
Abstract
Background:
Thoracic esophageal perforation (EP) is a life-threatening emergency. While minimally invasive techniques have been successfully utilized, the heterogeneity of clinical presentations (perforation location, delays in treatment, tissue quality, etc.) has prevented the establishment of a standardized management approach. We present our experience with a minimally invasive management protocol combining thoracoscopy and endoscopy.
Methods:
Between December 2023 and January 2025, 5 patients with thoracic EP underwent a thoracoscopic approach. Primary closure via direct suturing, lavage, and drainage was performed when feasible. Persistent leaks were addressed with endoscopic interventions, including vacuum-assisted therapy and stent placement. A retrospective review of patient medical records was conducted.
Results:
Of the five perforations, four were right-sided, and one was left-sided. Three cases were spontaneous, while two were iatrogenic (one following bariatric surgery and the other after endoscopic dilation). One patient had a perforation associated with malignancy, and another was on long-term high-dose steroid therapy. Management was initiated within 24 hours after the onset of symptoms in 3 patients and after 48 hours in 2 patients. Persistent leaks occurred in 3 patients (two late presentations and one corticosteroid impregnation). There were no fatalities. Esophageal preservation was achieved in all cases, and all patients resumed oral intake by the end of follow-up.
Conclusions:
Thoracic EP can be effectively managed using minimally invasive techniques. Avoiding thoracotomy and complex surgical procedures may offer significant benefits for critically ill patients.
Keywords
Introduction
Esophageal perforation (EP) is a rare yet severe medical condition.1–3 The majority of cases are iatrogenic, 4 arising from medical procedures such as endoscopy and surgery. The recent increase in EP incidence is closely associated with the rise of interventional endoscopic procedures. Spontaneous EP is less common but can occur following significant retching, which results in a rapid elevation of intraluminal pressure, leading to esophageal wall rupture. 5
EP can occur at various anatomical levels, including the cervical, thoracic, and, less frequently, abdominal regions. However, perforations in the thoracic region present the greatest diagnostic and therapeutic challenges. Thoracic EP can lead to extensive contamination of the mediastinum and pleura, resulting in septic shock and death without prompt and effective treatment. 6 Despite substantial advancements in resuscitation and surgical techniques over recent decades, mortality rates for EP remain high. 7 Contributing factors to the lack of improvement in survival rates include delays in diagnosis, underlying patient comorbidities 8 (e.g., advanced age and coexisting diseases), as well as trauma, stress, and postoperative pain associated with surgical intervention.
Thoracotomy and laparotomy were considered the standard treatment for EP in the past but are associated with significant pain, surgical trauma, and operative stress. In contrast, minimally invasive surgery has been shown to reduced trauma, 9 postoperative pain, decreased systemic inflammatory response, postoperative endotoxemia, and preserved immune function. 10 In the context of elective esophageal cancer surgery, minimally invasive approaches have been associated with decreased overall morbidity and pulmonary complications compared with open surgery. 11
Relying on our expertise in minimally invasive surgery for esophageal cancer, we began offering minimally invasive surgery to patients with EP in December 2023. The objective of this study is to report patient outcomes and the lessons learned during the implementation of minimally invasive management for EP.
Methods
Patients and methods
We included all adult patients who required emergency surgery for thoracic EP between December 1, 2023, and January 1, 2025. The management of EP at our institution followed the guidelines recently endorsed by the World Society of Emergency Surgery. 12 Emergency surgery was offered to patients with thoracic EP if at least one of the following criteria was met: Signs and symptoms of sepsis are defined as suspected or confirmed infection associated with acute organ dysfunction (SOFA (Sequential Organ Failure Assessment) score increase ≥2), including hemodynamic instability, altered mental status, or laboratory evidence of organ failure; noncontained perforation with leakage of contrast product on the CT scan with significant pleural contamination; or preexisting esophageal disease, including malignancy, severe stricture, or radiation-induced injury.
During the study period, we transitioned from an open approach via posterolateral thoracotomy to a minimally invasive thoracoscopic approach. Initially, patients were positioned in a semiprone position to allow for conversion to thoracotomy if necessary. However, the last 2 patients were positioned in the prone position. Selective intubation was performed in all cases to enable pulmonary exclusion in the event of conversion to thoracotomy. The side of the incision was determined based on the location of the largest pleural effusion or the extravasation of contrast material, if present.
Three or four 10 mm ports were inserted in a triangular configuration, with the first port placed below the scapular tip. After lavage of the thoracic cavity, the inferior pulmonary ligament was dissected, and the mediastinal and parietal pleura were opened. The esophageal defect was then identified. On the right side, the azygos vein arch was usually transected using a stapler to improve exposure. The muscular layer at both the upper and lower extremities of the perforation was incised to expose the mucosa, which was then sutured using barbed suture. If feasible, the muscular layer was partially or completely closed with interrupted sutures. A nasogastric tube was systematically placed under direct visual control before closing the esophageal parietal defect. The thoracic cavity was drained by placing a posterior drain adjacent to the esophageal suture and an additional drain in the anterior mediastinum.
If the postoperative course was uneventful, the anterior drain was removed on postoperative day (POD) 2. An oral and vascular contrast-enhanced Computed Tomography (CT) scan was routinely performed on POD 5, or sooner if there were any signs or symptoms suggestive of an esophageal leak. In the absence of leakage, oral nutrition was resumed, and chest drains were gradually removed.
In the case of a manifest leak, improvement in thoracic drainage was achieved, with radiological guidance if necessary. Subsequently, endoscopic treatment using the endoscopic vacuum therapy (EVT) device was initiated. The EVT sponge was introduced into the pleural cavity through the fistulous opening, or if the fistula was too small to allow the passage of the foam, it was positioned in the esophageal lumen opposite the perforation. The sponge was replaced every 3–4 days until reduction in the pleural cavity, drainage, and drying of the fistula were achieved. Mobilization and gradual removal of thoracic drains were initiated when the drainage output was less than 50 cc/day.
Results
Patient cohort
Five consecutive adults with thoracic EP underwent a minimally invasive surgical approach between December 2023 and January 2025. These patients accounted for one-third of the total EP cases managed during this period (5 out of 15). Etiology was spontaneous rupture (Boerhaave syndrome) in 3 patients and iatrogenic injury in 2 patients (one after laparoscopic sleeve gastrectomy and the other after endoscopic dilation of a radiation-induced stricture). Three patients were managed within 24 hours of symptom onset, whereas 2 patients presented after a delay of ≥72 hours. A thoracoscopic primary repair was attempted in 4 patients and was feasible in all 4 patients; in one delayed malignant perforation, the defect edges were rigid and primary closure was not feasible, and wide drainage with early endoscopic therapy was performed. Postoperative persistent leak occurred in 3 patients and was treated with EVT with a covered stent added in one oncologic case. There were no in-hospital deaths, no conversions to thoracotomy, and esophageal continuity was preserved in all patients. Two operative cases were recorded and are provided as Supplementary Videos (Video 1 and Video 2).
Illustrative cases
Case 1 (Video 1)—acute perforation in a high-risk patient (chronic corticosteroids)
A 69-year-old woman with long-standing rheumatoid arthritis treated with high-dose corticosteroids presented 3 hours after sudden severe right basal thoracic pain. Contrast-enhanced CT demonstrated a large right pleural contrast leak consistent with distal thoracic EP; a large left pleural serous effusion was drained percutaneously preoperatively. She underwent right thoracoscopy in a semiprone position with extensive pleural lavage. A 5-cm longitudinal perforation was identified approximately 3 cm above the diaphragmatic hiatus. The mucosal defect was closed with a running barbed suture, and the thoracic cavity was drained with anterior and posterior chest tubes. On POD 5, enteric content appeared in the posterior drain. CT confirmed a persistent esophageal defect with ongoing right pleural extravasation. Because the left pleural collection persisted despite the left drain, a left thoracoscopy washout/debridement and drainage were performed, followed by laparoscopic feeding jejunostomy. Upper endoscopy confirmed an approximately 3-cm residual leak, and EVT was initiated. Six EVT sponge exchanges were required over 45 days to achieve closure. She was discharged to rehabilitation on POD 59 on combined oral and enteral nutrition; the jejunostomy was removed 5 months later, and she resumed a normal diet without symptoms at 1 year.
Case 2 (Video 2)—delayed Boerhaave syndrome managed thoracoscopically with EVT rescue
A 66-year-old man with active smoking and alcohol use disorder presented with sepsis and left thoracic pain evolving over 3 days after vomiting. CT showed pneumomediastinum, bilateral pleural effusions, and a left-sided contrast leak. Surgery was initiated in the prone position to allow bilateral access. A left thoracoscopic approach was attempted first; however, effective left lung exclusion could not be achieved. A right thoracoscopy identified an intubation issue (accidental selective left intubation), and a contralateral approach was aborted due to severe inflammation and adhesions with concern for esophageal devascularization. After repositioning the endotracheal tube above the carina, the left thoracoscopic approach was resumed. A 3-cm perforation was identified approximately 4 cm below the aortic arch and was repaired with direct suturing despite the 72-hour delay; two additional trocars were required for exposure. Drainage was performed with anterior and posterior chest tubes. POD-5 CT showed no leak, the nasogastric tube was removed, and oral intake resumed on POD 6. On POD 11, he developed respiratory distress, and imaging demonstrated a recurrent esophagopleural fistula; percutaneous drainage was placed, and EVT was initiated. The defect healed by POD 35 after five sponge exchanges, and he was discharged to rehabilitation on POD 40. Enteral nutrition was discontinued 2 months later, and he tolerated a normal diet at 5 months.
Remaining cases—brief outcomes
All cases are briefly summarized in Table 1.
Summary of Cases
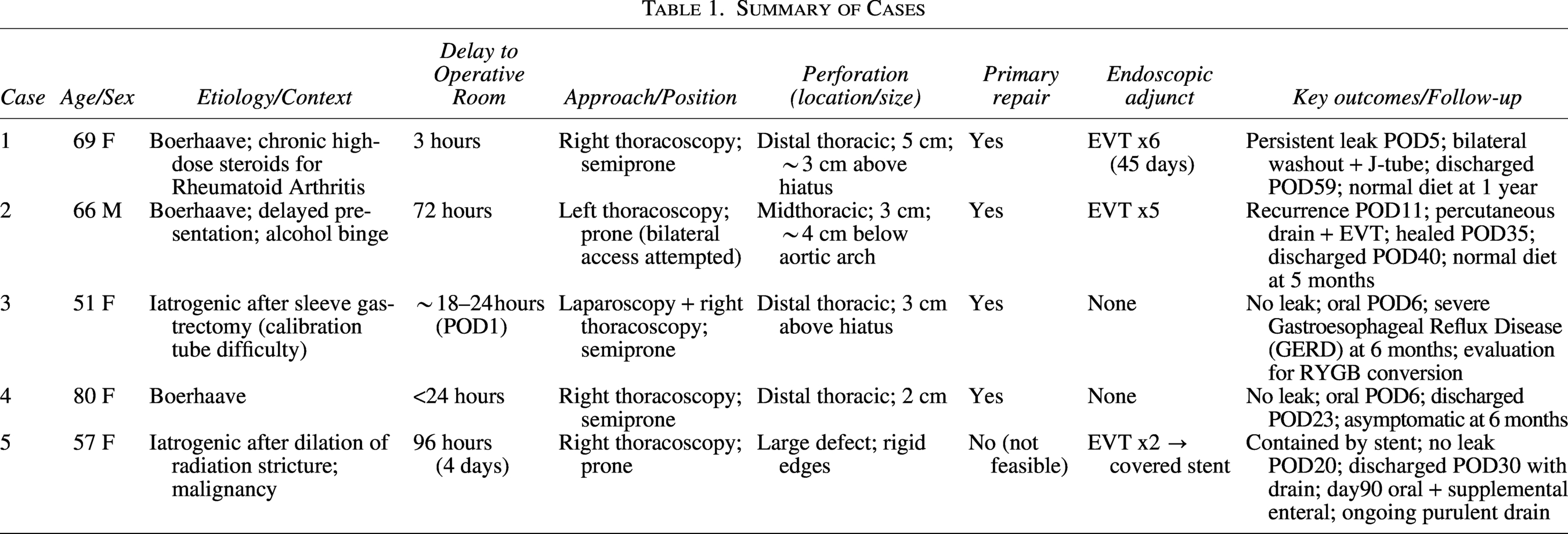
Case 3: An 80-year-old woman presented with fever and chest pain. CT demonstrated right pleural effusion, pneumomediastinum, and right pleural contrast leak. Right semiprone thoracoscopy found a 2-cm perforation in the distal esophagus. Primary repair was performed with barbed suture and thoracic drainage. Oral intake started on POD 6, drains were removed on PODs 3 and 9, and she was discharged on POD 23; she remained asymptomatic at 6 months.
Case 4: A 51-year-old woman developed severe sepsis and right thoracic pain on POD 1 after laparoscopic sleeve gastrectomy; the anesthetist reported difficulty inserting the calibration tube. CT showed right pleural contrast extravasation without abdominal contamination. Exploratory laparoscopy confirmed no abdominal contamination. Right semiprone thoracoscopy identified a 3-cm distal thoracic EP above the hiatus. Primary repair was performed with direct suturing and thoracic drainage. The postoperative course was uneventful, and oral intake began on POD 6. At 6 months, she had full nutritional autonomy but significant reflux symptoms and was being evaluated for conversion to Roux-en-Y gastric bypass (RYGB).
Case 5: A 57-year-old woman with lung cancer treated with chemo-radiotherapy had radiation-induced esophageal stenosis and presented with sepsis and thoracic pain 4 days after endoscopic dilation. CT revealed massive right pleural contrast extravasation. Right prone thoracoscopy showed a delayed EP with dense adhesions, extensive pleural inflammation, and a large rigid-edged defect not amenable to suturing; extensive lavage/debridement and drainage were performed. EVT was initiated on POD 2, and a laparoscopic gastrostomy was created for nutrition. Pathology showed poorly differentiated esophageal adenocarcinoma; EVT was discontinued after two sponge changes, and a covered esophageal stent was placed. POD-20 contrast CT showed no further leak. She was discharged on POD 30 with ongoing low-volume purulent drainage (∼30 mL/day). At day 90, she tolerated oral intake but still required supplemental enteral nutrition; the drain remained in place, and she resumed chemotherapy under oncology follow-up.
Discussion
In a pivotal study, Vogel et al. 13 demonstrated that effective thoracic and mediastinal drainage, using a combination of surgical (minimal thoracotomy), endoscopic, and radiological techniques, was the mainstay of EP management. Using their aggressive conservative approach, they reported an impressive mortality rate of 4.2% in a series of 47 consecutive patients; of them, 34 had thoracic EP, and their mortality was 5.8%. The goals highlighted by Vogel et al. can now be achieved by using minimally invasive surgery techniques (thoracoscopy and laparoscopy).
As expected, several expert teams in esophageal surgery have started offering minimally invasive surgery for the treatment of EP.14,15 Given the rarity of the condition, most publications consist of clinical cases or small series. Aiolfi et al. 16 conducted a recent literature review focusing on minimally invasive surgery for spontaneous EP. They collected a total of 16 articles involving 48 patients and demonstrated the feasibility of the minimally invasive surgical approach in expert hands. The management primarily involved a thoracic approach with direct repair, showing encouraging results, as the overall mortality was relatively low (8.3%). However, the overall morbidity (64.5%) and the risk of persistent esophageal fistula (19.3%) were comparable to historical series (Table 2). summarizes the literature and the different technical details reported for the laparoscopic management of EP.
Technical Details of Laparoscopic Management of Esophageal Perforation
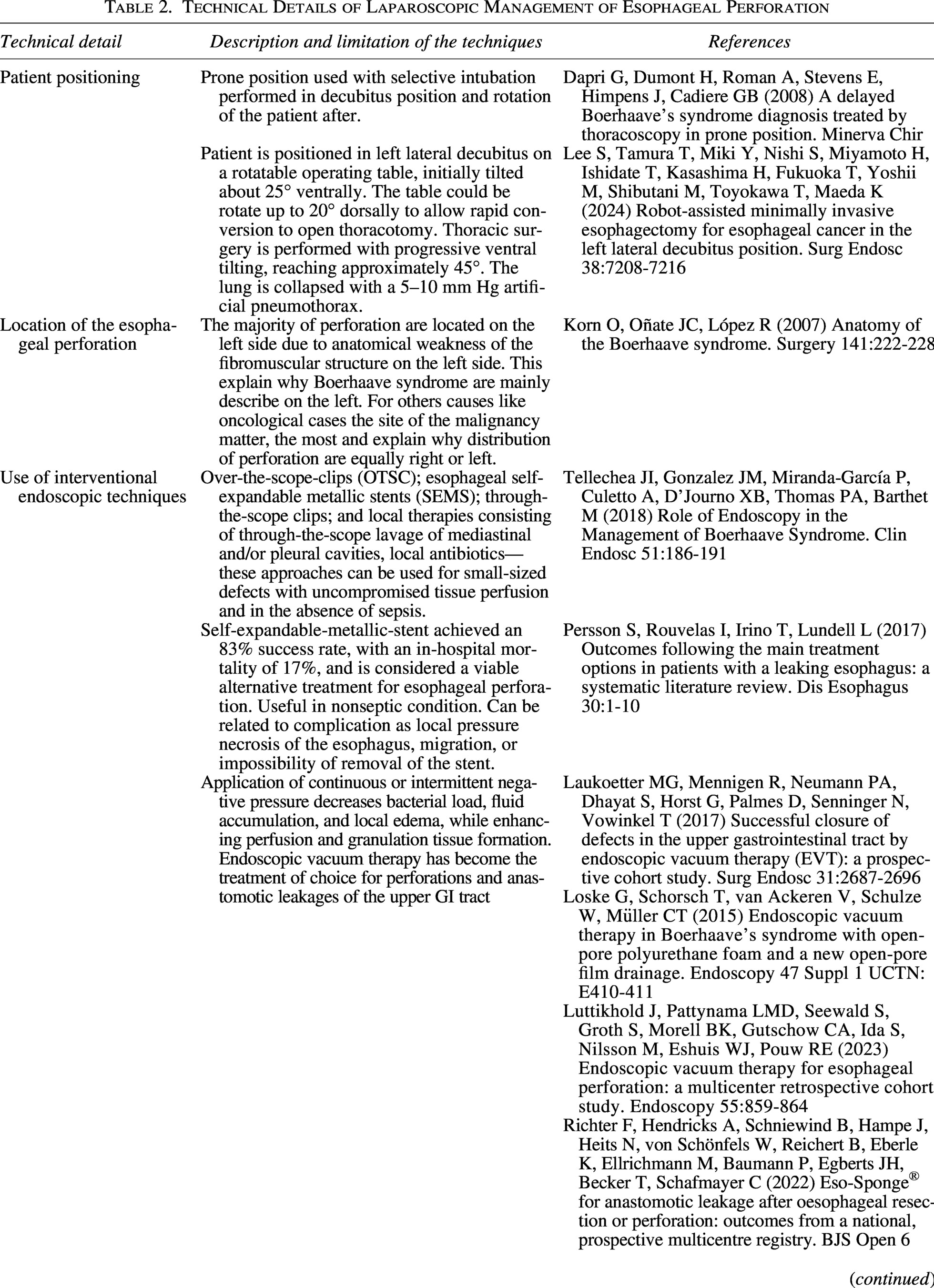

Based on our experience with esophageal cancer patients, we decided to use minimally invasive surgery combined with endoscopic techniques for the management of EPs. We compiled a series of 5 patients requiring emergency surgery over 1 year. This relatively small series represented well the spectrum of the most frequently encountered clinical scenarios: Iatrogenic EP, spontaneous EP, left- and right-sided locations, variable delays in treatment, and EP occurring both in healthy and pathological esophagi. Thanks to this broad range of clinical situations, we have learned some valuable lessons worth discussing.
The prone position is optimal for accessing the esophagus, but its main drawback is the difficulty of conversion to thoracotomy in case of technical issues (bleeding, dissection, or reconstruction difficulties). We placed the first 2 patients in the semiprone position, which we employ in esophageal cancer surgery, as we consider it a good compromise in terms of the benefit–risk balance between lateral decubitus (suboptimal esophageal exposure and easy conversion to thoracoscopy) and prone (excellent esophageal exposure and difficult conversion). Unlike thoracoscopy for cancer, in the case of EP, the esophageal defect is relatively easily identifiable without the need for extensive dissection; there is no need for reconstruction with all its pitfalls. Thus, the risk of requiring an emergency conversion to thoracotomy is minimal, and our experience suggests that positioning the patient in the prone position is preferable in the context of EP. The major advantage is that the prone position allows easy access to both hemithoraxes, which can be useful in the case of intubation errors (as in the case of patient 3) or if exploration/drainage of the contralateral hemithorax is needed.
It is generally accepted that the approach should be preferentially made from the side of the perforation. Esophageal surgery can be performed by thoracic surgeons who are comfortable on both sides or, more commonly, by gastrointestinal or general surgeons who are more comfortable with the right hemithorax (the usual side for esophageal cancer approaches). The approach to left-sided esophageal diverticula through the right side has been described, but the presence of inflammatory tissues and adhesions can make dissection of the left/right edges of the esophagus tricky when attempted from the contralateral side. In fact, our attempt to approach a delayed left-sided perforation from the right failed, highlighting the importance of approaching the perforation from the appropriate side. If the side of the EP could not be clearly identified during preoperative work-up, putting the patient in the prone position allows for the identification of the perforation site and its treatment via a bilateral thoracoscopic approach if required. Technically, the left thoracoscopic approach is more challenging. The main difficulty is related to the aortic arch, which narrows the operative field, and the position of the descending aorta, which overhangs the esophagus. To overcome such technical issues, it is sometimes necessary to position the trocars lower than on the right side and, if needed, add additional trocars.
Management of delayed EP and EP on pathological esophagus. Management of persistent esophageal leaks. Persistent leaks are a relatively frequent event after direct repair of EP, occurring in 20%–50% of cases. 17 The risk is higher when suturing inflammatory (delayed perforations) or pathological tissues (cancer, achalasia, etc.). In our experience, a persistent leak was recorded in 3 (60%) of 5 patients; leaks occurred in patients with well-known risk factors (steroid use, delayed perforation, and perforation in cancer). Treatment of delayed EP and EP in immunocompromised patients is a difficult challenge, 18 and a wide variety of procedures have been described over the years, ranging from simple reinforcement of the esophageal suture (pleural or pericardial flaps) to more complex approaches 19 (pedicled muscle flaps, free flaps, two-stage procedures, etc.). Most of these solutions are beyond the expertise field of the average emergency surgeon who takes care of such patients. For EP occurring on a pathological esophagus, most authors recommend performing an emergency esophagectomy. 20 These challenging situations are typically associated with significant increase in mortality.21,22
The use of EVT techniques resulted in definitive closure of persistent esophageal leaks after direct suture of delayed EP and in a patient with long-term corticosteroid treatment. The patient with perforation due to cancer would have required an esophagectomy, with disastrous physical and psychological consequences. Di Franco et al. 4 showed that patients with EP due to cancer have a 12-month limited survival, often without the possibility of subsequent reconstruction or resumption of oncological treatment; they questioned the reasonableness of proposing such a heavy treatment in this context. Instead, the minimally invasive management of our patient allowed for discharge, resumption of partial oral intake, and continuation of cancer-directed treatment aim.
The major drawback of the present study is the small number of patients, which is due to the scarcity of EP and decreasing indications for emergency surgery. There is the need for confirmation of these results by other teams.
In conclusion, our data suggest that a standardized approach may be considered for thoracic EPs requiring emergency surgery. A minimally invasive strategy, combined with endoscopic management of persistent fistulas using modern techniques such as EVT or covered esophageal stents, appears to be a feasible option in selected patients, regardless of treatment delay or esophageal condition. From a technical perspective, the thoracoscopic approach may be performed from the side of the perforation with the patient in the prone position. Although based on a limited series, our findings support the feasibility of this strategy and may help guide surgical management in this challenging clinical setting.
Authors’ Contributions
Q.C.-P. and M.C.: Study concept, study design, and writing—original draft preparation. E.D., P.Y.S., J.A., and E.G.: Writing—editing and writing—review. The authors did not preregister the research with an analysis plan in an independent, institutional registry, as the study was conducted retrospectively after the data were collected.
Footnotes
Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.