
Abstract
Introduction:
Whether the robotic approach in total mesorectal excision (TME) is associated with increased clear radial and distal margins, compared to the laparoscopic approach, is yet to be determined.
Methods:
We analyzed the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) participant user files for all elective rectal cancer cases performed with minimally invasive surgical techniques (robotic and laparoscopic). Natural orifice, single incisional, and transanal approaches were excluded from the analysis. We calculated relative risks (RR) through Poisson regression models after adjusting for age, body mass index, American Society of Anesthesiologists scores, pathologic T and N status, locations of tumor (low, middle, or high in rectum), neoadjuvant therapy, and surgical specialty.
Outcomes:
Our primary outcome was the result of both radial and distal clear surgical margins upon pathologic analysis. Secondary outcomes included distance of clear distal margins and number of harvested lymph nodes.
Results:
Our cohort consisted of 1321 robotic cases and 2039 laparoscopic cases. There were no significant differences in demographics or tumor staging across groups, except a higher proportion of low rectal cancer in the robotic cohort. The robotic approach was associated with improved radial and distal clear margins in pathological analysis (adjusted RR: 1.06, 95% CI: [1.03–1.10], P < .001). There was a nonsignificant trend toward longer clear distal margin in the robotic cohort. No difference was observed in lymph node harvesting.
Limitations:
As a retrospective and nonrandomized study, residual bias and confounding variables are likely to exist. Relevant information such as mesorectal fascia involvement in clinical preoperative staging could also limit the findings.
Conclusions:
Robotic TME is associated with a higher likelihood of clear surgical margins when compared to laparoscopy.
Introduction
Adoption of robotic surgery continues to grow across specialties at an accelerated pace. As the robotic technology has continued to progress, improvements have been made with significant impact on colorectal procedures. These improvements include 3D high-definition visualization, wristed instrumentation, integrated table motion, increased-angle robotic staplers, 1 enhanced imaging, and multi-quadrant access within the abdomen. These technologic advancements have paralleled an increased adoption of robotic colorectal procedures as well as the adoption of more intracorporeal anastomosis techniques. 2
The current literature has demonstrated the safety and efficacy of robotic colectomy procedures in comparison to laparoscopic.3–6 Many studies have even shown improved perioperative outcomes between robotic and laparoscopic colectomy procedures, 7 including reduced length of stay, reduced opioid use, less blood loss, fewer complications, and reduced conversion rates.8–11 The authors have previously reported on improved oncologic outcome when the robot is adopted in colon cancer surgery. 12
Total mesorectal excision (TME) is the gold-standard surgical treatment for rectal adenocarcinoma. 13 Although the adoption of robotic in TME has been associated with improved surgical outcomes, such as reduced conversion rates, the oncologic safety of robotic TME is yet to be determined. 14 The objective of our study was to provide a real-world comparison of the oncologic outcomes between robotic and laparoscopic TME through the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.
Methods
Study oversight
The data in this study were de-identified and thus were exempt from formal review by our Institutional Review Board.
Cohort abstraction
We abstracted data from the ACS-NSQIP participant user files from 1/2022 to 12/2022. 10 First, we identified all patients who underwent surgery at participating NSQIP hospitals and collected the data for the procedure, targeted rectal cancer surgery. We included only patients treated with minimally invasive (laparoscopic or robotic) approaches. We included all cases in which robotic and laparoscopic surgery were included for the overall analysis, according to the NSQIP built-in classification for surgical approach. NSQIP codes cases as purely robotic as well as robotic with open assist and robotic with unplanned conversion. We included all cases of robotic approach and excluded unplanned conversions. Similarly, the laparoscopic group included case codes as purely laparoscopic without converted cases. All patients with missing data in the pathologic report were excluded from analysis.
Covariates
Trained clinical research abstractors collected the covariates of age, gender, body mass index, presence of diabetes mellitus with and without insulin use, hypertension, smoking history, use of steroids, and history of heart failure. American Society of Anesthesiologists scores were abstracted and included in the adjustment.
We also adjusted ou analysis by cancer characteristics, including T and N status, location of the tumor within the rectum (low, middle, or upper), by neoadjuvant treatment status, and by specialty of the provider.
Primary outcome
Our primary outcome was rate of clear surgical margins upon pathologic analysis, a composite outcome of both radial and distal margins free of adenocarcinoma.
Secondary outcomes
Our secondary outcomes included the number of harvested lymph nodes and the distance of clear distal margins.
Statistical analysis
We aggregated the data to compare robotic versus laparoscopic TME outcomes. We performed univariate analysis incorporating χ2 tests, Fisher’s exact tests, and independent-sample t-tests to compare patient baseline characteristics by time to intervention. Chi-squared risk ratios were used for categorical data. Next, our multivariable analyses used Poisson regression models to estimate relative risks adjusted for potential confounders. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
Results
Cohort
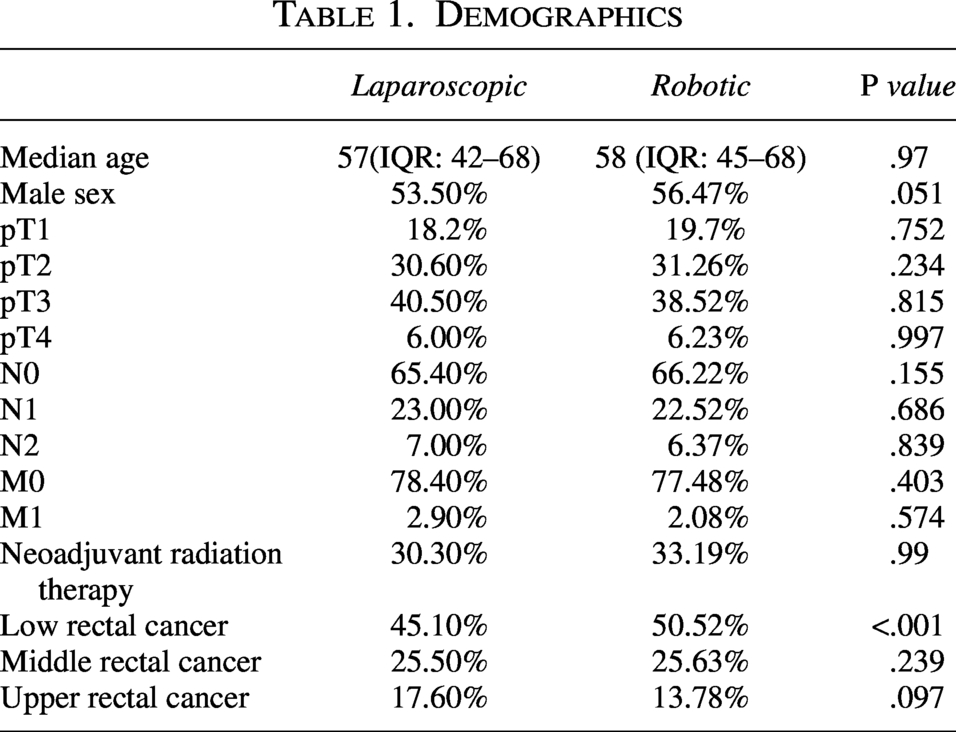
The NSQIP registered 4454 patients with rectal procedures from January 1, 2022, to December 31, 2022. For the purpose of this analysis, we excluded single incision, natural orifice, and transanal procedures. Our final cohort included 1321 robotic cases, and 2039 cases were laparoscopic. Patients had similar demographic characteristics across the cohorts, except for a significant higher proportion of low rectal cancer in the robotic cohort. Demographic results are summarized in Table 1.
Demographics
Primary Outcome—Combined clear surgical margins
The robotic approach was associated with significant increased clear radial and distal surgical margins when compared to laparoscopy. Our primary outcome of combined clear margins was observed in 89.33% of patients in the robotic cohort, compared to 86.44% in the laparoscopic cohort. This result was significant even after multivariate analysis (adjusted RR: 1.06, 95% CI: [1.03 to 1.10], P < .001).
Secondary outcomes
Clear radial margins
Clear radio margins were observed in 90.96% of patients in the robotic cohort, compared to 87.72% in the laparoscopic cohort. This result was significant even after multivariate analysis (adjusted RR: 1.03, 95% CI: [1.01–1.07], P = .041).
Clear distal margins
Clear radio margins were observed in 96.44% of patients in the robotic cohort, compared with 94.59% in the laparoscopic cohort. This result was significant even after multivariate analysis (adjusted RR: 1.03, 95% CI [1.01–1.05], P = .042).
Median distal margin distance
The median distal margin difference was 2.9 cm in the robotic approach (IQR: 1.5–4.5), compared to 2.75 cm in the laparoscopic cohort (IQR: 1.5–4.3). There was no significant difference across groups (P = .219).
Number of harvested lymph nodes
In the robotic cohort, the median number of harvested lymph nodes were 16 (IQR: 13–22). The laparoscopic cohort had a similar result, with 16 median harvested nodes (IQR: 13–22). There was no statistical difference across groups (P = .855)
Results are summarized in Table 2.
Oncologic Outcomes
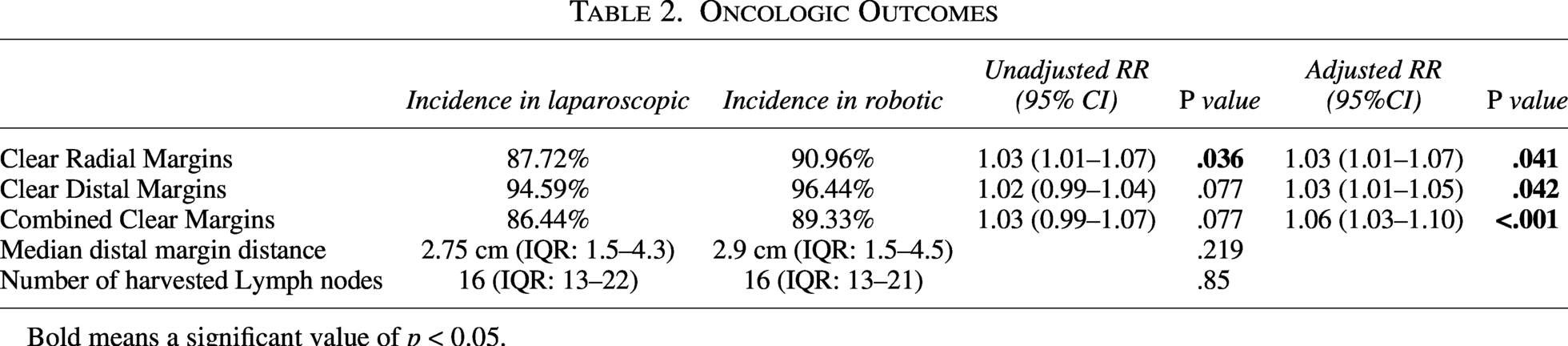
Bold means a significant value of p < 0.05.
Discussion
In this retrospective analysis of a large national database, the robotic approach in TME has been associated with improved clear surgical margins, both radial and distal. Also, our composite outcome of combined clear margins upon pathological analysis saw a significant increase. The results were significant both in the crude and multivariate analysis.
Regarding secondary oncologic outcomes, the robotic approach was associated with a nonsignificant trend towards longer distal margins. As for the number of harvested lymph nodes, there was no observed difference regarding surgical approach. These findings are especially relevant due to the higher proportion of low rectal cancer in the robotic cohort.
To our knowledge, our study is the first to analyze the role of robotics in improving the oncologic quality of mesorectal excision compared to the laparoscopic approach. One recent meta analysis 15 has associated the robotic approach with improved distal margins, as compared to the open approach. No difference was observed for radial margin or complete mesorectal excision.
Recent studies have shown improved lymph node harvesting in robotic colectomy for colon cancer. We observed no difference in the present analysis regarding this particular outcome. A possible reason for this difference is that TME has a similar standardization of technique in both robotic and laparoscopic approaches. This finding adds to the validity of our study, as is shows that in spite of similar oncologic technique across the groups, the quality of the mesorectal excision per se may benefit from the robotic approach.
Our study has several limitations. NSQIP registered a relatively high missing information or unknown rates for tumor staging and pathologic margins status. Also, relevant information regarding the clinical staging, such as mesorectal fascia involvement in the preoperative MRI are not included, which could account for possible unobserved bias. Finally, the observational nature of the study cannot exclude residual bias.
In summary, our study shows that the robotic approach in TME may be associated with improved oncologic quality as it relates to clear radial and distal margins.
Authors’ Contributions
R.M.A.L. has contributed to data collection, statistical analysis and article writing. R.R. has contributed to article writing. S.S. has contributed to article writing. L.E.C.C.A. has contributed to article writing. L.F.B.J. has contributed to article writing. S.E.A.A. has contributed to article writing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was self-funded.