
Abstract
Introduction:
Inguinoscrotal hernia (ISH) hernias pose higher risk of complications. Traditionally, complete dissection of the hernia sac has been considered the standard approach but, more recently, primary abandonment of the sac (PAS) has emerged as simpler alternative and potentially reduced complications. Seromas are common postoperatively, but their association with sac abandonment remains debatable.
Objective:
To evaluate the long-term impact of PAS in minimally invasive ISH repairs.
Methods:
A total of 29 patients, in a prospective observational study, who underwent minimally invasive IHS repair with PAS technique were included. ISH was defined as hernia sac longer than 7 cm from the deep inguinal annulus. Primary outcome was seroma incidence and its impact in at least 1 year follow-up.
Results:
Seroma was observed in 62.1% of patients at 7 days, decreasing to 31.0% at 30 days, 10.3% at 90 days, 6.9% at 6 months, and 3.4% at 12 months. No drainage procedure was required. One patient developed ischemic orchitis, and no postoperative hematoma or recurrence was observed. Patients with longer hernia sacs had a significantly higher risk of seroma, particularly those with sacs over 10 cm. L3 hernia classification was also associated with increased seroma rates compared with L2. No other patient-related or surgical factors were linked to seroma risk.
Conclusions:
Since seroma is usually an acute postoperative complication, 1 year of follow-up may be considered adequate for this outcome. Despite a higher early seroma rate, most resolved spontaneously within 3 months, and none required intervention. PAS does not increase long-term seroma risk and may represent a simple and promising alternative for ISH repair.
Introduction
Inguinoscrotal hernia (ISH) accounts for approximately 6%–10% of all inguinal hernias, and it is even more prevalent in developing countries. 1 Although there is no precise definition, ISH is characterized by the passage of abdominal contents through the inguinal canal into the scrotum. From clinical point of view, IHSs represent a challenge for surgeons since they are associated with a higher rate of postoperative complications and recurrence.1,2
Over the years, with the spread of the laparoscopic technique and more recently with the robotic approach, minimally invasive surgery (MIS) has proven to have significant advantages, mainly less pain and faster postoperative recovery, compared with conventional repairs.3,4 However, complex hernias, including ISH, have previously been considered a relative contraindication for MIS, mainly due to the difficulty of dissecting the hernia sac.5–7 In both conventional and MIS approaches, the general principle was to attempt complete reduction of the hernia sac. Abandoning the hernia sac was generally used only in cases of great technical difficulty in achieving it.8,9
Recently, primary abandonment of the sac (PAS) has been advocated by some authors to reduce the complexity of the procedure avoiding an extensive dissection inside of scrotum and potentially decreasing operative time and complications.8,10,11 However, there is a lack of studies reporting long-term follow-up of PAS technique, especially regarding the main question concern to abandonment of the sac, which is the risk of seroma formation.12,13
The aim of this study is to present the operative data and the postoperative complications of a series of patients who underwent PAS technique with at least 1 year of follow-up.
Methods
This is a prospective observational study of patients operated on single center in Curitiba, Brazil from January 2021 to January 2024. All procedures were performed by a single surgeon who is dedicated to abdominal wall surgery and MIS techniques. Definition of ISH was established by the extension of the hernia sac to the scrotum, exceeding the deep inguinal ring by at least 7 cm measured intraoperatively using a ruler, according to previous publications. 14
Inclusion criteria were male gender and age above 16 years old with ISH who underwent inguinal hernia repair by MIS approach (laparoscopic or robotic) using PAS technique and who completed at least 1 year of postoperative follow-up. Patients who had previously undergone preperitoneal surgeries such as prostatectomy and inguinal hernia repair or who underwent pelvic surgeries concomitantly with the inguinal repair were excluded from the study. The study was approved by the ethics committee of the Hospital Nossa Senhora das Graças CAAE:85476424.1.0000.0269. All patients given written informed consent.
All patients were operated upon using a transabdominal preperitoneal approach (TAPP). The first step of the procedure is to measure the hernia sac. For patients with hernia sac longer than 7 cm from the deep ring, the PAS technique was applied. Then, a circular incision of 360° was performed in the peritoneum at the level of the deep inguinal ring to disconnect the distal portion of the hernia sac as described by Claus et al. 14 In sequence, a standard TAPP technique was performed including8,15: (1) Opening the peritoneal flap 4 cm above the deep ring from the anterior superior iliac spine to the medial umbilical fold. (2) Dissection of preperitoneal space. During this step, after dissection of the lateral and medial areas (known as zones 1 and 2, respectively), we proceed with Zone 3/Central dissection where we encounter the previous peritoneal circular incision, which facilitates the recognition of the spermatic cord elements and avoids the extensive hernia sac dissection. (3) Inferior dissection of the peritoneum to at least 2 cm below the pubic bone, identification of iliopsoas muscle, and identification of the external iliac vein for diagnosis and repair of femoral hernia. (4) Inspection of the deep annulus for identification and dissection of the cord lipoma when present. (5) Placement of large mesh (at least 15 × 13 cm) covering the entire myopectineal orifice of Fruchaud. Mesh is secured with stitches, tacks, or even self-gripping meshes. (6) At the end of the procedure, before closing the peritoneal flap with suture, the “extra hole” created on the peritoneum is closed throughout running suture.
Demographic data and operative details including size and other hernia characteristics, operative time, complications, and length of hospital stay were collected. Postoperative outcomes, including seroma, hematoma, ischemic orchitis, recurrence, and patients perception, were prospectively evaluated. Seroma classification was based on previous publication by Claus et al.: (1) absent/incipient, (2) inguinal seroma, (3) scrotal seroma, and (4) inguinoscrotal seroma. Follow-up of the patients was carried out at 7 days, 30 days, 3 months, 6 months, and 12 months postoperatively.
Statistical analysis was carried out with the software JAMOVI version 2.5.0. To descriptively explore the behavior of the data, mean (± standard deviation) and median (min-max) values were used for the quantitative variables of interest. For qualitative variables, their behavior was expressed through absolute value and percentage of the total. For normally distributed data, the analysis of variance test was chosen. For nonnormal data, the Kruskal–Wallis technique was applied. Normality was checked through a Q–Q plot, as well as the homogeneity of variances through Levene’s test. In the case of comparisons between two qualitative variables, the Chi-square association test was applied, with continuity correction for cells that presented zero. In addition, a logistic regression was performed to assess the factors associated with the risk of developing postoperative seroma. For all tests, P values <.05 were considered sufficient to reject the null hypothesis and consider the result statistically significant.
Results
A total of 31 MIS inguinal hernia repairs with PAS technique were performed from January 2021 to January 2024. Two patients lost the 1-year follow-up and were excluded, remaining 29 patients in the analysis. Demographic data of these patients are listed in Table 1. Median age was 69 years old (30–89 years), and mean body mass index (BMI) was 26 (18.6–35) kg/m2. Regarding continuous medications, eight patients (27.6%) were taken anticoagulant or antiplatelet medications. Eleven patients (38%) had bilateral inguinal hernia, but, in all of them, ISH was present in only one side, in which PAS technique was performed. Six patients (20.7%) had recurrent hernias from previous repairs performed in other hospitals.
Demographic Characteristics
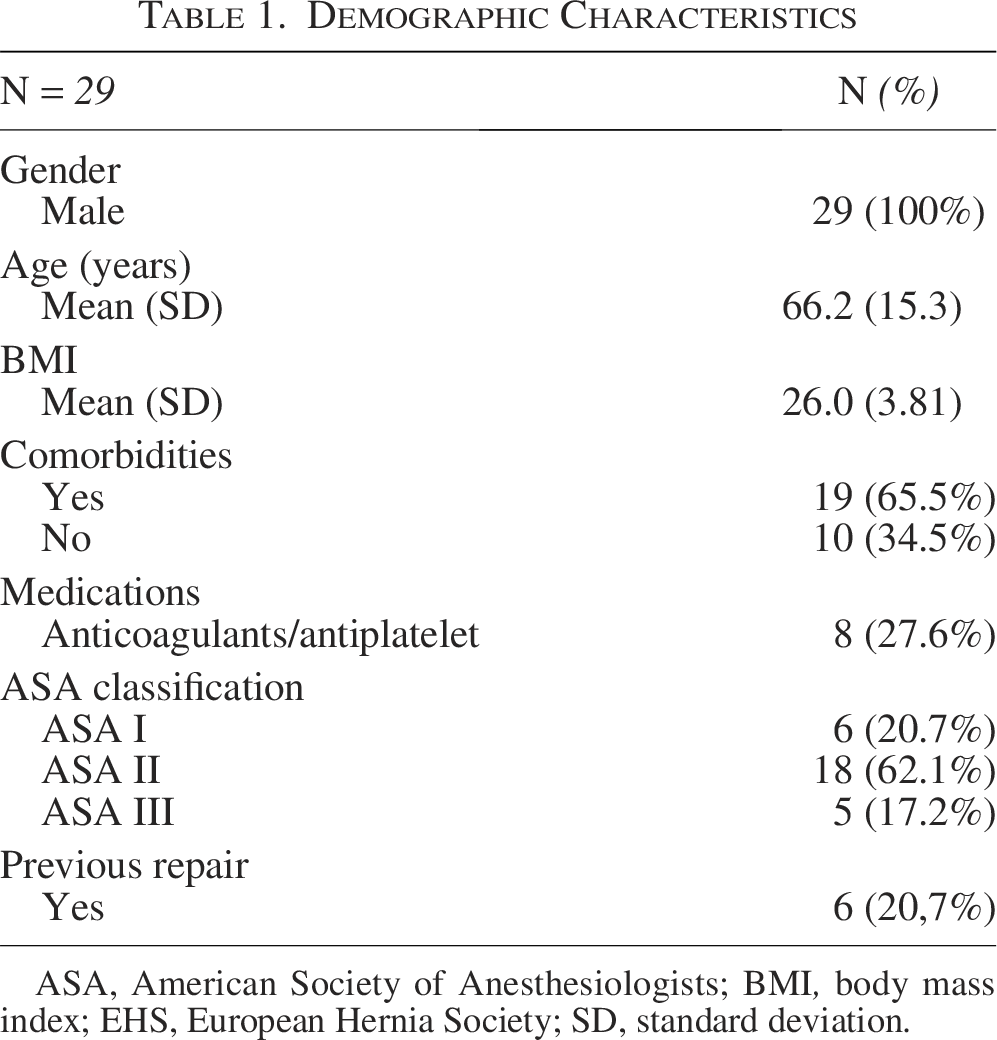
ASA, American Society of Anesthesiologists; BMI, body mass index; EHS, European Hernia Society; SD, standard deviation.
Herniorrhaphy was performed on emergency basis in only one patient (3.4%). The mean operative time was 74.4 minutes (range, 40–135 minutes). Twenty-three patients (79.3%) underwent laparoscopic surgery, whereas the remaining six (20.7%) were approached with robotic platform. The mean hernia sac size was 11.6 cm (8–20 cm), and 72.4% of patients presented sac longer than 10 cm. Type of mesh and fixation and other operative details are listed in Table 2. Drain was used in only three cases (10.3%), placed in the preperitoneal space due to continued use of anticoagulant or antiplatelet agent. Twenty-one patients (72.4%) were discharged from the hospital within 24 hours after the operation.
Operative Details
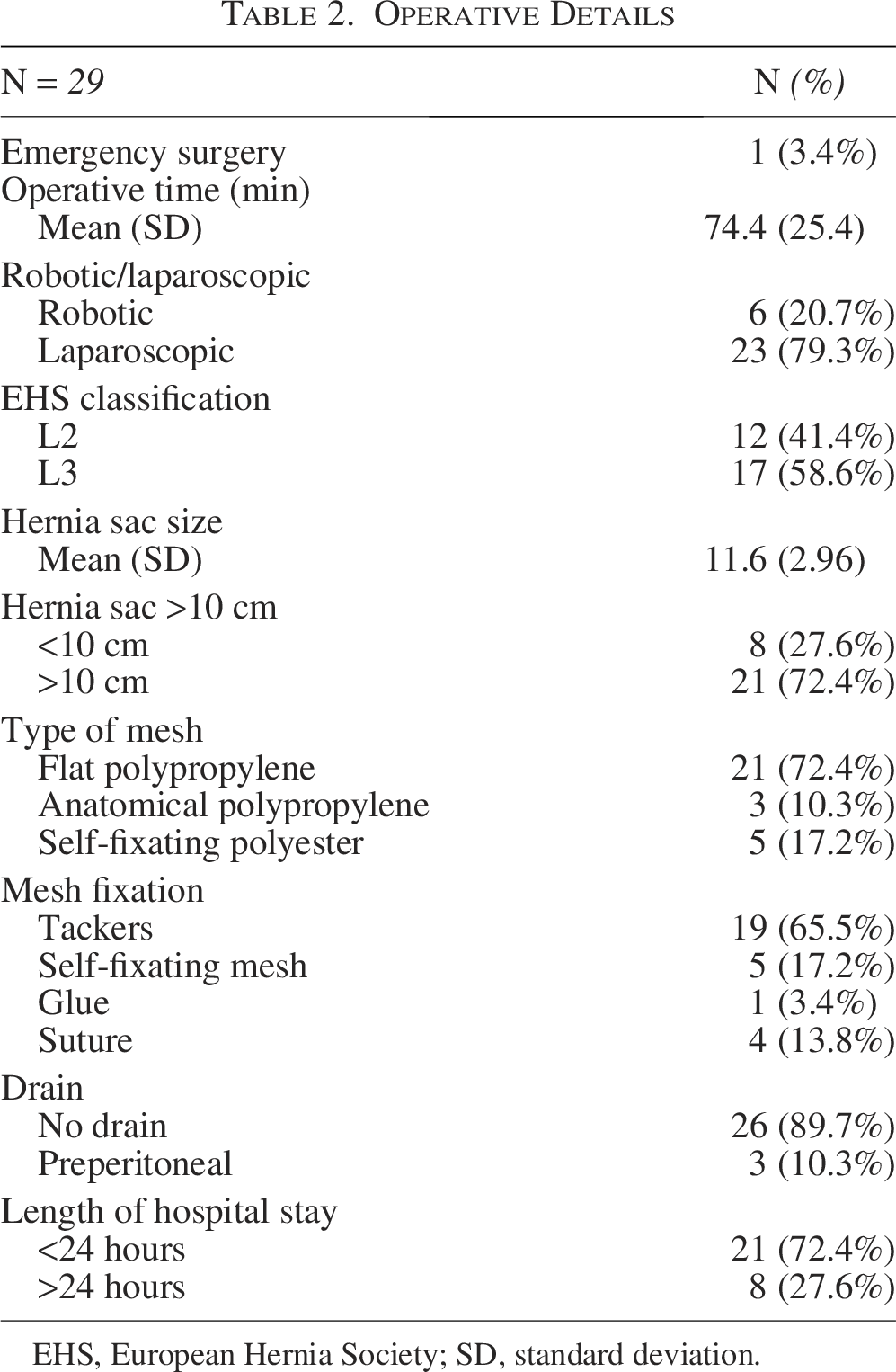
EHS, European Hernia Society; SD, standard deviation.
Eighteen patients (62%) presented seroma at 1-week evaluation. Most seromas were located only in the inguinal region. Larger seromas extending to the scrotum were observed in three patients (10.3%), as detailed in Table 3. One patient presented with ischemic orchitis and no scrotum hematoma was observed. Few port-site or scrotum equimoses were noticed with no further complications.
Postoperative Seroma
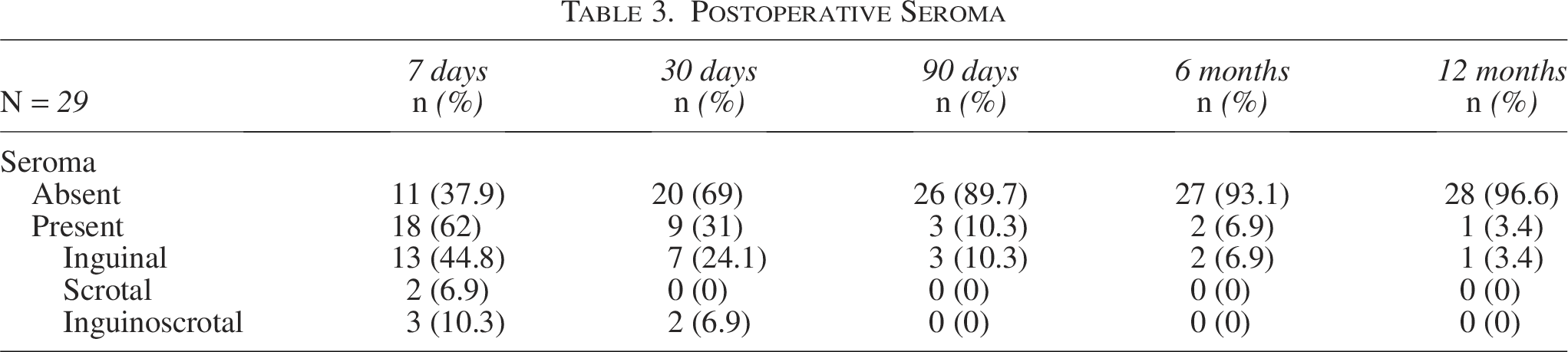
In the 30th postoperative period, nine patients (31%) presented seroma, seven (24.1%) of them classified as inguinal seromas and the remaining two (6.9%) as inguinoscrotal seromas. After 3, 6, and 12 months after the operation, seroma was diagnosed in three (10.3%), two (6.9%), and one (3.4%) patients, respectively (Table 3). During this period of time, all seromas were limited to the inguinal area. Neither seroma aspiration nor drainage was performed. Only conservative measures for reabsorption of the seroma were adopted.
In univariate analysis, the size of the hernia sac showed a positive relationship with the risk of postoperative seroma (Table 4). Patients with no seroma had shorter hernia sac than those with seroma (9.73 ± 1.56 versus 12.7 ± 3.06, respectively, P = .0017) Comparing the subgroups of patients: hernia sac shorter than 10 cm versus longer than 10 cm, the incidence of seroma was significantly higher in the second group (25% versus 76.2% respectively; P = .0348). Similarly, L3 versus L2 EHS hernia classification was also related to a higher risk of postoperative seroma (P = .022).
Risk Factors for Seroma on the 7th Postoperative Day
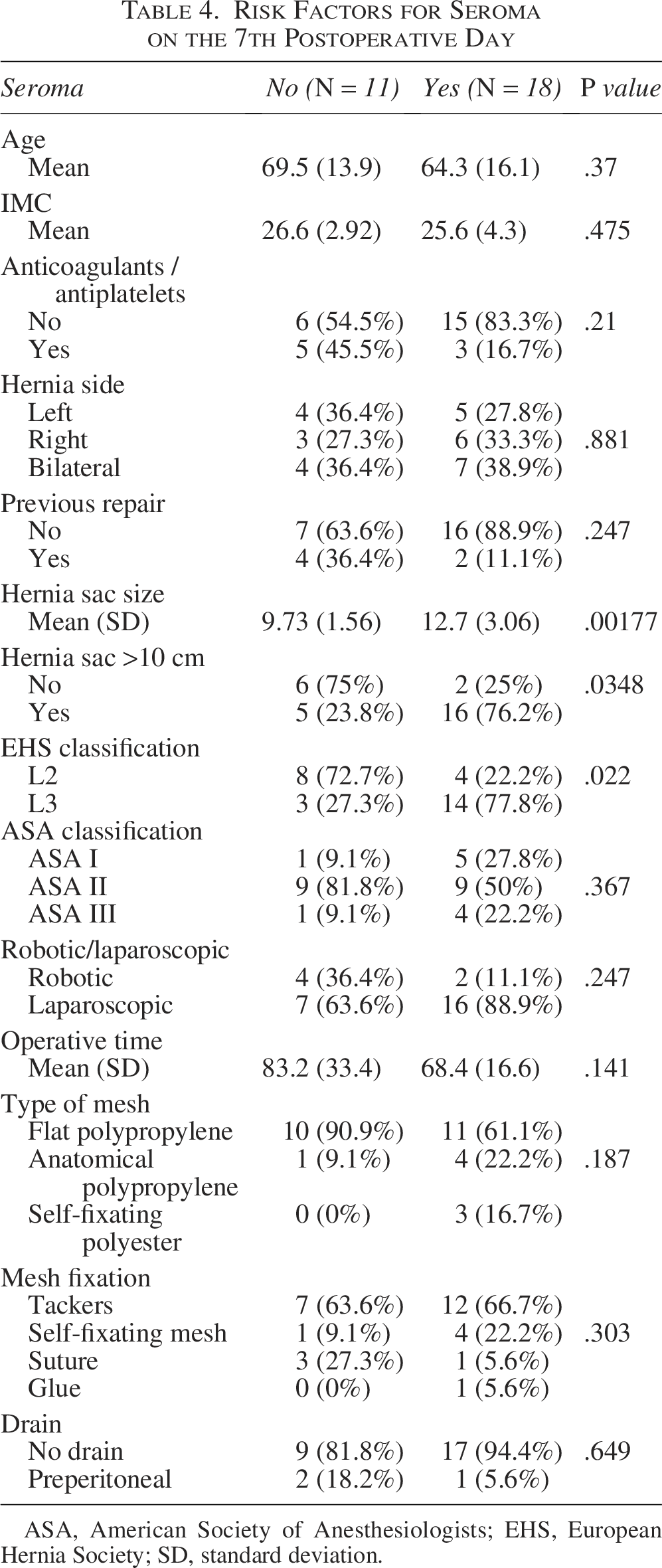
ASA, American Society of Anesthesiologists; EHS, European Hernia Society; SD, standard deviation.
Age, American Society of Anesthesiologists (ASA) classification, BMI, use of anticoagulants/antiplatelet agents, unilateral versus bilateral repair, and primary versus recurrent hernia did not correlate with the risk of postoperative seroma (Table 4). Technical aspects such as laparoscopic versus robotic surgery, type of mesh and fixation, and use of drain also had no effect on the risk of postoperative seroma.
By analyzing the variables potentially related to seroma reabsorption after 30 days (in patients who presented seroma on the 7th postoperative), no factor was found associated with a higher or lower chance of reabsorption, not even the size of the hernia sac, according to Table 5.
Epidemiological Data for Seroma Reabsorption on the 30th Postoperative Day
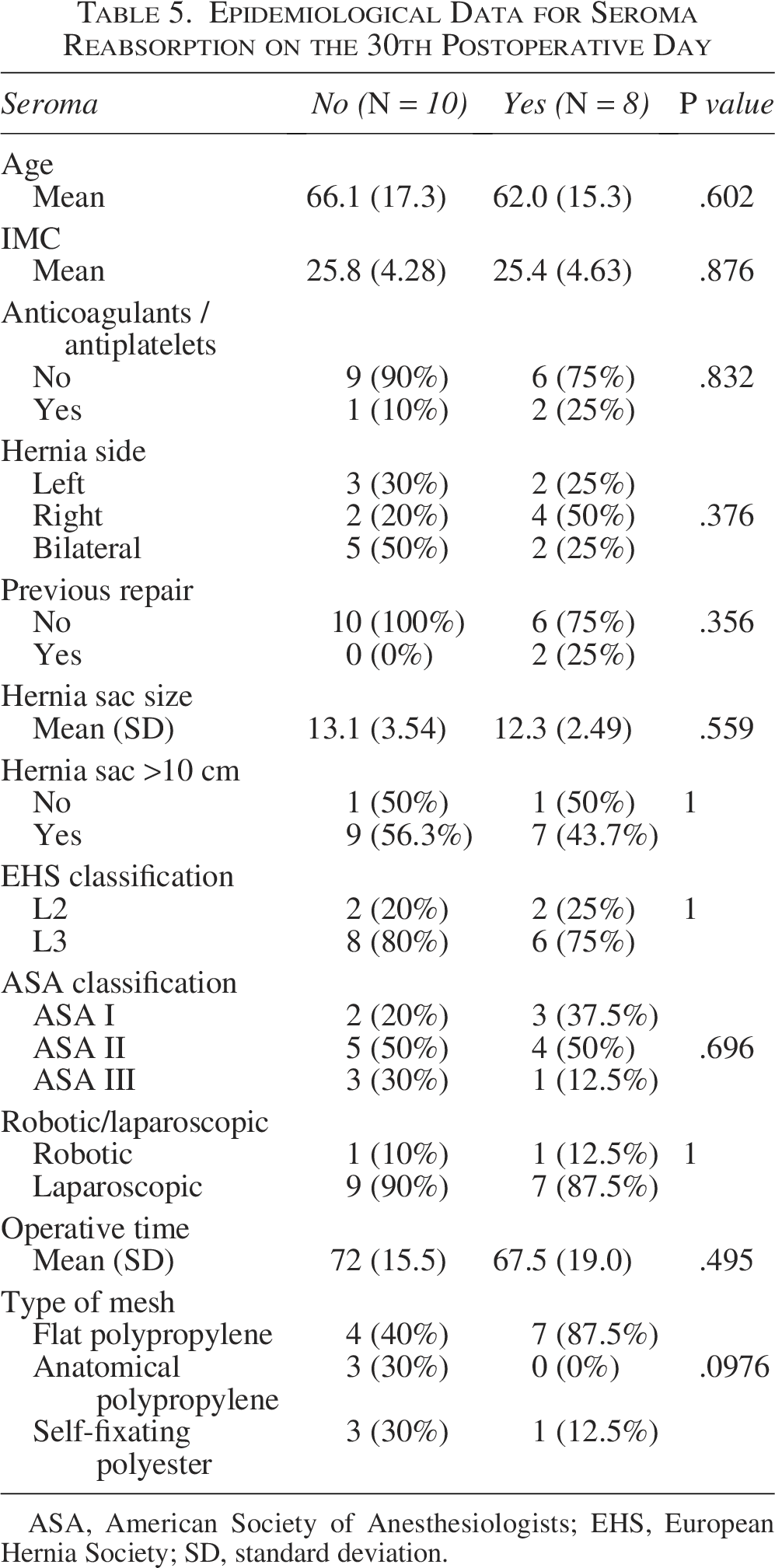
ASA, American Society of Anesthesiologists; EHS, European Hernia Society; SD, standard deviation.
There was no hernia recurrence within the 12-month follow-up period. Likewise, no patient complained of any perceived increase in volume in the scrotum caused by the remaining hernia sac.
Discussion
The incidence of ISH is up to 6% in developed countries, but, in developing or less resourced countries, this percentage rises up to 67% of patients undergoing surgical repair. 1 Although there is no precise definition, these are large hernias in which the abdominal content reaches the scrotum. The main concern from surgical point of view is that when compared with nonscrotal hernias, IHSs present a higher rate of postoperative complications, such as bleeding, seroma, wound infection, re-operation, and also higher risk of recurrence.5–7 ISH may represent a challenge even for experienced surgeons. 16
For a long time, ISHs were considered a contraindication for MIS approaches, whether laparoscopic or robotic.5–7 Although open surgery plays an important role in these repairs, mainly in hernias classified as ISH 3 and/or requiring scrotoplasty, lately MIS techniques became a safety surgical alternative. 17
One of the major challenges in these cases, whether by conventional or MIS approach, is the dissection of the entire hernia sac, which is large and often fibrotic in the scrotum, which is potentially associated with complications such as spermatic cord elements injury, ischemic orchitis, seroma, or hematoma in the scrotum.1,9
Recently, the technique of abandonment of the hernia sac during MIS repairs has gained supporters.8,10,11 The benefit of avoiding the extensive dissection of the hernia sac is potentially a lower complication rate.10,14,18 However, the major concerns about this approach are the risk of postoperative seroma and possibly increase patient’s discomfort due to the hernia sac remnant in the scrotum. Previous series have reported an incidence of seroma in 7%–29% of patients.10,14,18 In our series, 62% of patients had seroma in the 7th postoperative day. However, it is important to emphasize that, in addition to the patients having longer hernia sacs (mean of 11.6 cm from the deep inguinal ring), as the main endpoint of the study was to evaluate the incidence of seroma, any increase in inguinal volume was inferred as a seroma. It is noted that vast majority of seromas were “small” (about three quarts of them)—only located in the inguinal region and just 27.3% of them scrotal or inguinoscrotal seromas.
It is controversial whether the risk of seroma is higher with the technique of abandonment of the hernia sac compared with the procedure of complete dissection of the sac.12,19 Some reports suggest a higher incidence of seroma in cases of sac abandonment. A possible explanation is that the remaining peritoneum in the scrotum could not absorb or even produce liquid.13,20 However, in most published studies, the abandonment was not planned, that is, it occurred due to some difficulty in achieving complete dissection. In contrast, recent randomized controlled trial and meta-analyses have demonstrated a lower risk of seroma in cases of sac abandon potentially due to lower dissection.19,21
The timing of sac abandonment appears to be relevant, as recently demonstrated by Rasador et al. 22 The authors reported a higher incidence of seroma in the sac abandonment group versus complete resection. However, when stratified by timing of abandonment, a significant increase in seroma was observed in the late abandonment group (relative risk (RR) 1.51; 95% confidence interval 1.20, 1.90 P < .001), while no difference was seen between both groups for the primary abandonment.
The incidence of postoperative seroma was higher in patients with longer hernia sacs. Patients with hernia sacs longer than 10 cm had a significantly higher seroma rate than those below 10 cm, 76.2% versus 25%, respectively (P = .03). The relative risk of a patient with a hernia sac longer than 10 cm presenting seroma was almost five times greater than those with a sac shorter than 10 cm (RR = 4.91; 1.19–20.2). This is a different finding from previous report in which no difference was observed. 14 Similarly, patients with EHS L3 hernias had a higher incidence when compared with EHS L2 patients (P = .02). Patient-related factors, such as age, ASA/comorbidities, BMI, and use of anticoagulants/antiplatelet agents, were not correlated with the risk of developing postoperative seroma. In the same way, technical points such as laparoscopic versus robotic approach, type of mesh, and fixation were not related with this complication.
After 30 days postoperatively, in half of the cases the seroma had been reabsorbed (31% of persistent seroma), similar to that has been published by other authors. 14 No aspect related to the patient, the surgical technique, or the type of hernia (not even the size of the hernia sac) had any influence on the reabsorption of the seroma. After 3 and 6 months, only 10.3% and 6.9% of patients presented seroma, respectively.
Previous studies on PAS reported promising results, but most had limitations due to the short period of follow-up of the patients.11,14,18 In our study, we were able to follow the patients prospectively for 12 months, and it was demonstrated that the PAS tactic maintains these results over time. In our series, no cases of hernia recurrence were observed, and only one patient (3.4%) had persistent seroma over 1 year of follow-up. Although, in our series, aspiration and or drainage was not necessary in any patient, we believe that this may be necessary in some patients with large/symptomatic or persistent seroma. Seromas after PAS technique appear to have a benign evolution, that is, they are reabsorbed similar to that is described after complete sac dissection.
Some tactics have been used to reduce seroma after inguinal hernia repair, especially for ISH. 19 Although the use of intraoperative drains placed in the scrotum is recommended by some authors, it is not widely accepted. Most seromas appear from the 3rd/4th day postoperatively, so it would only have a practical effect if the drain was left in place for a relatively long period. In addition, drain placement may increase the risk of infection of the operative site, including the mesh. In our series, the drain was used in only three patients and placed in the dissection space, that is, preperitoneally and not in the scrotum. Indication for placing drain in these cases was due to the need for continued use of antiplatelet/anticoagulant agents. In all cases, the drain was removed within 48 hours.
Regarding other potential complications, one patient (3.4%) was diagnosed with ischemic orchitis, although we believe that this is an underdiagnosed condition after inguinal repairs. No patient presented scrotal hematoma or had recognized injury to the cord elements, which reinforces the advantage of PAS in these patients with large hernias.
We may wonder whether patients in the postoperative period are not bothered by the seroma or by the eventual volume caused by the persistence of part of the hernia sac inside the scrotum. First, it is important to emphasize that patients should be well informed that, even due to the size of the hernia, the occurrence of seroma is frequent and that the vast majority reabsorbs up to 12–16 weeks after surgery. In addition, patients who are used to having part of or all omentum or even several intestinal loops inside the scrotum tend not to be bothered by any small increase in local volume. In most patients, not even the surgeon is able to notice any changes when examining the scrotum of these patients who underwent PAS technique. In our series, no patient complained about increased volume in the scrotum due to the remanent of the hernia sac.
In most studies comparing complete dissection versus sac abandonment, operative time was similar.12,19,22 However, in most cases the abandonment did not occur “primarily” but rather after some attempt at dissection and the type of hernia included were not only ISH. We believe PAS technique is probably associated with shorter operative time for these cases. Although there are no comparative studies, the time to perform the circular incision in the peritoneum and its closure should be shorter than the complete dissection of a large and often fibrotic hernia sac inside the scrotum. 22 In our series, the mean operative time was 74 minutes, and 38% of patients underwent bilateral repair. This may have additional relevance in this group of patients with ISH, who are generally older and have more comorbidities. The median age of our patients was 69 years old, and 80% of them were classified as ASA II or III. Majority of patients (72.4%) were discharged within 24 hours after surgery.
Limitations of the study include the lack of a control group and the relatively small sample size. Furthermore, the arbitrary decision to use hernia sacs longer than 7 cm as the inclusion criterion can also be questioned, even though there is no well-established parameter in the literature. And although 1 year of follow-up for an acute complication such as seroma may be considered sufficient, in general longer follow-ups may be recommended.
Primary or planned abandonment of the hernia sac appears to be a simple and promising alternative for MIS repair of ISHs, which are generally considered complex. In our study, with 1-year follow-up, the incidence of seroma was high, but it should not be different from what occurs after complete dissection for large and fibrotic hernia sacs. Seromas in these cases have a benign evolution and most are reabsorbed spontaneously. The risk of other complications is quite low. A comparative study on abandonment versus complete dissection of the sac specifically in ISH is necessary and may provide a more definitive answer on the application of this technique.
Authors’ Contributions
C.C.: Conceptualization; project administration; methodology; supervision; and writing. J.C.: Validation and writing—review and editing. J.R.: Data curation; investigation; and writing—original draft. A.Z.: Data curation; investigation; and writing—original draft. V.S.: Investigation and validation. G.R.: Investigation and validation.
Footnotes
Acknowledgments
The authors thank Márcia Olandoski for statistical analysis and Hospital Nossa Senhora das Graças for providing facilities and technical equipments.
Author Disclosure Statement
Christiano Claus reports speakers consultancy fees on behalf of Medtronic. Julio Coelho, João Ruggeri, Adriana Zilli, Vivian Sasaki, and Guilherme Rhoden have no conflicts of interest to disclose.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.