
Abstract
Background:
This study aimed to compare the safety and efficacy of laparoscopic sleeve gastrectomy (LSG) and Roux-en-Y gastric bypass (RYGB) in patients aged 60 and older, focusing on postoperative weight loss, improvement in obesity-related comorbidities, and perioperative outcomes.
Methods:
This was a retrospective analysis of data from three bariatric surgery centers with surgeries performed between January 2019 and September 2024. The study included patients aged ≥60 years who underwent either LSG or RYGB. The primary outcome was the comparison of weight loss metrics (excess weight loss [%EWL] and total weight loss [%TWL]) between LSG and RYGB. Secondary outcomes included the remission or improvement of type 2 diabetes mellitus (T2DM) and hypertension (HTN), 30-day postoperative complications, operative time, and length of hospital stay.
Results:
A total of 168 patients aged ≥60 who underwent LSG (n = 130) or RYGB (n = 38) were included. Both procedures resulted in similar weight loss outcomes, with a median %EWL of 58.6% for LSG and 61.2% for RYGB. The median %TWL was 23.1% for LSG and 26% for RYGB, with no significant differences between the groups (P = .275). The operative time was significantly shorter for LSG (60 minutes versus 110 minutes for RYGB, P < .001), and LSG patients had a shorter hospital stay (2 versus 3 days, P < .001). The 30-day complication rate was low for both groups, with no significant difference in complications between LSG and RYGB. Regarding comorbidity resolution, 90.7% of patients with T2DM and 93.6% with HTN experienced improvement or remission. Complete remission was achieved in 39% of all T2DM cases (37.5% in LSG, 42.9% in RYGB) and in 33% of all HTN cases (33.3% in LSG, 31.6% in RYGB), with no statistically significant differences between the groups.
Conclusions:
Bariatric surgery appears safe in older adults when guided by careful patient and procedure selection through multidisciplinary assessment. Both LSG and RYGB yielded comparable weight loss and remission outcomes for T2DM and HTN in this population.
Keywords
Introduction
The global burden of obesity continues to escalate, with significant implications for public health and health care systems worldwide. Metabolic and bariatric surgery (MBS) remains the most effective treatment for sustained weight loss and improvement of obesity-related comorbidities, particularly in patients with severe or medically complicated obesity. Advances in surgical techniques and perioperative care have expanded the safety profile of these procedures across a broader range of patients. 1
Historically, advanced age was viewed as a relative contraindication to MBS due to concerns about perioperative risk and frailty. However, with increasing life expectancy and rising obesity prevalence in older adults, the demand for surgical treatment has grown.2,3 Evidence now suggests that age alone should not exclude patients from receiving bariatric surgery, provided that a thorough multidisciplinary evaluation—including assessment of frailty, functional status, and comorbidity burden—is conducted.1,4
Several studies have demonstrated that older patients can achieve significant weight loss and improvement in comorbidities with complication rates comparable to younger patients5–7 However, the selection of the appropriate surgical procedure and the comparison of outcomes in this age group remain debated.8,9 A meta-analysis comparing Roux-en-Y gastric bypass (RYGB) and laparoscopic sleeve gastrectomy (LSG) in older adults indicated that LSG may offer a superior short-term safety profile with comparable metabolic outcomes. 10 These results suggest that both procedures are effective, though definitive guidance on procedure selection and outcome prediction is still lacking.
The 2022 ASMBS/IFSO joint guidelines emphasize that frailty, rather than chronological age, should guide patient selection for bariatric surgery. Nevertheless, further research is needed to clarify optimal procedure choice and outcomes among older adults.1,11 This study aims to retrospectively evaluate the safety and efficacy of LSG and RYGB in patients aged over 60 years. The age threshold of 60 years was chosen in accordance with previous bariatric studies and meta-analyses evaluating outcomes in older populations.5,10 Specifically, we compared postoperative complication rates, weight loss trajectories, and improvement in obesity-related comorbidities to inform evidence-based surgical decision-making in the older population.
Methods
Study design and ethical approval
This study was conducted as a retrospective analysis of data from three bariatric surgery centers in Istanbul, with surgeries performed between January 2019 and September 2024. The study protocol was approved by the Ethics Committee of Marmara University (Approval No: 09.2024.302). The study adhered to the ethical principles of the Declaration of Helsinki and followed all relevant national regulations.
Patient and procedure selection, and eligibility criteria
Patients aged 60 years or older with a preoperative body mass index (BMI) of ≥35 kg/m2 who underwent primary LSG or RYGB for the treatment of obesity were included in this study. All patients were thoroughly evaluated by a multidisciplinary team prior to surgery, which included specialists from geriatrics, cardiology, pulmonology, anesthesia, endocrinology, and other relevant fields. As part of the routine preoperative workup, all patients underwent abdominal ultrasound and esophagogastroduodenoscopy. In all participating institutions, patients were also required to obtain nutritional and psychological clearance, achieve medical optimization of comorbidities, and demonstrate adherence to lifestyle modification programs before being approved for surgery.
Based on the comprehensive preoperative evaluation, each patient received individualized counseling to determine the most appropriate surgical procedure according to clinical characteristics, comorbidity profile, and surgical risk.
Exclusion criteria included previous bariatric, hiatal, esophageal, gastric, anti-reflux surgery, incomplete clinical records, loss of follow-up, and patients who did not receive approval from the multidisciplinary team. A minimum follow-up period of 3 months after surgery was required for inclusion in the analysis.
Surgical techniques
All procedures were performed laparoscopically under general anesthesia by experienced bariatric surgeons. In the LSG group, a 36 French bougie was used for calibration, and the gastric transection was initiated 4–6 cm proximal to the pylorus. The stomach was resected along the greater curvature up to the angle of His. The entire staple line was routinely oversewn with a continuous absorbable suture and reinforced with an omental patch (omentopexy).
For the RYGB, a gastric pouch (50–70 mL) was created, and the jejunum was divided 75–100 cm distal to the ligament of Treitz. The alimentary limb was measured between 100 and 125 cm depending on BMI and institutional preference. A side-to-side gastrojejunostomy was constructed using a linear staple. To minimize the long-term risk of internal herniation, all mesenteric and Petersen’s defects were routinely closed with a non-absorbable suture. All patients received perioperative care, including venous thromboembolism prophylaxis, proton pump inhibitors, and micronutrient supplementation according to ERAS-based protocols.
Postoperative management followed institutional protocols emphasizing early ambulation and oral intake. Discharge criteria included hemodynamic stability, tolerance of oral liquids, adequate pain control, and absence of postoperative complications such as bleeding, fever, or nausea/vomiting.
Outcomes
The primary outcome of the study was the comparison of the percentage of total weight loss (%TWL) between the LSG and RYGB groups.
Secondary outcomes included:
Percentage of excess weight loss (%EWL) and current BMI Improvement or remission of type 2 diabetes mellitus (T2DM) and hypertension (HTN) Incidence of 30-day postoperative complications, classified according to the Clavien–Dindo system Operative time Length of hospital stay
Definitions of comorbidity remission and improvement
Comorbidity remission and improvement were defined according to standardized criteria described by Brethauer et al. (2015). 12 Other comorbidities, such as dyslipidemia and obstructive sleep apnea, were recorded at baseline but were not included in remission analysis due to nonstandardized follow-up data and lack of consistent remission criteria.
Data collection
Demographic variables, comorbidities, operative characteristics, complications, and weight loss outcomes were extracted from institutional electronic medical records and maintained in bariatric databases. Weight loss metrics (%EWL and %TWL) were calculated using standardized formulas. 12 For %EWL calculation, ideal weight was defined as the weight corresponding to a BMI of 25 kg/m2 for each patient’s height. Current weight and BMI values were obtained from the most recent follow-up visit available for each patient.
Sample size calculation
To evaluate whether the sample size was adequate to detect clinically meaningful differences in weight loss outcomes between groups, a power analysis was performed. Based on prior literature reporting small-to-moderate effect sizes (Cohen’s d ≈ 0.3) for %EWL differences between LSG and RYGB, a total sample size of 150 was estimated to provide 80% power with a significance level of 0.05. With 168 patients included (LSG: 130; RYGB: 38), the sample size was deemed sufficient to detect clinically relevant differences in primary outcomes. Although the number of patients differed between the two groups, post-hoc power analysis confirmed that the sample was adequate.
Statistical analysis
Continuous data were expressed as mean ± standard deviation (SD) for normally distributed variables and as median and min–max values for abnormally distributed variables. Categorical data were presented as frequencies and percentages. The normality of the variables was assessed using the Kolmogorov-Smirnov test. Continuous values were compared between the groups using appropriate statistical tests: the Mann–Whitney U test for nonparametric data and the Student’s t-test for parametric data. Categorical variables were analyzed using the chi-square test or Fisher’s exact test when appropriate. Chi-squared analysis was initially performed on a 4 × 2 contingency table to compare comorbidity outcomes between the groups. However, the analysis was invalid due to more than 20% of expected cell frequencies being less than 5. To resolve this issue, certain categories were combined as follows: Change versus No Change, Complete Remission versus Partial Remission, Improvement or No Change, and Partial and Complete Remission versus Improvement or No Change. After these adjustments, the chi-squared test was reapplied to assess group differences. A P value of <.05 was considered statistically significant. All statistical analyses were performed using SPSS software for Mac, version 26 (IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
A total of 272 patients aged 60 years or older underwent LSG or RYGB during the study period across the three participating bariatric centers. Of these, 67 patients were excluded due to revisional bariatric surgery, 30 were lost to follow-up, and 7 patients had a history of previous gastric or anti-reflux surgery. After applying these criteria, 168 patients were eligible and included in the final analysis: 130 (77.4%) underwent sleeve gastrectomy, and 38 (22.6%) underwent RYGB. The median age was 62 years (range: 60–72), and 70% of the cohort were female. Baseline demographic variables, including age, gender distribution, BMI, and comorbidity burden, were similar between the groups.
The most common comorbidities were HTN (56%), T2DM (32.3%), dyslipidemia (28.6%), and obstructive sleep apnea (20.8%). There were no statistically significant differences in the distribution of comorbidities between the two groups (Table 1).
Demographic Parameters of Patients
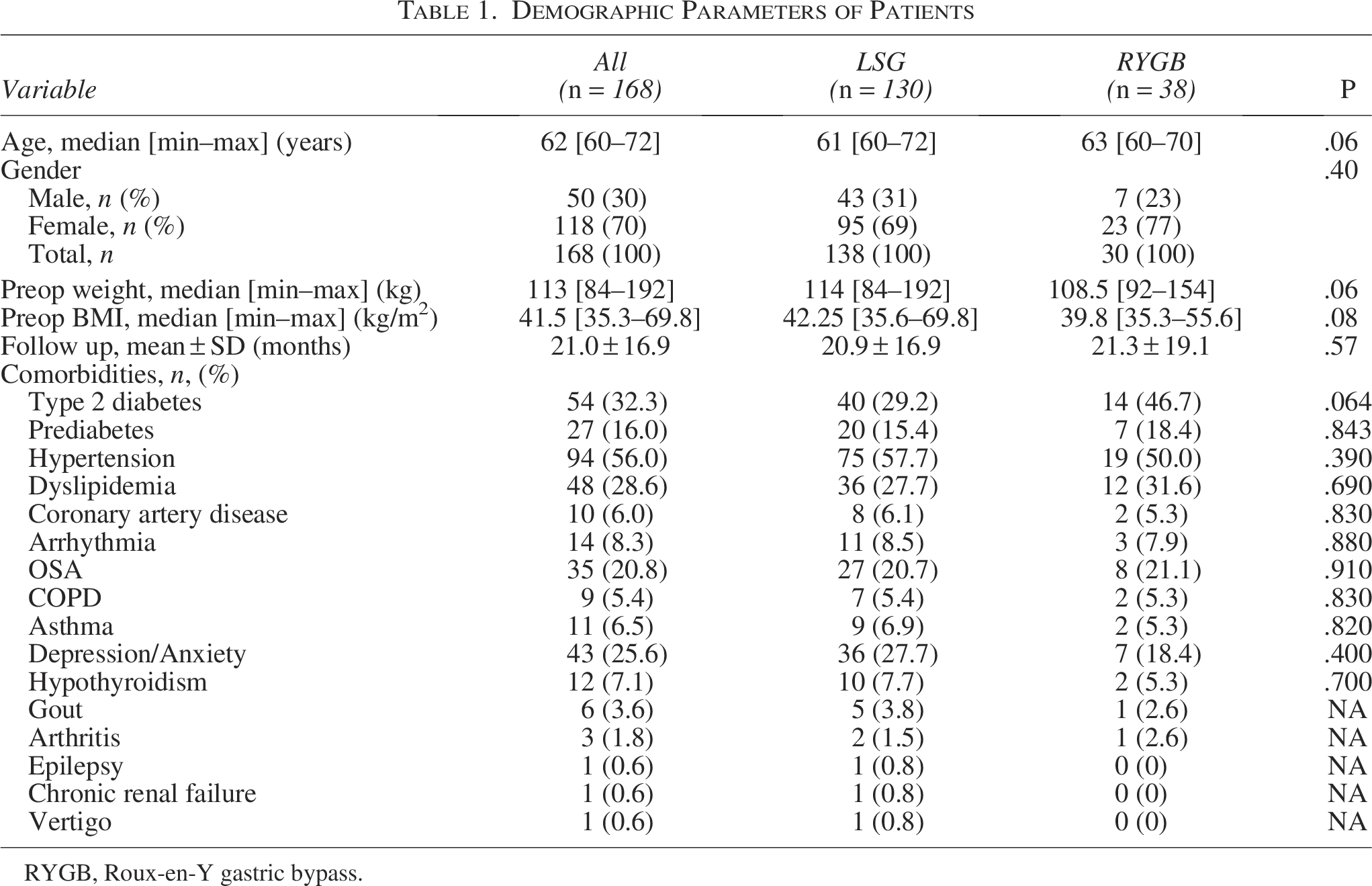
RYGB, Roux-en-Y gastric bypass.
Weight loss outcomes
At a mean follow-up of 21.0 ± 16.9 months, the overall median %TWL was 24.2%, and %EWL was 59.1%, with no significant difference between surgical groups (P = .275 and P = .266, respectively). The RYGB group showed a slightly lower median BMI at follow-up (30.5 versus 32.0 kg/m2), although not statistically significant (P = .111) (Table 2).
Operative and Weight Loss Outcomes of Groups
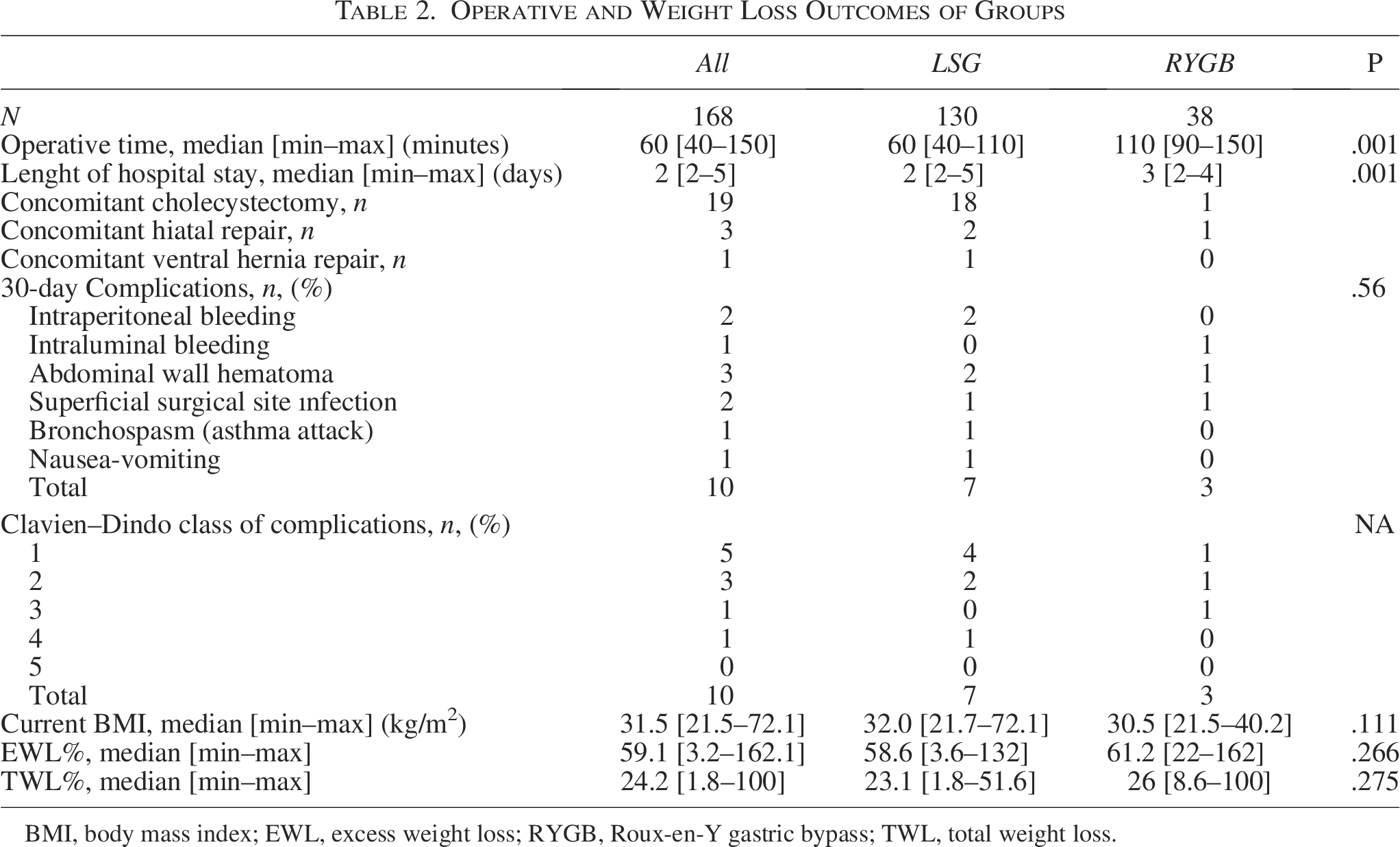
BMI, body mass index; EWL, excess weight loss; RYGB, Roux-en-Y gastric bypass; TWL, total weight loss.
Comorbidity outcomes
Among patients with preoperative type 2 diabetes (n = 54), 90.7% experienced improvement or remission postoperatively, with no significant difference between groups. Complete remission was observed in 39% of cases. Similarly, patients with HTN (n = 94) showed improvement or remission in 93.6% of the cases, with comparable results between LSG and RYGB.
While adjusting for low expected frequencies in contingency tables, categories were combined as follows: Change versus No Change, Complete Remission versus Partial Remission, Improvement or No Change, and Partial & Complete Remission versus Improvement or No Change. After these adjustments, no significant differences were observed between LSG and RYGB in T2DM or HTN outcomes.
For T2DM, any improvement or remission (Change) was observed in 92.5% of LSG and 85.7% of RYGB patients (P = .83). Complete or partial remission occurred in 55.0% of LSG and 57.2% of RYGB patients (P = 1.00), while complete remission alone was achieved in 37.5% of LSG versus 42.9% of RYGB (P = .97).
For HTN, any improvement or remission (Change) was observed in 93.3% of LSG and 94.7% of RYGB patients (P = 1.00). Complete or partial remission occurred in 46.6% of LSG and 68.4% of RYGB patients (P = .15), and complete remission alone in 33.3% of LSG versus 31.6% of RYGB (P = 1.00) (Table 3).
Diabetes and Hypertension Remission and Improvement Rates by Bariatric Procedure
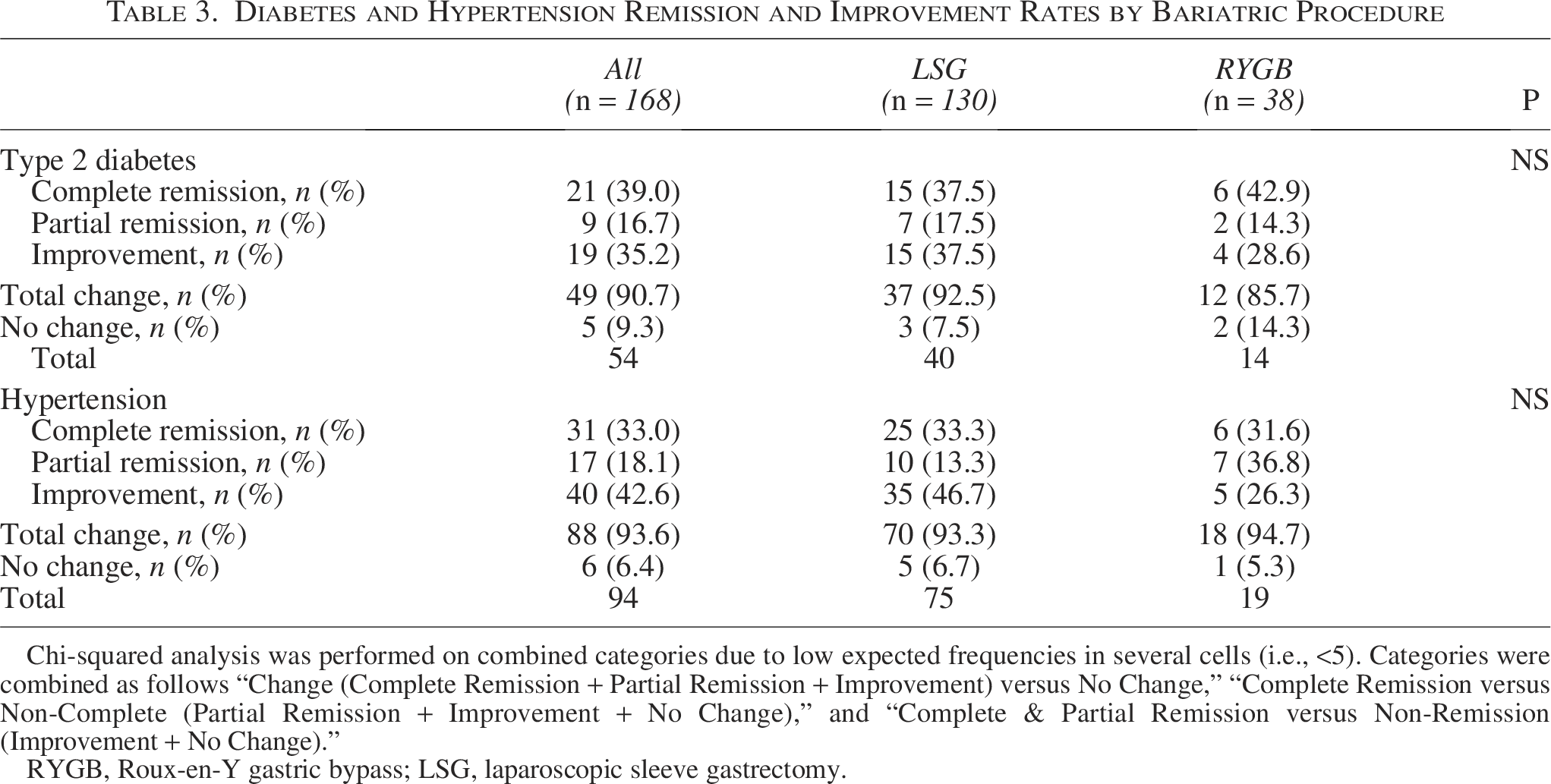
Chi-squared analysis was performed on combined categories due to low expected frequencies in several cells (i.e., <5). Categories were combined as follows “Change (Complete Remission + Partial Remission + Improvement) versus No Change,” “Complete Remission versus Non-Complete (Partial Remission + Improvement + No Change),” and “Complete & Partial Remission versus Non-Remission (Improvement + No Change).”
RYGB, Roux-en-Y gastric bypass; LSG, laparoscopic sleeve gastrectomy.
Operative and postoperative outcomes
Operative time was significantly longer in the RYGB group (median: 110 minutes) compared with the LSG group (median: 60 minutes, P < .001). Length of hospital stay was also longer in the RYGB group (median: 3 versus 2 days, P < .001).
Thirty-day postoperative complications occurred in 10 patients (5.9%), with no mortality reported. Complications included intraperitoneal bleeding (n = 2), intraluminal bleeding (n = 1), abdominal wall hematoma (n = 3), superficial surgical site infection (n = 2), bronchospasm (n = 1), and nausea/vomiting (n = 1). Complication severity was mostly low (Clavien–Dindo grade I–II), and there was no significant difference in complication rates between LSG and RYGB groups (P = .56) (Table 2).
Discussion
This retrospective multicenter study aimed to compare the safety and efficacy of LSG and RYGB in patients aged 60 and older. Our results demonstrated that both LSG and RYGB were associated with significant weight loss and improvement in obesity-related comorbidities, with acceptable and low complication rates in this population. The weight loss outcomes between the two procedures were similar, with median %TWL and %EWL showing no significant differences, suggesting that both procedures are effective in achieving sustained weight loss in older adults. Despite growing evidence, data comparing LSG and RYGB specifically in patients over 60 remain limited. Our study contributes to this gap by providing real-world, multicenter data focused on older patients, a group often underrepresented in bariatric literature.
In our study, both LSG and RYGB achieved substantial weight loss in patients aged 60 years and older. The median %EWL was 58.6% for LSG and 61.2% for RYGB, with a %TWL of 23.1% and 26.0%, respectively. These outcomes are consistent with those reported by Dowgiałło-Gornowicz et al., who found mean %EWL and %TWL values of 49.0% and 20.1% for LSG and 57.8% and 21.7% for RYGB in a large Polish cohort of patients over 65 years. 13 The similarity in results across studies highlights the effectiveness of both procedures in achieving clinically meaningful weight reduction in older populations.
In terms of metabolic outcomes, our study demonstrated that complete or partial remission of T2DM occurred in 55.0% of LSG patients and 57.2% of RYGB patients, while complete or partial remission of HTN was achieved in 46.6% of LSG and 68.4% of RYGB patients. These remission rates are consistent with those reported by Dowgiałło-Gornowicz et al., who found complete or partial remission in 63.7% of patients with T2DM and 45.9% with HTN following bariatric surgery in individuals over 65 years. 13 While our T2DM remission rates are slightly lower, our HTN remission rates—particularly after RYGB—appear even higher. These differences may be attributed to variation in follow-up duration, remission definitions, or baseline disease severity. Nevertheless, both studies confirm that bariatric surgery is effective in improving obesity-related comorbidities in the older population.
Perioperative outcomes in our cohort further support the safety of bariatric surgery in older adults. The median operative time and hospital stay were notably shorter for LSG (60 minutes, 2 days) compared to RYGB (110 minutes, 3 days). Our overall 30-day complication rate was 5.9%, with no perioperative mortality. These outcomes compare favorably with the complication rate of 7.0% reported by Dowgiałło-Gornowicz et al., which included a 1.1% leak rate and no deaths. 13 Also, in a recent study by Barajas-Gamboa et al., it was noted that primary and revisional bariatric surgeries provided significant weight loss and metabolic improvements, with acceptable risks and low complication rates in patients aged 60 and older. 14 Additionally, Xu et al. found significantly higher early complications and mortality risks for RYGB versus LSG in older patients. 10 Differing from the meta-analysis conducted by Xu et al. in our study, no significant differences were observed between LSG and RYGB regarding 30-day morbidity and mortality in the older patient group. The study by Xu et al. encompasses a larger sample size due to its meta-analytic design. The consistency of our results with these studies underscores the importance of experienced surgical teams, standardized perioperative protocols, perioperative multidisciplinary evaluation and individualized treatment decision in achieving favorable outcomes for older bariatric patients.
Although both LSG and RYGB are established and effective bariatric procedures, the present study was not designed to determine procedural superiority or to guide surgical decision-making. Our results indicate that in patients aged 60 years and older, LSG and RYGB yield comparable outcomes in terms of weight loss and remission of obesity-related comorbidities such as type 2 diabetes and HTN. These findings suggest that either procedure may be considered safe and effective in appropriately selected older adults.
While RYGB is associated with a higher technical complexity and a risk of procedure-specific complications such as marginal ulcer, internal herniation, and dumping syndrome, these outcomes were not directly evaluated in our analysis. 15 Similarly, LSG carries potential risks, including postoperative gastroesophageal reflux disease (GERD) and stricture formation, which also warrant consideration. 15 In this context, our findings should be interpreted as supporting comparable short- to mid-term efficacy rather than advocating for a particular procedure. Overall, our findings highlight the importance of individualized, multidisciplinary assessment in guiding procedure choice for older patients undergoing bariatric surgery.
This study has several limitations. First, its retrospective, nonrandomized design introduces potential selection bias, as treatment decisions were based on clinical judgment rather than random allocation. Factors such as frailty or GERD severity may have influenced procedure choice, and the study was not powered to control for these confounders. Second, the small sample size of the RYGB group (n = 38) limits statistical power for secondary outcomes such as complication and remission rates. Although a matched analysis approach was considered to address this imbalance, it was ultimately deemed methodologically unsuitable. Matching 38 RYGB patients with an equal number of LSG patients would have reduced the cohort to 76 total patients, resulting in a substantial loss of statistical power and an increased risk of type II error. More importantly, such matching would have limited the external validity and real-world representativeness of the findings, which was a key objective of this multicenter analysis. Third, the reliance on existing clinical records may have resulted in missing data, and long-term outcomes—particularly nutritional deficiencies and reflux-related complications—were not assessed. Finally, although the study included three bariatric centers with standardized protocols, the findings may not be generalizable to lower-volume or less experienced settings. Future prospective studies with larger, balanced cohorts and extended follow-up are warranted to evaluate nutritional status, quality of life, and long-term functional outcomes in older adults undergoing bariatric surgery.
Conclusion
Our study supports the safety and effectiveness of both LSG and RYGB in older patients. Comparable outcomes were observed in terms of weight loss and remission of obesity-related comorbidities, including T2DM and HTN. These results may reflect the individualized, multidisciplinary approach to patient and procedure selection applied across centers. Future prospective studies are warranted to evaluate long-term nutritional, reflux-related, and quality-of-life outcomes in this population.
Human Ethics, Ethics Approval, and Consent to Participate
This study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. The study was approved by the Ethics Committee of Marmara University (Approval No: 09.2024.302). All participants provided written informed consent for participation in the study. All patients included in the study provided informed consent for participation. The consent was obtained in writing, and participants were fully informed about the study’s objectives, procedures, and potential risks. Additionally, all participants were assured of the confidentiality of their personal and medical information, which was anonymized before analysis.
Consent for Publication
Informed consent for publication was obtained from all individual participants included in the study. The participants’ consent covers publication of anonymized data related to their health and surgical outcomes.
Authors’ Contributions
Conceptualization—M.B.S.O., A.Ş., and K.Y.; Data curation—N.Ö., C.A.F., and H.K.; Formal analysis—A.Ş., M.S.D., and K.Y.; Funding acquisition—A.Ş. and K.Y.; Investigation—M.S.D., N.Ö., and K.Y.; Methodology—A.Ş., M.S.D., and M.B.S.O.; Project administration—A.Ş., M.S.D., and K.Y.; Resources—M.S.D. and C.A.F.; Software—N.Ö., M.S.D., and M.B.S.O.; Supervision—K.Y. and A.Ş.; Validation—M.S.D., A.Ş., and C.A.F.; Visualization—M.S.D. and H.K.; Writing—original draft—M.S.D., A.Ş., and H.K.; Writing—review and editing—A.Ş. and M.S.D.
Footnotes
Funding Information
The authors declare that no funding was received for the conduct of this study or the preparation of this article.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. All data are stored in compliance with institutional guidelines for data protection.
Disclosure Statement
The authors declare that they have no conflict of interest. The authors declare that they have no competing interests. No financial or nonfinancial conflicts of interest have been identified in relation to this study.