated in the study across Lima (n = 608) and Iquitos (n = 619). Each health network comprises multiple health facilities serving a defined geographic area or “catchments,” Proyecto Precancer purposively selected five catchments within a single health network in each city to capture heterogeneity in population characteristics (rural, urban, and peri-urban in one city; urban and peri-urban in the other).
Within these catchments, survey teams employed systematic household sampling, selecting every sixth household per block starting on a corner house. Screen-eligible women aged 18 to 65 years were invited to participate. Although Peruvian screening guidelines recommend initiation at age 25, women aged 18 to 24 were included because some may have received HPV vaccination or undergone screening while pregnant. Participants were selected from the general population of these two health networks, which represented mostly women below the poverty line, with approximately 75% to 80% covered by the public health insurance program (Seguro Integral de Salud or SIS; Ministerio de Salud del Perú, n.d.).
The survey was administered once, lasted approximately 30 minutes, and assessed KAPs associated with cervical cancer, its prevention and treatment, cervical Pap smears, and the HPV vaccine, as well as sociodemographic characteristics of the sample. The target sample was 600 women per city (120 per area).
Paper-based surveys were administered by an interviewer in Spanish. To minimize interviewer bias, all survey administrators were trained using a standardized protocol. Each city’s team had a research coordinator to ensure using the same recruitment process and to check for quality control. For security reasons in both sites, the surveys were administered with paper and pencil by trained field staff, and data were entered into an Access database.
Given this study’s focus on understanding the willingness of women to vaccinate their daughters, women who reported that they did not have daughters (n = 241) were excluded from the analysis. After removing these noneligible women, there were 986 women in the analyzed cohort, with 43.7% of the women from Lima (n = 431) and 56.3% of the women from Iquitos (n = 555).
Study Variables
The primary dependent variable was parental willingness to vaccinate their daughters (the Behavioral variable in the COM-B model). The survey assessed self-reported willingness to vaccinate daughters against HPV and did not measure actual vaccine uptake or verified vaccination status. Women who reported unwillingness to vaccinate their daughter(s) (n = 60) were combined with women who did not know if they were willing to vaccinate their daughter(s) (n = 34). Survey questions were separated into four categories: sociodemographic variables, capability variables (C), opportunity variables (O), and motivation variables (M) (Table 1). Sociodemographic variables were analyzed by city and parental willingness, and the COM-B variables were analyzed by parental willingness.
COM-B Variable Classification.
Statistical Analyses
Descriptive statistics were computed to characterize socioeconomic demographics, health care-related variables, and KAP responses. Chi-square and student’s t-tests were used to compare women who reported willingness to vaccinate their daughters with women who reported unwillingness or uncertainty about vaccinating their daughters.
All analyses were conducted in R (R version 4.4.2). Surveys were not missing data on key variables and no imputation was performed. Statistical tests were two-tailed with p < .05. Continuous data were presented as means and SD, while categorical data were displayed as frequencies and percentages. Group comparisons were performed using Pearson’s chi-square and Welch’s two-sample t-tests. Welch’s t-test was used as a conservative approach to avoid reliance on the equal-variance assumption across groups. No adjustment for multiple comparisons nor multivariable regression analysis was performed because analyses were exploratory and intended to identify patterns for future hypothesis-driven research.
Ethical Considerations
The study was approved by the Institutional Review Boards of the Peruvian nongovernmental organization PRISMA (CE0251.09) and Tulane University (16–891039IAA). All procedures were followed in accordance with ethical standards, and informed verbal consent was obtained from participants as participants’ data were collected in the absence of special personal identifiers.
Results
Sociodemographic Characteristics, by City
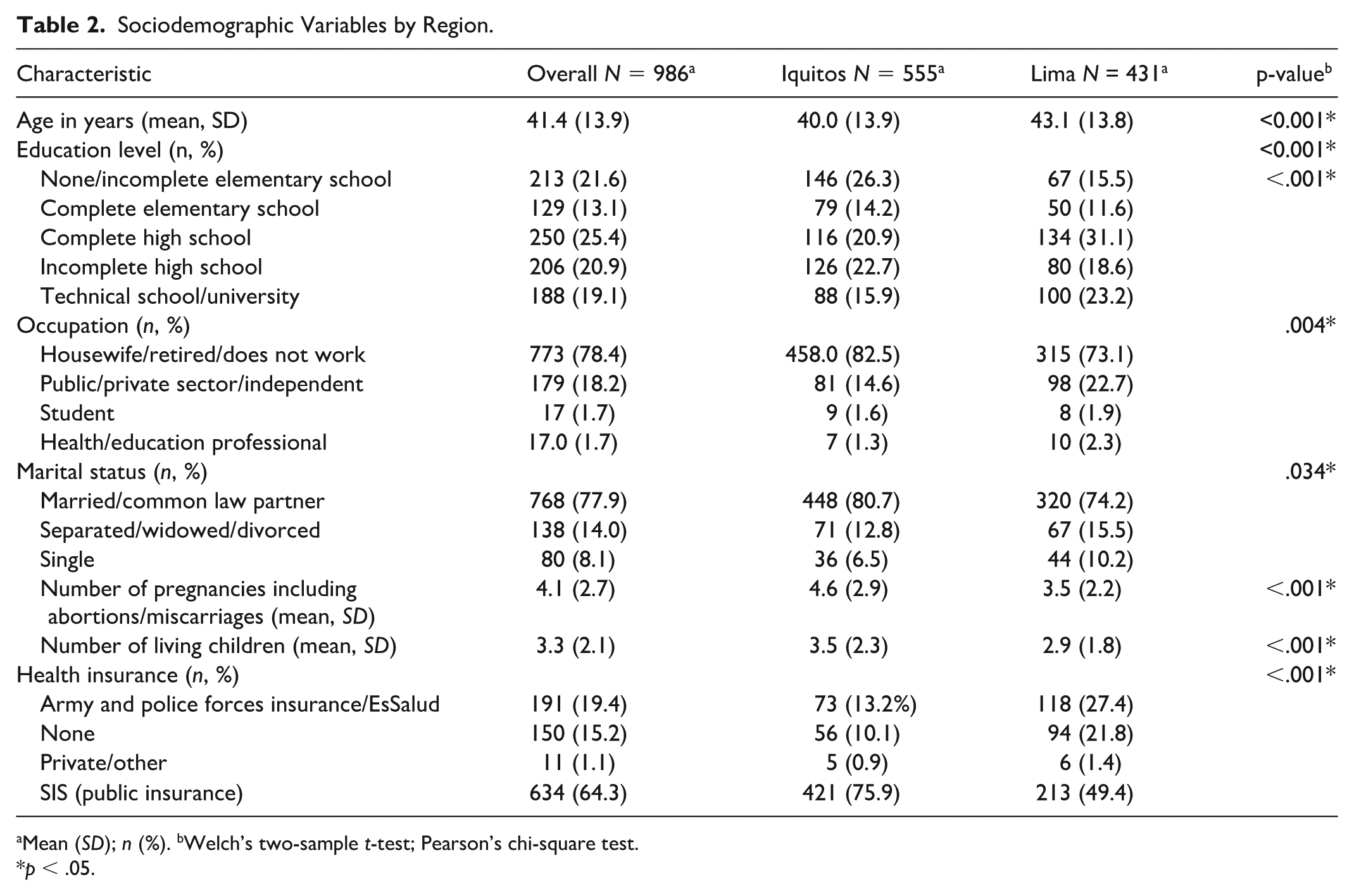
Sociodemographic characteristics of women in the cohort were different across cities (see Table 2). Overall, the average age of the women was 41.4 years (SD = 13.9). Women from Lima were slightly older, more educated, and likely to be employed than those in Iquitos. Most women in both cities were married or in a common-law marriage, but women in Lima were more likely to be single and have fewer children and pregnancies than those from Iquitos. Most women (64%) participated in the country’s Integral Health Insurance (SIS) program; there were more women from Iquitos with SIS than from Lima. Differences detected between women in both cities were significant at the 95% confidence level.
Sociodemographic Variables by Region.
Mean (SD); n (%). bWelch’s two-sample t-test; Pearson’s chi-square test.
p < .05.
Differences by Willingness to Vaccinate Their Daughters
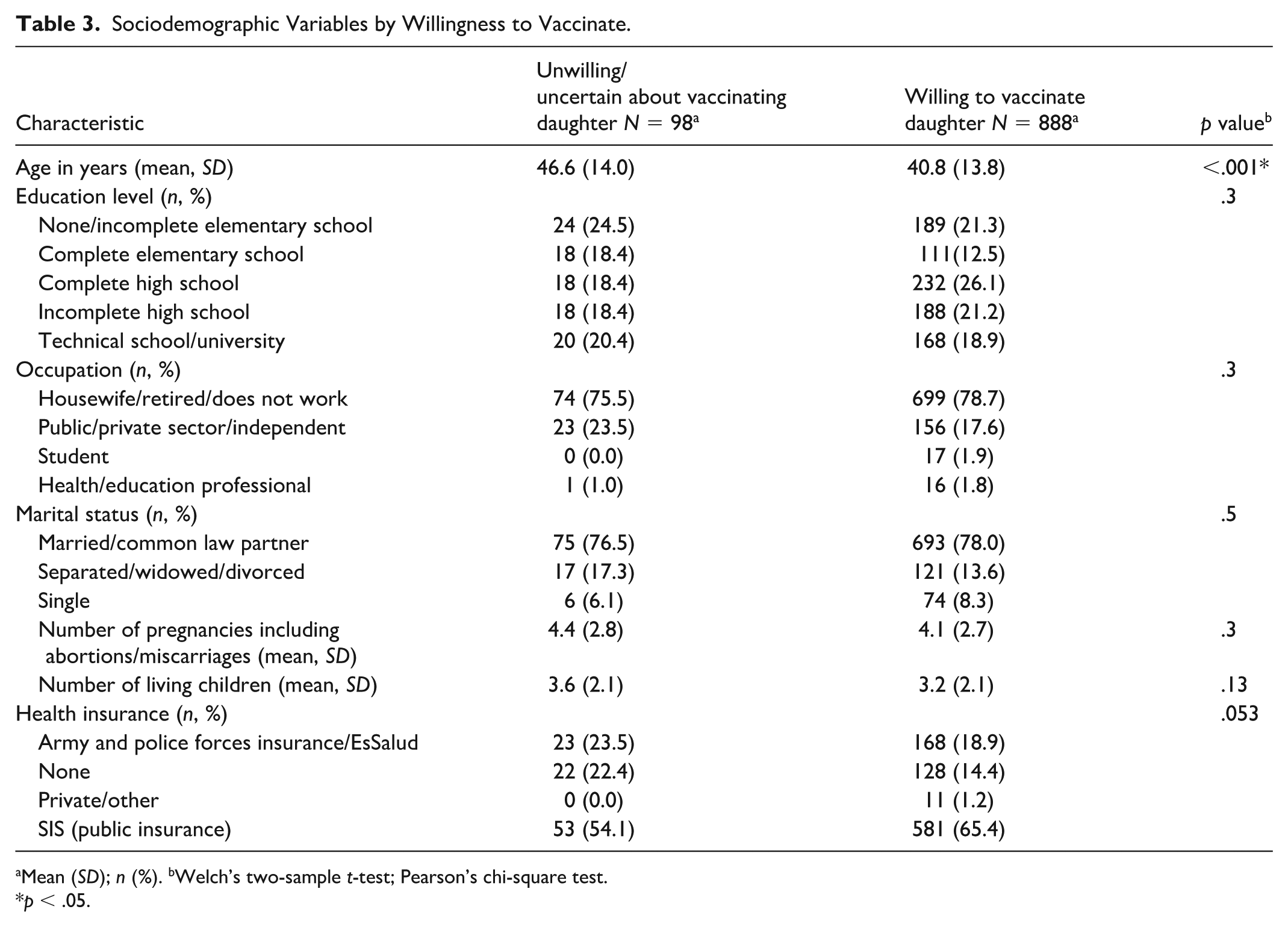
A great majority (90.1%) of women reported willingness to vaccinate their daughters against HPV, with women in Iquitos more willing to vaccinate their daughters than those from Lima (94.2% vs. 84.7%) wTable 3illing to vaccinate their daughters than those from Lima (94.2% vs. 84.7%). Table 3 provides demographic characteristics by willingness to vaccinate daughters against HPV.
Sociodemographic Variables by Willingness to Vaccinate.
Mean (SD); n (%). bWelch’s two-sample t-test; Pearson’s chi-square test.
p < .05.
Women who were willing to vaccinate their daughters against HPV were similar to women who were not willing to vaccinate their daughters. Both groups had similar rates of working outside of the home and being married or in a common-law marriage. Women who were willing to vaccinate their daughters had on average fewer pregnancies and live children compared with women who were not willing to vaccinate their daughters. Women who reported willingness to vaccinate their daughters were also more likely to be younger and more likely to have slightly higher education levels than their less willing counterparts. They were also more likely to have SIS (public insurance) and less likely to have other insurance compared with their nonsupportive counterparts. Only age was statistically significant across these groups: the mean age of women reporting willingness to vaccinate their children was 40.8 years, compared with the mean age of women reporting not being willing to vaccinate who were 46.6 years (p < .001).
Capability-Related Variables
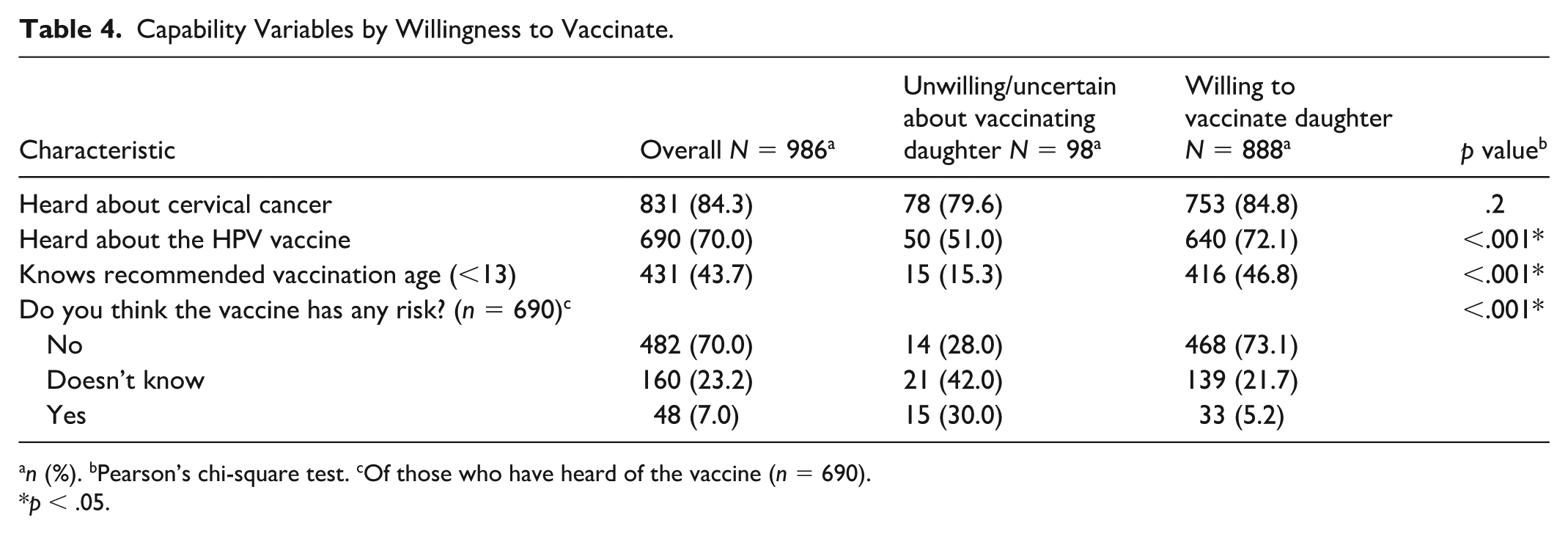
Women who were willing to vaccinate their daughters scored higher on capability variables (see Table 1 for description of variables) than women who were not (see Table 4). These women were more likely to have heard about the HPV vaccine (72.1% vs. 51%). Women who were willing to vaccinate their daughters were also much more likely to believe that the vaccine did not pose any risks and know that the best age to be vaccinated was before 13 years old, which aligned with the national strategy at the time of the survey. These women were also more likely to have heard about cervical cancer than women not willing to vaccinate their daughters, although this difference was not statistically significant.
Capability Variables by Willingness to Vaccinate.
n (%). bPearson’s chi-square test. cOf those who have heard of the vaccine (n = 690).
p < .05.
Opportunity-Related Variables
Women across the cohort had relatively low levels of knowledge about opportunity variables (see Table 1 for variables included). Women had limited knowledge on one of the two main outreach strategies used for HPV vaccination for girls at the time of the study: door-to-door visits (see Table 5). However, women who supported vaccination were more likely to know that vaccines were available at schools than those who did not support vaccination. Less than a third (28%) of women knew the vaccine was free, with women who were willing to vaccinate their daughters more likely to know that than their counterparts. Looking at willingness to pay for the vaccine, there was some divergence among mothers willing to vaccinate their daughters: there were similar proportions of mothers who were not willing to pay any amount to get their daughters vaccinated (14.8%) and mothers who were willing to pay more than 50 soles (U.S.$15.34 in 2017) to vaccinate their daughters (14.9%). Women who were not willing to vaccinate their daughters were not asked about willingness to pay for the vaccine.
Opportunity Variables by Willingness to Vaccinate.
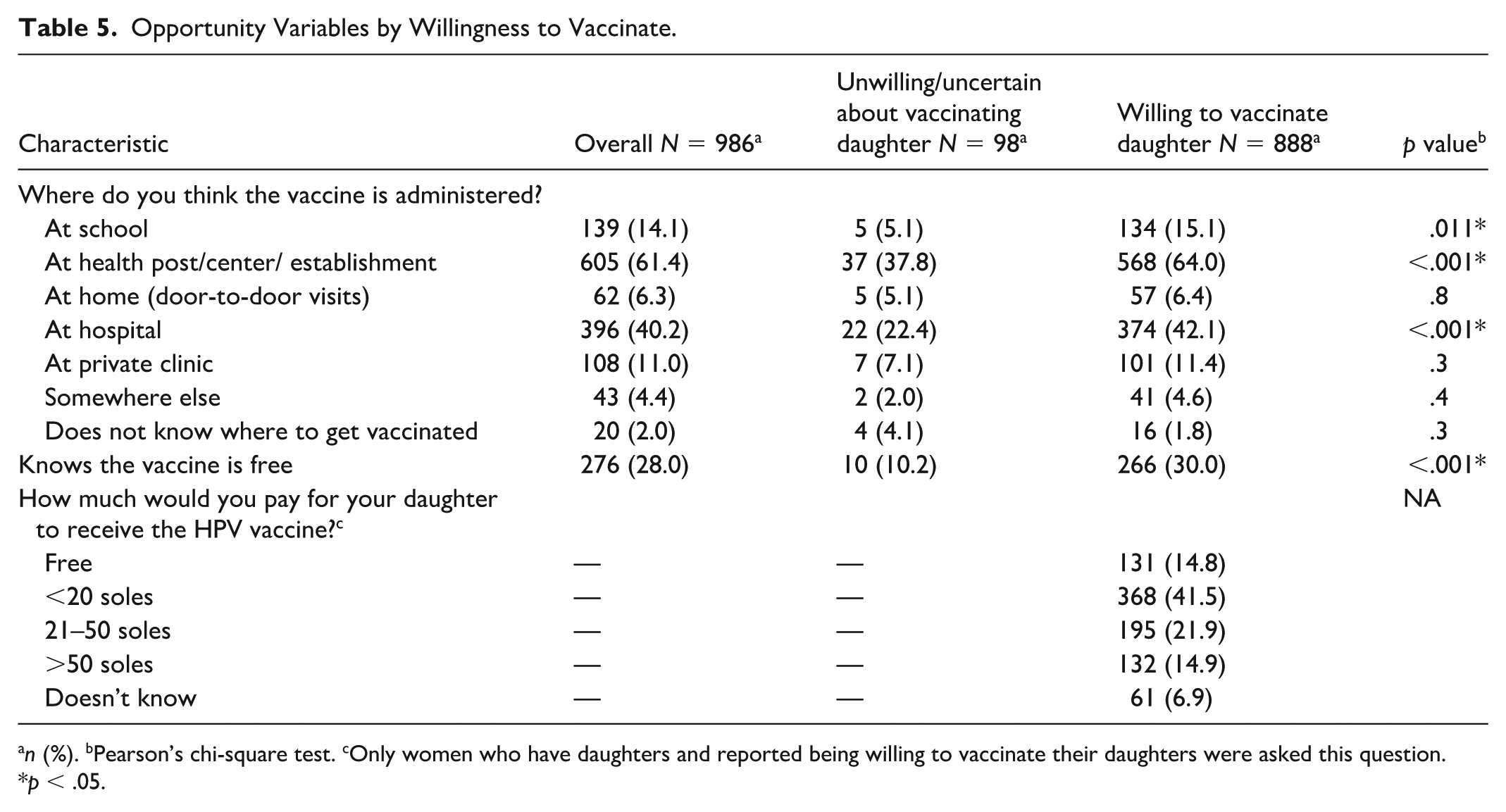
n (%). bPearson’s chi-square test. cOnly women who have daughters and reported being willing to vaccinate their daughters were asked this question.
p < .05.
Motivation-Related Variables
The primary reason women reported willingness to vaccinate their daughters was to prevent HPV infection (see Table 6). Willingness to vaccinate among women was statistically associated with knowing someone who had been vaccinated. Reasons given to not vaccinate daughters were more complex; there was no single factor. While fear of side effects and believing the vaccine was unnecessary were cited concerns, nearly a third reported another reason.
Motivation Variables by Willingness to Vaccinate.
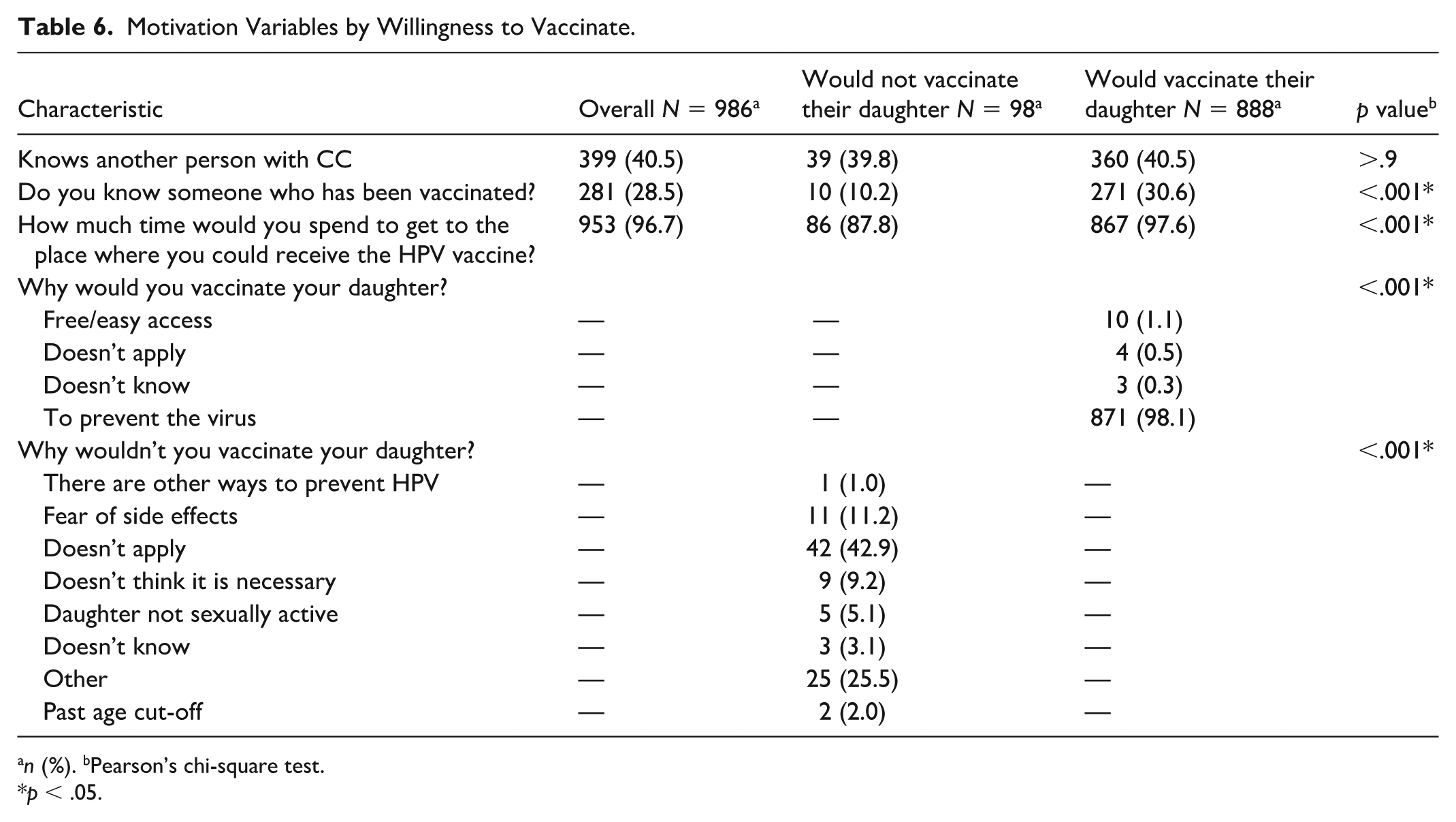
n (%). bPearson’s chi-square test.
p < .05.
Differences Observed by Cities
Differences were observed in mothers’ willingness to vaccinate their daughters in Lima and Iquitos. Associated with the Capability variables, mothers who reported willingness to vaccinate their daughters in Lima were more likely to have heard about cervical cancer (87.7%) and the HPV vaccine (78.9%) than women in Iquitos (82.8% and 67.3%, respectively). For the Opportunity variables, “vaccine supportive” mothers in Lima were slightly more likely to know that the vaccines are available at schools and home through door-to-door visits, whereas mothers reporting willingness to vaccinate their daughters in Iquitos were more likely to know that the vaccines were available at no cost compared with these women in Lima (37.3% vs. 18.9%). Despite overall lower educational and economic status in Iquitos, vaccine supportive women there reported being more willing to pay for the vaccine (82.6%) compared with these women in Lima (72.3%). Finally, examining the Motivation variables, vaccine supportive women in Lima were slightly more likely to know someone who received the HPV vaccine (34.1%) compared with vaccine supportive women in Iquitos (28.1%). Despite these differences, women from both cities were similarly motivated by the vaccine’s ability to prevent HPV (97.5% and 98.5%).
Discussion
Understanding parental willingness to vaccinate their daughters against HPV is critical for cervical cancer prevention efforts, especially in low-resource countries where screening and treatment programs have not been as effective—for multiple reasons including implementation challenges—than higher-income countries. Peru has not yet achieved the WHO’s recommendation of 90% of young women vaccinated by the age of 15 years, despite the wide availability of the HPV vaccine and the implementation of national strategies. Identifying factors associated with parental willingness to vaccinate their daughters can inform interventions that improve coverage (and as of 2025, young men can also be vaccinated for free as part of the national strategy), particularly in settings with diverse sociodemographic and geographic challenges.
The study revealed that most mothers in both cities supported HPV vaccination of their daughters, primarily because of its role in preventing HPV infection. These results are consistent with previous research suggesting that parental acceptability may influence vaccine uptake (Xie et al., 2023) and the role of safety concerns of the vaccine in willingness to vaccinate (Salazar-Valdivia et al., 2024). Nearly, all mothers reporting willingness to vaccinate were motivated by the opportunity to prevent HPV. Importantly, the high levels of stated parental willingness observed in both cities contrast with Peru’s persistent gaps in HPV vaccine coverage. This discrepancy suggests that incomplete HPV vaccine coverage may reflect operational, structural, and health-system barriers that limit consistent vaccine delivery and access more than lack of parental willingness to vaccinate daughters. These findings reinforce the importance of distinguishing between parental willingness to vaccinate daughters and the health-system factors necessary to achieve high vaccination coverage.
Using the COM-B model, the study identified characteristics associated with a mother’s willingness to vaccinate her daughters. Women who believed the vaccine was safe and knew the recommended vaccination age were more likely to support vaccination (Capability). Knowledge that the vaccine was free and willingness to pay for vaccination were both associated with parental support for HPV vaccination (Opportunity). Women who knew someone who had received the HPV vaccine and wanted to prevent the virus were more likely to support vaccination (Motivation). These variables were consistent across both cities, despite sociodemographic differences.
Women who reported unwillingness to vaccinate their daughters cited various reasons, including fears about potential side effects of the vaccine; belief that the vaccine was not necessary; or not knowing or having a clear reason for not wanting to vaccinate their daughters. The lack of dominant reasons for not supporting vaccination emphasizes the dynamic nature of attitudes toward HPV vaccination, underscoring the complexity of parental decision-making for vaccinations (Salazar-Valdivia et al., 2024).
This study is among the first in Peru to apply the COM-B behavioral model to explore parental willingness to vaccinate daughters against HPV. By comparing a large dataset of women in two distinct cities with differing awareness and vaccine uptake, the study illustrates how behavioral drivers interact with local context. The only other COM-B-based study on parental support of HPV vaccination to date was conducted in Greece (Efkarpidis et al., 2024), highlighting the uniqueness of our work in a Latin American context. Other recent research on parental support of HPV vaccination in Peru was limited to the capital city or small sample sizes (Barja-Ore et al., 2025; Juárez-Leon et al., 2025).
The comparison of COM-B variables in two large cities suggests that tailored and place-based interventions may be beneficial. In Lima, where awareness of cervical cancer is higher but willingness to vaccinate is lower, public health messaging strategies could focus on addressing specific misconceptions of vaccine risk, emphasizing the vaccine’s safety, highlighting the prevalence of vaccine uptake in their communities, and reminding them that the vaccine is free. In Iquitos, where willingness to vaccinate is quite high, findings suggest that implementation and vaccine availability may warrant greater attention than educational components to increase parental support. A place-based approach also addresses other differences in the cities beyond sociodemographic factors studied in this paper that may be influencing parental support, such as cultural and traditional beliefs about gender and medicine, geographic access to health care and information, and historical trust in the government and federal health authorities.
Globally, parental willingness to vaccinate their children for HPV differs widely, with one estimated range of 12% to 97.5% (Heyde et al., 2024). Compared with limited data from neighboring Latin American countries, parental willingness observed in this study appears relatively high, consistent with findings from Argentina and Brazil included in a recent meta-analysis (Heyde et al., 2024). Compared further across other limited-resourced countries such as those in Sub-Saharan Africa, this study found a slightly higher acceptance rate with similar associations of younger parents, higher education, and knowledge as factors to stronger support of the HPV vaccine (Asmelash et al., 2025). Other research, conducted in various contexts such as Kazakhstan and the United States, reveals that a mother’s support may be associated with their refusal or acceptance of their own HPV vaccination (Babi et al., 2023; Gray & Fisher, 2023). However, as in other regional and middle- and higher-income settings, gaps between stated willingness and actual vaccine uptake persist, suggesting that structural and operational barriers to vaccine access remain a greater challenge than parental willingness.
Despite high reported parental willingness to vaccinate daughters against HPV, Peru has not achieved the WHO-recommended vaccination target. This divergence between high acceptability and incomplete coverage suggests that barriers beyond parental attitudes continue to affect vaccine uptake. Data collection for this survey took place in 2017, 6 years after the launch of the national HPV vaccination program and during implementation of the national school-based strategy (Venegas Rodríguez et al., 2020). While Peru’s overall coverage rate of girls aged 15 years has increased since 2017, and as of 2025 also includes boys, there is still a gap between the existing HPV vaccine coverage rate for the first dose for girls aged 9 to 13 years old in 2023 (78%) and the coverage goal (90%) (World Health Organization, n.d.). This gap persists despite broad parental willingness, suggesting that structural and systemic barriers continue to limit vaccine coverage. Specifically, the persistence of vaccine disparities observed in Peru echoes previous findings in cervical cancer prevention, which showed that women in Iquitos overwhelmingly want HPV screenings and treatment for cervical cancer, but they face intersecting and systemic barriers to accessing these services (Morse et al., 2023). These findings suggest a similar pattern: mothers in Lima want their daughters to be vaccinated but may be limited by existing and deeply rooted barriers in the public health system.
Such findings must also be considered in a post-COVID-19 context. Peru was particularly affected during the COVID-19 pandemic with one of the highest rates of mortality in Latin America and the highest rate of incidence per million in the world (Schwalb & Seas, 2021). Both the public and vulnerable populations suffered from a lack of prepared infrastructure, leadership, and investment in the public health system (Vázquez-Rowe & Gandolfi, 2020). Peruvian children were out of school for approximately 2 years from March 2020 to March 2022, and girls in rural areas, including throughout the Amazon rainforest, faced great challenges during that time including a lack of health care (Woodson et al., 2024).
As a result of school closures and broader social concerns regarding the COVID-19 virus, including the school-based HPV vaccination strategy, HPV vaccination rates fell greatly during that time. Rates of HPV vaccination decreased by 16.7% in 2020 and 29.8% in 2021 compared with 2019 (Parellada et al., 2023). Although the government restarted vaccinations again in March 2022, research has projected that it would take several years to catch up to 2019 coverage levels (Parellada et al., 2023). In addition, anti-vaccine messages against the COVID-19 vaccine may have eroded trust in public health institutions and vaccination (Salazar-Valdivia et al., 2024). This is particularly concerning given our finding linking willingness to vaccinate with perceptions of vaccine risk. The residual effects from the COVID-19 pandemic combined with uneven vaccination coverage may jeopardize Peru’s future success of achieving its vaccination goals.
These findings should be considered in light of their limitations. While the survey instrument was designed and reviewed by experts and piloted with women to ensure their comprehension, it was not formally validated. Participants were predominantly low-income women receiving care within the public health system and were drawn from both rural and urban settings. These characteristics should be considered when interpreting the findings and their generalizability. The survey design focused on parental willingness for daughters and did not capture information for sons (who at that time did not have access to publicly funded HPV vaccination) or future children if the mother did not have a daughter at the time of the survey (to avoid including hypothetical responses). The individuals surveyed only included mothers since this was part of a larger survey about cervical cancer prevention and control applied only to women. In addition, the interviewer-administered nature of the survey may have introduced social desirability bias, particularly given that HPV vaccination is widely promoted as a socially desirable preventive behavior within the public health system. As a result, stated willingness to vaccinate daughters may have been overestimated. Recall bias may also have influenced responses to prevention-related questions. In addition, the study measured stated willingness to vaccinate daughters rather than confirmed vaccination behavior, and therefore findings may not directly reflect actual vaccine uptake. Despite these limitations, these findings present important insights for policy and intervention planning in Peru, especially in a post-COVID-19 context.
From a public health perspective, this study suggests that increasing HPV vaccination coverage in Peru is likely to benefit from tailored, place-based interventions that extend beyond education alone. The high levels of parental willingness observed in both cities indicate that improving coverage may depend less on changing attitudes and more on strengthening implementation strategies, access, and continuity of vaccine delivery. Local and regional efforts to strengthen trust in vaccine safety, ensure reliable access through schools and health facilities, and address structural barriers are essential for translating high parental willingness into sustained vaccine uptake.
Supplemental Material
sj-docx-1-heb-10.1177_10901981261455312 – Supplemental material for Factors Associated With Parental Willingness to Vaccinate Daughters Against Human Papillomavirus in Peru
Supplemental material, sj-docx-1-heb-10.1177_10901981261455312 for Factors Associated With Parental Willingness to Vaccinate Daughters Against Human Papillomavirus in Peru by Astrid Wagner, Emily J. Johnson, Cecilia Montes, Jhonny J. Córdova López, Joanna Brown, Patti E. Gravitt and Valerie A. Paz-Soldan in Health Education & Behavior
Supplemental Material
sj-docx-2-heb-10.1177_10901981261455312 – Supplemental material for Factors Associated With Parental Willingness to Vaccinate Daughters Against Human Papillomavirus in Peru
Supplemental material, sj-docx-2-heb-10.1177_10901981261455312 for Factors Associated With Parental Willingness to Vaccinate Daughters Against Human Papillomavirus in Peru by Astrid Wagner, Emily J. Johnson, Cecilia Montes, Jhonny J. Córdova López, Joanna Brown, Patti E. Gravitt and Valerie A. Paz-Soldan in Health Education & Behavior
Footnotes
Acknowledgements
The authors thank the participants of this study who took the time to complete the surveys. The authors also recognize the members of the
Author’s note
Patti E. Gravitt is now affiliated to Georgia Cancer Center, Augusta University, Augusta, GA, USA.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was received through the National Institutes of Health/National Cancer Institute (Grant ID: R01-CA190366, mPI to P.E. Gravitt/V.A. Paz-Soldan, and U01-CA190366, mPI to J.K. Tracy/V.A. Paz-Soldan).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.