
Abstract
Family-based interventions may reduce the risk of acquiring HIV and other sexually transmitted infections (STIs) among Black girls in the United States, but few have engaged Black male caregivers. We examined key implementation outcomes of IMAGE, IMARA for Black Male Caregivers, and Girls Empowerment, an adapted evidence-based intervention for Black girls (13–18 years old) and their male caregivers. We conducted a pilot test of IMAGE with 40 girl-male caregiver dyads, using a pre-post-test design at baseline and 1-month follow-up. We assessed four implementation outcomes: feasibility, acceptability, appropriateness, and fidelity. Descriptive statistics were used to evaluate the change from baseline to 1-month follow-up for girls and their male caregivers. Feasibility was strong; 87% of those approached agreed to participate, and 93% completed the intervention. Acceptability was also high, with more than 75% of girls and male caregivers reporting being extremely satisfied with IMAGE, and 76% of participants feeling there was an appropriate amount of time spent on the topics. Intervention fidelity, as rated by observers, was 98%. At 1-month follow-up, girls and male caregivers endorsed improvements in their relationship, namely closeness and communication. IMAGE is a promising program designed to protect and reduce transmission of HIV and STIs among Black girls. We found strong evidence of feasibility, acceptability, appropriateness, and fidelity; therefore, a fully powered randomized controlled trial is warranted.
Introduction
HIV remains a persistent public health problem in the United States that disproportionately impacts Black girls and women. In 2021, Black women accounted for 54% of new HIV infections in the United States despite making up less than 15% of the female population (Centers of Disease Control and Prevention [CDC], 2022a). Compared to women of all other races and ethnicities, 91% of Black women’s new HIV infections were attributed to heterosexual contact (CDC, 2022). Rates of sexually transmitted infections (STIs) such as chlamydia, gonorrhea, and syphilis are rising, with the greatest increases in Black girls and women aged between 15 and 24 (Campbell & Stockman, 2024; CDC, 2022b). In Chicago, Illinois, STI rates are highest among Black girls between the ages of 13 and 29, and they represent 56% of new HIV diagnoses (Chicago Department of Public Health, 2022). Black girls are disproportionately impacted by sexual violence, as one in four will be sexually abused before the age of 18 (Brinkman, 2018; Klot et al., 2013). Taken together, Black girls are navigating overlapping public health crises, including HIV, STIs, and sexual violence, that call for targeted interventions to ensure their safety and protection.
Previous studies have identified several structural determinants of health contributing to poor HIV/STI outcomes among Black girls in the United States (Centers of Disease Control and Prevention, 2022; National Institute on Minority Health and Health Disparities, 2023). The Becoming a Sexual Black Woman framework underscores the impact of structural determinants of health (racism, discrimination, sexual violence, stereotyped messages, and adultification) on Black female development and highlights factors that impede the protection of Black girls’ sexual development pathways, sexual health, and decision-making (Crooks et al., 2019). One such factor, the adultification of Black girls, amplifies their vulnerability to early sexual debut (i.e., having sex at or before the age of 14 years) and low condom use, thereby increasing their susceptibility to HIV and STIs (Epstein et al., 2017; Pflieger et al., 2013). In the United States, incidents of HIV/STI infections among Black girls surpassed every other racial-ethnic group and continue to rise among adolescents and young adults aged 13 to 24 (Bosh, 2021). The reality is that ending the HIV epidemic requires addressing deep-rooted social and structural factors and developing community-led and culturally tailored interventions for Black girls and women (Campbell & Stockman, 2024; Rajabiun, 2025).
Families are uniquely positioned to protect Black girls and eliminate persistent racial disparities in HIV and STIs among Black females because they can directly address sociocultural conditions that influence Black sexual and reproductive health (Crooks et al., 2024; Donenberg et al., 2012; Johnson & Briggs, 2021). While several family-based HIV/STI interventions engage female caregivers (Aronowitz et al., 2015; Dancy et al., 2009; Donenberg et al., 2020), Black men offer a distinct form of protection for girls (Dorsey, 2022; Hutchinson & Cederbaum, 2011; Rostad et al., 2014) and have been underrepresented in HIV/STI prevention programming. Prior research indicates that Black girls want to receive SRH information from male caregivers, noting their unique perspectives as men (Crooks et al., 2024; Hutchinson & Cederbaum, 2011; Johnson & Briggs, 2021; Rostad et al., 2014). Further, evidence shows that the presence of Black male caregivers delays sexual debut and increases condom use among sexually active adolescents (Burns, 2008; Guilamo-Ramos et al., 2012; Johnson & Briggs, 2021; Randolph et al., 2017, 2019; Wight & Fullerton, 2013). Engaging male caregivers helps to address harmful gender norms, foster respectful relationships, and empower men as active participants in Black girls’ development and positive role models to more effectively address sexual violence and HIV/STI prevention efforts (Johnson & Briggs, 2021).
Informed, Motivated, Aware, and Responsible Adolescents and Adults (IMARA) is an evidence-based HIV/STI prevention program for Black girls (14–18 years old) and their female caregivers (mothers, aunts, grandmothers) in Chicago (Donenberg et al., 2020). IMARA combines three evidence-based interventions (Brown et al., 2014; Collins et al., 2007; DiClemente, 1995) and utilizes interactive activities to strengthen girls’ condom use through improved caregiver-girl communication and HIV/STI prevention skills (Donenberg et al., 2020). Results from a 2-arm, randomized controlled trial revealed a 43% reduced risk of acquiring a new STI among girls who received IMARA compared with those who received a time-matched health promotion program at 1-year follow-up (Donenberg et al., 2020).
Building on IMARA, the current study used the ADAPT-ITT model to guide a rigorous adaptation process (Wingood & DiClemente, 2008). As detailed elsewhere (Crooks et al., 2023), community-based qualitative methods were employed to systematically tailor IMARA for Black girls and Black male caregivers (BMC) (fathers, grandfathers, brothers, male cousins). The adapted intervention is called IMAGE: IMARA for Black Male Caregivers and Girls Empowerment (Crooks et al., 2023).
Researchers are increasingly incorporating the study of implementation determinants, processes, and outcomes (Nilsen, 2020; Nilsen & Bernhardsson, 2019). There is growing recognition that realizing the full public health benefit of research requires consideration of implementation, prompting a new generation of hybrid trials that examine health effects, implementation strategies, and outcomes (Curran et al., 2012). We present the implementation outcomes of a small pilot test of IMAGE in Chicago. Consistent with the Implementation Outcomes Framework (Proctor et al., 2011), we report on the feasibility, acceptability, appropriateness, and fidelity of IMAGE.
Methods
Setting
We partnered with the Lawndale Amachi Mentoring Program (LAMP) to implement the pilot test. LAMP, located in Chicago, facilitates positive youth development by building partnerships and providing space for young people and their families to express themselves and thrive (Chicago Lawndale AMACHI Mentoring Program [LAMP], 2022). LAMP was extensively involved in the adaptation process and development of IMAGE (Crooks et al., 2023). We hired LAMP staff to act as a liaison to the research project and ensure the voices and perspectives of LAMP families were represented.
Participants
Procedures
Participant enrollment (N = 40; n = 20 girls and n = 20 BMC) occurred from July to September 2022, and 1-month follow-ups concluded in October 2022. Girls self-identified as female, Black or mixed race, between the ages of 13 and 18, and English speaking, and reside in Chicago. Male caregivers who self-identified as Black or mixed race, were identified by the girl as a caregiver, were 18 years or older, lived with or had daily contact with the girl, and spoke English. Girls and BMCs had to agree to participate as a dyad, and girls’ refusal superseded BMCs’ agreement. The girl’s primary female caregiver gave consent for the girl to participate in the BMC.
Study Team and Procedures
The PI (first author) hired an all-Black, female research team familiar with the greater Chicago area and with prior experience at community organizations and/or implementing HIV prevention interventions. Girls and BMC were approached by a trained recruiter in community spaces (e.g., barbershops, block parties, and community organizations) and provided with information about the IMAGE study (Crooks et al., 2024). Most (n = 46) participants were interested in learning more and were directed to contact the liaison at LAMP to assess eligibility and obtain consent. Before the IMAGE workshops, staff reviewed consent and assent with participants, who then received a Qualtrics link on their phones to complete a 45- to 90-min baseline survey about their demographic characteristics, sexual behavior, familial norms, and relationships (i.e., communication, monitoring), and other topics (e.g., stereotypes). If surveys were not completed before the interview day, participants were asked to complete them on the morning of their scheduled workshop.
IMAGE was delivered over 2 days for a total of 8 hr, approximately 4 hr each day. A multi-session format was used because: (1) It maximizes participation so girl-male caregiver dyads can benefit from the full program. (2) Two days ease the burden on families’ financial resources. (3) Two sessions have real-life utility; they are pragmatic and responsive to the needs of urban low-income families. (4) Research supports psychosocial and behavioral change among girls following brief HIV prevention interventions (Donenberg et al., 2020). IMAGE workshop sessions were held at LAMP over four weekends. Participants were compensated for their time: $60 for completion of day 1 of the workshop, $65 for day 2, and $70 for a 1-month follow-up survey, totaling $195. Snacks and meals were provided on both workshop days. Participants completed implementation evaluations regarding IMAGE’s content, materials, delivery, and relevance at the end of the 2-day sessions. Participants received a Qualtrics link to complete the 1-month follow-up assessment.
IMARA for Black Male Caregiver and Girls Empowerment (IMAGE)
IMAGE emphasizes BMC’s desire and willingness to participate in girls’ lives to protect and support them while challenging toxic masculinity (i.e., use of dominance, violence, and control) to assert power over girls and women. IMAGE was conducted in groups of six to eight girl-BMC dyads, facilitated by four trained Black women (two for girls and two for BMC). Some components were delivered individually to girls and BMC, while others were delivered together to both. IMAGE comprises 35 modules focused on Black girls’ sexual development, sexual violence, female anatomy, body positivity, HIV/STI knowledge and attitudes, contraception use, girl-BMC communication and relationships, stereotypes, and sexual objectification of Black girls and women. IMAGE was created to foster healthy communication and connection between male caregivers and their girls by encouraging conflict resolution and perspective-taking. BMC learn about the importance of mental health, role modeling, and partner choices. Through IMAGE, BMC will become more aware of their presence in their girls’ lives, discuss absenteeism (if BMC are incarcerated/ unable to be physically present), and learn to be present. IMAGE emphasizes how Black girls and women are portrayed in the media, which creates unhealthy stereotypes, decreases self-image, and increases vulnerability to sexual violence. Girls and caregivers will discuss intimate partner violence and the power in healthy relationships, as well as discuss the use of contraceptives, specifically condoms. IMAGE directly addresses structural factors on girls’ susceptibility to HIV and STIs, namely male incarceration, sexual violence, domestic violence, and negative stereotyping. Woven throughout IMAGE is the impact of mental health, gender-based violence, and alcohol and drug use on HIV/STI risk.
Facilitator Training
Facilitator training lasted approximately 24 hr. Facilitators, some of whom had previously delivered IMARA, reviewed the IMAGE curriculum and related training manuals. Training stressed the importance of being open, relatable, engaging, and following the manual to ensure intervention fidelity (i.e., adherence) across facilitators. After carefully reviewing the curriculum, facilitators practiced delivering each activity, taking turns serving as group leaders and participants.
Facilitator Supervision
Each workshop was observed by a trained individual familiar with the curriculum and trained to assess the facilitator’s adherence to and competence with the manual. Fidelity ratings were reviewed by a supervisor and discussed with facilitators during weekly supervision. When ratings showed gaps in adherence, the supervisor provided targeted support to the facilitator until adherence was achieved.
Measures
Measures were selected because they have been used in several prior studies, including IMARA (Donenberg et al., 2020; Merrill et al., 2023).
Primary Outcomes
Sexual behavior was measured using the AIDS-Risk Behavior Assessment (ARBA) (Donenberg et al., 2001), a measure of adolescent sexual activity widely used with youth and Black girls (Danielson et al., 2014; Donenberg et al., 2020). Analyses examined differences at follow-up in sexual behavior among girls who reported vaginal and/or anal sex in the past month: condom use at last sex (yes/no); and consistency of condom use (always/less than always), number of sexual partners (one/two or more) in the past month. We also asked if the girls would be willing to provide urine for STI testing (yes/no).
Secondary Outcomes
Participants self-reported on the girl-male caregiver relationship, including attachment, open communication, communication process, and family protection.
The Inventory of Parents and Peer Attachment-Revised (IPPA) (Armsden & Greenberg, 1987; Gullone & Robinson, 2005) is a 25-item measure with a 5-point Likert-type scale (1 = almost never true to 5 = always true) that asks adolescents to rate their relationships with their parents. A sample item is “My father/male caregiver understands me.” Scale reliability was (α = .66–.86).
Open Communication
Girls reported their perceptions of male caregivers’ openness of communication on a 10-item measure and response options “yes” or “no” (Miller et al., 1998). A sample item is, “Have you and your father/male caregiver ever talked about when to start having sex?” Scale reliability was (α = .87).
Process of Communication
Girls reported on their communication with male caregivers using a 10-item Likert-type scale (1 = strongly disagree to 4 = strongly agree; Dutra et al., 1999). Sample questions include: (1) “My father/male caregiver doesn’t know enough about topics like this to talk to me.” (2) “My father/male caregiver wants to know my questions about these topics.” (3) “My father/male caregiver tries to understand how I feel about topics like this.” Scale reliability was (α =.87).
Family Risk and Protective Factors
The 38-item Communities That Care Youth Survey includes seven subscales: family management, involvement, behavior, attitudes, and attachment (Arthur et al., 2007; Substance Abuse and Mental Health Services Administration, 2004). We examined the attachment scale, which provides protective (or promotive) factors, while the remaining six subscales are risk factors. The attachment scale consisted of 4 items on a 4-point Likert-type scale, where 1 = definitely not true to 4 = definitely true. The attachment scale provides protective (or promotive) factors; the remaining six subscales are risk factors. Attachment scale items included “Do you feel very close to your father/male caregiver?”
Implementation Outcomes
Feasibility was determined by the proportion of girl-BMC dyads who (1) consented/assented to participate in the study and (2) attended one session and the entire 8–hour intervention (Donenberg et al., 2020; Merrill et al., 2023).
Acceptability was measured using a combination of items used in prior research. Girls and BMC at the end of the 2-day workshop. Girls and BMC reported their satisfaction (1 = not at all satisfied to 5 = extremely satisfied) with IMAGE at the end of the 2-day intervention. They also completed items (16 by girls and 17 by BMC) from the Applied Mental Health Research (AMHR) scale, adapted to assess comfort with the material and knowledge gained (Haroz et al., 2019; Murray et al., 2014; Nguyen et al., 2019; Proctor et al., 2011). Response options were on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Scale reliability was α = .85.
Appropriateness was measured with 1 item regarding the length of the intervention from the AMHR on a Likert-type scale from 1 = much too short to 5 = much too long. Scale reliability was α = .91).
Intervention Fidelity
Two trained observers completed measures of adherence to the manual and competence in delivering the curriculum on both intervention days. A 5-item checklist indicated whether a session topic (i.e., facilitator introductions, project goals explained, welcomed new/returning participants, developed/reviewed group rules) was completed (Yes/No). Twelve items described facilitation skills (i.e., following script, pacing, open and nonjudgmental communication) and were rated on a 5-point Likert-type scale (0 = not very well to 4 = very well). Facilitator adherence and competence of module activities were assessed with a 35-item Likert-type scale (0 = not very well to 4 = very well), and intervention session flow was assessed with a 5-item 5-point Likert-type scale (1 = poor to 5 = excellent). Scores were averaged across observers. Checklists were customized to each intervention day’s activities (Lane et al., 2004). Intervention fidelity ratings were averaged across observers to determine the proportion of activities completed as planned. Finally, three open-ended questions invited girls and BMCs to share feedback and suggestions to improve IMAGE.
Data Analysis
We used RStudio and paired t-tests to examine participant change from baseline to 1-month follow-up in the girl-BMC relationship and communication. Implementation outcomes are summarized with descriptive analyses, and open-ended responses are thematically coded (Braun & Clarke, 2006).
Ethics
Ethical approval was obtained from the University of Illinois Chicago, protocol number: 2021-833.
Results
Participants
A total of 59 people were invited to participate in the IMAGE pilot; 46 were assessed for eligibility, and 20 dyads (N = 40) were enrolled (see Figure 1). Over half of the girls (n = 9; 52%) participated in IMAGE with their biological fathers. The remaining BMCs were brothers, cousins, stepfathers, grandfathers, uncles, and mentors. Girls ranged in age from 13 to 18 years (M = 15; SD = 1.7) and were in high school (71%). For girls, the age of first menstruation varied between 8 and 14 years old. Twenty-four percent experienced their first period by 11 years old. Eight girls (47%) reported being attracted to both genders. Five girls (29%) reported using birth control.
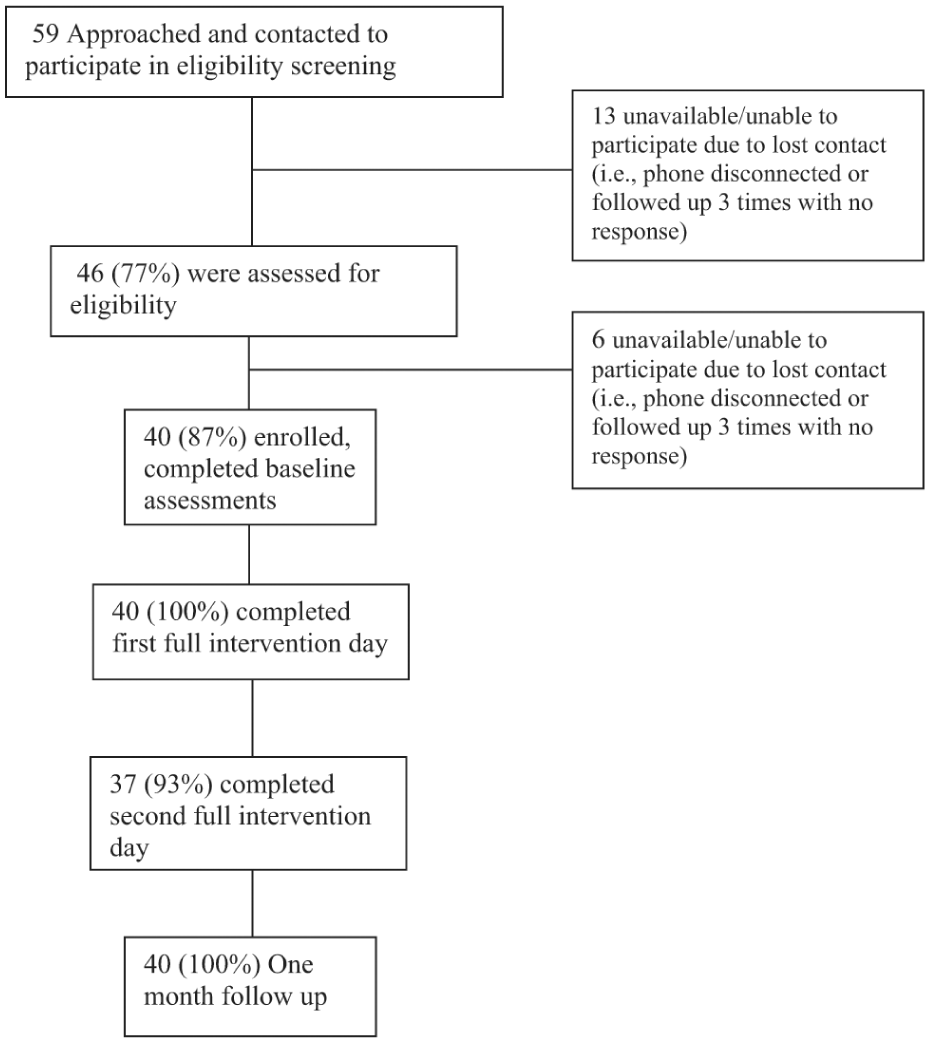
Consort diagram.
Sexual Behaviors
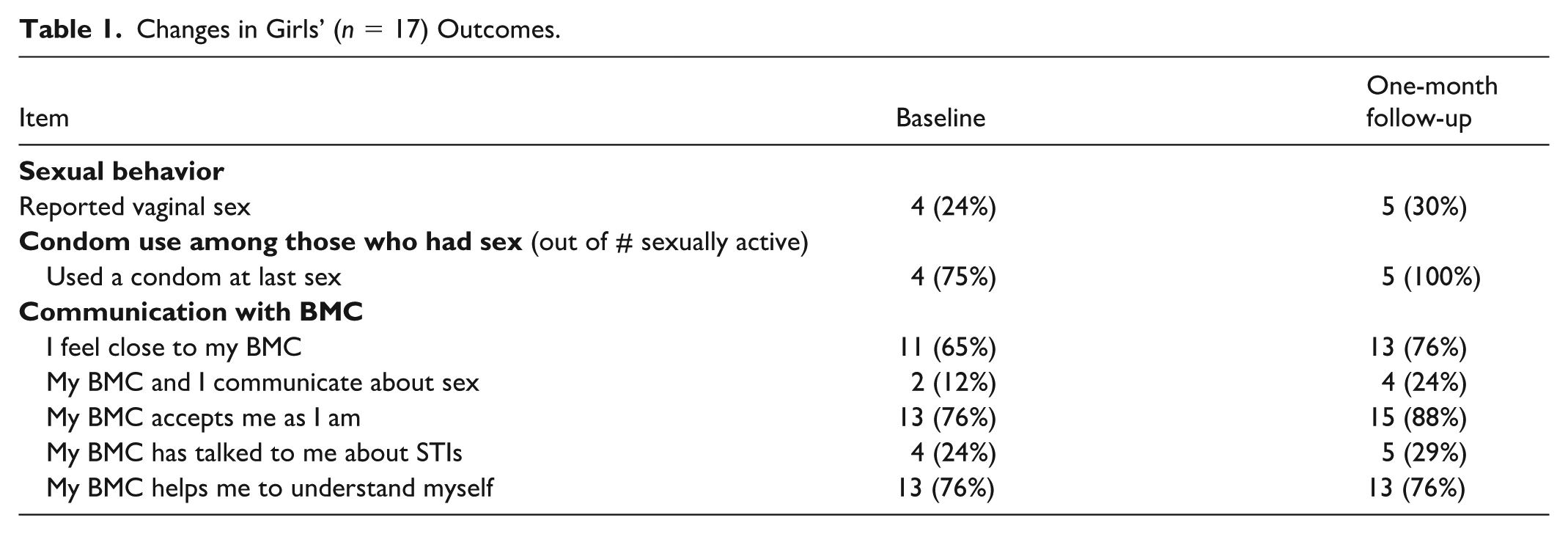
At baseline, four girls reported being sexually active (20%), and three of them reported condom use. At 1-month follow-up, a total of five girls endorsed being sexually active, and all indicated condom use. All girls said that they would be willing to provide urine for an STI test.
Girls-BMC Closeness
At baseline, ten (59%) girls endorsed “definitely true” regarding feeling close to their BMC, and 11 (64%) indicated that it was “definitely true” that they did not receive enough attention from their BMC. At 1-month follow-up, 13 (76%) girls responded “definitely true” about feeling close to their BMC, while 10 (58%) indicated that it was “definitely true” that they did not receive enough attention from their BMC.
Girl-BMC Communication
At baseline, all girls reported that it was “almost always or mostly true” that they often talk to their BMC when experiencing problems or troubles, and 14 (82%) reported that it was “almost always true” that they trust their BMC with whom they confided. At baseline, only two (12%) girls reported discussing sex with their BMC, while three girls (18%) had talked about birth control, five (29%) spoke about condoms, four (24%) spoke about AIDS or HIV, and three (18%) communicated about STIs. Four (24%) girls had conversations with their BMC on how to handle sexual pressure from friends or potential partners. Eight (47%) girls said they felt it was “always true” that they could discuss these topics openly and freely with their BMC.
At 1-month follow-up, there were no changes in the number of girls who reported talking to their BMC when experiencing problems or troubles, or who indicated that they trusted their BMC and confided in them. However, four out of 17 girls (24%) indicated that they talked about sex with their BMC, six (35%) talked about birth control, eight (47%) had conversations about condom use, five (29%) spoke about AIDS or HIV, and four (24%) communicated about STIs. Four (24%) girls had conversations on how to handle sexual pressure from friends or potential partners with their BMC. Nine (53%) participants reported feeling it was “always true” that they could discuss these topics openly and freely with their BMC (Table 1).
Changes in Girls’ (n = 17) Outcomes.
Implementation Outcomes
Feasibility
Of those eligible, 87% agreed to enroll in the study, and retention rates were high: 100% (n = 40) completed day 1 of the intervention, and 93% (n = 37) completed both days.
Acceptability
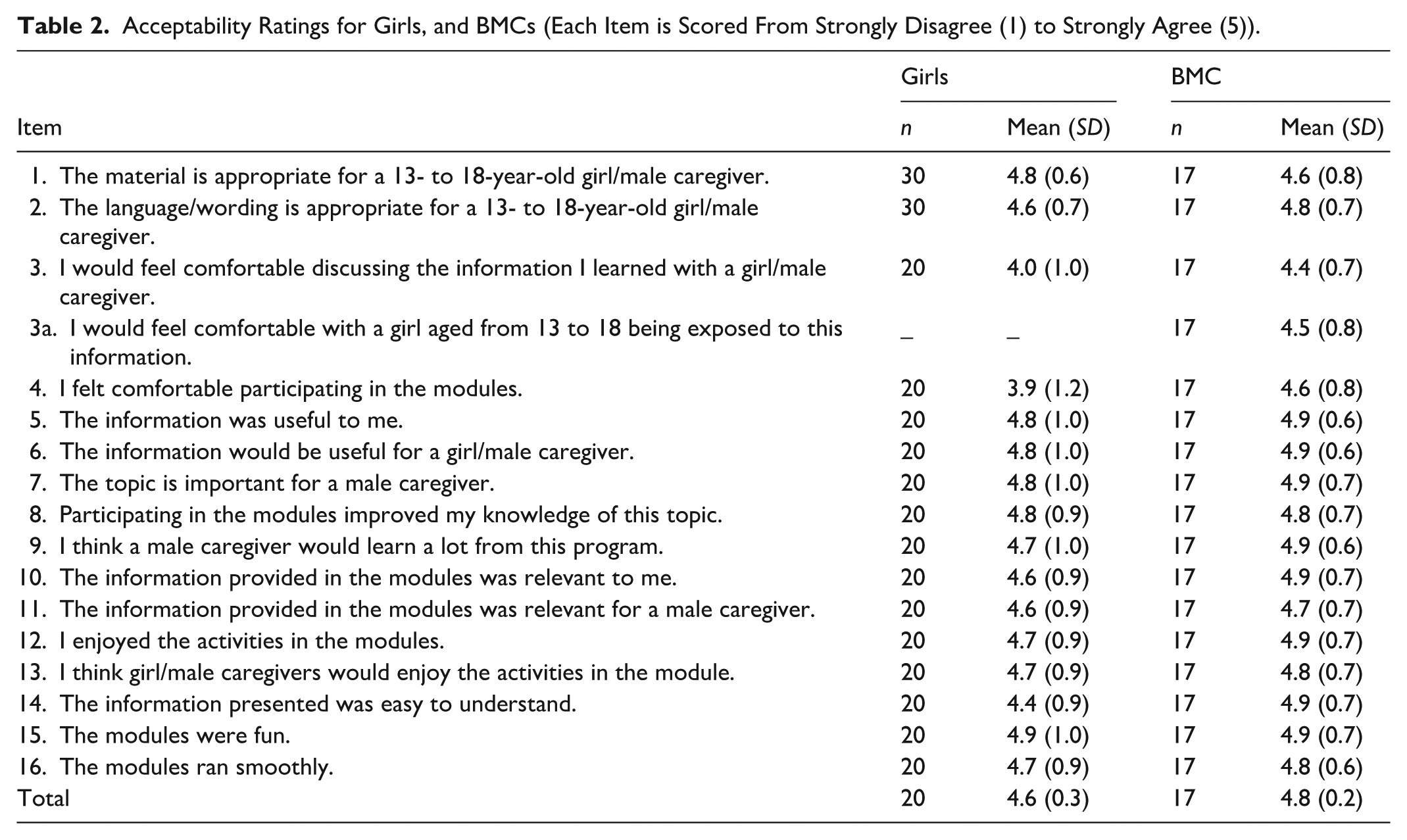
IMAGE evaluations were completed by 93% (n = 37) of participants at the end of the full intervention. Three-fourths of girls and BMC reported being “very satisfied” and “extremely satisfied” with the program. Ratings averaged 4.7/5.0 (SD: 0.2) (Table 2).
Acceptability Ratings for Girls, and BMCs (Each Item is Scored From Strongly Disagree (1) to Strongly Agree (5)).
Appropriateness
When asked, “How appropriate was the amount of time we spent on the modules?” Most participants (76%) felt that the time spent on the modules was just right. A smaller portion, 22%, thought it was a “little long,” while only 2% felt it was “much too long.” No participants considered the time too short.
Fidelity
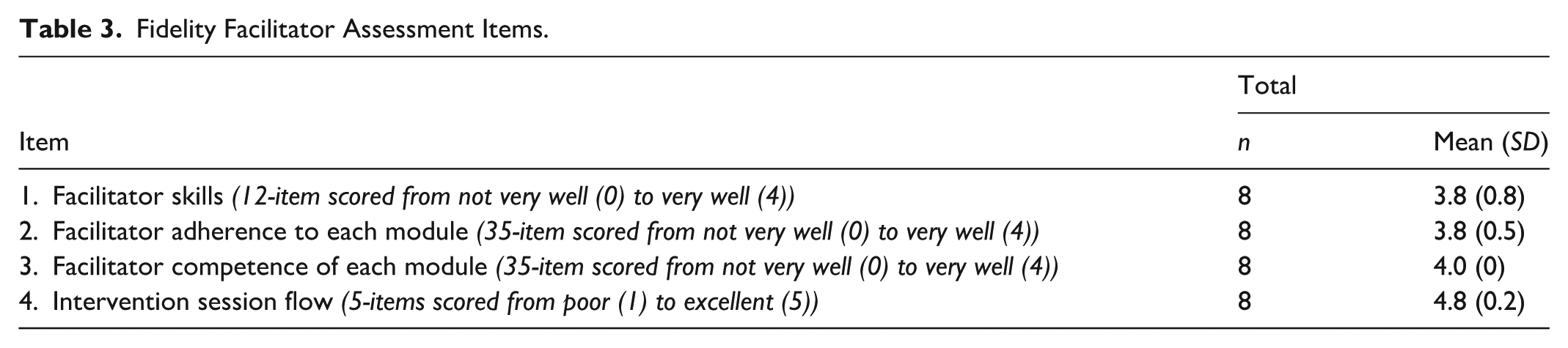
Observations were conducted in all four 2-day workshops (100%). We held four workshops with two observers rating fidelity, resulting in a total of eight fidelity forms. Observers were trained to assess whether specific session components were delivered, using a 100% (yes/no) scale. Facilitation skills (i.e., following script, explaining and demonstrating activities, being active and engaging, etc.) were assessed in 12 items, which were 95% (M = 3.8/4; SD = 0.8). According to observer ratings, facilitator adherence to the curriculum was 95% (M = 3.8/4; SD = 0.5). Observers also rated facilitators highly competent (100%). The intervention session flow was rated as 96% (M = 4.8/5; SD = 0.2) regarding the facilitator’s delivery and comfort of intervention (Table 3).
Fidelity Facilitator Assessment Items.
Open-Ended Feedback
Girls described several lessons learned, such as “We need to know these things in life so we can prevent them from happening.” Girls recommended more content related to sexual assault, catcalling, and “everyday” experiences like bullying to help normalize Black girls’ experiences. One girl suggested we add more about pregnancy, “I think you guys could add a section where we talk about early pregnancy in the Black community and ways to deal with it.” Two girls suggested we add more content about expressing emotions: “How to show emotions and explain that it isn’t feminine and there’s nothing wrong with it.”
BMCs stated that there were no changes to be made, everything went well, and they enjoyed the program. One BMC said, “I feel we got all the information we need to have these conversations with our girls.” Another stated, “Great people [facilitators] and supervisor” when referring to the IMAGE team.
Discussion
To the best of our knowledge, this pilot is the first to engage male caregivers in sexual and reproductive health programming for Black girls. This small pilot study provides preliminary evidence for the feasibility, acceptability, and perceived value of an innovative HIV prevention intervention for Black girls and their male caregivers. Girls and BMC participants uniformly liked the program, reported acquiring new knowledge, and appreciated the opportunity to participate together.
IMAGE builds on previous literature showing the positive impact of communication among Black families on reducing adolescent sexual risk-taking behaviors and adds new data on girls and their male caregivers (Dorsey, 2022; Kachingwe et al., 2023). Sexual communication between girls and their male caregivers is important in promoting healthier sexual behaviors among Black girls (Hutchinson & Cederbaum, 2011; McDade et al., 2020; Rostad et al., 2014). Black father-daughter sexual health communication is facilitated by close father-daughter relationships, non-authoritative parenting styles, and open, supportive, and non-judgmental communication. Closeness and communication are protective for Black girls’ sexual health (Crooks et al., 2024; Dorsey, 2022; Kachingwe et al., 2024). Parents play an important role in teaching girls about their bodies and supporting their sexual development. When parents or caregivers initiate an open discussion of SRH topics, girls can ask questions more easily. Parents can recognize and respond to their girls’ unique needs and facilitate their transition into adulthood (Buzi et al., 2009; Munz, 2016; Sutton et al., 2014).
The IMAGE program is designed to improve BMC-girl communication and relationships to increase girls’ knowledge about relationships and sexual health and reduce STIs. IMAGE seeks to empower Black girls by teaching them how to communicate about SRH topics without embarrassment, shame, or stigma. Sexual health communication provides the opportunity for Black girls to acquire the knowledge and skills necessary to have a positive outcome on their sexual health and develop communication skills to talk to their parents, which can contribute to reducing Black girls’ vulnerability to adverse sexual health experiences.
We found promising evidence for IMAGE’s feasibility, acceptability, appropriateness, and fidelity. IMAGE was feasible to implement in community-based organizations in Chicago, as indicated by strong attendance, positive ratings, and open-ended responses by girls and BMCs. Feasibility and acceptability are “leading indicators” of intervention success and key predictors of adoption, which is essential for community settings and in partnerships with community-based organizations where IMAGE workshops will be implemented. BMCs and girls were uniformly satisfied with the program’s content and facilitators, and the intervention was delivered with high fidelity. Fidelity is critical to attribute observed circumstances to the actual intervention (Toomey et al., 2020), and positive perceptions of facilitators are linked to better program outcomes (Bellg et al., 2004; Castro et al., 2004).
Limitations
Findings should be interpreted with caution. This small pilot study was not powered to evaluate behavior change in girls or change from baseline to follow-up. A larger trial is needed to test statistical changes in sexual behavior, dyad relationship, and communication factors over time. COVID-related lockdowns and restrictions hampered our ability to recruit a larger sample and delayed IMAGE workshops. Data collection inconsistencies arose when participants created the same “unique identifiers” or forgot them between surveys. This made it difficult to link the baseline and 1-month surveys. The research team reconciled misclassifications by recontacting participants and fixing these through manual review. Although all 20 girls completed the surveys, three participants selected “I do not want to answer” for the 1-month follow-up survey. Therefore, they were not included in the analysis.
Conclusion
Findings from this pilot study support the feasibility, acceptability, and fidelity of an HIV prevention program for Black male caregivers and girls. Ninety-three percent of the participants attended the complete 8-hr program over 2 days, reaching a highly vulnerable population, and it was acceptable to Black girls and male caregivers alike. IMAGE can be implemented with fidelity in community-based organizations with adequate training and supervision. These findings support the conduct of a fully powered randomized controlled trial in partnership with community-based organizations.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institutes of Health U54MD012523 Chicago Center for Health Equity Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.