
Abstract
Preserving anal function in ultra-low rectal cancer surgery remains challenging in terms of technique and perioperative management. With advancements in minimally invasive techniques, Da Vinci robot-assisted intersphincteric resection (ISR) has been increasingly utilized, yet its clinical benefits remain unclear. This retrospective cohort study included 142 patients who underwent ISR at the Second Xiangya Hospital of Central South University from January 2019 to December 2024, divided into the robot-assisted ISR (RoISR) group (n = 71) and the laparoscopic ISR (LaISR) group (n = 71). Perioperative outcomes, postoperative complications, pain scores (numerical rating scale [NRS]), Wexner scores, quality of life (Functional Assessment of Cancer Therapy-Colorectal [FACT-C] scale), and long-term survival outcomes were compared. Results showed that RoISR had a longer operative time (220.27 ± 32.21 versus 179.63 ± 23.88 minutes, P < .001) but earlier time to first flatus (1.77 ± 1.50 versus 2.32 ± 1.67 days, P = .041) and shorter hospital stay (8.25 ± 3.38 versus 9.77 ± 4.63 days, P = .027), with comparable blood loss and costs. The 30-day complication rate was lower in the RoISR group (7.04% versus 19.72%, P = .027), including reduced anastomotic complications (1.41% versus 5.63%) and bleeding (0% versus 4.23%). NRS pain scores were lower in the RoISR group at 12 hours (3.56 ± 0.84 versus 4.79 ± 1.11, P < .001), 24 hours (1.90 ± 0.85 versus 2.35 ± 1.02, P = .05), and 48 hours (1.07 ± 0.87 versus 1.61 ± 0.80, P < .001). Wexner scores showed greater improvement in the RoISR group at 3 months (9.49 ± 2.26 versus 10.45 ± 2.10, P = .01) and 6 months (7.18 ± 1.88 versus 7.94 ± 1.96, P = .02). Emotional functioning on the FACT-C scale was significantly better in the RoISR group (P = .028). Kaplan–Meier analysis indicated no significant differences in overall survival or recurrence-free survival (RFS) between groups. In conclusion, RoISR offers advantages in perioperative recovery, reduced complications, and improved aspects of quality of life, with long-term survival outcomes comparable to LaISR.
Keywords
Background
Rectal cancer ranks among the most prevalent gastrointestinal malignancies globally. Ultra-low rectal cancer, defined as tumors with a distal margin ≤3 cm from the dentate line, presents a clinical challenge due to the need to balance oncologic radicality with anal sphincter preservation. 1 Intersphincteric resection (ISR), which involves dissection of the intersphincteric plane between the internal and external anal sphincters, has become a standard approach for anal-preserving surgery in ultra-low rectal cancer. 2
Laparoscopic ISR (LaISR) offers minimally invasive advantages but is constrained by two-dimensional imaging and rigid instruments, leading to technical difficulties in the narrow pelvis, increased conversion to open surgery, and suboptimal total mesorectal excision (TME) quality. 3 The Da Vinci robotic surgical system, with its high-definition three-dimensional imaging, 7-degree-of-freedom instruments, and tremor filtration, significantly enhances precision and safety in deep pelvic procedures. 4 Recent studies suggest that robot-assisted ISR (RoISR) reduces conversion rates, improves TME completeness, and facilitates postoperative recovery.5,6 However, existing research primarily focuses on short-term perioperative outcomes (e.g., operative time, intraoperative blood loss, hospital stay, and complication rates) and oncologic results, with limited exploration of functional recovery and quality of life.2–4 A 2013 retrospective study compared short-term outcomes such as blood loss and hospital stay but was limited by a small sample size and short follow-up (<12 months). 6 Flynn et al.’s multicenter study evaluated short-term outcomes of robot-assisted surgery for mid- and low rectal cancer but omitted anal function assessment. 7 Gao et al. investigated learning curves and perioperative complications but excluded long-term prognosis and quality of life metrics. 8 These studies are often constrained by small sample sizes, retrospective designs, or high heterogeneity in multicenter data, lacking comprehensive evaluation of long-term oncologic outcomes, anal function recovery, and quality of life, thus limiting the broader adoption of RoISR.
In contrast, this single-center retrospective cohort study (n = 142) systematically compares the clinical efficacy of RoISR versus LaISR in ultra-low rectal cancer with anal preservation, emphasizing perioperative outcomes (operative time, blood loss, and hospital stay), postoperative complications, pain scores (numerical rating scale [NRS]), anal function, quality of life, and oncologic outcomes (overall survival [OS] and recurrence-free survival [RFS]). By incorporating functional recovery and quality of life metrics, this study provides robust long-term evidence to guide optimized surgical decision-making.
Materials and Methods
Study population
This single-center retrospective cohort study enrolled 142 patients with ultra-low rectal cancer who underwent anal-preserving surgery at the Second Xiangya Hospital of Central South University between January 2018 and December 2022. Patients were divided into the RoISR group (RoISR, n = 71) and the LaISR group (LaISR, n = 71) based on surgical approach (nonrandomized). Baseline characteristics showed no significant differences between groups (P > .05; see subsection Baseline Characteristics Comparison under Results section). This study was approved by the hospital ethics committee (2019NZKY-034-01), and informed consent was obtained from patients or their families.
Inclusion criteria
(1) Histologically confirmed ultra-low rectal adenocarcinoma via colonoscopy and biopsy, with the distal tumor margin ≤3 cm from the dentate line; (2) clinical stage cT1-3N0-2M0 (based on MRI/CT); (3) age 18–75 years; (4) American Society of Anesthesiologists (ASA) grade I–III; (5) Signed informed consent for surgery; and (6) complete follow-up data for ≥12 months.
Exclusion criteria
(1) Tumor invasion of the sphincter requiring abdominoperineal resection; (2) intraoperative conversion to open surgery; (3) history of pelvic surgery or other malignancies; (4) severe liver, kidney, lung, or coagulation dysfunction; (5) pregnant women; (6) noncompliant or lost-to-follow-up patients; and (7) locally advanced or multifocal tumors.
Methods
All procedures were performed by a single surgical team with experience in >50 ISR cases, using the Da Vinci Xi system (Intuitive Surgical, USA) for RoISR or standard laparoscopic equipment for LaISR. Surgeries adhered to TME principles and neoadjuvant therapy (chemotherapy/radiotherapy, per National Comprehensive Cancer Network guidelines).
RoISR group
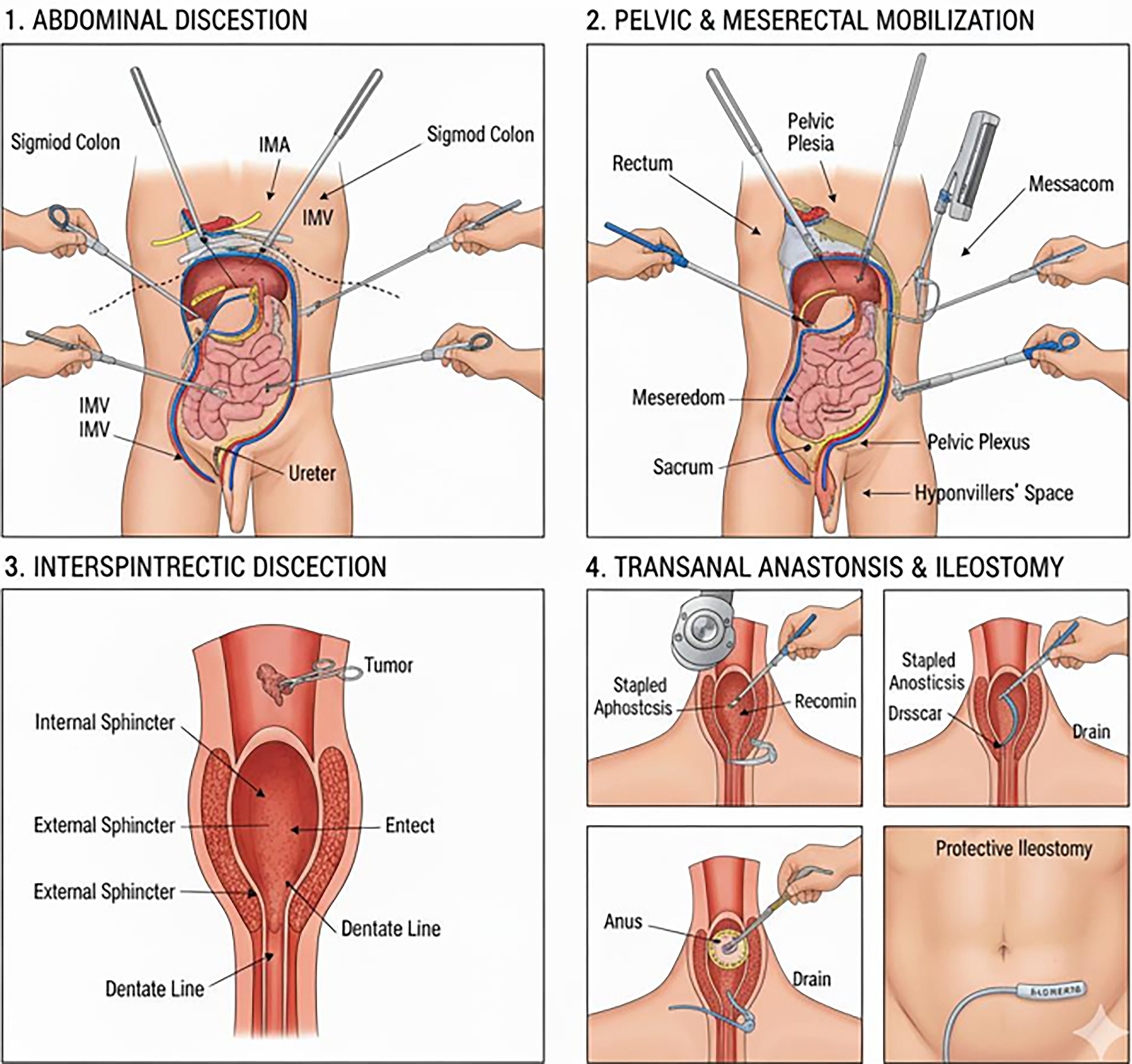
RoISR was performed under general anesthesia in the modified lithotomy position with routine sterilization and draping. Pneumoperitoneum (12–15 mmHg) was established, and 45 trocars (including robotic arms and assistant ports) were placed. The patient was positioned in a head-down, feet-up tilt. The Da Vinci robotic arms were docked, and the abdominal cavity was explored. The sigmoid mesocolon was elevated, and the peritoneum was incised from the midline at the sacral promontory, entering the retro-sigmoid mesocolic space to expose the left gonadal vessels and ureter, reaching the left Toldt’s line. Cranial dissection in the retro-sigmoid mesocolic space exposed the inferior mesenteric artery (IMA) root and superior hypogastric plexus. The left colonic mesocolic space was entered cranially, clearing No. 253 lymph nodes, ligating the IMA at its root, and transecting the inferior mesenteric vein at the same level. The sigmoid mesocolon was elevated, the left Toldt’s line was incised, and the mesocolon was trimmed. Dissection proceeded along the retro-sigmoid mesocolic space into the pelvic cavity, entering the retrorectal space, preserving bilateral hypogastric nerves, and transecting the rectosacral ligament to access the presacral space. The peritoneal reflection was incised anteriorly, entering Denonvilliers’ space, with partial transection of the lateral rectal ligaments bilaterally while preserving the pelvic nerve plexuses. The mesorectum was mobilized, and the posterior hiatal ligament was incised to the levator ani hiatus, entering the intersphincteric plane, which was connected to the bilaterally dissected intersphincteric spaces, reaching the dentate line (visible varicose veins). The robotic arms were detached, the rectal stump was irrigated, and anal retractors were used for exposure. Under direct anoscopic visualization, the rectal mucosa, submucosa, and internal anal sphincter were circumferentially incised 1–1.5 cm distal to the tumor, dissecting upward along the intersphincteric plane, partially resecting the internal sphincter if necessary, and joining the abdominal dissection. The proximal bowel was exteriorized transanally, transected 12 cm proximal to the tumor, and fitted with an anvil for sigmoid-rectal/anal canal anastomosis. Anastomotic integrity was tested with no abnormalities observed. A presacral drain was placed, and a protective ileostomy was performed (Fig. 1).

Robot-Assisted Intersphincteric Resection (RoISR).
LaISR group
LaISR was performed under general anesthesia in the modified lithotomy position with routine sterilization and draping. Pneumoperitoneum (12–15 mmHg) was established, and 5 trocars were placed. The abdominal cavity was explored, and the peritoneum was incised near the midline to expose and dissect the inferior mesenteric vessels, clearing No. 253 lymph nodes. The inferior mesenteric vessels were clipped and transected near their origin. The sigmoid mesocolon was elevated, and dissection proceeded along Toldt’s plane to the left Toldt’s white line, mobilizing the rectum and mesorectum per TME principles. The peritoneal reflection was incised, and Denonvilliers’ fascia was opened along the seminal vesicle/vaginal posterior plane. The lateral rectal ligaments were transected, and the pelvic floor was mobilized to the levator ani hiatus. The mesorectum was dissected, and the sigmoid colon was transected using a linear cutting stapler. The rectal stump was irrigated, and under direct anoscopic visualization, the rectal mucosa, submucosa, and internal anal sphincter were circumferentially incised 1–1.5 cm distal to the tumor, dissecting upward along the intersphincteric plane to join the abdominal dissection. The proximal bowel was exteriorized transanally, transected 12 cm proximal to the tumor, and a sigmoid-rectal/anal canal anastomosis was performed. Anastomotic integrity was tested with no abnormalities observed. A presacral drain was placed, and a protective ileostomy was performed (Fig. 2).
Laparoscopic Intersphincteric Resection (LaISR).
Postoperative care was standardized, including early mobilization, pain management, and nutritional support. Data were extracted from the electronic medical record system, with double-blind review to minimize bias and the last-observation-carried-forward method for handling missing data.
Outcome measures
Perioperative outcomes: Operative time (min, from skin incision to closure), intraoperative blood loss (mL, measured via suction), time to first flatus/stoma output (h), postoperative hospital stay (d), time to urinary catheter removal (d), and number of lymph nodes harvested. Complications: Assessed using the Clavien–Dindo classification (≥Grade II considered major complications, including anastomotic leakage, wound infection, intra-abdominal bleeding, bowel obstruction, stoma complications, postoperative urinary retention, and pulmonary infection). Pain scores: Evaluated using the numerical rating scale (NRS: 0–10) at 1, 3, and 7 days postoperatively. Anal function: Assessed using the Wexner score (0–20, higher scores indicating worse incontinence/constipation) at 0, 3, 6, and 12 months postoperatively. Quality of life: Evaluated using the Functional Assessment of Cancer Therapy-Colorectal (FACT-C) scale (each domain scored up to 100, higher scores indicating better quality of life) at 6, 12, and 24 months postoperatively. Oncologic outcomes: R0 resection rate (pathologically confirmed), local recurrence rate (imaging follow-up), OS, and RFS, with a median follow-up of 36 months (range: 12–60 months, via telephone/clinic visits, loss to follow-up <5%).
Statistical analysis
Data were analyzed using SPSS 20.0. Continuous variables were expressed as mean ± standard deviation and compared using independent t-tests (normal distribution) or Mann–Whitney U tests (nonnormal distribution). Categorical variables were expressed as percentages and compared using χ2 tests or Fisher’s exact test. Survival analysis was performed using the Kaplan–Meier method to generate OS and RFS curves, with differences compared using the log-rank test. Normality was assessed using the Shapiro-Wilk test, with multiple comparison corrections applied when necessary. A P value <.05 was considered statistically significant.
Results
Baseline characteristics comparison
This study included 142 patients, with 71 (50.00%) in the LaISR group and 71 (50.00%) in the RoISR group. No statistically significant differences were observed between the two groups in terms of age, BMI (kg/m2), tumor diameter, sex, past surgical history, CEA levels, CA19-9 levels, hypertension, anemia, diabetes, coronary heart disease, cerebral infarction, other comorbidities, smoking status, alcohol use, tumor stage, T stage, N stage, or ASA grade (P > .05), indicating comparable baseline characteristics (Table 1).
Comparison of Baseline Characteristics Between the Two Groups
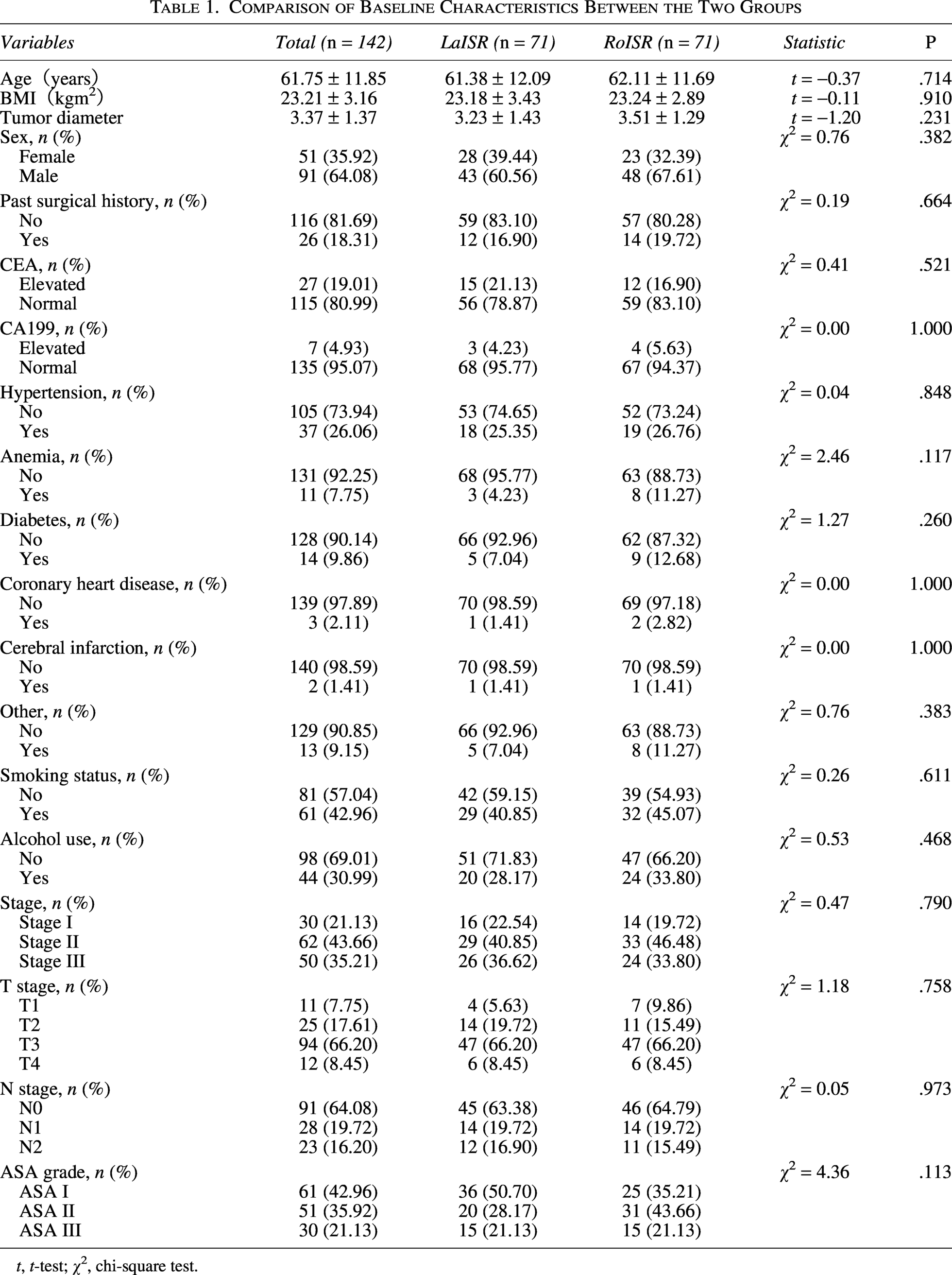
t, t-test; χ², chi-square test.
Comparison of perioperative outcomes
Perioperative outcomes are presented in Table 2. The RoISR group had a significantly longer operative time compared to the LaISR group (220.27 ± 32.21 versus 179.63 ± 23.88 minutes, P < .001). However, the time to first flatus (1.77 ± 1.50 versus 2.32 ± 1.67 days, P = .041) and hospital stay (8.25 ± 3.38 versus 9.77 ± 4.63 days, P = .027) were significantly shorter in the RoISR group, suggesting enhanced postoperative recovery. No significant differences were observed in intraoperative blood loss (71.41 ± 42.37 versus 67.83 ± 53.87 mL, P = .661), hospital costs (97066.34 ± 27651.18 versus 92501.63 ± 24177.10 CNY, P = .297), or time to early ambulation (1.64 ± 0.08 versus 1.64 ± 0.11 days, P = .742).
Comparison of Perioperative Outcomes

Comparison of postoperative complications
Postoperative complications are shown in Table 3. The overall complication rate was significantly lower in the RoISR group (7.04%, 5/71) compared to the LaISR group (19.72%, 14/71) (χ2 = 4.922, P = .027). No significant differences were observed for specific complications, including anastomotic complications (P = .363), abdominal bleeding (P = .243), pulmonary infection (P = .612), incision infection (P = 1.000), intestinal obstruction (P = 1.000), stoma complications (P = 1.000), or postoperative urinary retention (P = 1.000). Overall, the RoISR group demonstrated a significantly lower complication rate, indicating improved safety.
Comparison of Postoperative Complications

Comparison of NRS pain scores
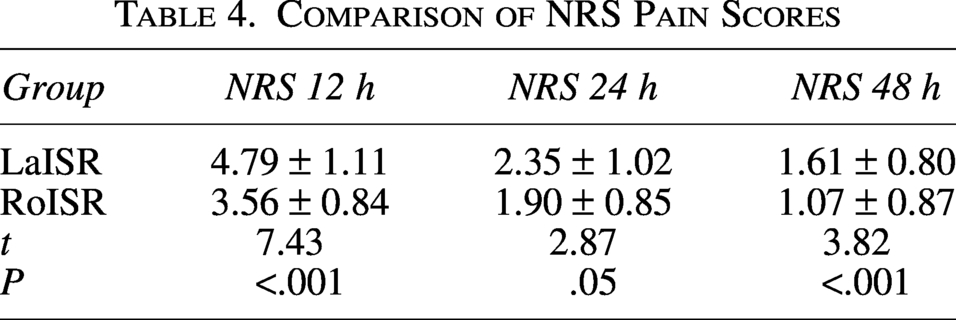
NRS pain scores are presented in Table 4. The RoISR group had significantly lower pain scores at 12 hours (3.56 ± 0.84 versus 4.79 ± 1.11, P < .001) and 48 hours (1.07 ± 0.87 versus 1.61 ± 0.80, P < .001) postoperatively compared to the LaISR group. The difference at 24 hours approached significance (1.90 ± 0.85 versus 2.35 ± 1.02, P = .05). These results suggest that robot-assisted surgery may reduce early postoperative pain.
Comparison of NRS Pain Scores
Comparison of Wexner scores
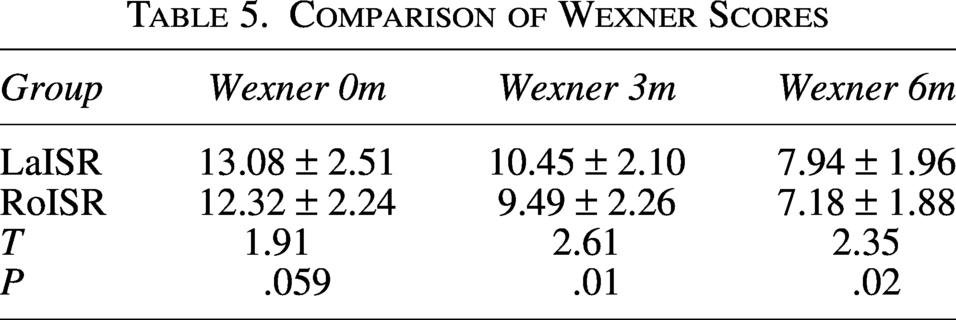
Wexner scores are shown in Table 5. At discharge (0 months), no significant difference was observed between groups (13.08 ± 2.51 versus 12.32 ± 2.24, P = .059). At 3 months (10.45 ± 2.10 versus 9.49 ± 2.26, P = .01) and 6 months (7.94 ± 1.96 versus 7.18 ± 1.88, P = .02) postoperatively, the RoISR group had significantly lower scores, indicating better anal function recovery compared to the LaISR group.
Comparison of Wexner Scores
Comparison of FACT-C scores
FACT-C scores are presented in Table 6. Preoperatively, no significant differences were observed between groups across all domains (P > .05). Postoperatively, the RoISR group showed significantly greater improvement in emotional well-being (EWB) (21.63 ± 2.87 versus 20.31 ± 4.11, P = .028). No significant differences were observed in other domains (physical well-being, social/family well-being, functional well-being, colorectal cancer subscale) or total FACT-C scores (P > .05), suggesting similar overall quality of life improvements, with a slight advantage in EWB for the RoISR group.
Comparison of FACT-C Scores

PWB, physical well-being; SWB, social/family well-being; EWB, emotional well-being; FWB, functional well-being; CCS, colorectal cancer subscale; FACTC, Functional Assessment of Cancer Therapy—Colorectal (Total Score).
Overall survival and recurrence-free survival analysis
Kaplan–Meier survival curves showed no significant difference in OS between the two groups (Fig. 3A, Log-rank P = .24; adjusted Cox model HR = 2.09, 95% CI: 0.60 to 7.23). Similarly, no significant difference was observed in RFS (Fig. 3B, log-rank P = .32; HR = 1.48, 95% CI: 0.68 to 3.22). These results indicate comparable oncologic outcomes between the two groups.
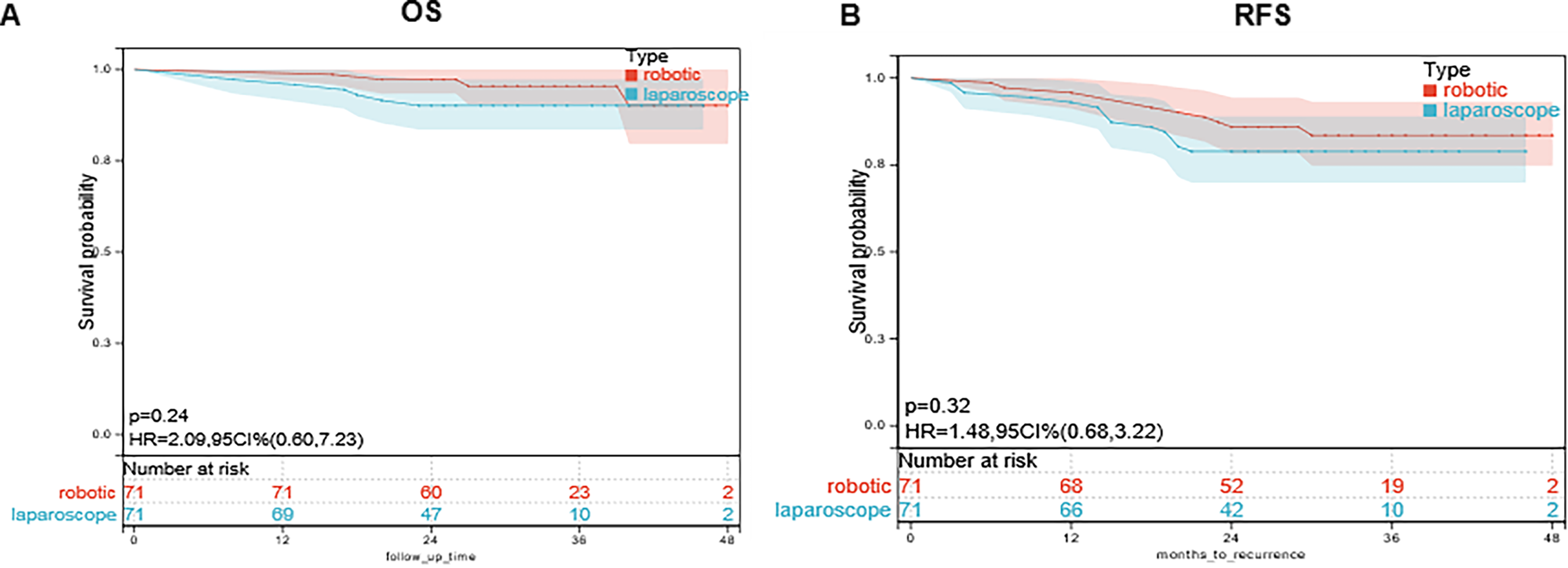
Comparison of Survival Curves Between Da Vinci Robot-Assisted and Laparoscopic ISR.
Discussion
Rectal cancer is a major global malignancy, with over 700,000 new cases reported worldwide in 2020. Low and ultra-low rectal tumors, accounting for approximately 30%–40% of cases, often require anal-preserving surgery to maintain quality of life. 9 ISR is a standard anal-preserving strategy for low rectal cancer, but conventional LaISR is limited by the narrow pelvis and complex anatomy, resulting in higher complication rates and suboptimal functional recovery.10,11 Ro-ISR, leveraging three-dimensional high-definition imaging and high-degree-of-freedom instruments, offers potential advantages in precise dissection and stable manipulation. 12
In the early 1990s, Braun et al. and Schiessel et al. first reported the use of ISR for low rectal cancer as an extreme anal-preserving technique, avoiding permanent stoma while achieving satisfactory oncologic outcomes.13,14 Subsequent studies by Berger et al., Saito et al., and Portier et al. confirmed the oncologic safety of ISR, with a 5-year local recurrence rate of approximately 5%–10%, a perioperative mortality rate of about 0.8%, and an overall complication rate of approximately 25.8%, alongside significant quality-of-life improvements through sphincter preservation.15–17 Currently, ISR can be performed via open (O-ISR), laparoscopic (L-ISR), or robot-assisted (R-ISR) approaches. Multiple studies comparing Ro-ISR and L-ISR, such as Pai et al., demonstrated that L-ISR for low rectal cancer results in less intraoperative blood loss, clearer operative fields, and lower postoperative complication rates, with noninferior oncologic outcomes. 18 Baek et al. and Kwak et al. also supported the short-term recovery advantages of L-ISR.19,20 However, direct comparisons between L-ISR and R-ISR remain limited, often focusing on short-term outcomes without systematic exploration of long-term functional results or underlying biological mechanisms.
Existing evidence suggests that R-ISR has potential advantages in technical quality and short-term safety. A systematic review by Piozzi et al. reported higher TME completeness rates (85% versus 65%) and lower complication rates (18% versus 35%) for R-ISR, with superior 7-year functional and oncologic outcomes, indicating that high-magnification imaging and articulated instruments reduce surgical trauma and enhance TME quality. 21 A meta-analysis by Tang et al. showed shorter hospital stays and lower complication rates with R-ISR, though neural protection mechanisms were not thoroughly explored. 22 Colombari et al. observed higher sphincter preservation rates (93% versus 82%) and better functional scores in R-ISR patients following neoadjuvant therapy, potentially due to reduced neuroinflammation from precise dissection. 23 An updated meta-analysis by Zou et al. indicated slightly lower local recurrence rates (6.5% versus 7.0%) and shorter hospital stays with R-ISR, though significant heterogeneity persisted across centers. 24 While the short-term benefits of R-ISR are increasingly evident, retrospective biases, sample heterogeneity, and limited follow-up restrict the generalizability of these findings, particularly regarding neural protection and EWB mechanisms.
This study, based on a single-center retrospective cohort (n = 142, median follow-up 36 months), conducted by a highly experienced team with baseline matching and standardized perioperative management, systematically compared the efficacy of R-ISR versus L-ISR in ultra-low rectal cancer, covering perioperative outcomes, complications, anal function, quality of life, and oncologic outcomes, aiming to provide consistent clinical evidence while controlling for biases.
Tang et al. found that R-ISR had longer operative times but less blood loss (mean difference = −50 mL) and shorter hospital stays, attributed to precise vascular dissection and trauma control enabled by three-dimensional imaging and high-degree-of-freedom instruments, reducing inflammatory responses (e.g., IL-6, CRP). In this study, R-ISR had significantly longer operative times (P < .05), but earlier time to first oral intake, bowel recovery (flatus/defecation), and shorter hospital stays (P < .05), consistent with prior literature. 22 The Da Vinci system’s high-magnification imaging and wrist-like instruments enable precise dissection in the intersphincteric plane, minimizing vascular and soft tissue damage, suppressing postoperative inflammatory cascades, and promoting bowel motility recovery, aligning with enhanced recovery after surgery principles. Unlike earlier studies, our team’s experience (>50 ISR cases) suggests that the operative time difference primarily stems from equipment setup and calibration rather than dissection challenges.21–23 Reduced tissue edema and bleeding facilitated earlier implementation of nutritional and rehabilitation measures. Hospital costs showed no significant difference, consistent with Tang et al.’s economic analysis, suggesting that shorter hospital stays may partially offset equipment costs. 21 Notably, Lee et al.’s meta-analysis reported less blood loss and longer operative times with R-ISR, whereas this study found no difference in blood loss, likely due to surgeon experience and standardized protocols reducing variability. 23
Postoperative complications directly impact safety and prognosis. Ge et al. suggested that R-ISR has lower overall complication rates and reduced conversion-to-open surgery risk, reflecting the robotic platform’s stability and control. 24 Piozzi et al. 1 reported lower complication rates and higher TME completeness with R-ISR, indicating advantages in preserving rectal blood supply and reducing anastomotic stress. 1 Liu et al. noted lower local recurrence rates with R-ISR, potentially linked to higher-quality TME. In this study, the R-ISR group had a significantly lower 30-day complication rate (P < .05), with fewer anastomotic complications and bleeding events. 25 Potential mechanisms include enhanced identification and preservation of the intersphincteric plane and pelvic neurovascular structures due to high-magnification imaging and tremor filtration; reduced ischemic and micro-injuries from articulated instruments; and greater accessibility and stability in ultra-low and narrow pelvises, resembling open surgery, ensuring TME completeness and anastomotic blood supply. Compared to multicenter heterogeneous studies, this study’s baseline matching and uniform care protocols reduced bias. No differences were observed in urinary retention or stoma complications, possibly due to limited sample size; overall trends support R-ISR’s safety advantages in complex cases.
Anal function is a core dimension of quality of life post-ISR. This study used the Wexner incontinence score to assess postoperative anal function, showing superior outcomes in the R-ISR group (P < .05). This difference may stem from the robotic platform’s high-magnification imaging and articulated instruments, enabling clearer identification of the internal and external anal sphincters, levator ani, and pelvic autonomic nerves, reducing mechanical traction and thermal injury, and minimizing secondary neuroinflammation and fibrosis. This leads to improved continence, reduced defecation frequency, and alleviation of low anterior resection syndrome (LARS). 26 Prior studies also suggest that robot-assisted mesorectal excision offers potential advantages in neural protection and functional outcomes, evidenced by lower incontinence scores and better bowel function recovery. Notably, neoadjuvant chemoradiotherapy may exacerbate postoperative bowel dysfunction and increase LARS risk, but the limited number of such cases in this study precludes definitive subgroup conclusions. 27
Regarding quality of life, long-term follow-up evidence indicates that improvements in complication and pain control with robotic surgery may translate to better functional and psychological outcomes (e.g., EORTC QLQ-C30/CR29 or FACT-C). 28 In this study, the R-ISR group showed significantly greater improvement in EWB (P < .05), potentially due to reduced postoperative pain and complications lowering stress burden, alongside neural protection and inflammation suppression promoting overall recovery. Compared to single-domain metrics, multidimensional scales better reflect patient-reported benefits, and future studies should incorporate standardized, longitudinal quality-of-life assessments.
Oncologic outcomes remain the cornerstone of surgical evaluation. Long-term follow-up from systematic reviews and large-scale real-world studies indicates that robotic and laparoscopic approaches yield comparable OS and RFS, with robotics potentially offering slight or context-dependent advantages in TME quality (e.g., circumferential resection margin positivity, mesorectal integrity) and local recurrence. In this study, R-ISR and L-ISR showed no significant differences in OS or RFS, with R-ISR achieving reliable R0 resection margins, consistent with prior literature.15–17 Previous studies also reported comparable or nonsignificant differences in lymph node harvest between robotic and laparoscopic approaches, and this study similarly observed no statistical difference, suggesting that under standardized protocols and experienced teams, R-ISR is non-inferior to L-ISR in oncologic safety.15–18
The robotic platform’s primary limitations include high equipment costs, lack of haptic feedback, and longer operative times. However, learning curve studies and meta-analyses show that with increased surgical volume and team experience, operative time differences diminish or disappear, alongside improvements in complications and conversion rates. 8 This study’s strengths include its single-center design, consistent surgical team, standardized perioperative protocols, comprehensive functional and quality-of-life assessments, and a median 36-month follow-up, offering greater consistency than small-sample or heterogeneous multicenter studies. Limitations include retrospective design-related selection and information biases, limited sample size, and lack of systematic sexual function assessment. Future high-quality, adequately powered prospective randomized controlled trials are needed, incorporating preregistered outcomes (OS/RFS, TME quality, complications, bowel and urogenital function, LARS, and multidimensional quality of life) and stratified analyses (e.g., neoadjuvant therapy, tumor height, sex, and pelvic anatomy differences), alongside cost-effectiveness evaluations to clarify R-ISR’s long-term net benefits and optimal patient populations.
Conclusion
R-ISR is safe and feasible for low and ultra-low rectal cancer. Despite longer operative times, it offers advantages over L-ISR in bowel function recovery, complication control, and anal function, with comparable oncologic outcomes, particularly in anatomically complex or ultra-low cases. Its long-term efficacy and cost-effectiveness require validation through prospective randomized studies to optimize clinical decision-making and individualized treatment strategies.
Footnotes
Authors’ Contributions
C.F. and S.L. had access to all patient information in the study and also had access to all data in the study and took responsibility for the integrity of the data and accuracy of data analysis. Conceptualization and data curation were carried out by N.Y. Formal analysis was done by J.L. Writing—original draft was done by C.F. and S.L. Writing—review and editing was done by J.L.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (the Second Xiangya Hospital of Central South University) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.