
Abstract
Intimate partner violence (IPV) is a significant public health concern, affecting over 41% of women in the United States during their lifetime. IPV is particularly prevalent during reproductive years, including pregnancy and postpartum periods, and has severe adverse effects on both maternal and child health. Home visiting offers a promising context for prevention; however, persistent barriers to screening underscore the need for practical, implementation-ready tools to support home visitors in addressing IPV. This brief report describes a quality improvement initiative examining the implementation of the Futures Without Violence Connected Parents, Connected Kids (CPCK) cards within Alabama home visiting programs. Between September and December 2024, four Alabama local implementing agencies (LIAs) participated in the Home Visiting Collaborative Innovation and Improvement Network’s (HV CoIIN) Sprint to Sustain Improvement in IPV (sprint). The sprint aimed to integrate CPCK cards into home visits, with a goal of educating 90% of families on healthy relationships and improving support for home visitors in discussing IPV. Data from Alabama’s home visiting database were used to track IPV screening rates before and after the sprint. In addition, a survey was conducted to gather home visitors’ perspectives on CPCK cards. Results showed that by the end of the sprint, all caregivers were educated about healthy relationships, and IPV screening rates improved at three LIAs and remained 100% at the fourth. Survey responses indicated that CPCK cards were valuable tools for facilitating conversations about healthy relationships and screening for IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a significant public health concern. More than 41% of women in the United States will experience IPV in their lifetime, including physical violence, sexual violence, stalking, and psychological aggression (Centers for Disease Control and Prevention [CDC], 2024). While common at every stage of life, IPV is most prevalent during reproductive years, particularly during pregnancy and postpartum periods (American College of Obstetricians and Gynecologists [ACOG], 2022; Office of Planning Research and Evaluation, U. S. Department of Health and Human Services [OPRE], 2020).
IPV has significant adverse effects on the health of both caregivers and their children. IPV is associated with inadequate prenatal care, substance abuse, and maternal depression (Agrawal et al., 2014; Alhusen et al., 2015). In addition, IPV correlates with poor birth outcomes, such as low birth weight, preterm birth, and increased maternal and infant mortality (Alhusen et al., 2015). While IPV is a prevalent and significant public health issue, it is largely preventable (ACOG, 2022; CDC, 2024).
Home visiting programs offer repeated, relationship-based contact with families, positioning home visitors to address sensitive and stigmatized topics, such as IPV (Office of Planning Research and Evaluation, U. S. Department of Health and Human Services [OPRE], 2020). However, prior research within home visiting settings documented persistent barriers to IPV screening, including home visitor discomfort, lack of training, and concerns about damaging rapport (Davidov et al., 2018; Tandon et al., 2008). This underscores the need for practical, implementation-ready tools (Davidov et al., 2018; Sprague et al., 2012). Furthermore, universal education on healthy relationships has been shown to normalize IPV conversations and increase opportunities for IPV identification and support (Todahl et al., 2020).
Methods
Setting and Participants
Between September and December 2024, four Alabama local implementing agencies (LIAs), implementing the Parents as Teachers (PAT) home visiting model, participated in a quality improvement initiative as part of the Home Visiting Collaborative Innovation and Improvement Network’s (HV CoIIN) Sprint to Sustain Improvement in IPV (sprint). The sprint focused on integrating Futures Without Violence Connected Parents, Connected Kids (CPCK) cards into routine home visits. CPCK cards were used by home visitors to facilitate conversations about healthy and unhealthy relationships, normalize IPV screening, and share relevant services and resources.
All home visitors at participating LIAs participated in this effort. Families were not selected for home visitation or participation in this initiative specifically for the purposes of this project, rather CPCK cards were implemented with all families receiving home visits at participating LIAs, rather than targeting a subset of families. While the overarching aim of the sprint was to ensure that 90% of families received education on healthy relationships by December 2024, the purpose of this effort was to describe the implementation of CPCK cards during the sprint and to examine associated changes in IPV screening rates and home visitor perceptions. In addition, Alabama aimed to improve support for having difficult conversations about IPV with families.
Intervention Description
The CPCK cards are brief, family-facing educational tools developed by Futures Without Violence to support conversations about healthy relationships, warning signs of IPV, and available support resources. The cards are designed for use by a range of professionals and can be easily integrated into standard practice (Futures Without Violence, 2014). As part of the sprint, participating home visitors received structured guidance, opportunities for peer learning, and ongoing technical assistance to support use of the cards during home visits.
Data Sources and Measures
IPV screening was conducted using the Abuse Assessment Screen (AAS), a validated screening tool commonly used in home visiting. The AAS has demonstrated reliability and validity in prior research and has been widely adopted in home visiting programs (Soeken et al., 1998).
IPV screening data were extracted from Alabama’s home visiting database and used to calculate the percentage of families screened for IPV at participating LIAs before and after participation in the sprint. The baseline screening rate was calculated using 3 years of data (FYs 2022, 2023, and 2024); this baseline was then compared against the sprint screening rate, or the average percent of families screened during the months of October 2024 through February 2025. This period was chosen as a comparison because the sprint kickoff occurred in mid-September 2024 and concluded in December 2024, allowing the team to see screening rates post-kickoff through the 2 months immediately following sprint completion. Finally, during the sprint, home visitors self-reported the number of families with whom they had engaged in a conversation about healthy relationships.
To better understand home visitor perspectives on the use of CPCK cards, our team distributed a survey to participating LIAs. The survey asked home visitors to rate their level of agreement, on a five-point Likert-type scale with 1 = strongly disagree to 5 = strongly agree, with the following statements:
The cards made it easier for me to have a conversation with families about healthy relationships.
The cards provided needed information and resources for families regarding healthy relationships.
The cards made it easier to screen families for IPV.
Using the cards may help identify signs of IPV that I might have missed otherwise.
It was easy to integrate the cards into my model curriculum and home visits.
I would recommend the use of these cards to other home visitors.
At the end of the survey, home visitors were given the opportunity to elaborate on their responses to the questions above through an open-ended survey question. Home visitors were also asked what other resources, training, or tools would be helpful for discussing healthy relationships and screening for IPV.
The survey was built in Qualtrics (Provo, UT; Qualtrics, 2005) and emailed to LIA supervisors for distribution to the home visitors who participated in the sprint. The survey was open from February 17, 2025, to February 28, 2025. All responses remained confidential.
Data Analysis
Descriptive statistics were used to summarize IPV screening rates and survey responses.
Figures were generated using Microsoft Excel (Microsoft Corporation). This study was approved by the University of Alabama at Birmingham Institutional Review Board (IRB #300008693).
Results
By the end of the sprint, all caregivers in participating home visiting programs were educated about healthy relationships using CPCK cards. IPV screening rates, though known to be high prior to sprint performance, improved at three of the participating LIAs and remained 100% for the fourth LIA (Figure 1).
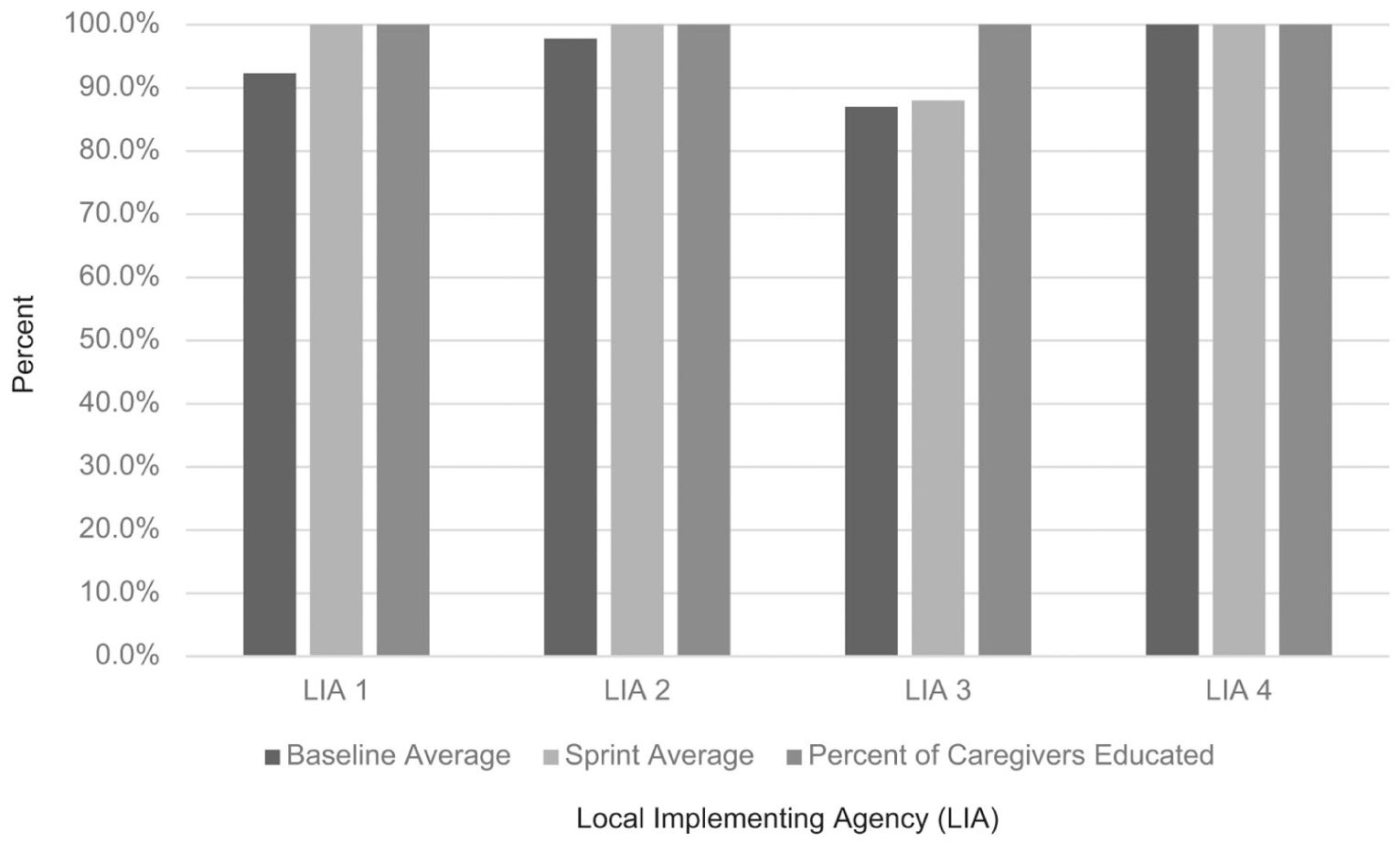
Percentage of caregivers provided education and screened for IPV within six months of enrollment at four participating local implementing agencies (LIAs).
All 22 home visitors who participated in the sprint completed the survey for a 100% response rate. Survey responses were generally positive with noted variability. Most home visitors agreed or strongly agreed that CPCK cards were valuable tools for discussing healthy relationships (65%), providing resources (75%), and screening for (60%) or recognizing signs of IPV (65%). Most home visitors agreed or strongly agreed that integrating the cards into visits was easy (80%) and would recommend these cards to other home visitors (80%) (Figure 2).
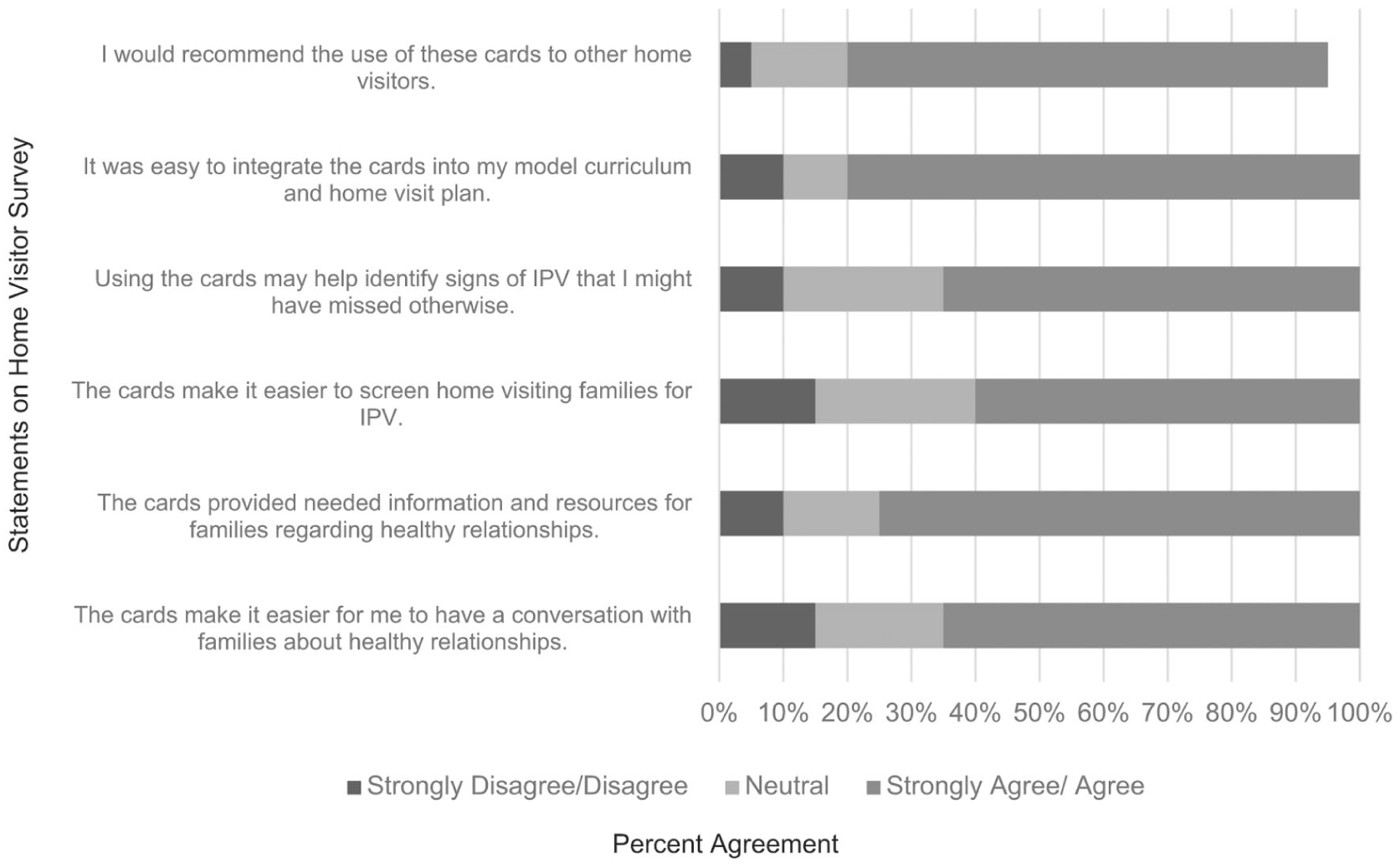
IPV survey results: home visitor level of agreement.
Open-ended survey responses provided insights into the use of CPCK cards during home visits. One home visitor shared, “The cards have facilitated difficult and uncomfortable conversations about IPV. Having a physical copy of the card has personally helped me navigate through some awkward moments.” Another home visitor explained, “The cards were very beneficial and helped uncover situations with families that I was previously unaware of.”
However, some home visitors highlighted challenges. For instance, one mentioned that the comfort level of both the home visitor and the family could still be an issue, stating, “It depends on how comfortable the parent educator is with the discussion and how open the families are to answering them.” Another home visitor pointed out that using the cards could add to their workload, “Visits are unpredictable, so while tools are helpful, they can also become additional work.” Finally, one home visitor suggested that the cards might be more effective with less information, “. . . less information on the card might be better to avoid overwhelming the reader.” When asked what additional resources, training, or tools would be helpful, home visitors listed the need for additional trainings and additional information on available resources in their communities.
Discussion
IPV is a challenging topic for home visitors to address with families. However, results from this study suggest that the use of CPCK cards may help home visitors engage in meaningful discussion about IPV without jeopardizing rapport. Home visitors largely agreed that the cards could improve IPV screening. While most open-ended comments were positive, home visitors shared ways in which CPCK cards could be more effective as well as needs for further training and resources.
Findings from this implementation effort align with existing literature highlighting the challenges home visitors face when addressing IPV (Davidov et al., 2018; Tandon et al., 2008) and the value of structured tools to support universal education approaches (Miller et al., 2011; Miller et al., 2016). This study contributes to the literature by demonstrating how a brief, universal education approach can be integrated into routine practice within established home visiting systems.
Limitations
Despite positive results, there are several limitations of note. First, data relied on home visitor self-report. Further, despite the confidentiality of survey responses, home visitors may have provided positive feedback on the survey due to social desirability bias (Paulhus, 1984). In addition, all four participating sites implement the PAT home visiting model, which may limit the generalizability of the findings to other locations and other home visiting models. Also, the study measured the effects of the sprint during a relatively short follow-up period; therefore, the team could not assess longer-term effects and the sustainability of the intervention. Regarding the implementation and impact of CPCK cards, there may have been variability in how home visitors implemented the cards, and while the study measured the number of families educated and screened for IPV, it did not directly assess IPV outcomes. Finally, the lack of a comparison group is a limitation, making it difficult to directly link improvements to the use of CPCK cards.
Implications for Practice
Enhanced Training for Home Visitors: The positive feedback of CPCK cards paired with responses to questions regarding additional resources, training, and support needed suggests that home visitors could benefit from additional training that focuses on improving comfort levels when discussing sensitive topics like IPV.
Integration of Universal Education: The success of the CPCK cards suggests that integrating universal education on this topic into home visiting programs can help normalize discussions about IPV and reduce stigma.
Ongoing Support and Evaluation: Study findings underscore the importance of ongoing support and evaluation to sustain improvements in IPV screening and education. Regular check-ins and feedback loops can help identify challenges and areas for further improvement.
Implications for Research
Evaluation of Long-Term Impact: Future research should focus on evaluating the long-term impact of using CPCK cards in home visiting programs. This includes assessing sustained improvements in IPV screening rates. In addition, future research should explore the effectiveness of CPCK cards on family attitudes and behaviors, including changes in understanding of healthy relationships and willingness to disclose IPV.
Comparative Studies: Conducting studies with comparison groups can help determine the specific impact of CPCK cards on IPV screening and education. This would provide more robust evidence of the effectiveness of using the cards.
Home Visitor Input: Future research should place additional emphasis on home visitor feedback, particularly among those who expressed neutral or mixed perspectives regarding the use of CPCK cards. Qualitative studies engaging home visitors could provide deeper insight into which aspects of the cards are most useful, which present challenges, and how the tools might be refined or adapted to better support home visitors.
Conclusion
The implementation of the CPCK cards in Alabama home visiting programs has demonstrated promising results in educating caregivers about healthy relationships and improving IPV screening rates. The findings highlight the potential benefits of integrating structured educational materials into home visiting programs. Enhanced training and ongoing support for home visitors are essential to sustain these improvements and address the challenges identified, such as the added workload and comfort levels in discussing sensitive topics. Overall, study findings underscore the importance of structured tools in improving IPV education and screening and suggest that with adequate support and resources, home visiting programs can play a crucial role in addressing IPV and promoting healthy relationships.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Health Resources and Services Administration (HRSA), Department of Health and Human Services (HHS) provided financial support for this project. The contents are those of the author. They may not reflect the policies of HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.