
Abstract
Background:
Ectopic testis (ET), testicular descent outside the normal pathway, is a rare condition with variants such as perineal ET (PET), femoral ET (FET), and transverse testicular ectopia (TTE). Most studies on ET have reported open surgical techniques, whereas laparoscopic evidence remains limited. This retrospective single-center study evaluated the feasibility and safety of laparoscopic orchiopexy for pediatric ET.
Methods:
We retrospectively reviewed 2306 pediatric patients aged <10 years who underwent laparoscopic orchiopexy for abnormal testicular descent between January 2016 and December 2024 at Damsoyu Hospital, Seoul, Republic of Korea. Among them, 11 were diagnosed with ET and classified as PET, FET, or TTE based on the location of the testis. PET and FET showed the testis elevated into the abdominal cavity and repositioned through the inguinal canal. On TTE, both testes were separated intraabdominally and fixed bilaterally.
Results:
The cohort included 3 PET, 3 FET, and 5 TTE patients, with a mean age of 19.8 months (6–86) and a mean operating time of 38.4 minutes (31–1). The average testicular size increased from 12 mm preoperatively to 13 mm on the 3-month postoperative follow-up ultrasonography. No intraoperative or postoperative complications occurred in the ET group, and conversion to open surgery was not required. During the mean follow-up of 55.7 months, no testicular atrophy or reoperation was observed.
Conclusion:
Although the cohort size is small due to the rarity of ET, these findings demonstrate that laparoscopic orchiopexy is feasible and safe for pediatric ET.
Keywords
Introduction
The incidence of undescended testis (UDT), one of the most common congenital anomalies in male infants, is 1%–5% in full-term neonates, and higher rates are reported among premature infants.1,2 Unlike UDT, which represents arrest along the normal descent pathway, ectopic testis (ET) refers to deviation from this physiological route to an aberrant location. While UDT remains along the expected path (intraabdominal or inguinal), ET is found outside this pathway, such as in perineal (perineal ET [PET]), femoral (femoral ET [FET]), or contralateral (transverse testicular ectopia [TTE]) positions. 3 The aberrant descent pattern of ET has been attributed to abnormal gubernacular attachment or deviation during embryologic migration. 4 This anatomical distinction has important surgical implications, as ET requires redirection rather than simple mobilization. Detailed anatomical studies have further characterized variations in testicular descent and ectopic positioning. 4 These variants—PET, FET, and TTE—account for <1% of all reported UDT cases, 5 although they are clinically important due to diagnostic ambiguity, potential association with inguinal hernias, and the need for precise anatomical dissection.
When a child is diagnosed with UDT, timely orchiopexy is recommended to preserve fertility and facilitate the early detection of testicular malignancy.6,7 UDTs are generally treated via inguinal or scrotal incisions or laparoscopy.8,9 ET deviates entirely from the physiological descent pathway and often requires individualized surgical access based on its location. Unlike UDT, which involves failure of descent, ET entails aberrant descent to a nonscrotal position, necessitating repositioning rather than simple mobilization.
PET, TTE, and FET require nonstandard incisions due to their atypical locations. Therefore, repositioning the ET through the physiological inguinal pathway is essential to restore normal anatomical descent. Most ETs divert from the inguinoscrotal pathway at the internal inguinal ring level. Laparoscopic surgery enables traction of the ET on the internal ring.
Laparoscopic orchiopexy, first introduced by Jordan et al. in the early 1990s, 9 has become the preferred approach for nonpalpable UDT owing to its diagnostic and therapeutic advantages. Over the past decades, various laparoscopic techniques for orchiopexy have been developed, including single-stage vessel-preserving approaches, staged Fowler–Stephens procedures, and traction-based methods for high intraabdominal testes. 10 Recent large single-center series and systematic reviews have demonstrated favorable safety profiles and satisfactory testicular growth outcomes following laparoscopic orchiopexy across different anatomical scenarios. These evolving minimally invasive strategies have refined surgical decision-making and expanded the applicability of laparoscopy in pediatric testicular pathology.11–15
However, most published laparoscopic data focus primarily on UDT or intraabdominal testis, and systematic evaluation across the major subtypes of ET remains limited. In this context, we applied a unified laparoscopic approach to PET, FET, and TTE to assess feasibility and reproducibility.
Due to the low incidence and anatomical variability of ET, there is limited consensus regarding the optimal surgical management approach. Existing reports are limited in scale and technical heterogeneity, which impede standardization. Nonetheless, the laparoscopic approach offers several advantages, including precise anatomical assessment, careful dissection, and minimal invasiveness.16,17 These strengths support its potential role in ET management. However, no systematic reports have evaluated laparoscopic outcomes for all ET subtypes, including PET and FET. This study aims to address this gap in the literature by assessing the safety and efficacy of laparoscopic orchiopexy in pediatric patients who underwent PET, FET, and TTE.
Materials and Methods
This retrospective study included pediatric patients aged ≤10 years old who underwent laparoscopic orchiopexy for abnormal testicular descent at Damsoyu Hospital, Seoul, Republic of Korea, between January 2016 and December 2024 (Fig. 1). Patients with preoperative testicular atrophy were excluded from the analysis. A total of 2319 pediatric patients underwent laparoscopic orchiopexy during the study period. Of these, 13 patients in the UDT group were excluded due to loss to follow-up. Thus, 2306 patients were included in the final analysis. All patients in the ET group completed follow-up. Among them, 11 were diagnosed with ET and classified as PET, FET, or TTE based on the location of the ET. This study was approved by the Institutional Review Board of Damsoyu Hospital (DSY-2025-002, approved on July 14, 2025).
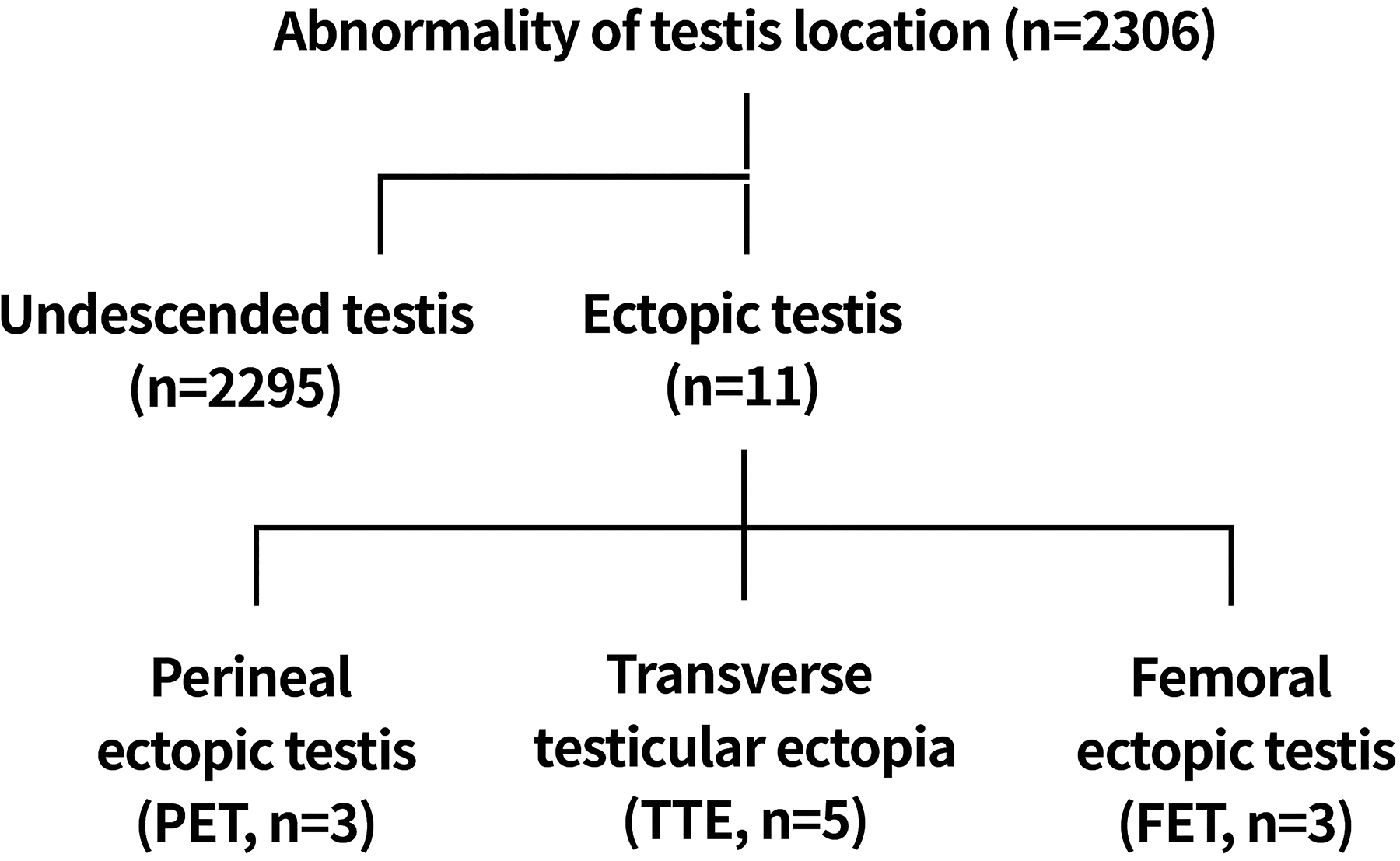
Patient flowchart.
Study outcomes
The primary outcome of this study was the feasibility and safety of laparoscopic orchiopexy for ET, defined by successful completion without conversion to open surgery, the absence of intraoperative or postoperative complications, and the absence of testicular atrophy.
Secondary outcomes included postoperative scrotal position, early ultrasonographic testicular growth at 3 months, and detection of associated inguinal hernia or patent processus vaginalis.
Laparoscopic procedures
Under general anesthesia, the patients were placed in the supine position. A 2.9-mm 0° rigid camera and 2.7-mm laparoscopic instruments were used. After umbilical eversion, a 3-mm trocar was placed via a 3-mm incision to establish pneumoperitoneum (6–8 mm Hg). Two additional 3-mm stab incisions were made bilaterally on the lower abdomen parallel to the umbilicus. The laparoscopic instruments were inserted directly without trocars.
The ectopic testes were first mobilized into the abdominal cavity. Adequate mobilization was defined as sufficient length of the spermatic cord to allow tension-free placement of the testis within the scrotum without vascular compromise. Care was taken to avoid excessive traction or torsion of the cord structures during dissection. For PET (Fig. 2) and FET (Fig. 3), the testes were redirected through the inguinal canal and fixed in the dartos pouch of the scrotum. A subdartos pouch was created through a small transverse scrotal incision, and the testis was secured within the pouch using an absorbable suture to prevent retraction. For TTE (Fig. 4), the testes were separated intraabdominally and individually transferred through the respective inguinal canals for bilateral scrotal fixation.
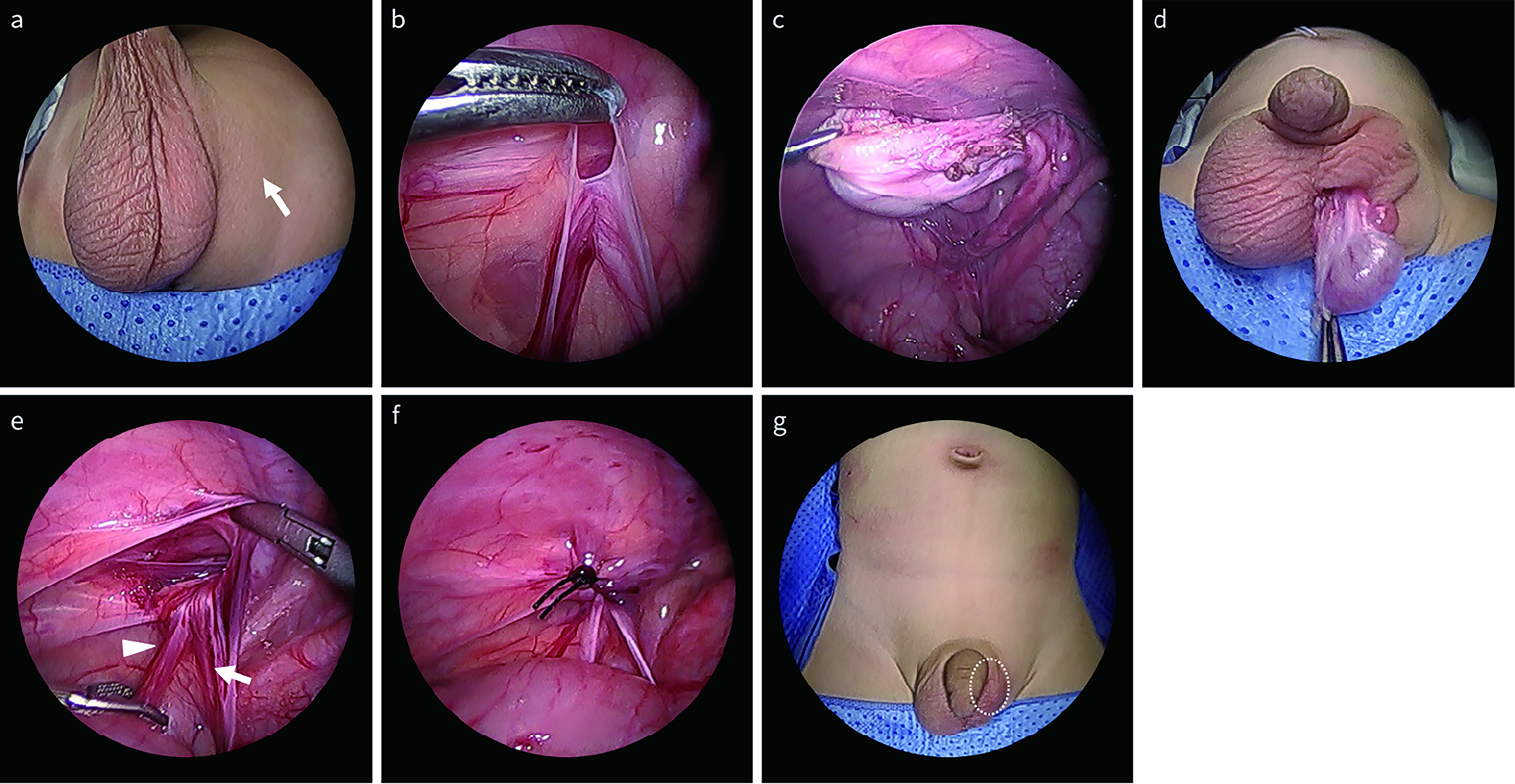
Laparoscopic orchiopexy for PET.
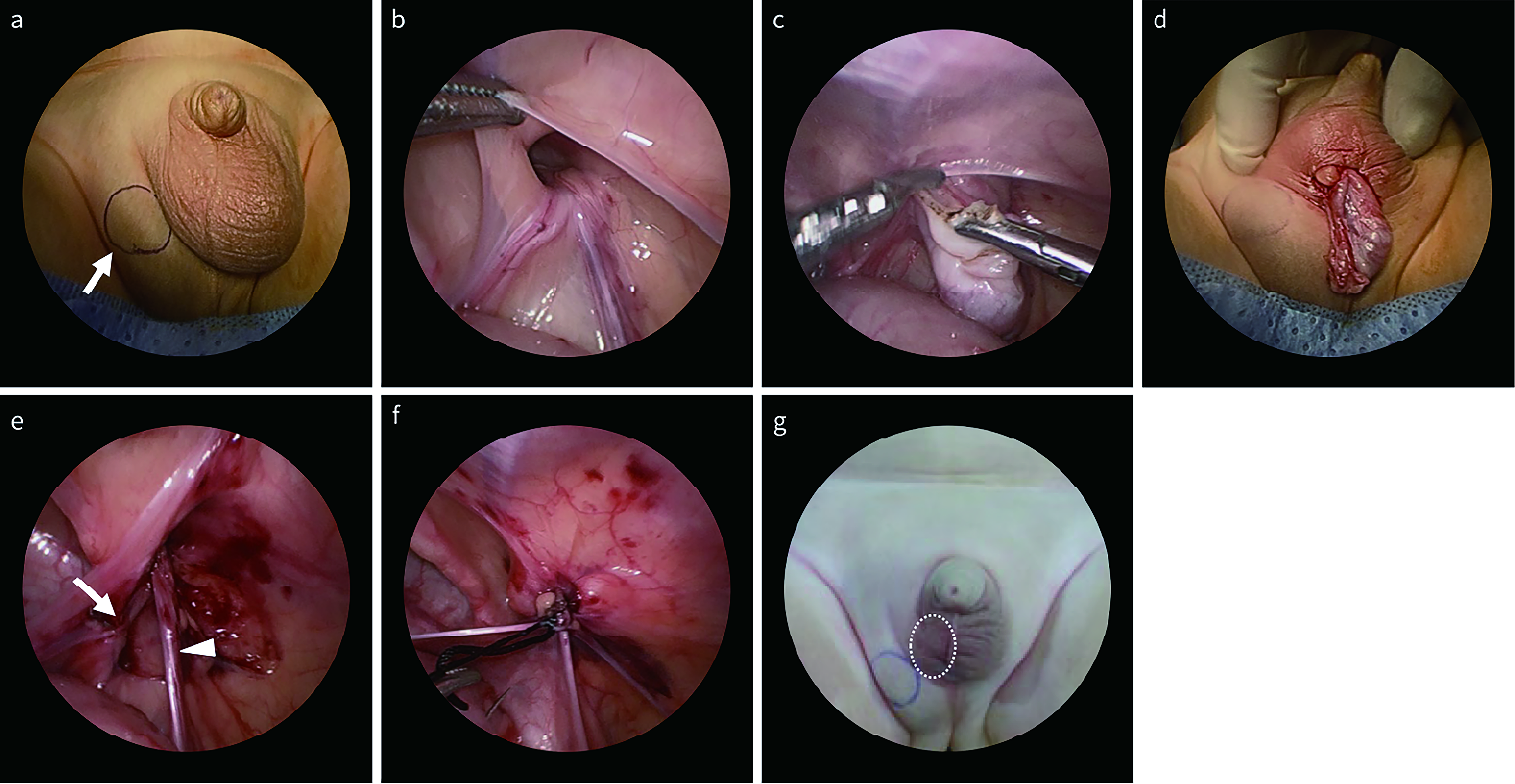
Laparoscopic orchiopexy for FET.
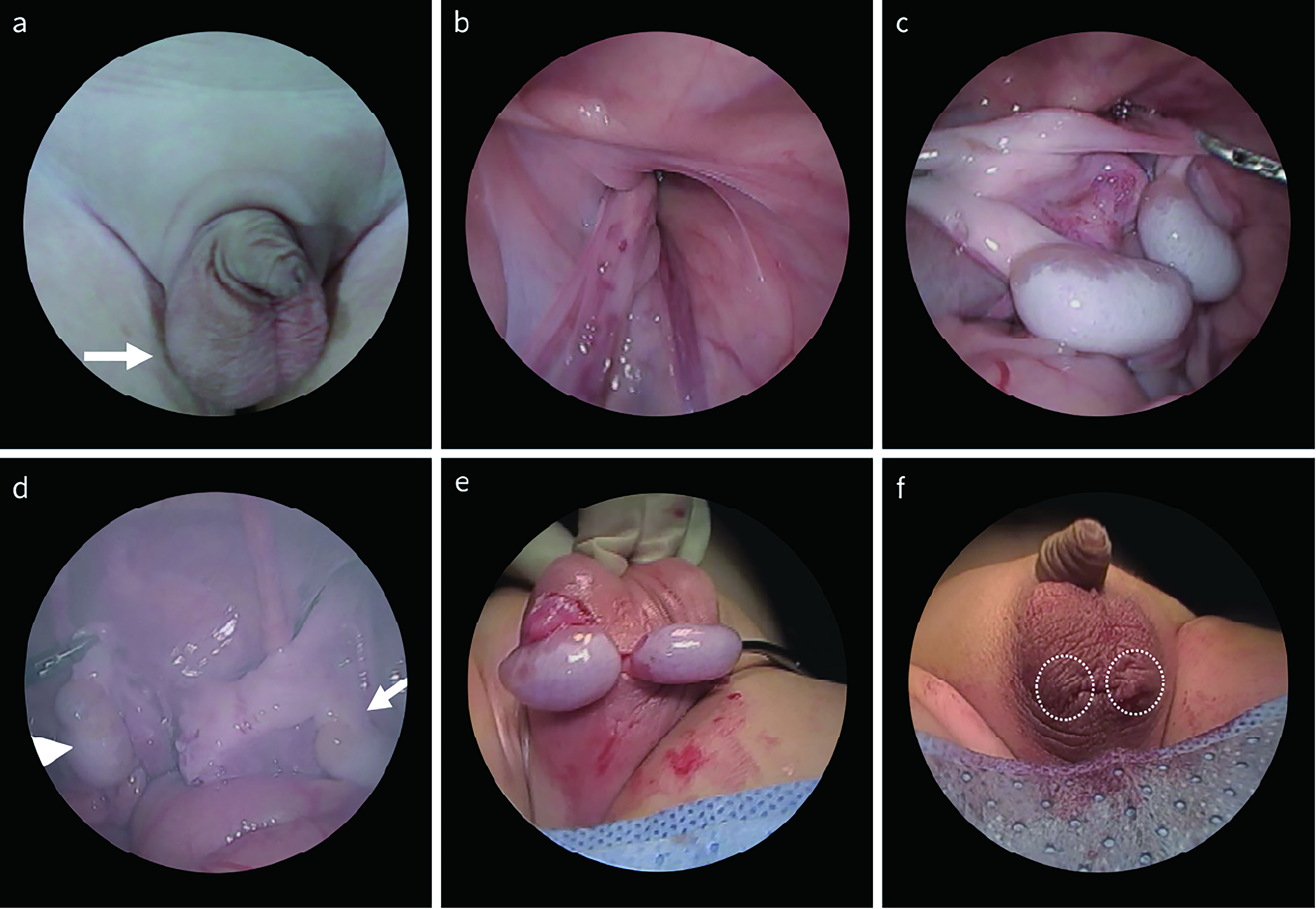
Laparoscopic orchiopexy for TTE.
In one patient with PET, the internal inguinal ring was obliterated, necessitating careful canalization to allow safe passage into the scrotum. The peritoneum was carefully incised to allow further mobilization of the spermatic cord. Gentle dissection of the cord structures, including the vas deferens and testicular vessels, was performed to obtain additional length while avoiding vascular compromise.
After adequate mobilization, the testes were fixed to the scrotum using absorbable sutures (Monosyn® 5-0; B. Braun Surgical, S.A., Rubí, Spain). Skin closure was performed using a topical adhesive (Dermabond; Ethicon, Inc.).
Statistical methods
Statistical analyses were performed using the R software (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation and compared using Welch’s t-test. In addition, the Mann–Whitney U test was performed as a nonparametric sensitivity analysis to account for potential distributional differences between groups. Categorical variables were analyzed using Fisher’s exact test or the chi-square test, as appropriate. All tests were two-sided, and a P value of <0.05 was considered statistically significant. Comparative analyses between ET and UDT were exploratory in nature and not inferential.
Results
Table 1 lists the comparison results between the UDT and ET. Table 1 summarizes the descriptive comparison between the UDT and ET groups. Given the small number of ET cases, these comparisons were intended to provide contextual reference rather than definitive statistical inference. Among the 2306 pediatric patients who underwent laparoscopic orchiopexy, 11 (0.48%) were diagnosed with ET, comprising 5 TTE, 3 FET, and 3 PET cases. In the ET group, the mean age was 19.8 months (6–86), and the mean operating time was 38.4 minutes (31–51).
Comparison of Demographic and Operative Variables Between Undescended Testis and Ectopic Testis
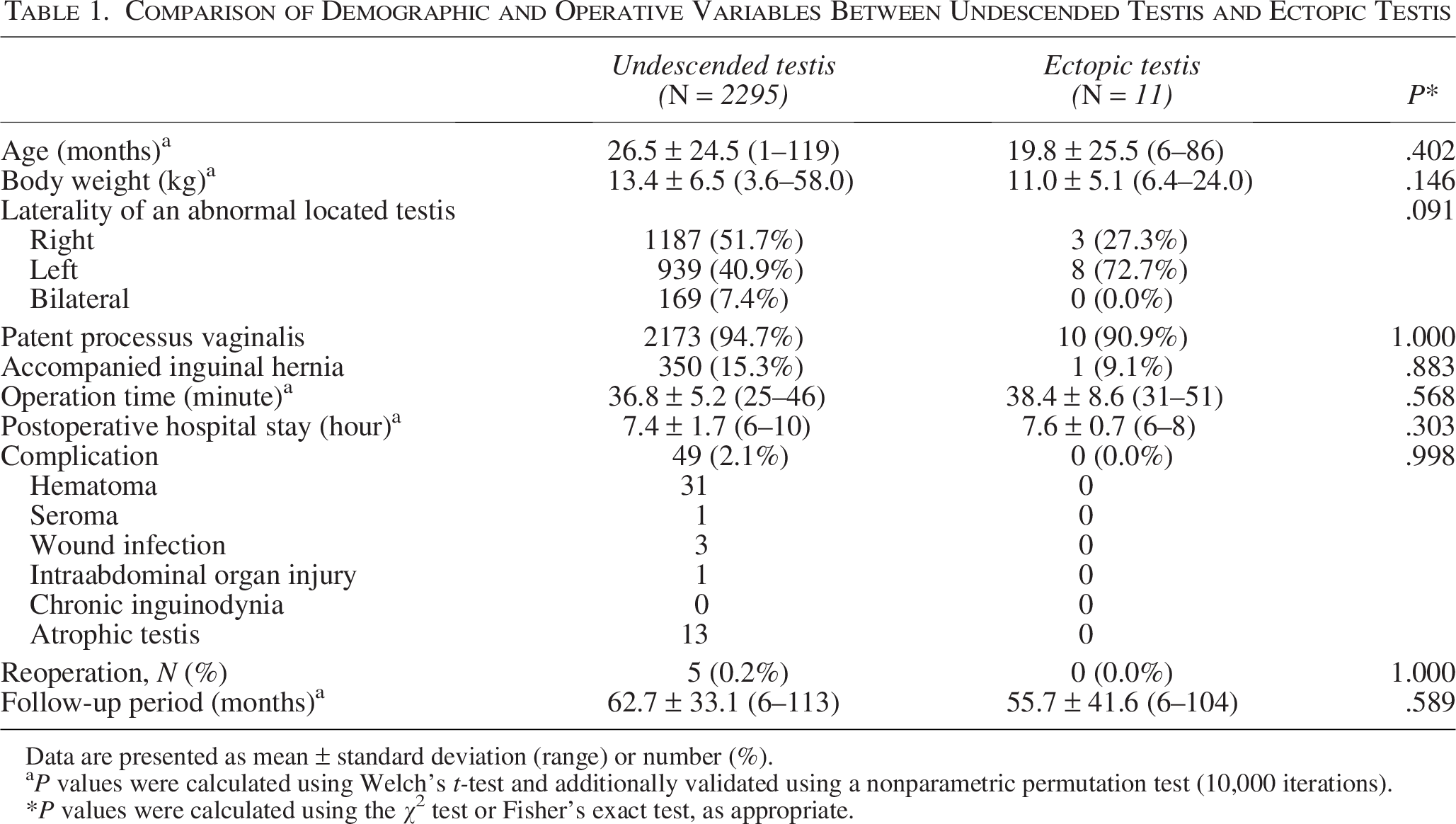
Data are presented as mean ± standard deviation (range) or number (%).
P values were calculated using Welch’s t-test and additionally validated using a nonparametric permutation test (10,000 iterations).
*P values were calculated using the χ² test or Fisher’s exact test, as appropriate.
The ET was more frequently left-sided (8/11, 72.7%), and patent processus vaginalis was present in 10 patients (91%). Moreover, 1 patient had a concomitant inguinal hernia. The mean clinical follow-up period of the ET group was 55.7 months, during which annual outpatient evaluations were performed. Ultrasonographic assessment was routinely conducted at 3 months and 1 year postoperatively.
Individual analysis (Table 2) demonstrated consistent postoperative testicular growth and vascularity across all patients, with the average testicular size increasing from 12 mm preoperatively to 13 mm on the 3-month postoperative follow-up ultrasonography (Fig. 5). No intraoperative or postoperative complications, testicular atrophy, reoperation, or open conversion were observed. These findings indicate successful surgical outcomes and the preservation of testicular viability.
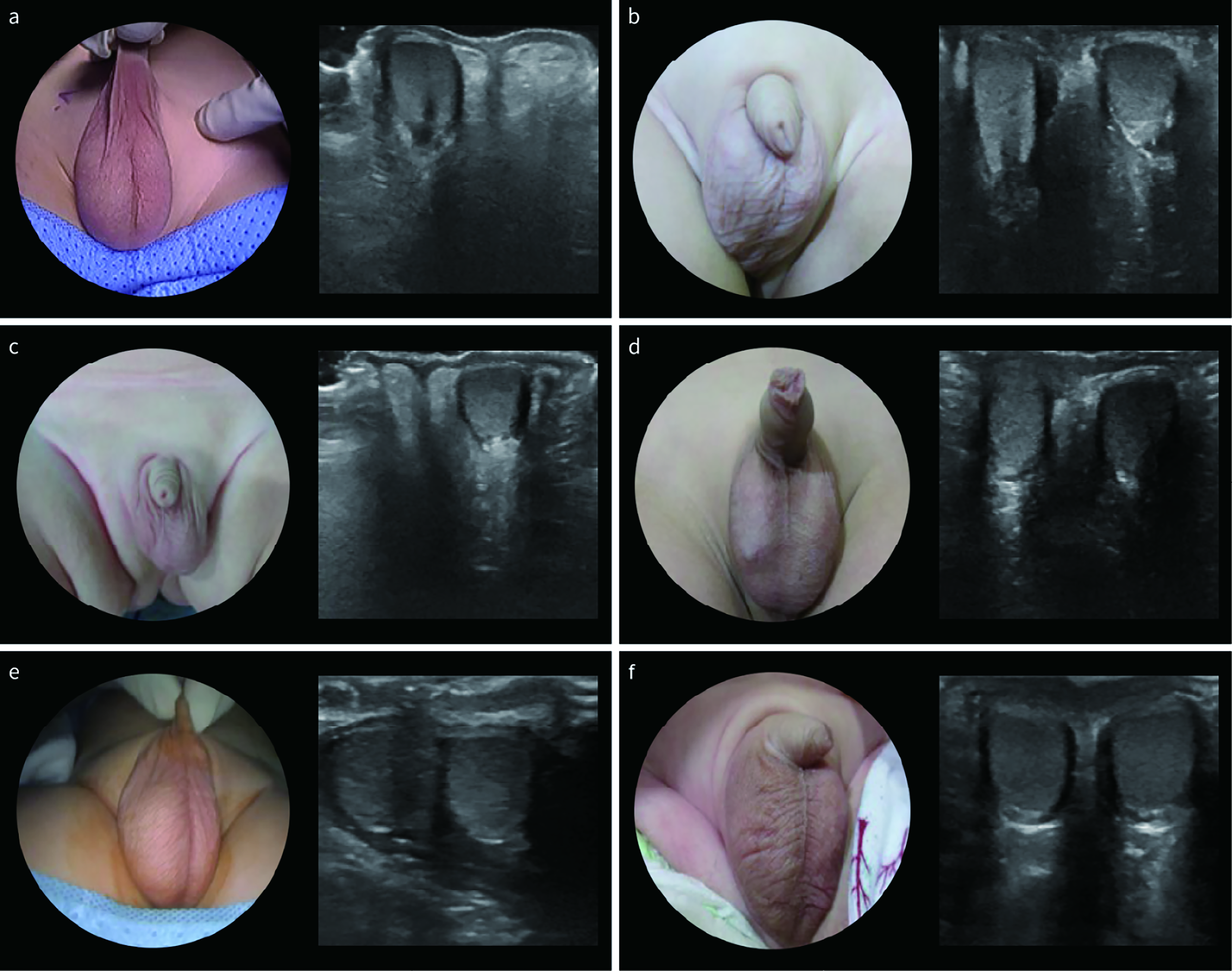
Preoperative and 3-month postoperative appearance and ultrasonography.
Clinical Characteristics of Ectopic Testis
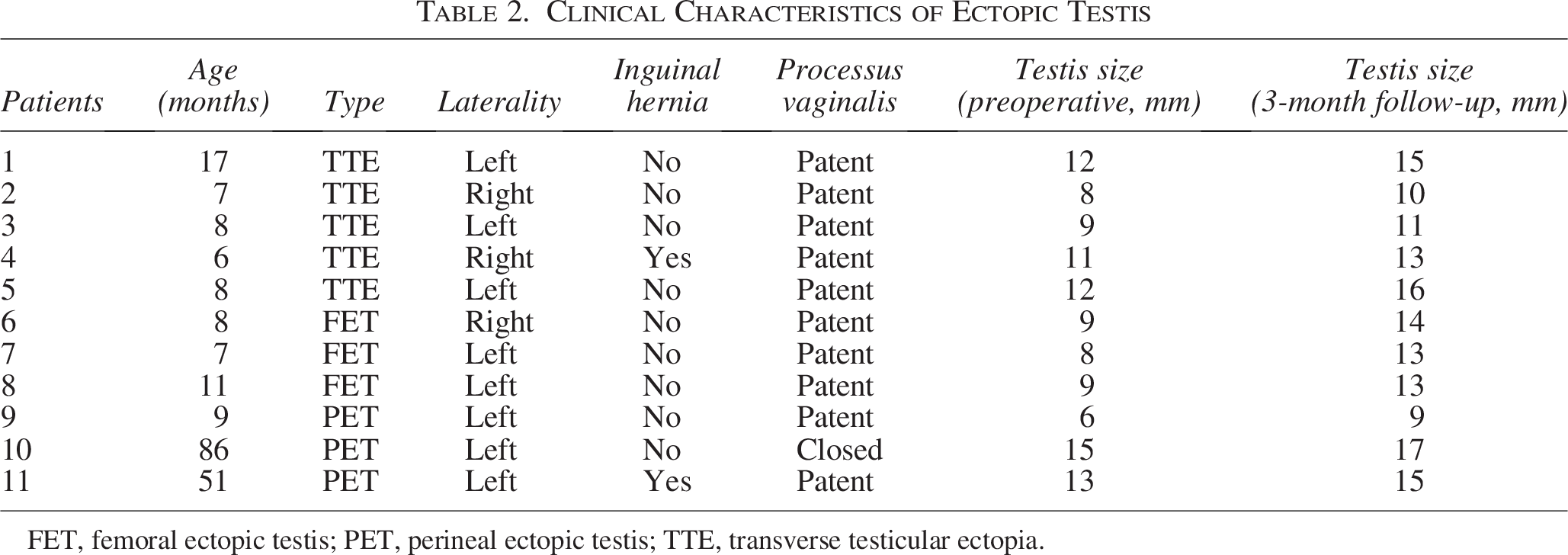
FET, femoral ectopic testis; PET, perineal ectopic testis; TTE, transverse testicular ectopia.
Discussion
This case series evaluated the feasibility and outcomes of laparoscopic orchiopexy, including rare variants of PET, FET, and TTE, in patients with ET. All procedures were completed without conversion to open surgery. At follow-up, all testes were well-positioned in the scrotum with preserved vascularity and normal growth. No postoperative complications, such as testicular atrophy or inguinal hernia recurrence, were observed. Our findings reinforce that laparoscopic orchiopexy is a safe and effective approach for treating ET, consistent with previously reported long-term outcomes. 18
Most existing reports on the treatment of ET are limited to individual case reports or small retrospective series, with a greater focus on TTE owing to its distinct anatomy and frequent association with intraabdominal exploration.19–21 Several successful laparoscopic orchiopexies have been documented for TTE, particularly in settings requiring diagnostic laparoscopy.16,17,22 PET and FET have traditionally been managed with open orchiopexy via the perineal, inguinal, or scrotal approaches, based on the ectopic location.5,23,24 This discrepancy reflects the conventional reliance on localized incisions and superficial accessibility of PET and FET. However, the laparoscopic approach offers superior intraabdominal visualization and the ability to reposition the testis through the physiological inguinal canal, thereby maintaining anatomical orientation and minimizing tissue dissection. Although laparoscopic dissection for PET and FET requires careful mobilization and may appear technically demanding, it provides the advantage of restoring descent along the natural pathway, reducing the risk of tension or torsion on the spermatic cord.
A notable advantage of the laparoscopic approach is its ability to restore the ET to its anatomical point of origin within the abdominal cavity, followed by physiological redirection through the natural inguinal canal into the scrotum. This technique respects the embryological pathway of testicular descent and minimizes unnecessary dissection of the surrounding tissues. Consequently, laparoscopic orchiopexy may reduce the risk of cord injury, inadequate fixation, and postoperative complications.6,9
For TTE, laparoscopy is particularly advantageous, as it allows bilateral exploration, separation of crossed cords, and simultaneous orchiopexy. This consistency across all ET subtypes supports the adoption of laparoscopy as a unifying approach. Nevertheless, it must be acknowledged that open orchiopexy remains a practical and safe option for PET and FET in many settings, especially where laparoscopic expertise or instruments are limited.
Moreover, real-time intraabdominal visualization provided by laparoscopy enables the accurate localization of the testes and related structures, the assessment of vascular anatomy, and the identification of associated anomalies, such as a patent processus vaginalis or Müllerian remnants. Importantly, by employing a unified surgical route, irrespective of the ectopic location, this approach preserves anatomical continuity and enhances surgical reproducibility. This, in turn, contributes to greater surgical standardization and facilitates training in pediatric orchiopexy. Although pediatric laparoscopy entails technical challenges, such as restricted working space and the need for delicate instrumentation, these challenges are frequently outweighed by the diagnostic clarity and anatomical precision it affords.
This study has several strengths. To the best of our knowledge, this is among the first systematic laparoscopic series to include PET and FET using a unified surgical protocol. All operations were conducted by a single experienced surgeon to ensure consistency in the technique and outcomes. The limitations of this study include its retrospective design and small cohort size inherent to the rarity of ET. The comparison between ET and UDT groups was underpowered due to the limited number of ET cases and should be interpreted cautiously. These analyses were exploratory and intended to provide contextual understanding rather than definitive comparative conclusions. Additionally, postoperative testicular size was quantitatively assessed at 3 months, as this time point was considered sufficient to confirm early viability and stable scrotal positioning after surgery. In our clinical protocol, ultrasonographic evaluation is routinely performed at 3 months and 1 year postoperatively, followed by the annual outpatient follow-up. The mean clinical follow-up period was 55.7 months. However, standardized serial volumetric measurements beyond 3 months were not consistently recorded in a format suitable for formal longitudinal statistical analysis. Therefore, long-term volumetric growth and endocrine or fertility-related outcomes were not formally evaluated. All procedures were performed by a single experienced surgeon at a high-volume center, which may limit the generalizability of the findings. Although the described technique is conceptually reproducible, validation in lower-volume institutions and by surgeons with varying levels of laparoscopic experience is warranted.
Despite these limitations, this case series is among the first to apply a unified laparoscopic technique to all major ET subtypes, providing valuable evidence that the approach is feasible and reproducible in pediatric practice. Accumulating additional pediatric ET cases will allow the refinement of laparoscopic dissection and fixation strategies and optimize treatment guidelines specific to each ET subtype.
In conclusion, laparoscopic orchiopexy offers a feasible and safe approach for correcting pediatric ET, including rare variants such as perineal, femoral, and transverse types. While open surgery remains appropriate in select cases, laparoscopy provides consistent anatomical visualization and standardized management.
Ethics Approval
This study was approved by the Institutional Review Board of Damsoyu Hospital (DSY-2025-002, approved on July 14, 2025).
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Acknowledgments
The authors thank Hyejin Park for conducting the primary English grammar correction of this article, and Beom Seok Oh from the Research Center of Damsoyu Hospital and Young Hyun Lee from the Ewha Womans University Graduate School of Engineering for their assistance with statistical analysis and data organization.
Disclosure Statement
S.R.L. and R.Y.J. have no conflicts of interest or financial ties to disclose.
Funding Information
The authors have no financial ties to disclose.