
Abstract
Background:
Magnetic sphincter augmentation (MSA) using the LINX device is a minimally invasive treatment for gastroesophageal reflux disease (GERD). With increasing rates of sleeve gastrectomy and associated postoperative GERD, evaluating MSA outcomes in both post-bariatric and de novo patients is clinically relevant. Data from the Middle East remain limited.
Methods:
This retrospective cohort study included 30 consecutive patients who underwent LINX placement for GERD at King Abdulaziz University Hospital between 2018 and 2024. Briefly, 20 patients (66.7%) had prior sleeve gastrectomy, while 10 patients (33.3%) were de novo cases. Primary outcomes were improvement in GERD–Health-Related Quality of Life (GERD-HRQL) scores and proton pump inhibitor (PPI) discontinuation. Secondary outcomes included perioperative complications and comparison between patient groups.
Results:
The mean age was 42.8 years, and the mean body mass index was 26.9 kg/m2. Hiatal hernia was present in 76.7% of patients (23/30). The mean operative time was 65 minutes, with a median LINX size of 15 beads. Early postoperative dysphagia occurred in 23.3% (7/30), with 10% (3/30) requiring endoscopic dilation (two postsleeve and one de novo). One postsleeve patient (3.3%) required laparoscopic device removal for migration after failed dilation; removal was technically challenging but uncomplicated, with sustained GERD improvement, likely related to hiatal scarring. Mean GERD-HRQL scores improved from 27.2 to 7.1 (P < .001), with 76.7% achieving a ≥50% reduction. Complete PPI cessation occurred in 66.7% (20/30), and 86.7% (26/30) achieved at least a 50% dose reduction. Outcomes were comparable between postsleeve and de novo patients.
Conclusions:
MSA appears safe and effective for GERD management in this Middle Eastern cohort, with outcomes comparable to international reports. Similar results in postsleeve gastrectomy and de novo patients support broader applicability. This series provides valuable regional outcome data.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) affects approximately 10%–20% of adults worldwide,1–4 with a rising prevalence in the Middle East that parallels increasing obesity rates and expanding bariatric surgery volumes.5,6 Sleeve gastrectomy, now the most commonly performed bariatric procedure in the region, is associated with postoperative GERD rates ranging from 20% to 60%,7–9 posing a significant clinical challenge.
Although proton pump inhibitors (PPIs) are commonly used as first-line therapy, many patients report incomplete symptom control. 7 Conventional fundoplication is effective in managing GERD but is associated with adverse effects such as gas-bloat syndrome and dysphagia.8,10 Furthermore, altered gastric anatomy following sleeve gastrectomy or gastric bypass often precludes standard fundoplication. Hiatal hernia repair alone has shown limited efficacy in resolving GERD symptoms or esophagitis.8,9
Magnetic sphincter augmentation (MSA) using the LINX device, approved by the U.S. Food and Drug Administration in 2012, reinforces lower esophageal sphincter (LES) function through a ring of magnetic titanium beads. 11 This approach preserves normal anatomy while reducing reflux, offering potential advantages over long-term medical therapy and fundoplication. Despite growing international evidence supporting its use, data from the Middle East remain limited, particularly in regions with a high prevalence of bariatric surgery.
We report outcomes from 30 consecutive LINX procedures performed at King Abdulaziz University Hospital in Jeddah, Saudi Arabia, including patients with prior sleeve gastrectomy (66.7%) and de novo GERD (33.3%). This series may represent the first published Middle Eastern experience with MSA, helping to address an important gap in regional GERD management.
Materials and Methods
Study design and patient population
This retrospective cohort study included consecutive patients who underwent LINX placement for GERD at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, between 2018 and 2024. The study protocol was approved by the King Abdulaziz University Research Ethics Committee. Given the retrospective design and anonymized data analysis, the committee granted a waiver of informed consent, in accordance with the Declaration of Helsinki.
The inclusion criteria were (1) age of ≥18 years, (2) confirmed GERD diagnosis based on endoscopy or pH monitoring, and (3) minimum follow-up of 18 months (median follow-up, 28 months). The exclusion criteria included incomplete documentation or non-GERD indications for MSA. All patients underwent preoperative esophageal manometry, confirming reduced gastroesophageal junction pressure with at least 70% of esophageal contractions within the normal range.
Patient selection criteria
Appropriate candidate selection is critical for successful LINX implantation. The device reinforces LES function through magnetic bead attraction, allowing food to pass while limiting reflux. Potential adverse effects include transient dysphagia. All patients underwent a comprehensive preoperative evaluation, which included barium swallow to quantify reflux severity and exclude gastric torsion (a relative contraindication), upper endoscopy to assess esophagitis, hiatal hernia, and Barrett esophagus, esophageal manometry to confirm adequate peristalsis, and ambulatory pH monitoring in most patients to document pathological acid exposure. Patients with elevated body mass index (BMI) were more likely to undergo gastric bypass rather than LINX, explaining the relatively normal BMI distribution in this cohort.
Data collection
Data were extracted from electronic medical records using standardized forms and transferred to Microsoft Excel for analysis in SPSS Statistics version 21 (IBM Corp., Armonk, NY). Preoperative variables included age, BMI, respiratory symptoms, esophagitis, Barrett esophagus, type 1 hiatal hernia, prior sleeve gastrectomy, prior fundoplication, LES pressure, and GERD-HRQL scores. Operative variables included LINX device size (Ethicon, Johnson & Johnson, Somerville, NJ) and operative duration. Postoperative GERD-HRQL scores were collected via questionnaire sheets during scheduled clinic visits at regular intervals. Postoperative variables comprised GERD-HRQL scores, PPI usage, complications (early dysphagia [<3 months], persistent dysphagia [≥3 months], endoscopic dilation, device removal), and hospital length of stay.
Surgical technique
A standard five-port laparoscopy approach was used. Following circumferential esophageal mobilization at the hiatus with preservation of the vagal nerves (Fig. 1), intraabdominal esophageal length was confirmed at 4–6 cm. Posterior crural approximation was performed using nonabsorbable sutures. A retroesophageal window was then created between the posterior vagus and the esophageal wall at the gastroesophageal junction (Fig. 2).
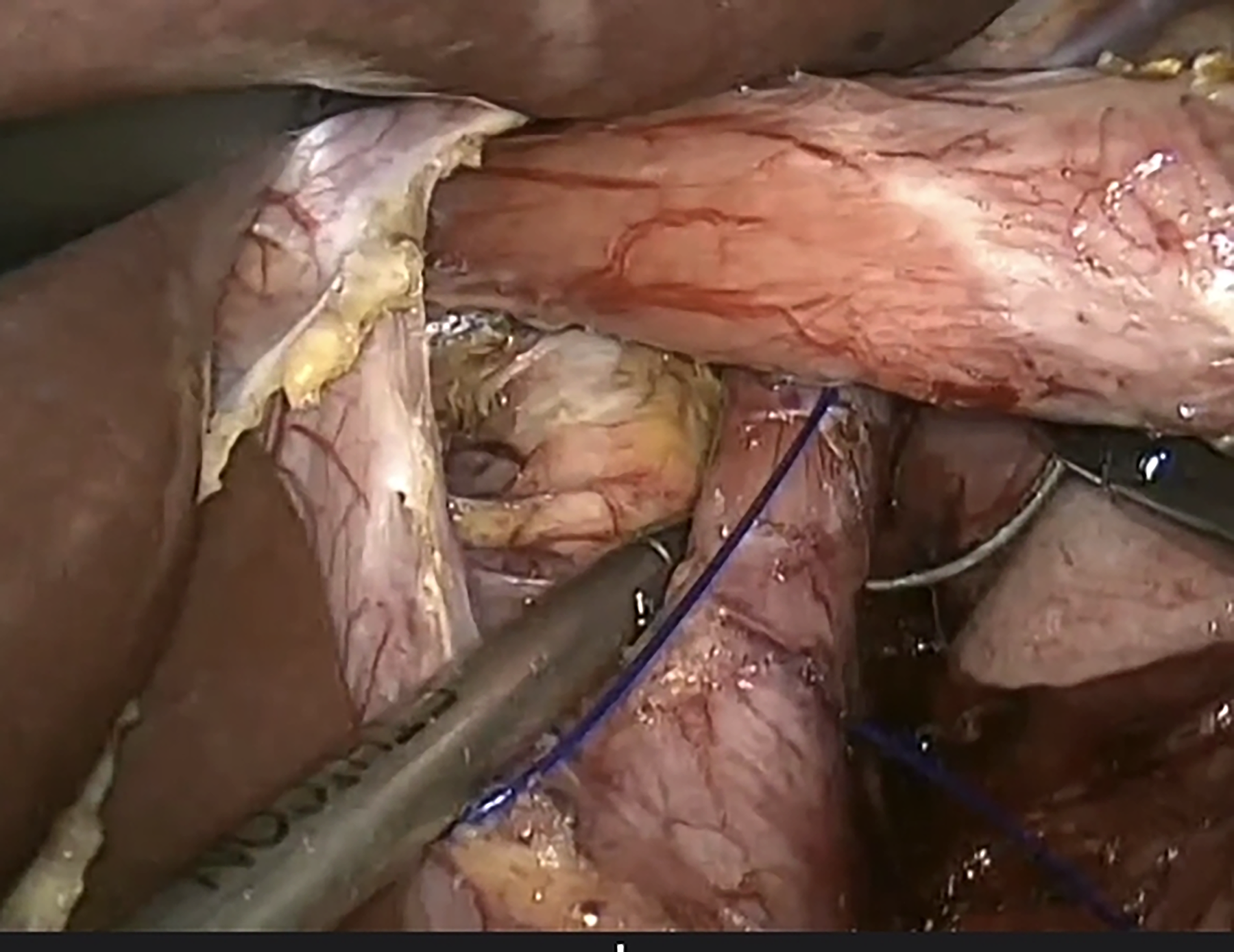
Hiatal dissection demonstrating circumferential esophageal mobilization with a minimum intraabdominal length of 4 cm.
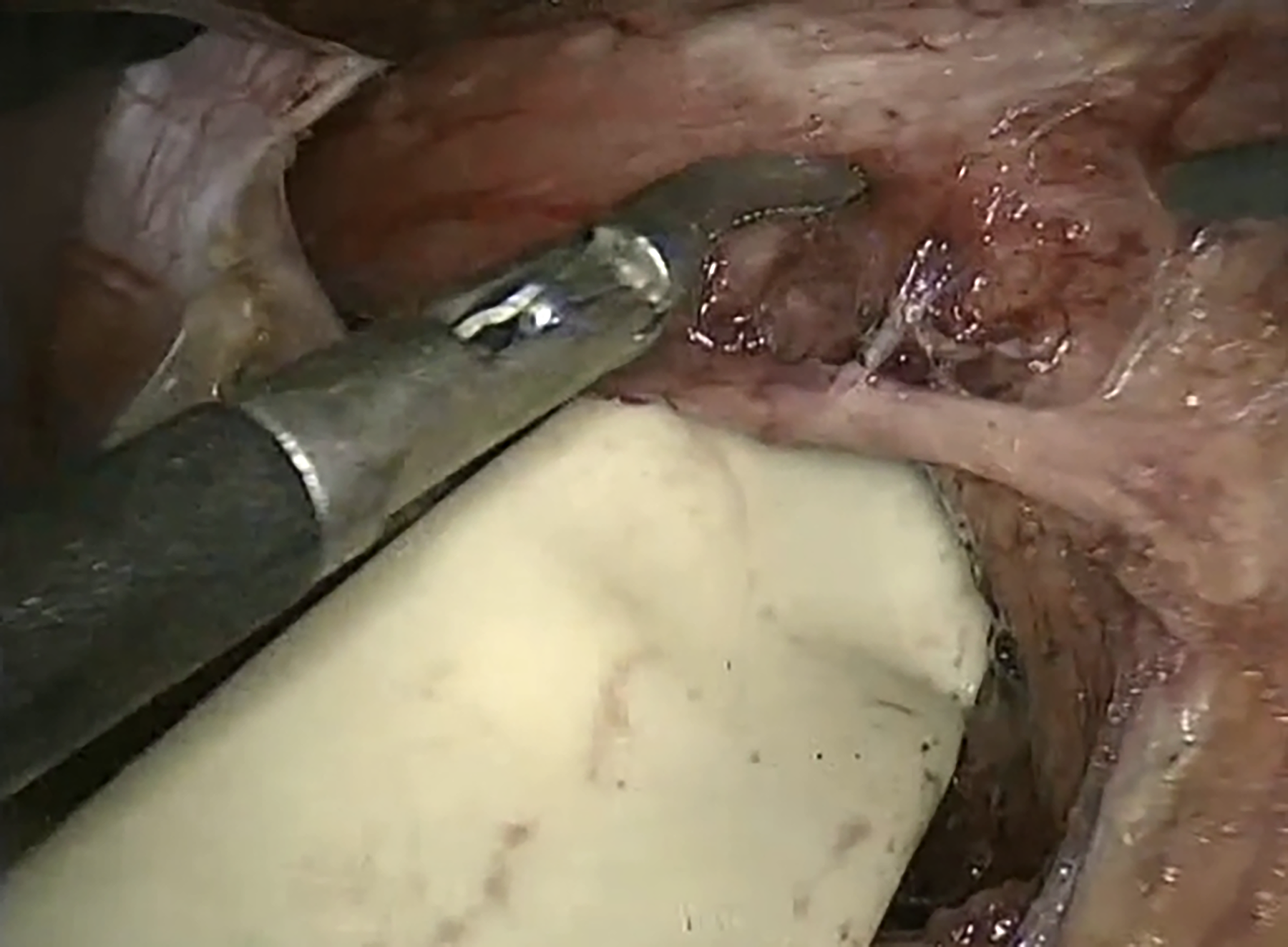
Creation of a retroesophageal window between the posterior vagus nerve and the esophageal wall at the gastroesophageal junction.
LES sizing was performed using a proprietary sizer under minimal tension (Fig. 3). Device size selection involved adding two beads to the closed pop-off measurement for de novo patients and three beads for postsleeve gastrectomy patients. The LINX device (13–16 beads) was positioned between the esophagus and posterior vagus (Fig. 4), secured magnetically, and endoscopic confirmation of luminal patency was performed.
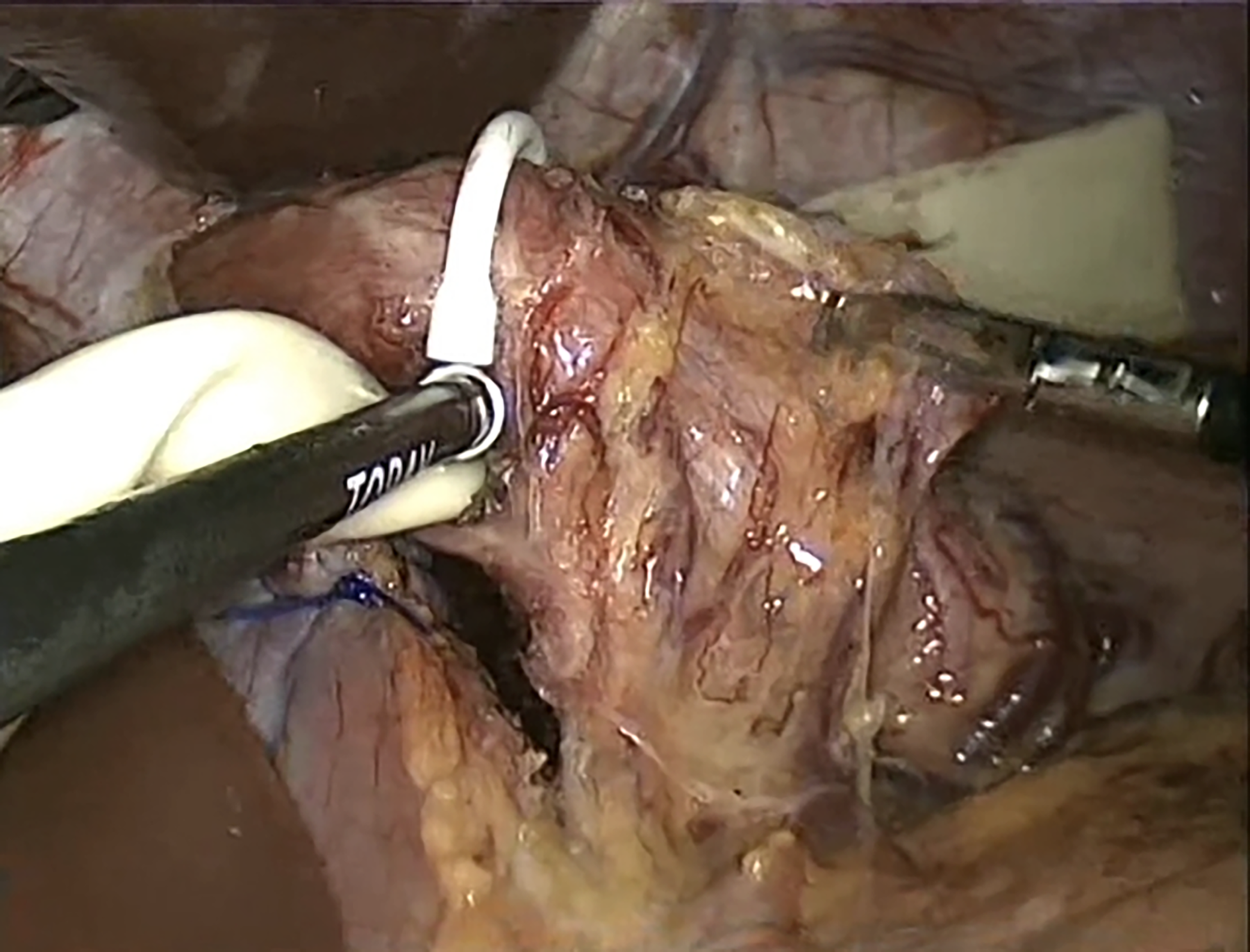
Proprietary sizing instrument used to determine appropriate LINX ring dimensions.
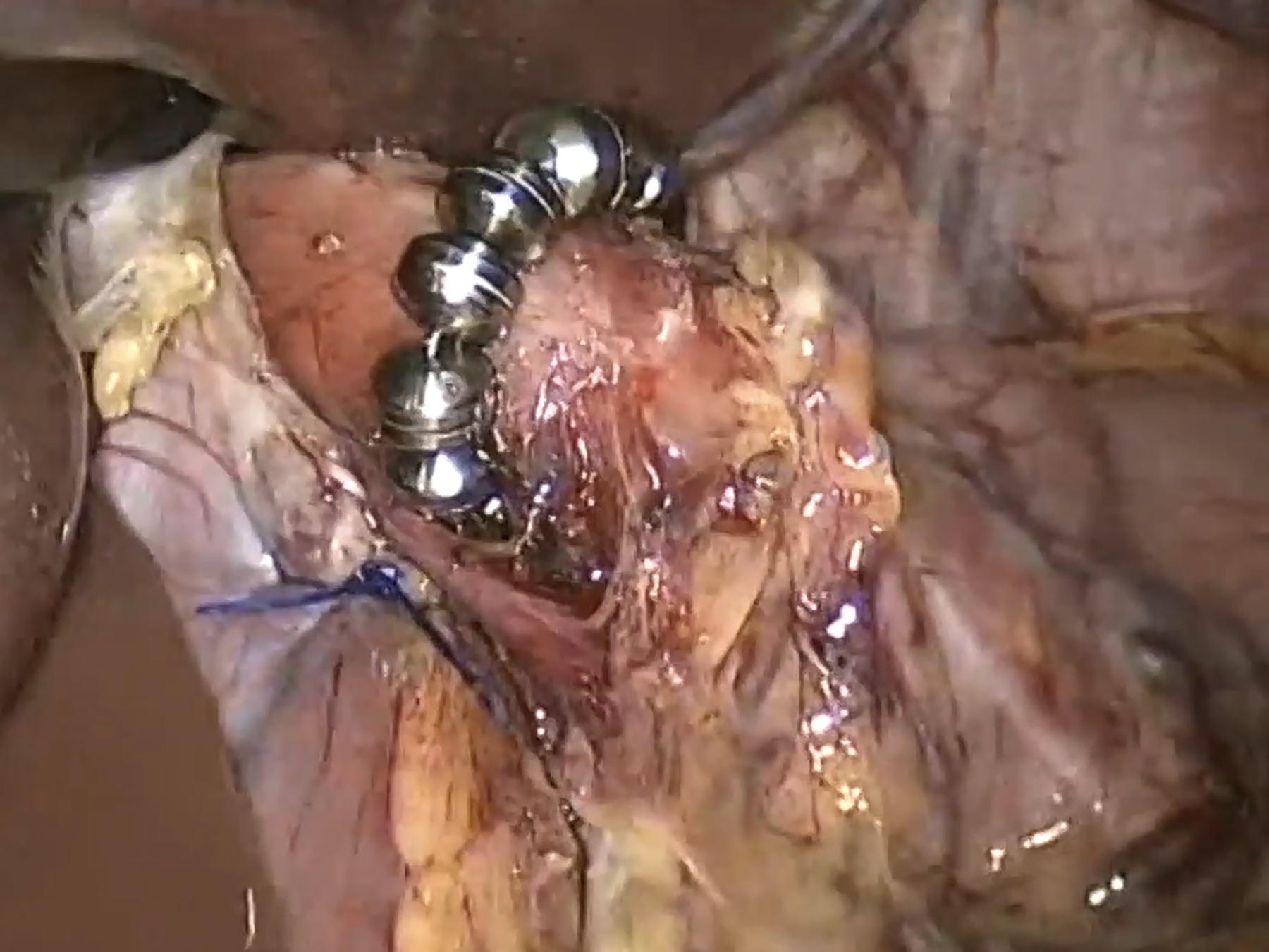
Final LINX device positioned between the esophagus and posterior vagus nerve.
Postoperative management included advancement from a liquid diet as tolerated to a soft diet for 2 weeks, followed by a regular diet. Patients received PPI therapy (40 mg daily) for 1 month. Supplementary Video S1 illustrates the detailed operative technique.
Outcome measures
Primary outcomes were defined as a ≥50% reduction in GERD-HRQL scores from baseline and complete PPI discontinuation. Secondary outcomes included ≥50% PPI dose reduction, overall complication rates, and associations between outcomes and patient-related factors.
Statistical analysis
Categorical variables are presented as frequencies and percentages with 95% confidence intervals (CIs). Continuous variables are reported as means ± standard deviations or medians with interquartile ranges, depending on distribution normality. Paired t-tests, chi-squared or Fisher’s exact tests, and logistic regression analyses were performed, with statistical significance defined as P < .05.
Results
Patient demographics
Table 1 summarizes baseline characteristics. The mean age was 42.8 ± 10.2 years, with a mean BMI of 26.9 ± 4.5 kg/m2. Type 1 hiatal hernia was present in 76.7% of patients (23/30; 95% CI, 59.1%–88.2%). Prior sleeve gastrectomy was reported in 66.7% (20/30; 95% CI, 48.8%–80.8%), with the remaining 33.3% (10/30; 95% CI, 19.2%–51.2%) representing de novo GERD cases. Esophagitis was documented in 73.3% (22/30; 95% CI, 55.6%–85.8%), and respiratory symptoms occurred in 23.3% (7/30; 95% CI, 11.8%–40.9%). No cases of Barrett esophagus were identified. Mean preoperative LES pressure was 8.5 ± 2.3 mm Hg. The mean baseline GERD-HRQL score was 27.2 ± 8.1. Median follow-up was 28 months (Interquartile Range: 22–36).
Baseline Patient Characteristics (n = 30)
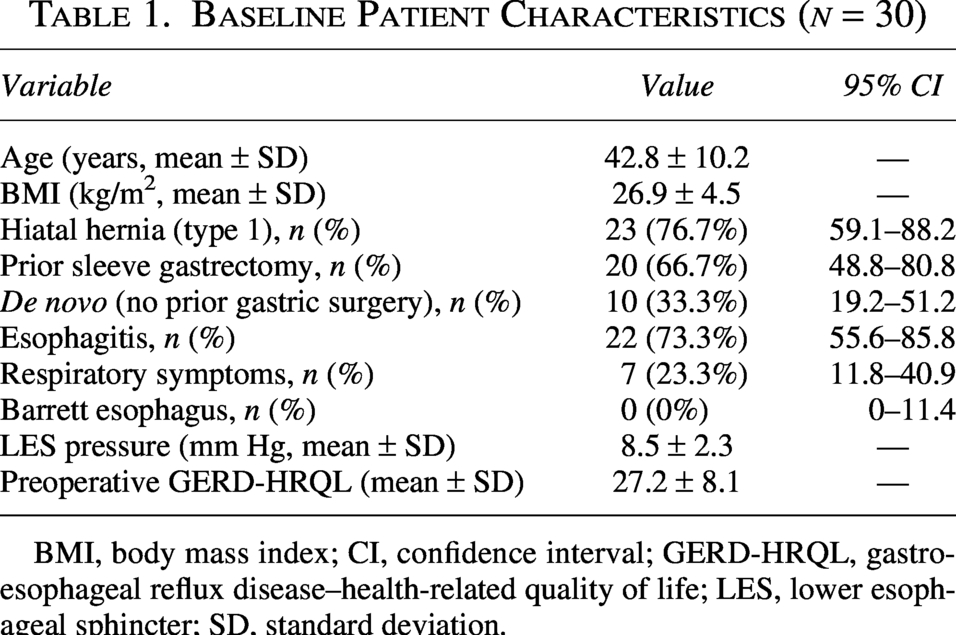
BMI, body mass index; CI, confidence interval; GERD-HRQL, gastroesophageal reflux disease–health-related quality of life; LES, lower esophageal sphincter; SD, standard deviation.
Operative and postoperative outcomes
Table 2 summarizes operative details and postoperative complications. The median LINX device size was 15 beads (range: 13–16), with a mean operative time of 65 ± 15 minutes and a mean hospital length of stay of 2 ± 1 days. Early postoperative dysphagia (<3 months) occurred in 7 patients (23.3%), of whom 3 (10%) required endoscopic dilation—2 in the postsleeve gastrectomy group and 1 in the de novo group.
Operative and Postoperative Outcomes (n = 30)
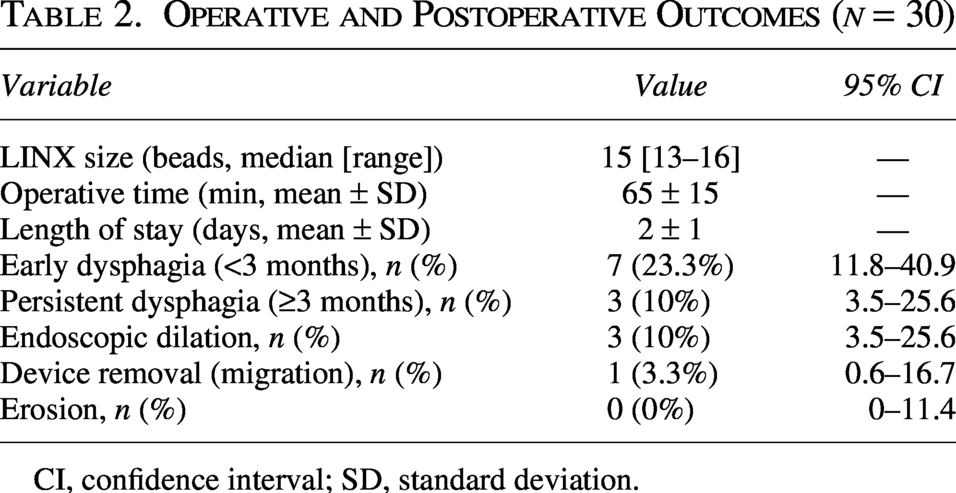
CI, confidence interval; SD, standard deviation.
One postsleeve gastrectomy patient (3.3%) ultimately required laparoscopic device removal at 3 months due to persistent dysphagia and distal migration of the device (approximately 4 cm into the sleeved stomach) despite attempted endoscopic dilation. During initial implantation, the posterior vagus nerve could not be identified, resulting in placement of a size-16 LINX device between the esophagus and the anterior vagus nerve. Removal proved technically challenging, primarily owing to dense adhesions encasing the device. No additional antireflux procedure (e.g., conversion to Roux-en-Y gastric bypass) was undertaken, as the patient declined further surgical intervention for GERD. At a 6-month follow-up after explantation, dysphagia had substantially improved, with only mild residual reflux symptoms controlled by 20 mg of omeprazole every other day. Notably, this patient continued to experience meaningful improvement in GERD symptoms postexplantation consistent with residual antireflux effects from hiatal scarring and fibrosis, as previously reported. 10
The other 2 patients who underwent dilation (1 requiring two sessions and 1 a single session) achieved complete resolution of dysphagia and became fully PPI independent. No cases of device erosion were observed.
Efficacy outcomes
GERD-HRQL scores improved significantly from baseline, decreasing from a mean of 27.2 ± 8.1 to 7.1 ± 4.8 (P < .001), with a ≥50% reduction achieved in 76.7% of patients (23/30). Table 3 summarizes pre- and postoperative GERD-HRQL total and component scores, demonstrating substantial improvement across all domains. Figure 5 illustrates GERD-HRQL score improvement over the 24-month follow-up period. Complete PPI discontinuation was achieved in 66.7% of patients (20/30), while 86.7% (26/30) achieved at least 50% dose reduction, with PPI discontinuation counted as a 100% reduction. All patients underwent follow-up endoscopy at 1 year; 28 of 30 patients (93.3%) demonstrated improvement or resolution of esophagitis, while 2 patients experienced worsening from Los Angeles grade A to grade B esophagitis.
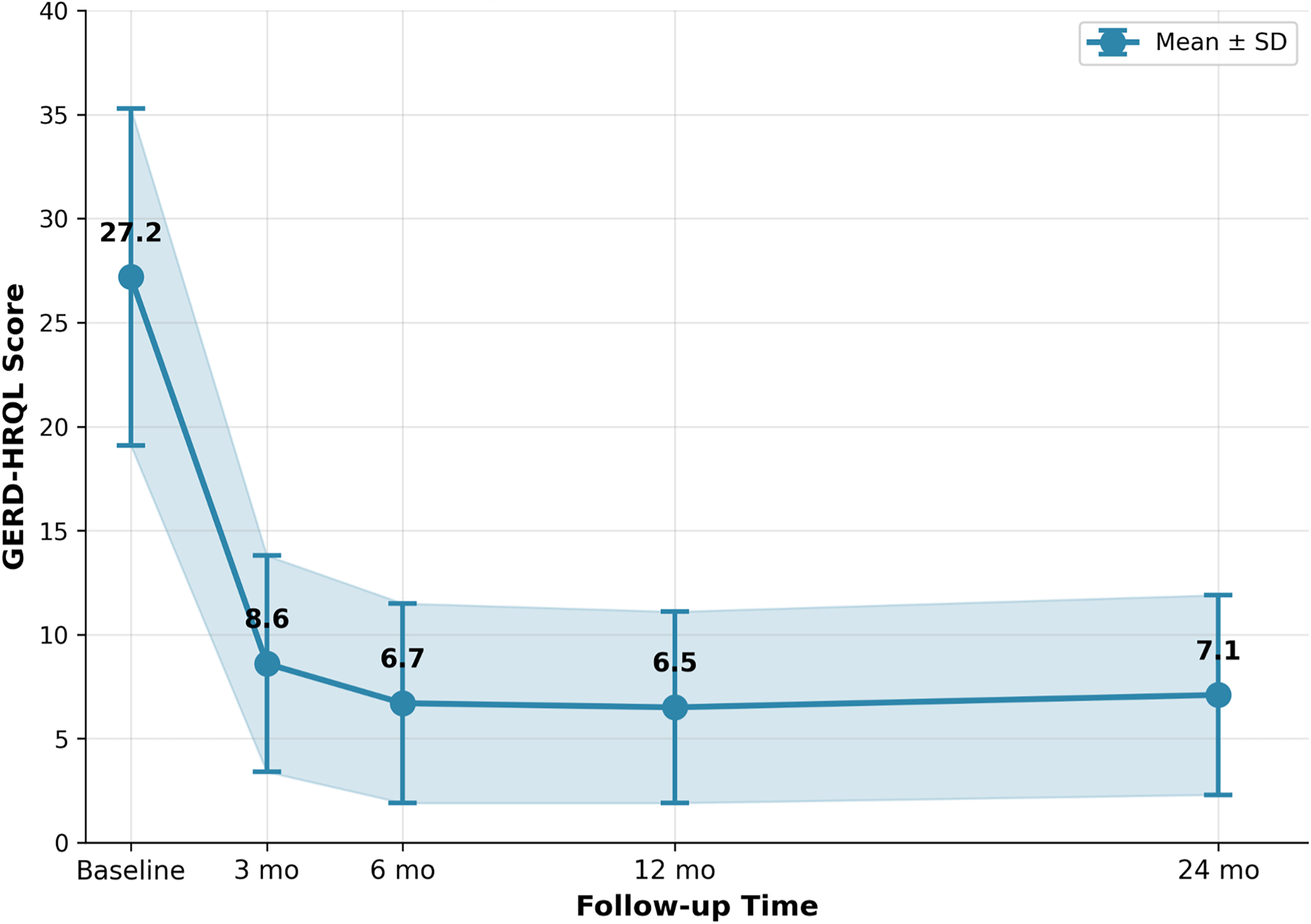
GERD-HRQL scores following magnetic sphincter augmentation over 24-month follow-up (n = 30). Data are shown as mean ± standard deviation. *Including the patient who had device removal. GERD-HRQL, gastroesophageal reflux disease–health-related quality of life.
Preoperative and Postoperative Gastroesophageal Reflux Disease–Health-Related Quality of Life Scores (n = 30)
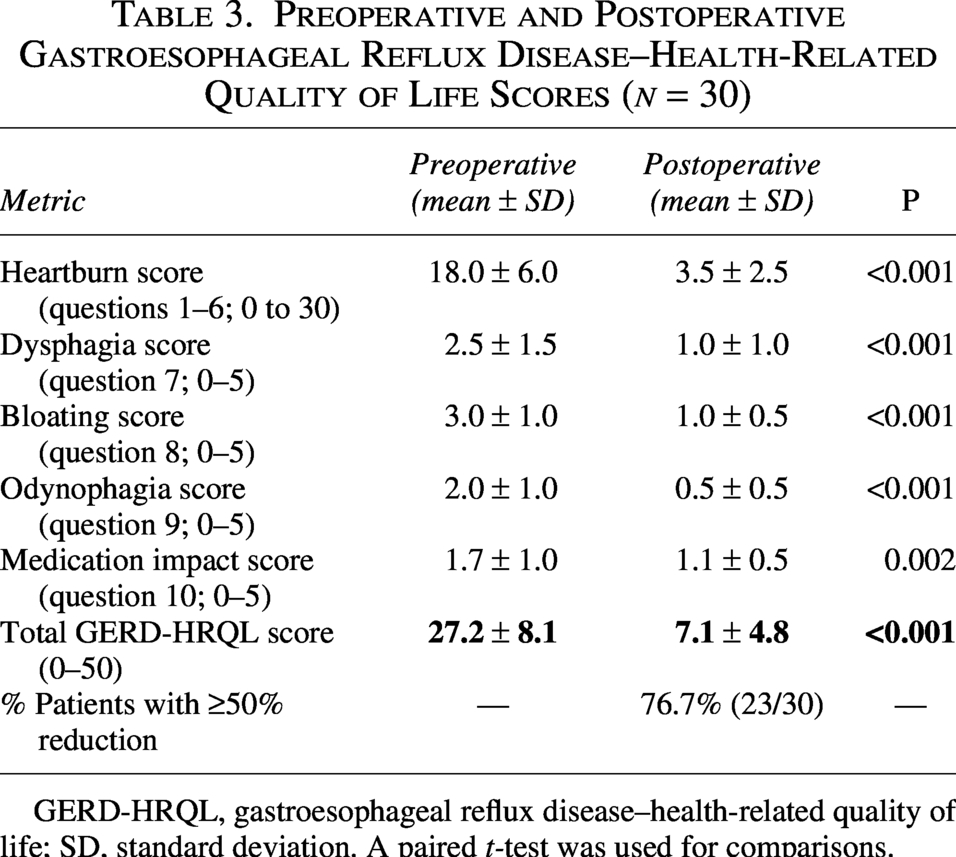
GERD-HRQL, gastroesophageal reflux disease–health-related quality of life; SD, standard deviation. A paired t-test was used for comparisons.
Subgroup analysis
No statistically significant associations were observed between prior sleeve gastrectomy and early dysphagia (P = .71) or between the presence of hiatal hernia and overall complications (Table 4). Logistic regression analysis did not identify significant predictors for persistent dysphagia or device removal (all P > .05). BMI was similar between patients with prior sleeve gastrectomy (25.8 ± 5.0 kg/m2) and de novo patients (25.2 ± 4.7 kg/m2; P = .68). These findings suggest comparable outcomes between postsleeve and de novo GERD patients.
Comparison of Outcomes between Patients with Prior Sleeve Gastrectomy and de Novo Patients (no Prior Gastric Surgery)
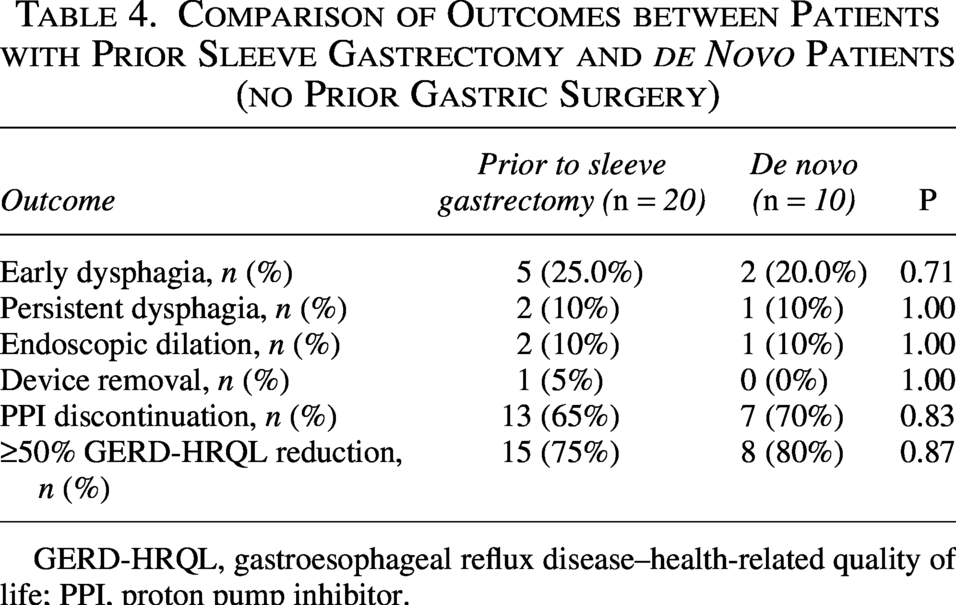
GERD-HRQL, gastroesophageal reflux disease–health-related quality of life; PPI, proton pump inhibitor.
Discussion
This series may represent the first published experience with MSA from the Middle East, demonstrating safety and efficacy comparable to international benchmarks. In a cohort comprising 66.7% postsleeve gastrectomy patients and 33.3% de novo cases, with a 76.7% prevalence of hiatal hernia, MSA resulted in significant improvement in GERD-HRQL scores (27.2–7.1; P < .001) and complete PPI discontinuation in 66.7% of patients.
The observed complication profile aligns with published literature. Early dysphagia occurred in 23.3% of patients, lower than the 68% reported immediately postoperatively in the Ganz et al. pivotal trial, which declined to 11% at 1 year. 8 Persistent dysphagia (10%) and the need for endoscopic dilation (10%) compare favorably with Lipham et al.’s 1000-patient registry (5.6% dilation) and the meta-analysis by Valinoti et al., including 4663 patients (5.6% dilation, 4% device removal).10,12 Device removal in our series (3.3%) is consistent with these benchmarks, and the absence of erosion aligns with reported rates of 0.1%–1%.12,13 As reported by Buniak et al. in a series of 8 patients requiring MSA device removal, GERD symptoms often remained improved or resolved postexplantation in 62% of cases due to residual fibrosis/scar tissue at the explantation site restricting LES relaxation and preventing reflux. 10
Efficacy outcomes in our cohort are consistent with global standards. GERD-HRQL scores improved from 27.2 to 7.1, paralleling the sustained results reported by Bonavina et al. (24–2 at median follow-up of 6–12 years).14,15 Complete PPI discontinuation was achieved in 66.7% of patients, slightly lower than the 83%–85% reported by Ganz et al. and 85% by Bonavina et al.8,12 but still clinically significant. Moreover, 86.7% of patients attained a ≥50% reduction in PPI dose (Table 5). These findings support the durability and effectiveness of MSA for GERD management.
Comparison of Key Outcomes with the Published Literature

GERD-HRQL, gastroesophageal reflux disease–health-related quality of life; NR, not reported; PPI D/C, proton pump inhibitor discontinuation.
The 66.7% prevalence of prior sleeve gastrectomy in our cohort reflects regional bariatric surgery trends, where sleeve gastrectomy is the predominant procedure in the Middle East, 4 with 20%–60% of patients developing postoperative GERD.8,9,16 Cammarata et al. reviewed MSA outcomes in postsleeve patients and reported significant GERD-HRQL improvement, with only 25.3% of patients continuing PPI therapy. 16 Our subgroup analysis found no significant differences between postsleeve and de novo patients (Table 4), supporting the broad applicability of MSA across both populations.
Gastric bypass remains the standard surgical approach for postsleeve GERD. However, it carries distinct morbidities, including dumping syndrome, nutritional deficiencies (iron and vitamin B12), anastomotic leak risk, marginal ulcers, internal hernias, and weight regain, requiring lifelong supplementation. MSA offers several advantages, including preservation of normal anatomy, superior food tolerance (illustrated by one patient in our series who subsequently required bypass for weight gain post-LINX due to improved intake), fewer nutritional complications, and reversibility. Patient selection should carefully consider these factors in relation to individual goals and risk tolerance.
The observed 76.7% prevalence of hiatal hernia exceeds rates reported in typical Western series (50%–60%), 15 potentially reflecting regional anatomical variations, diagnostic practices, or referral bias. Low preoperative LES pressure (8.5 mm Hg) aligns with optimal MSA candidacy. 17 The absence of Barrett esophagus may reflect earlier intervention or demographic factors, warranting further investigation. 18
Operative efficiency in our series, with a mean operative time of 65 minutes and average hospital stay of 2 days, compares favorably with fundoplication,19,20 highlighting the minimally invasive advantages of MSA.
Limitations
The retrospective design introduces potential selection and information bias. The small sample size (n = 30) limits the statistical power of subgroup analyses and generalizability of findings. Variable follow-up duration (minimum 18 months, median of 28 months) and reliance on subjective outcome measures, without routine postoperative pH monitoring, represent recognized limitations in reflux surgery research. Prospective studies with larger cohorts, standardized protocols, and objective physiological testing would strengthen the evidence and clarify the impact of sleeve gastrectomy on MSA outcomes.
Conclusions
MSA is safe and effective for GERD management in this Middle Eastern cohort, with outcomes comparable to international benchmarks. Similar results between postsleeve gastrectomy and de novo patients support the broad clinical applicability of MSA. The high prevalence of bariatric-related GERD highlights the potential value of MSA in this growing patient population. As potentially the first published Middle Eastern MSA series, these findings provide baseline regional outcome data and support expanded MSA utilization for appropriately selected candidates.
Authors’ Contributions
A.M.: Conceptualization, investigation, and writing—original draft. M.A.: Conceptualization, methodology, data curation, formal analysis, writing—review and editing, and supervision. S.K., E.A., W.J., M.A., A.H., and A.K.: Investigation and writing—review and editing.
Statements and Declarations Ethical Considerations
The study protocol was approved by the King Abdulaziz University Research Ethics Committee. Given the retrospective design and anonymized data analysis, the committee granted a waiver of informed consent, in accordance with the Declaration of Helsinki. The King Abdulaziz University Research Ethics Committee approved the study.
Consent for Publication
Not applicable (no individual patient data, images, or videos identifying participants are included).
Footnotes
Consent to Participate
Not applicable (waiver of informed consent granted by the ethics committee due to retrospective nature).
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.