
Abstract
Backgrounds:
Indocyanine green (ICG) is a fluorescent biocompatible dye that emits light in the near-infrared spectrum upon excitation, enabling real-time visualization of vascular anatomy and tissue perfusion during surgery. Its favorable safety profile and rapid pharmacokinetics have led to widespread adoption across surgical specialties. More recently, ICG fluorescence imaging has been utilized for tumor localization in adrenalectomy, improving intraoperative decision-making, particularly in complex anatomical regions.
Methods:
A comprehensive literature search was conducted using PubMed, EMBASE, and Google Scholar databases. Tailored search strategies were applied for each topic addressed in this review. Articles were considered eligible for inclusion if they met the following criteria: (1) original research studies, randomized controlled trials, or systematic reviews with or without meta-analysis; (2) studies involving human subjects; and (3) publications in the English language. All selected studies underwent independent review by 2 authors, and any discrepancies were resolved through discussion with a third reviewer.
Results:
ICG fluorescence imaging is a valuable adjunct for adrenal gland identification, as the adrenal cortex demonstrates strong fluorescence due to its rich vascularization, allowing clear differentiation from surrounding retroperitoneal tissue. Adrenocortical tumors typically exhibit a hyperfluorescent pattern, whereas medullary tumors and malignant lesions more commonly demonstrate hypofluorescence, likely reflecting differences in their underlying biochemical and anatomical characteristics. Furthermore, ICG is particularly useful in partial adrenalectomy for bilateral tumors, facilitating precise tumor localization and resection while preserving functional adrenal cortical tissue.
Conclusions:
ICG fluorescence imaging is a valuable adjunct in adrenal surgery, enabling real-time visualization of adrenal anatomy, vascular structures, and tissue perfusion. Its application improves gland identification, facilitates accurate tumor localization, and supports cortical-sparing approaches by preserving functional adrenal tissue.
Introduction
Indocyanine green (ICG) is a fluorescent biocompatible dye that emits light in the near-infrared (NIR) spectrum when excited, which allows real-time visualization of vascular anatomy and tissue perfusion during surgical procedures.1–2 Used initially by ophthalmologists for retinal angiography, its application has since expanded to other surgical fields due to its safety profile. 3 In adrenal surgery, ICG fluorescence imaging has been shown to create a contrast distinction between the adrenal and surrounding structures. 4 This article aims to provide a comprehensive review of the current applications of ICG fluorescence in adrenalectomy.
Technical Background
Indocyanine green, first introduced into clinical practice in the mid-1950s, is a relatively nontoxic, NIR fluorescent tricarbocyanine dye characterized by rapid hepatic uptake and biliary excretion. 5 Following intravenous administration, ICG rapidly binds to plasma proteins, primarily albumin, thereby restricting the majority of the injected bolus to the intravascular compartment. 6 This protein binding does not induce structural alteration of the carrier proteins; rather, it creates a biologically inert complex that minimizes systemic toxicity and limits extravasation of the dye.6,7 ICG fluorescence provides high contrast and sensitivity due to excitation and emission within the NIR spectrum. NIR light enhances tissue translucency and permits penetration several millimeters beyond the surface, facilitating improved visualization of subsurface structures compared with shorter wavelengths. 6 Moreover, the peak absorbance of ICG occurs near the isosbestic point of hemoglobin and oxyhemoglobin, at which their optical absorption remains constant regardless of oxygenation state. This property minimizes interference from blood and enhances the accuracy and reliability of fluorescence signal detection. 8 Although hemoglobin exhibits partial absorption within the excitation and emission spectra of ICG, this interaction enhances vascular delineation by increasing relative vessel transparency under NIR imaging. Additionally, the optical properties of blood contribute to an additive fluorescence signal in vascular cross-sections, thereby facilitating improved visualization of perfused structures. 7 A camera system equipped with appropriate optical filters enables visualization of NIR fluorescence emitted by the dye within tissues. This process is performed in real time, permitting the fluorescence signal to be superimposed onto the standard white-light image. 9 The intensity of the fluorescence signal correlates with tissue perfusion, demonstrating greater enhancement in well-vascularized structures, such as the adrenal gland. Intraoperative assessment of ICG fluorescence can be performed rapidly, resulting in only a minimal increase in operative time.
ICG use for gland identification
Precise differentiation of the adrenal gland from surrounding retroperitoneal adipose tissue, accurate delineation of the interface between neoplastic and normal adrenal parenchyma, and reliable identification of critical vascular structures such as the inferior vena cava and renal vessels are essential for the safe and efficient conduct of the procedure. 10 The use of ICG in adrenal surgery offers two principal advantages. First, it provides enhanced contrast distinction between the highly vascular, hyperfluorescent adrenal parenchyma and the relatively less vascular, hypofluorescent retroperitoneal tissues, thereby facilitating precise dissection. Second, ICG fluorescence imaging assists in guiding partial adrenalectomy (PA) by improving delineation between normal adrenal cortex and neoplastic tissue, particularly during the resection of pheochromocytomas. 4 ICG fluorescence imaging provides real-time intraoperative feedback to the surgical team. Hence, the immediate visual feedback afforded by ICG fluorescence may help compensate for the absence of or decreased tactile sensation inherent to minimally invasive surgical approaches. 11
The incorporation of intraoperative ICG fluorescence imaging may facilitate a reduction in the learning curve for surgical trainees, while simultaneously enhancing recognition of anatomical variability for experienced surgeons. 12 Fluorescence-guided visualization can be particularly advantageous during the identification and meticulous dissection of critical vascular structures. This is especially relevant in adrenal surgery, where prompt and accurate identification of the adrenal vein during pheochromocytoma resection is essential to mitigate catecholamine-induced hemodynamic instability associated with tumor manipulation. 13 For optimal imaging, ICG should be administered intravenously after adequate exposure of the retroperitoneum and prior to initiation of adrenal gland dissection. A 5-mg intravenous dose has been reported to provide optimal fluorescence intensity and tissue contrast. 10 Fluorescence of the adrenal gland and surrounding retroperitoneal tissues typically becomes apparent within 30–60 seconds of injection. Peak contrast resolution is generally achieved at approximately 5 minutes, when retroperitoneal adipose tissue demonstrates progressive washout of the dye while adrenocortical tissue retains fluorescence.9,10 This differential retention enhances contrast distinction and facilitates identification of glandular margins relative to adjacent fat and vascular structures. Adrenal fluorescence may persist for up to 20 minutes, providing a sufficient operative window for fluorescence-guided dissection and vascular control. 14
ICG use for adrenal tumor classification
Beginning in 2014, our group prospectively assessed the utility of intraoperative ICG fluorescence imaging in endocrine surgical procedures.10,15,16 By 2018, our findings indicated that adrenal neoplasms display differential fluorescence characteristics that correspond to their histopathologic origin. 17 In our research, 74% of adrenal tumors demonstrated hyperfluorescence relative to the surrounding retroperitoneal tissues, whereas 26% exhibited minimal or absent fluorescence. These findings support the presence of distinct ICG fluorescence patterns according to histological origin, particularly between cortical and medullary tumors. On multivariate analysis, adrenocortical origin emerged as the sole independent predictor of hyperfluorescence following ICG administration. Hyperfluorescence was observed in 95% of adrenocortical tumors, compared with 33% of medullary tumors and 50% of tumors arising from other tissue origins. 14
Consistent with our findings, we have previously reported that ICG fluorescence demonstrates greater utility in adrenocortical tumors, which characteristically exhibit hyperfluorescence relative to the surrounding retroperitoneal tissues. 10 Notably, we demonstrated that the majority of pheochromocytomas and malignant adrenal tumors do not exhibit fluorescence following ICG administration. In contrast, tumors of medullary origin, particularly pheochromocytomas, tend to exhibit hypo- or non-fluorescent patterns, thereby limiting the discriminatory value of ICG imaging in these lesions. 17 The hypofluorescent phenotype of pheochromocytomas has been consistently described in prior series and has been hypothesized to reflect reduced expression of bilitranslocase, a membrane transport protein implicated in ICG cellular uptake.18,19 Accordingly, ICG fluorescence imaging has demonstrated limited utility in pheochromocytomas and tumors of nonadrenocortical origin. An important exception is cortical-sparing adrenalectomy for pheochromocytoma, in which ICG facilitates clear delineation between hyperfluorescent viable cortical tissue and the nonfluorescent tumor. Furthermore, following excision of the adrenal mass, administration of an additional dose of ICG allows confirmation of adequate perfusion of the residual adrenal cortex. 17 In our experience, ICG fluorescence proved particularly useful in guiding cortical-sparing adrenalectomy when the tumor penetrated the healthy adrenal cortex and consequently appeared hypofluorescent. The normal adrenal cortex consistently demonstrated hyperfluorescence. In cases of cortical penetration, the distinct contrast between the nonfluorescent tumor and the hyperfluorescent residual cortex enabled clear identification of the optimal dissection plane. Conversely, when cortical penetration was absent, the entire adrenal mass exhibited heterogeneous fluorescence without a clearly distinguishable dissection line. Overall, our experience with ICG fluorescence has been highly favorable. Accordingly, as part of our ongoing research and surgical training initiatives, ICG imaging has been integrated into our standard robotic adrenalectomy practice (Figs. 1–4).
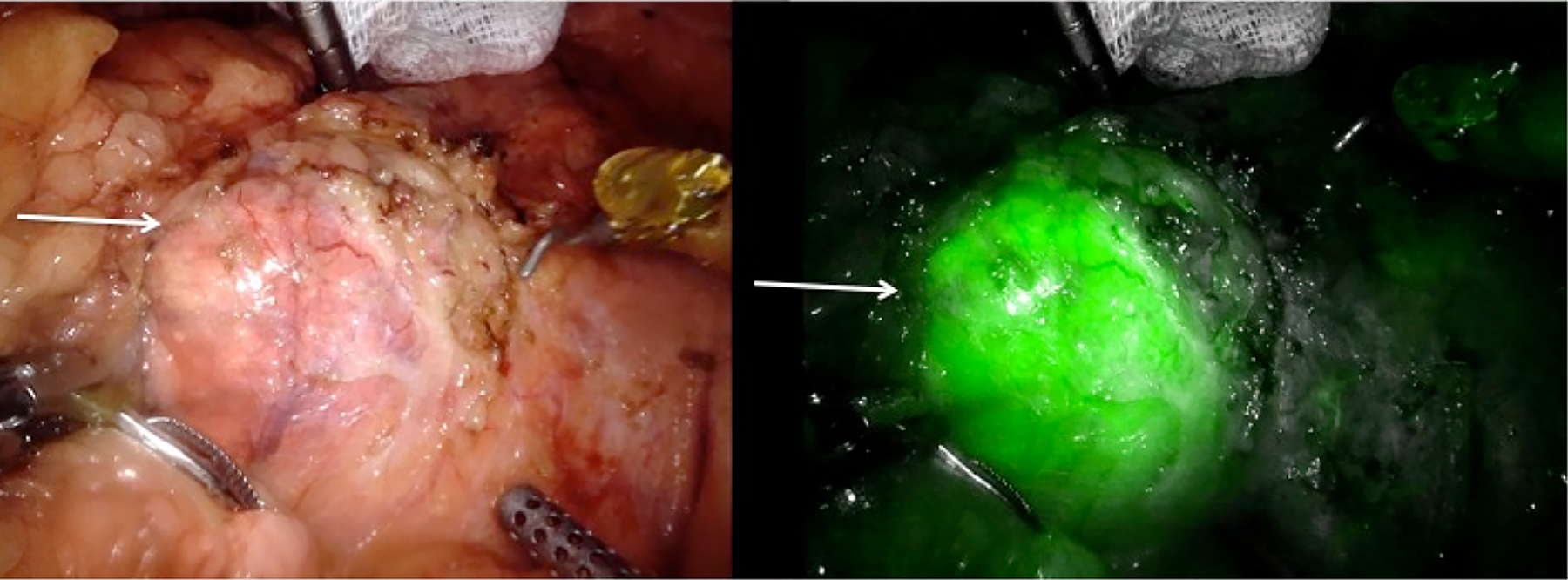
Hyperfluorescent pattern of ICG uptake in an adrenocortical tumor (arrow). ICG, indocyanine green.
ICG use for PA
PA or cortical-sparing adrenalectomy has been described as a strategy to avoid lifelong steroid supplementation and adrenal insufficiency for patients with or at risk of bilateral adrenal tumors. Tumor location within the adrenal gland and leaving enough remnant tissue with adequate perfusion represent the technical challenges of this surgical procedure. ICG fluorescence has found a role in improving this technique and the subsequent patient outcomes. Specifically, ICG provides real-time visual information regarding tissue perfusion and adrenal veins, enabling a more accurate delineation of adrenal tumor borders and preserving healthy cortical tissue.14,20 This allows for precise tumor resection while minimizing damage to the surrounding functional adrenal cortex. 12
Some of the published experiences include the Bǎlescu et al. series of minimally invasive PA in 2019, in which a subgroup of 3 patients underwent PA with ICG, and laparoscopic ultrasound was used for adrenal transection, showing it to be a safe procedure and recommending a preservation of at least 20% of the initial adrenal gland to maintain cortical function. 21 In the same year, Lerchenberger et al. published another small series of patients who underwent bilateral PA with ICG-fluorescence guidance for bilateral tumors. These authors found that ICG fluorescence signal after adrenal gland partial resection correlated with postoperative adrenal function, although the specifics of tissue remnant volume were not detailed. 22 The largest experience published on PA with ICG use is the study of Juan Manuel et al. in 2024. These authors reported a series of 7 patients in which they explored the use of ICG fluorescence imaging first to decide on performing PA based on primary tumor location within the adrenal gland and later to assess the remnant perfusion and correlation with postoperative adrenal function. The findings proved ICG’s utility to determine the feasibility of PA based on tumor location and to predict adrenal function when a well-vascularized remnant was left in situ and observed through ICG fluorescence imaging. 23
Although PA is not a consistent procedure during adrenal surgery, there is a need for future high-quality studies on this topic for a more evidence-based recommendation on ICG use for this purpose.
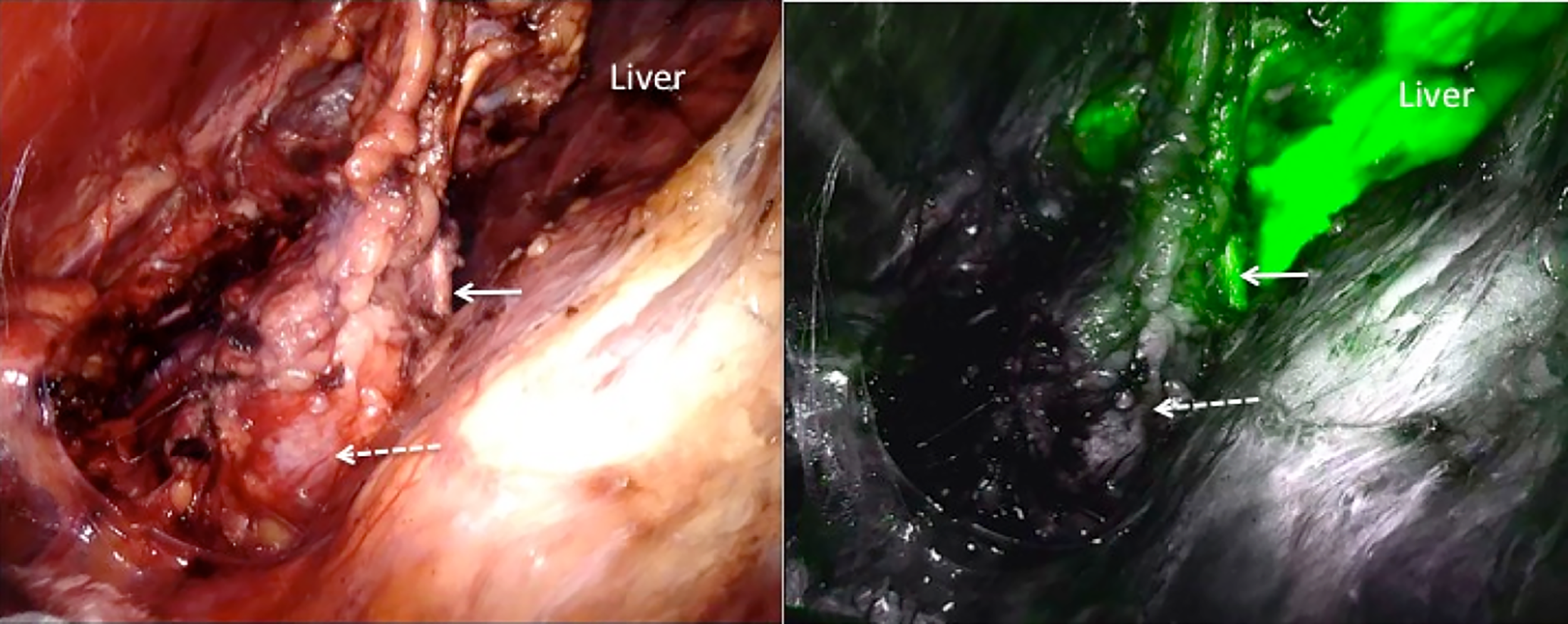
Hypofluorescent pattern of ICG uptake in a right-sided pheochromocytoma approached through a posterior approach. The solid arrow shows the normal adrenocortical tissue, and the dotted arrow shows the nonfluorescent pheochromocytoma portion of the lesion. ICG, indocyanine green.
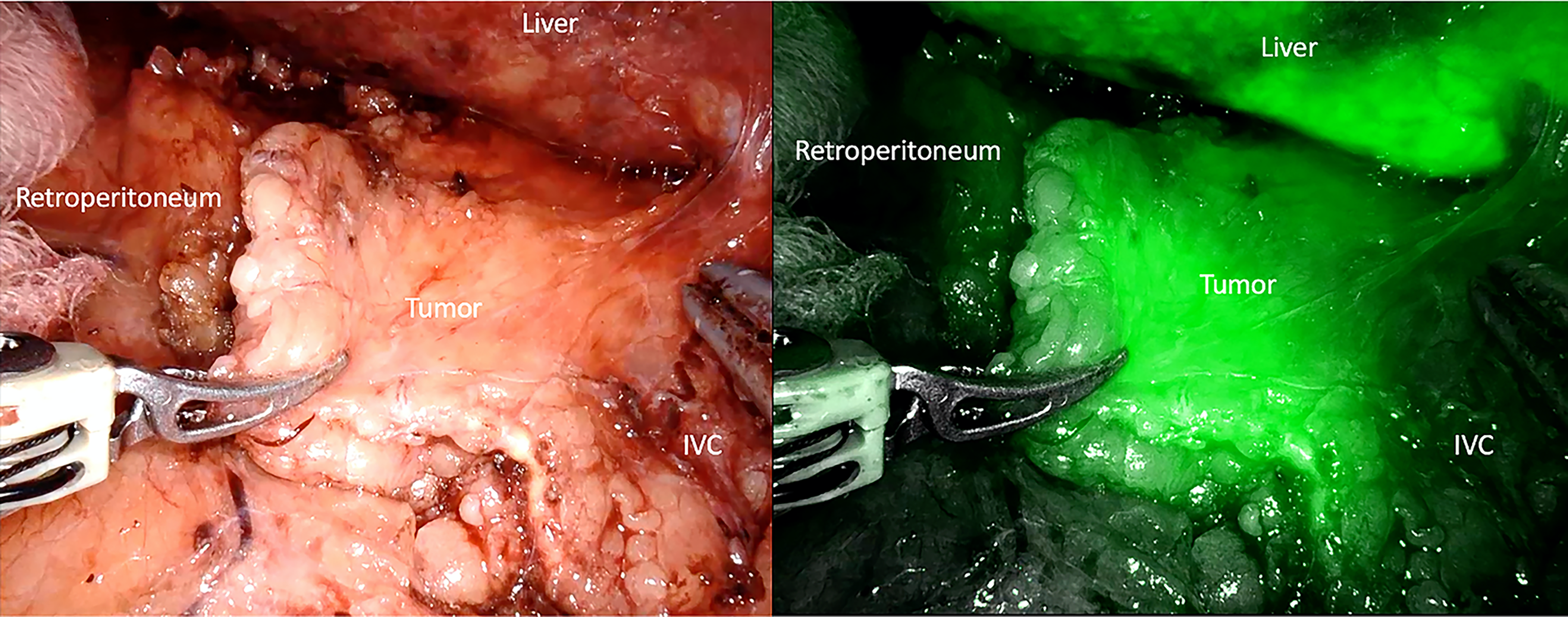
Intraoperative and ICG images of a right-sided adrenocortical tumor showing increased fluorescence compared with the surrounding tissues. ICG, indocyanine green; IVC, inferior vena cava.
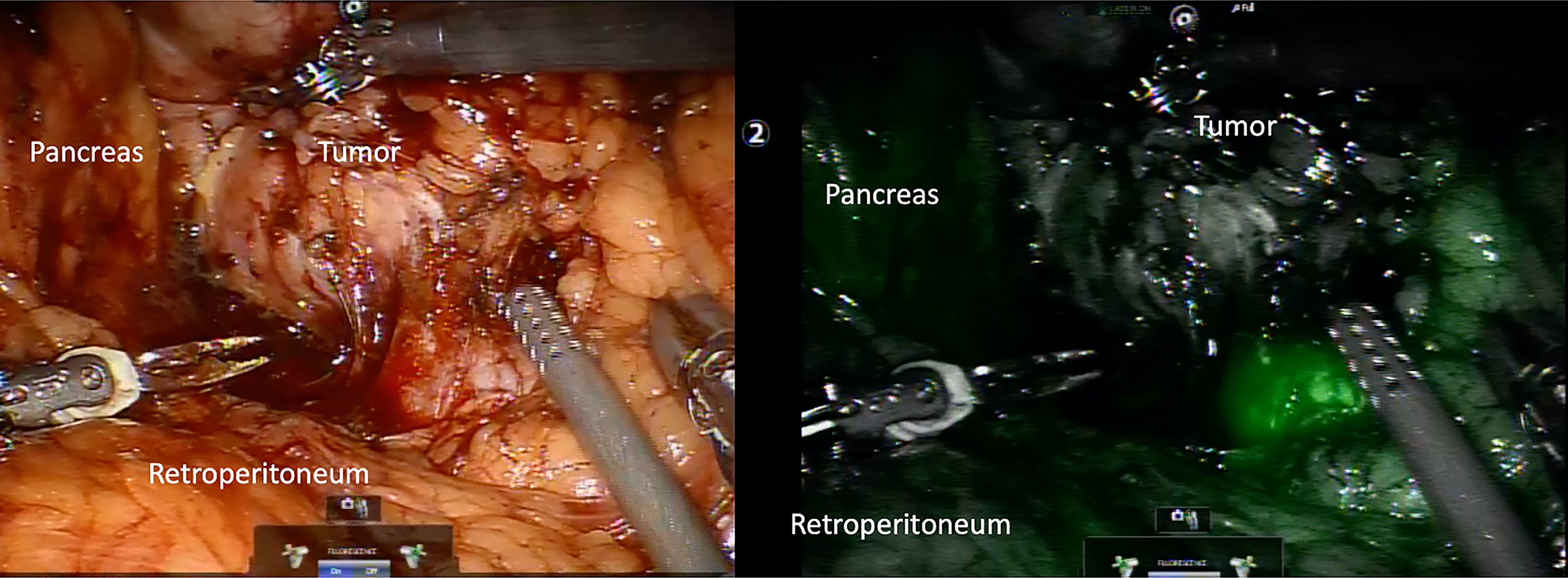
ICG fluorescence pattern in a lung cancer metastasis involving the left adrenal gland. Note the nonfluorescence compared with the surrounding tissues. ICG, indocyanine green.
ICG use for lymph node dissection in adrenalectomy
Adrenocortical carcinoma (ACC) is an exceptionally rare and aggressive endocrine malignancy, often presenting with a poor prognosis due to its propensity for local invasion and distant metastasis. 24 Historically, complete surgical resection is considered the only potentially curative treatment for localized ACC, with lymphadenectomy playing a crucial, yet not fully elucidated, role in both staging and potentially improving survival outcomes. 25 To increase the complexity of the surgical treatment of ACC, lymphatic drainage of the adrenal gland is considered to have moderate variability. Hence, there is a potential role for intraoperative imaging technologies, such as ICG fluorescence imaging, to ease this part of the surgical treatment. The literature on this matter is scarce; probably this is mainly due to the aberrant idea of injecting the primary adrenal tumor for lymph node mapping with the risk of rupturing the tumor, which increases the risk of local recurrence. In 2023, Baldari et al. published their experience on ICG use for lymphadenectomy for ACC patients. Interestingly, these authors propose the injection of 12.5 mg of ICG under ultrasound guidance between the cortex and medulla of an ipsilateral inguinal lymph node to map the retroperitoneal lymph nodes. 26 Further research to deepen this topic is still necessary, and it is a current opportunity area for ICG use in research on adrenal tumors.
In summary, ICG fluorescence imaging represents a valuable adjunct in adrenal surgery, providing real-time visualization of adrenal anatomy, vascular structures, and tissue perfusion. Its use facilitates gland identification, supports precise tumor localization, and enhances the safety and feasibility of cortical-sparing adrenalectomy by enabling preservation of functional adrenal tissue. Additionally, differential fluorescence patterns may assist in intraoperative tumor characterization and guide surgical decision-making. Although current evidence supports its safety and technical benefits, further prospective studies are needed to define standardized protocols and clarify its impact on long-term functional and oncologic outcomes.
Authors’ Contributions
Conceptualization: R.H.P.S., B.B., and D.A. Writing original draft preparation: R.H.P.S., B.B., and D.A. Writing, review and editing: R.H.P.S., B.B., and D.A. Supervision: R.H.P.S. Project Administration: R.H.P.S. and D.A. All authors have read and agreed to the published version of the manuscript.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.