
Abstract
Introduction:
Extragonadal germ cell tumors in pediatric patients are rare, accounting for approximately 10 to 15% of all germ cell tumors. High-risk chemotherapy followed by surgical resection represents the standard of care. Post-hepatectomy biliary complications, such as hepatic duct stenosis, constitute a relevant clinical challenge.
Case Presentation:
We present the case of a 10-year-old pediatric patient with a retroperitoneal and mediastinal extragonadal germ cell tumor treated with high-risk chemotherapy according to the GALOP 2017 protocol and multiple surgical procedures, including laparoscopic atypical left hepatectomy for residual disease. The patient subsequently developed stenosis of the main hepatic duct. Percutaneous biliary drainage and balloon cholangioplasty were performed, successfully restoring biliary patency and normalizing liver function tests, without immediate complications.
Discussion:
Post-hepatectomy biliary complications in pediatric patients, although uncommon, may be related to mechanical trauma or metallic clip placement. Percutaneous management is effective and safe, allowing avoidance of open reintervention. Multidisciplinary planning is essential to optimize outcomes in high-risk pediatric germ cell tumors.
Conclusion:
Post-hepatectomy biliary stenosis should be considered in pediatric patients presenting with jaundice and cholestasis. Percutaneous management of biliary complications is a safe and effective alternative, highlighting the importance of early intervention and close follow-up to preserve liver function.
Keywords
Introduction
Extragonadal germ cell tumors represent a rare entity in pediatric patients, accounting for approximately 10–15% of germ cell tumors in children. 1 Among these, mediastinal and retroperitoneal tumors may reach a significant size prior to diagnosis, leading to symptoms caused by compression of adjacent structures such as the intestine, urinary tract, and biliary ducts. 2 Elevated tumor markers, including alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (β-hCG), aid in subtype differentiation and assessment of risk stratification and therapeutic response.
Standard treatment consists of chemotherapy according to international protocols, 1 followed by surgical resection of residual masses when chemoresistant or mature components are present. 2 In cases involving hepatic compromise, liver resection may be indicated to achieve local tumor control.
Although laparoscopic liver resection is considered safe and effective, with low morbidity and mortality in experienced hands, it may be associated with postoperative biliary complications. Among these, bile leakage and hepatic duct stenosis represent clinically significant events, potentially presenting with jaundice, cholestasis, abdominal pain, and abnormal liver function tests. Early diagnosis and timely intervention—through percutaneous drainage, cholangioplasty, or reconstructive surgery—are essential to preserve hepatic function and improve clinical outcomes.
This report describes a pediatric patient with a retroperitoneal extragonadal germ cell tumor who underwent high-risk chemotherapy and multiple surgical resections and subsequently developed stenosis of the main hepatic duct following an atypical left hepatectomy, requiring percutaneous biliary drainage and cholangioplasty to resolve cholestasis.
Case Presentation
A 10-year-old patient with a history of multiple consultations for constipation presented with abdominal pain associated with abdominal distension, vomiting, and constipation. Physical examination revealed a hard, fixed abdominal mass occupying the central abdomen and extending to the hypogastrium and both iliac fossae. Ultrasound, computed tomography, and magnetic resonance imaging demonstrated a heterogeneous central abdominal mass with well-defined borders, containing solid and cystic components, measuring 119 × 188 mm. An additional calcified 2 × 2 cm mass was identified in the anterior mediastinum.
Tumor marker assessment revealed AFP 4603.4 ng/mL and β-hCG 5.4 mIU/mL. A diagnosis of high-risk secretory germ cell tumor with mediastinal metastatic involvement was established. 3
Treatment was initiated according to the GALOP 2017 protocol. During chemotherapy, the patient experienced several complications, including extended-spectrum beta-lactamase (E. coli) urinary tract infection, catheter-related infections, and syndrome of inappropriate antidiuretic hormone secretion secondary to chemotherapy.
After six cycles, tumor progression was observed, leading to compression of the urinary tract with bilateral hydronephrosis and compression of the common bile duct. A planned surgical procedure was performed, including bilateral double-J stent placement, right oophorectomy, and resection of peritoneal implants.
Early tumor recurrence occurred, requiring laparotomy and tumorectomy. Subsequent MRI revealed residual disease at the level of the round ligament. Following multidisciplinary discussion, a laparoscopic atypical left hepatectomy was indicated for a residual germ cell tumor involving hepatic segments II and III.3,4
Surgical Technique
The patient was placed in the supine position under general anesthesia. A cold scalpel umbilical incision was made, and the abdominal cavity was entered under direct vision. A 10-mm trocar was placed, pneumoperitoneum was established, and a 30° laparoscope was introduced. Exploration revealed multiple hepatoparietal, enteroenteric, and enteroparietal adhesions. A lesion involving segments II/III was identified, with no additional macroscopic findings.
Two 10-mm trocars were placed in the right and left flanks, and a 5-mm trocar in the epigastrium. Adhesiolysis was performed using blunt dissection and a harmonic scalpel for hepatic mobilization (Fig. 1). The left hepatic vein was dissected and divided using two 45-mm linear staplers. The transection plane was marked with a hook, and parenchymal transection was performed using energy devices. The specimen was divided using three 60-mm vascular linear staplers. Meticulous hemostasis was achieved, the cavity was irrigated and dried, and the specimen was retrieved through an enlarged right flank port site. Fibrillar hemostatic material was applied to the resection bed, and a drain was placed. Layered closure was performed.
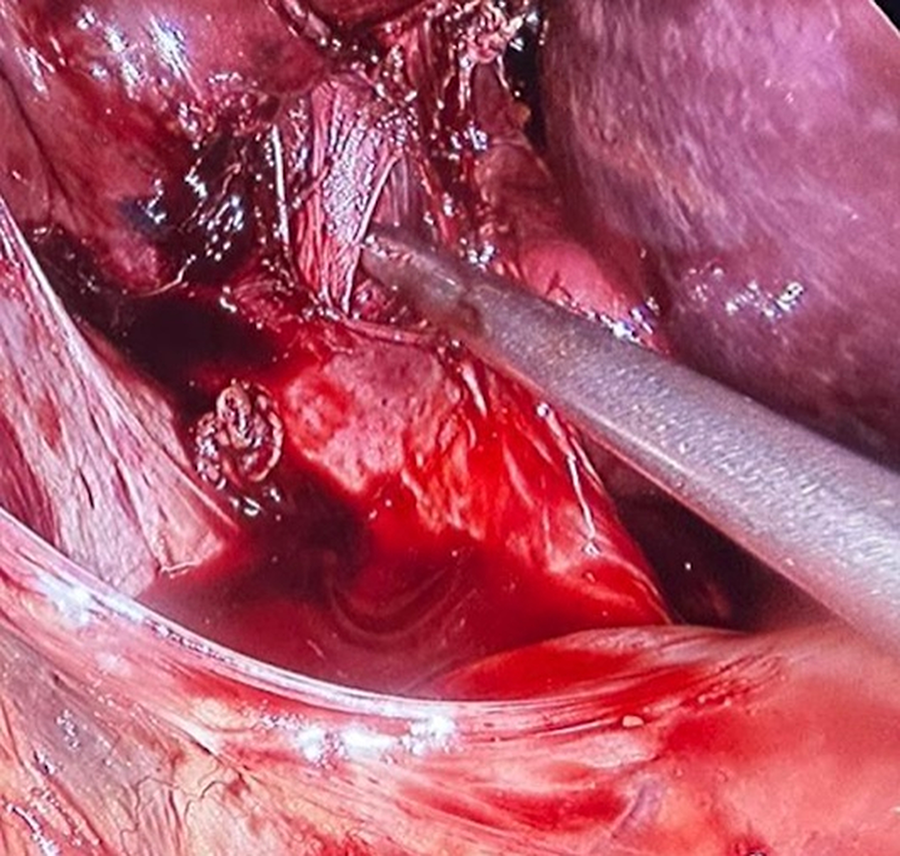
Release of adhesions with harmonic scalpel.
Postoperatively, the patient developed abdominal pain, mucocutaneous jaundice, and a cholestatic pattern on liver function tests. Imaging studies prompted biliary drainage placement. An 8.5-Fr right external biliary drain was inserted.
Under general anesthesia, a right transhepatic cholangiography was performed using a 22-G Chiba needle. Contrast injection demonstrated the absence of distal contrast passage. A 0.018-inch guidewire was advanced, and a D’Agostino biliary introducer was placed. Fistulography was performed, followed by insertion of a 4-Fr angiographic catheter with a 0.035-inch hydrophilic guidewire. The obstruction at the hepatic duct confluence could not initially be crossed, and an 8.5-Fr multipurpose catheter was placed using the Seldinger technique, forming a pigtail. Final fistulography was satisfactory, and the procedure was well tolerated without immediate complications.
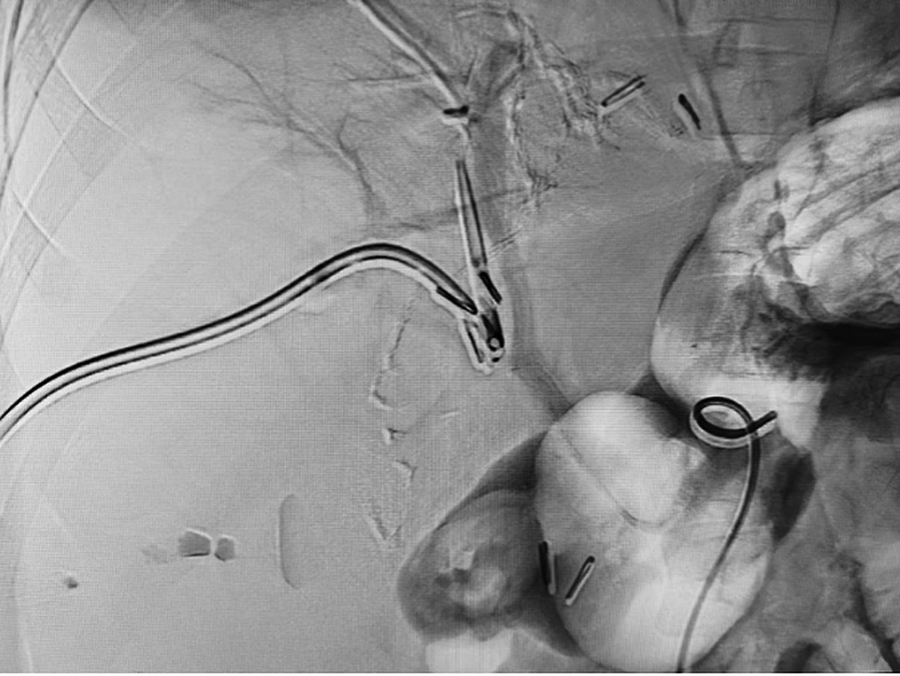
On the third day after catheter placement, hepatic arteriography and indirect portography showed no vascular injury. Transcatheter cholangiography revealed occlusion of the main hepatic duct approximately 1 cm from its origin, associated with adjacent metallic clips (Figs. 2 and 3). A hydrophilic guidewire was advanced, the catheter was withdrawn, and the stenosis was successfully crossed toward the intestinal loop. Repeat cholangiography demonstrated restored biliary continuity, with reduced caliber at the hepatic duct corresponding to clip placement. Balloon cholangioplasty was performed, achieving satisfactory biliary patency on control imaging (Fig. 4).
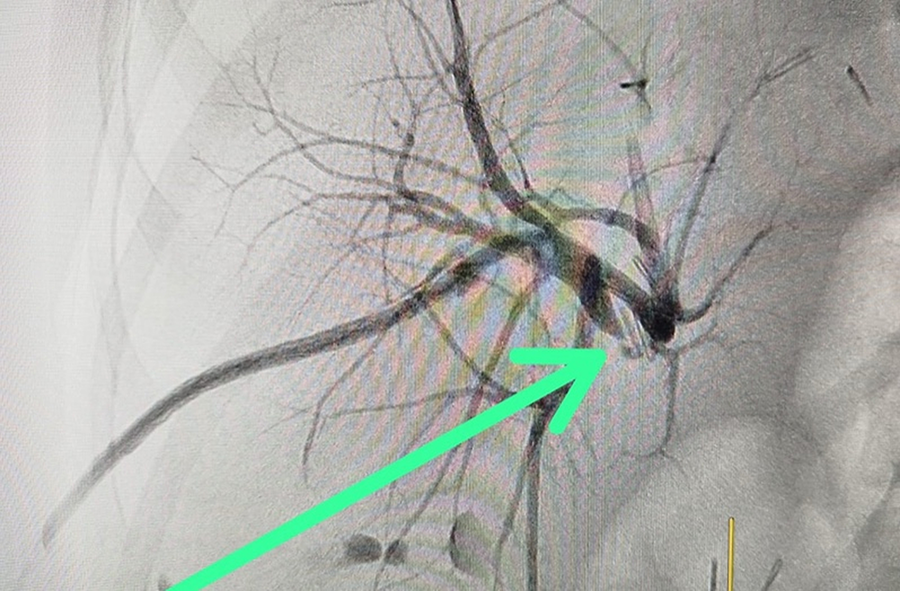
Cholangiography revealed occlusion of the main hepatic duct.
Metal clips in the biliary tract.

Cholangiography demonstrated restored biliary continuity.
Follow-up laboratory tests demonstrated normalization of liver function parameters, and the patient was discharged in good clinical condition, continuing outpatient follow-up.
Discussion
Biliary complications following hepatectomy, 5 although less frequent in pediatric patients than in adults, represent a significant diagnostic and therapeutic challenge. 6 Reported bile leak rates after hepatectomy range from 5 to 10%, while postoperative biliary stenosis occurs less frequently and is usually associated with major resections, mechanical trauma from surgical clips, or manipulation of the hepatic hilum. 7 In the present case, stenosis of the main hepatic duct was related to adjacent metallic clips, underscoring the role of surgical manipulation and hemostatic materials as predisposing factors.
Percutaneous and endovascular management of biliary stenosis has demonstrated high efficacy and low risk in pediatric patients. 8 Balloon cholangioplasty allows restoration of ductal patency without the need for open surgery, reducing postoperative morbidity and length of hospital stay. In this patient, percutaneous intervention led to the resolution of jaundice and normalization of liver function tests, confirming the value of this approach as a first-line strategy for post-hepatectomy biliary stenosis. 9
This case also highlights the complexity of managing high-risk pediatric germ cell tumors, where intensive chemotherapy, multiple surgical interventions, and residual disease increase the risk of biliary and vascular complications. 2 Multidisciplinary planning involving pediatric oncology, hepatobiliary surgery, and interventional radiology5,8 is crucial to optimize clinical outcomes and minimize postoperative morbidity.
Conclusion
Post-hepatectomy biliary stenosis, although uncommon, should be considered in pediatric patients presenting with jaundice and cholestasis following liver resection. Percutaneous balloon cholangioplasty represents a safe and effective therapeutic alternative. Close surveillance and timely intervention are essential to preserve hepatic function and improve recovery.
Footnotes
Acknowledgments
The authors would like to thank the Pediatric Surgery Department of Hospital Nacional Profesor Alejandro Posadas and Hospital de Niños Ricardo Gutiérrez, as well as the intensivists, oncologist and pediatricians, for their valuable collaboration in the comprehensive treatment and clinical follow-up of the patient.
Author Disclosure Statement
The authors declare no conflicts of interest related to this study.
Funding Information
This publication was conducted without specific external funding.
Informed Consent
Patient’s mother and father provided written informed consent, authorizing the publication of this article and the use of their clinical information for scientific purposes, ensuring the protection of their identity and adherence to established ethical principles.