
Abstract
Background:
The umbilical port is routinely used for camera insertion and specimen retrieval in laparoscopic cholecystectomy (LC). However, the umbilicus is anatomically vulnerable and may be associated with an increased risk of surgical site infection (SSI) and port-site hernia (PSH), particularly in obese patients. We evaluated the clinical impact of avoiding an umbilical incision in obese patients undergoing LC.
Methods:
This single-center retrospective cohort study included 75 patients with a body mass index (BMI) ≥ 32 who underwent LC between April 2019 and November 2025. Patients were divided into an umbilical incision group (n = 46) and a nonumbilical incision group (n = 29). The primary endpoint was overall postoperative complications (Clavien–Dindo grade ≥ II) within 6 months. Absolute risk differences and corrected odds ratios (ORs) with 95% confidence intervals (CIs) were calculated.
Results:
Postoperative complications occurred in six patients (12.8%) in the umbilical incision group and in none (0%) in the nonumbilical incision group (P = .076). Although the difference did not reach statistical significance, all observed complications occurred in the umbilical incision group. The absolute risk difference was 13.0% (95% CI 3.3%–22.8%). After Haldane–Anscombe correction, the estimated OR for complications associated with the umbilical incision approach was 9.47 (95% CI 0.51–174.76). All complications were wound-related (four SSIs and two PSHs). Operative time, blood loss, and postoperative hospital stay were significantly lower in the nonumbilical incision group. All outcome measures consistently favored the nonumbilical approach.
Conclusions:
Although statistical significance was not reached, all wound-related complications occurred exclusively in the umbilical incision group. Avoiding an umbilical incision in obese patients undergoing LC may represent a clinically reasonable strategy associated with a potential reduction in wound-related morbidity. Larger prospective studies are warranted.
Keywords
Introduction
In laparoscopic cholecystectomy (LC), the umbilical port is routinely used for camera insertion and specimen retrieval. Although this technique is widely accepted as standard practice, the umbilicus is anatomically distinct from other abdominal wall sites. As a congenital scar with relatively weak fascial support and a recessed morphology, it is inherently susceptible to hernia formation and wound complications. Previous studies have demonstrated that the umbilical port is associated with a higher incidence of port-site hernia (PSH) compared with nonmidline extraction sites,1,2 and the presence of an umbilical Hasson trocar has been identified as an independent risk factor for trocar-site hernia development. 3 In addition, trocar-site hernias after LC occur predominantly at the umbilical port, particularly when larger trocars are used or the incision is extended. 1
Obesity is an established independent risk factor for wound complications, including surgical site infection (SSI) and incisional hernia. Meta-analyses of abdominal surgery have demonstrated that obesity significantly increases the risk of incisional hernia formation and postoperative SSI.4,5 Increased subcutaneous fat thickness, elevated intra-abdominal pressure, and impaired wound healing contribute to higher rates of infection and hernia formation in obese individuals. Moreover, once wound complications occur in obese patients, they are often more difficult to manage and may require prolonged treatment or additional surgical intervention.
Acute cholecystitis further increases perioperative risk. Large cohort studies have identified the severity of cholecystitis as an independent predictor of postoperative complications after LC.6,7 Therefore, obese patients undergoing LC—particularly in the setting of inflammation—may represent a population at heightened risk of wound-related morbidity. Despite these considerations, the umbilical incision remains the conventional extraction site even in obese patients. Given the anatomical vulnerability of the umbilicus and the heightened risk profile associated with obesity and inflammation, the routine use of an umbilical incision in this high-risk population may warrant reconsideration. Avoiding an umbilical incision altogether may represent a reasonable strategy to mitigate wound-related morbidity; however, clinical evidence directly evaluating this approach in obese patients remains limited. Therefore, we conducted a single-center retrospective cohort study to evaluate the clinical impact of avoiding an umbilical incision in patients with a body mass index (BMI) ≥ 32 undergoing LC, with a particular focus on wound-related morbidity.
Methods
Study design and patients
This single-center retrospective cohort study was conducted at Ohama Daiichi Hospital and reported in accordance with the STROBE guidelines.
We identified 350 patients who underwent LC at our hospital between April 2019 and November 2025. Among these, 75 patients with a BMI ≥ 32 were included in the analysis. All patients underwent LC for benign gallbladder diseases such as cholelithiasis or cholecystitis, and cases involving concomitant procedures were excluded. No cases required conversion to open surgery. All eligible patients during the study period were included, and no additional exclusion criteria were applied.
Patients were classified into two groups: the umbilical incision group and the nonumbilical incision group. The choice of surgical approach was determined on a case-by-case basis at the discretion of the attending surgeon and was influenced primarily by operating room circumstances (e.g., staffing and scheduling factors). Both approaches were performed throughout the study period with substantial temporal overlap; allocation was not randomized. An additional subgroup analysis excluding patients with cholecystitis was performed to assess the influence of cholecystitis on perioperative outcomes. All procedures were performed by one of four board-certified gastrointestinal surgeons experienced in laparoscopic surgery.
Surgical technique
All procedures were performed as multiport LC. In the umbilical incision group, the first port (camera port) was placed at the umbilicus using the open technique. The camera port was 12 mm in diameter, and the additional working ports were 5 mm. Port diameters were identical between groups. All additional ports were placed under laparoscopic visualization. The specimen was extracted through the umbilical incision, which was extended when necessary depending on specimen size. The fascial defect at the umbilicus was closed using 0 absorbable sutures (Vicryl®).
In the nonumbilical incision group, the first port was placed in the left subcostal region using the optical technique. Pneumoperitoneum was initially established through the first port. After placement of the 12-mm camera port, the insufflation tubing was transferred to the camera port to facilitate specimen retrieval through the first port. Additional ports were placed under laparoscopic visualization (Fig. 1). The specimen was retrieved through the first port, and the incision was extended when necessary depending on specimen size. No fascial closure was performed at any port sites in this group. At our institution, routine fascial closure of port sites is not performed in patients with BMI ≥ 32, except at the umbilical incision in the umbilical incision group. Perioperative antibiotic prophylaxis was standardized according to the institutional clinical pathway for LC.
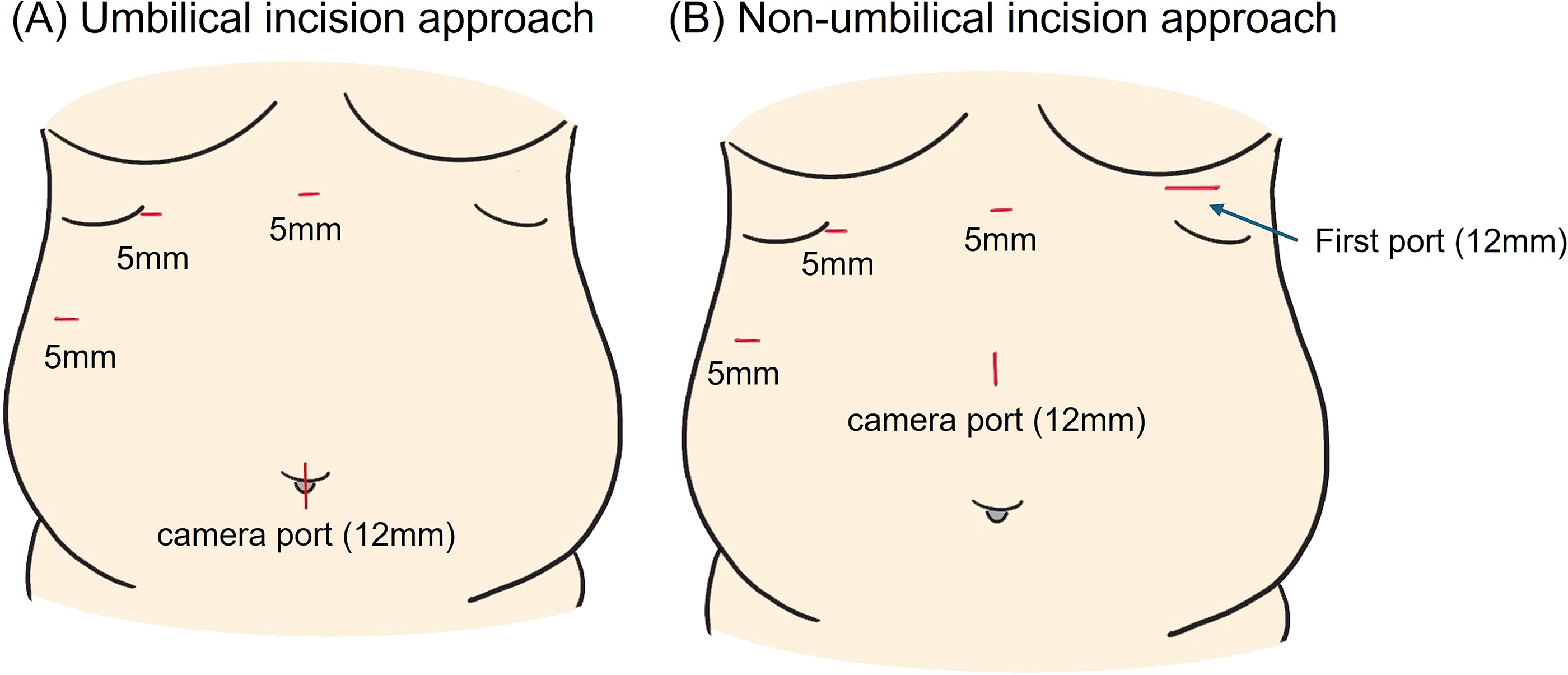
Port placement in laparoscopic cholecystectomy.
Data collection
Patient characteristics and perioperative data were retrospectively collected from electronic medical records. The collected variables included age, sex, BMI, HbA1c, presence of diabetes mellitus, ASA-PS classification, presence of cholecystitis, operative time, blood loss, postoperative complications, and postoperative length of hospital stay. Cholecystitis was defined based on documentation in the medical records, including either preoperative diagnosis or intraoperative findings.
Outcomes
The primary endpoint was overall postoperative complications, defined as complications of Clavien–Dindo classification grade II or higher occurring within 6 months after surgery.
Secondary endpoints included operative time, intraoperative blood loss, postoperative length of hospital stay, and wound-related complications, including SSIs and port-site hernias (PSHs), during the 6-month postoperative follow-up period.
SSIs were diagnosed according to the Centers for Disease Control and Prevention (CDC) criteria. PSHs were suspected based on symptoms (e.g., abdominal bulging or pain) and were confirmed by abdominal computed tomography. Routine imaging was not performed in asymptomatic patients.
Patients were routinely followed in the outpatient clinic for up to 6 months after surgery. All postoperative complications observed in this study were identified within this 6-month period.
Statistical analysis
Continuous variables were expressed as median (interquartile range) and compared using the Mann–Whitney U test. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. For the primary endpoint, absolute risk difference and odds ratios (ORs) with 95% confidence intervals (CI) were calculated. In the presence of zero events, Haldane–Anscombe correction was applied. A P value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 24 (IBM Corp., Armonk, NY, USA). No formal sample size calculation was performed because this was a retrospective cohort study including all eligible patients during the study period. Given the observed absolute risk difference of 13.0%, the study may have been underpowered to detect statistically significant differences, and therefore the results should be interpreted with consideration of the width of the CI. Because the number of outcome events was limited and no events occurred in the nonumbilical group, multivariable modeling was not pursued due to concerns regarding unstable estimates; therefore, the primary analysis focused on absolute risk differences and cautious interpretation of ORs.
Results
Patient flow
Between April 2019 and November 2025, a total of 350 patients underwent LC at our hospital. Among these, 75 patients with a BMI ≥ 32 were included in the present analysis. The umbilical incision approach was performed in 46 patients, and the nonumbilical incision approach was performed in 29 patients.
Patient characteristics
Patient characteristics are summarized in Table 1. The umbilical incision group was significantly older than the nonumbilical incision group (54.5 [45.0–66.0] versus 42.0 [38.0–53.3] years, P = .001). HbA1c levels were also higher in the umbilical incision group (5.9 [5.43–6.30] versus 5.5 [5.30–5.60] %, P = .002). The prevalence of cholecystitis was significantly higher in the umbilical incision group (39.1% versus 10.3%, P = .008). No significant differences were observed between the groups in sex (P = .629), BMI (P = .728), diabetes mellitus (P = .213), or ASA-PS classification ≥ III (P = 1.000).
Patient Characteristics of the Study Population
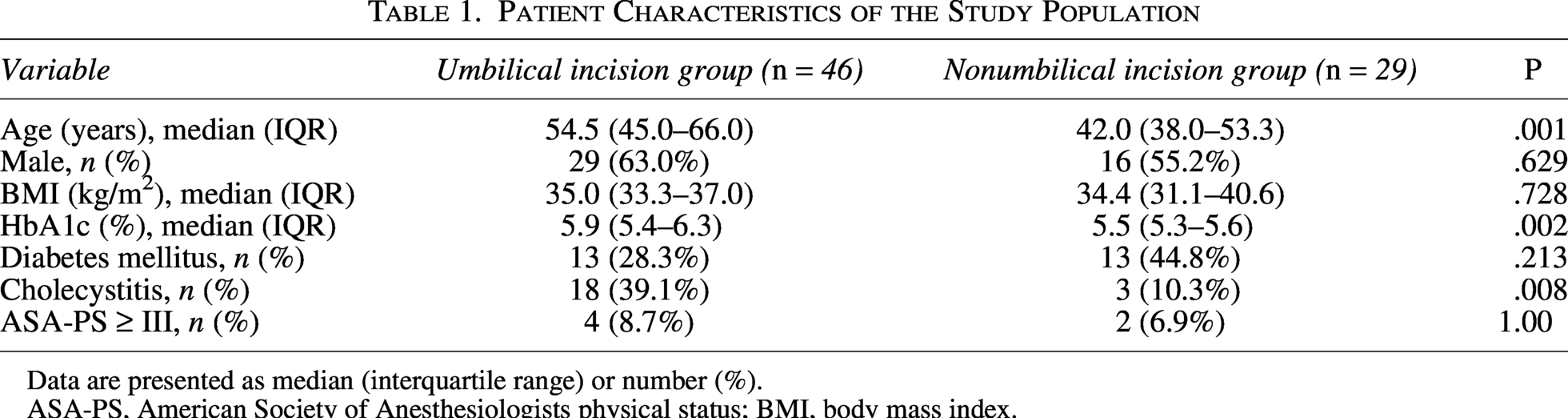
Data are presented as median (interquartile range) or number (%).
ASA-PS, American Society of Anesthesiologists physical status; BMI, body mass index.
Overall postoperative complications (primary endpoint)
Overall postoperative complications (Clavien–Dindo grade ≥ II within 6 months) occurred in 6 of 46 patients (12.8%) in the umbilical incision group and in none of the 29 patients (0%) in the nonumbilical incision group (P = .076; Table 2). The absolute risk difference was 13.0% (95% confidence interval [CI], 3.3%–22.8%). Using Haldane–Anscombe correction to account for zero events in the nonumbilical group, the estimated odds ratio for postoperative complications associated with the umbilical incision approach was 9.47 (95% CI, 0.51–174.76). All recorded complications were wound-related, consisting of four SSIs and two PSHs. No non–wound-related complications were observed. Although the difference did not reach statistical significance, all observed complications occurred in the umbilical incision group.
Perioperative Outcomes in the Overall Cohort
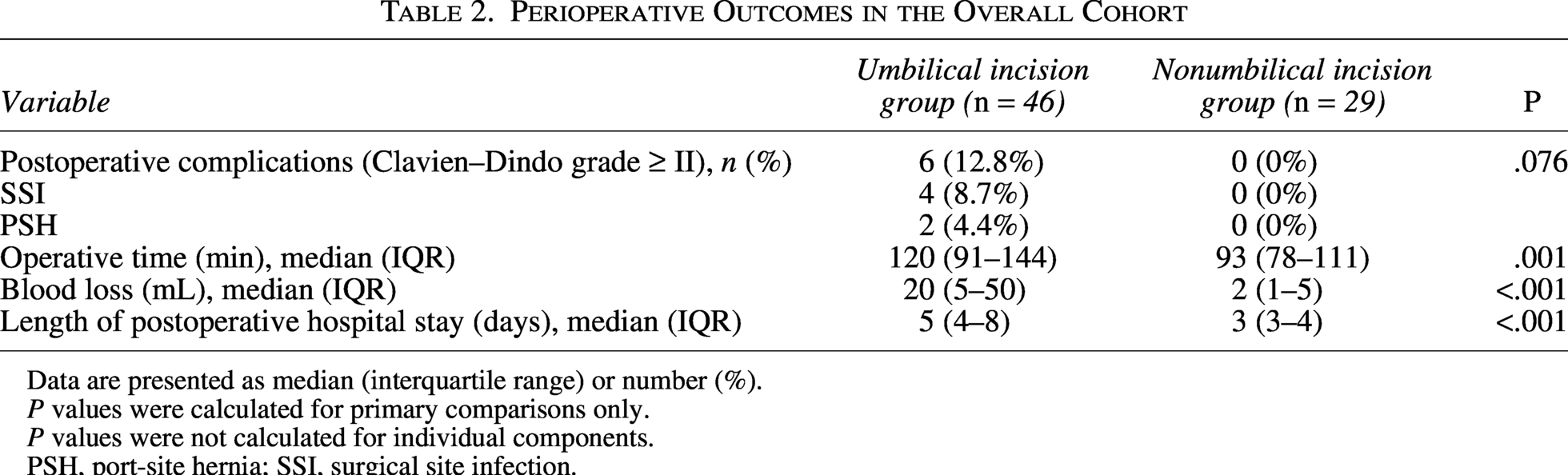
Data are presented as median (interquartile range) or number (%).
P values were calculated for primary comparisons only.
P values were not calculated for individual components.
PSH, port-site hernia; SSI, surgical site infection.
Secondary outcomes in the overall cohort
Operative time was significantly shorter in the nonumbilical incision group than in the umbilical incision group (93 [78–111] versus 120 [91–144] minutes, P = .001). Intraoperative blood loss was also significantly lower in the nonumbilical incision group (2 [1–5] versus 20 [5–50] mL, P < .001). Postoperative length of hospital stay was significantly shorter in the nonumbilical incision group (3 [3–4] versus 5 [4–8] days, P < .001).
Subgroup analysis excluding cholecystitis
Given the imbalance in cholecystitis between groups and its established association with postoperative morbidity, we additionally examined outcomes after excluding patients with cholecystitis (Table 3). The umbilical incision group remained significantly older (54.5 [46.5–64.3] versus 43.0 [38.0–53.3] years, P = .001). HbA1c was also slightly higher in the umbilical incision group (5.6 [5.38–6.20] versus 5.45 [5.30–5.57] %, P = .036). No significant differences were observed in sex, BMI, diabetes mellitus, or ASA-PS classification.
Patient Characteristics After Excluding Patients with Cholecystitis
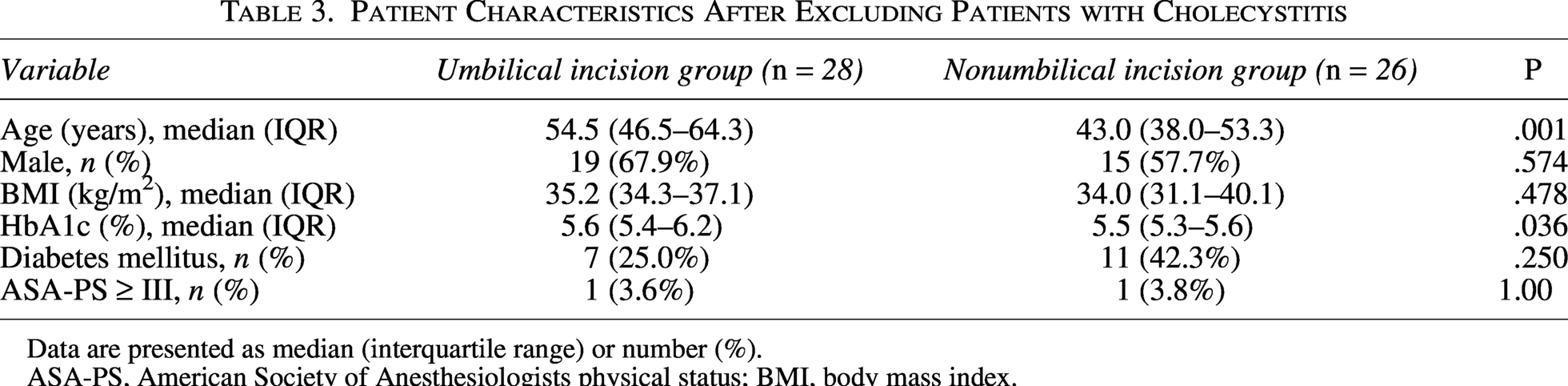
Data are presented as median (interquartile range) or number (%).
ASA-PS, American Society of Anesthesiologists physical status; BMI, body mass index.
In this subgroup, one postoperative complication (3.6%) occurred in the umbilical incision group and none in the nonumbilical incision group (P = 1.000). The single complication was an SSI. Operative time (90 [80–105] versus 111 [95–128] minutes, P = .022), blood loss (2.0 [1.0–3.0] versus 7.5 [5.0–15.0] mL, P < .001), and postoperative length of hospital stay (3 [3–3] versus 4 [4–5] days, P < .001) remained significantly lower in the nonumbilical incision group (Table 4).
Perioperative Outcomes After Excluding Patients with Cholecystitis
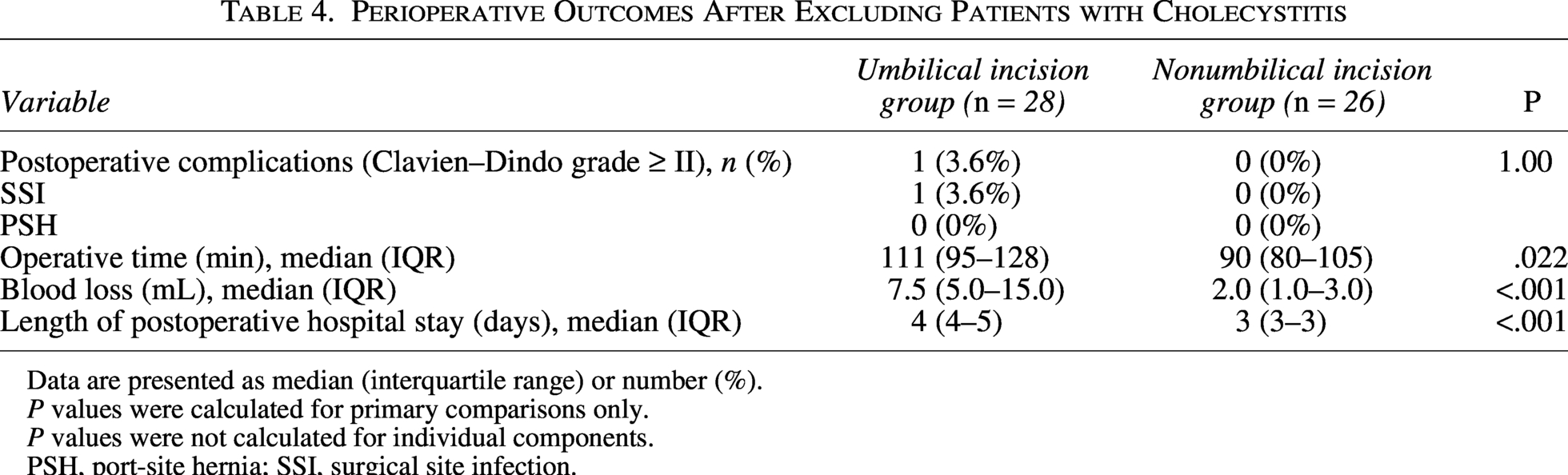
Data are presented as median (interquartile range) or number (%).
P values were calculated for primary comparisons only.
P values were not calculated for individual components.
PSH, port-site hernia; SSI, surgical site infection.
Discussion
In the present study, we compared the umbilical incision approach and the nonumbilical incision approach in obese patients (BMI ≥ 32) undergoing LC. Although no statistically significant difference was observed, all postoperative complications occurred exclusively in the umbilical incision group, whereas no complications were observed in the nonumbilical incision group. Notably, all recorded complications were wound-related and consisted of SSIs and PSHs localized to the umbilical site.
The umbilicus is anatomically distinct from other regions of the abdominal wall. As a congenital scar with relatively weak fascial support and a recessed morphology, it is predisposed to structural vulnerability. Previous studies have demonstrated that the umbilical port is associated with a higher incidence of PSH compared with non-midline extraction sites, and the presence of an umbilical Hasson trocar has been identified as an independent risk factor for trocar-site hernia development.1–3 Furthermore, trocar-site hernias after LC occur predominantly at the umbilical port, particularly when larger trocars are used or the incision is extended. 1 In obese patients, increased subcutaneous fat thickness and elevated intra-abdominal pressure may further amplify these risks. Obesity itself has been identified as an independent risk factor for incisional hernia formation in abdominal surgery and for postoperative SSI.4,5 The finding that all complications in our cohort were confined to the umbilical site is consistent with these anatomical and physiological considerations.
Although the overall complication rate did not differ significantly between groups (P = .076), the absolute risk difference was 13.0% (95% CI 3.3%–22.8%), and the corrected odds ratio yielded a higher point estimate for complications in the umbilical incision group; however, the wide confidence interval indicates substantial statistical uncertainty due to the limited number of events. These estimates should be interpreted with caution and considered exploratory due to the limited number of events. Rather than demonstrating superiority, these findings suggest a potentially clinically meaningful difference that warrants confirmation in larger studies.
Cholecystitis was significantly more frequent in the umbilical incision group. Acute inflammation and disease severity have been reported as independent predictors of postoperative complications after LC.6,7 Therefore, the imbalance in cholecystitis between groups may have influenced the observed outcomes. This imbalance may have biased the results toward a higher complication rate in the umbilical incision group.
However, even after excluding patients with cholecystitis, the only postoperative complication occurred in the umbilical incision group, and none were observed in the nonumbilical group. This suggests that the anatomical vulnerability of the umbilical wound may contribute to complications independently of inflammatory status.
Another important consideration is fascial management. In our institutional practice, fascial closure was performed at the umbilical site in the umbilical incision group, whereas nonumbilical port sites were not routinely closed in obese patients. Despite the absence of fascial closure at nonumbilical ports, no PSHs occurred outside the umbilicus. Prior studies have suggested that midline port sites and larger trocar diameters are major determinants of trocar-site hernia development, whereas the protective effect of fascial closure alone remains inconsistent.1,3 This observation implies that the intrinsic characteristics of the umbilicus, rather than fascial closure alone, may play a central role in the development of wound-related complications. Nevertheless, the potential influence of fascial closure cannot be completely excluded and warrants further investigation.
An additional consideration is the number of ports. The nonumbilical incision approach requires one additional port compared with the conventional umbilical approach. In theory, increasing the number of ports may raise concerns regarding postoperative pain or additional wound complications. However, previous randomized and comparative studies evaluating extraction sites have reported mixed results regarding port-site morbidity and operative outcomes.2,8,9 In the present study, the nonumbilical approach was not associated with increased morbidity. No wound-related complications were observed at nonumbilical port sites, and postoperative hospital stay was not prolonged. These findings suggest that, in obese patients, the clinical impact of adding one small port may be minimal when weighed against the potential vulnerability of the umbilical incision.
In addition to wound outcomes, the nonumbilical incision approach was associated with shorter operative time, reduced blood loss, and shorter postoperative hospital stay. A recent meta-analysis suggested that epigastric retrieval may be associated with shorter operative time compared with umbilical retrieval in certain analyses. 2 The shorter operative time observed in our cohort may also be partially attributable to the omission of umbilical fascial closure. From a practical surgical perspective, these findings suggest that avoiding the umbilical incision does not increase technical difficulty and may be associated with procedural advantages. Notably, all outcome measures consistently favored the nonumbilical approach, including complications, operative time, blood loss, and length of hospital stay. Although a four-port configuration may be technically feasible for the nonumbilical approach, dissection from the left subcostal port was often technically challenging due to suboptimal instrument angles. In our experience, attempts to perform the procedure with four ports were associated with increased technical difficulty and a potential risk of bleeding or gallbladder perforation. Therefore, an additional 5-mm port was introduced to facilitate safer and more controlled dissection, allowing the procedure to be performed in a manner similar to conventional LC. Importantly, the addition of one small port was not associated with increased postoperative pain, impaired cosmesis, or a higher risk of PSH in our cohort. Furthermore, the first port occasionally provided a useful alternative angle for dissection or facilitated instrument exchange, serving as a complementary option during the procedure.
Several limitations should be acknowledged. First, this was a retrospective, single-center study, and the choice of surgical approach was at the discretion of the attending surgeon, introducing potential selection bias. Second, the number of events was limited, which may have reduced statistical power. Third, follow-up was restricted to six months, and asymptomatic PSHs were not routinely screened. Fourth, baseline age differed between groups, and age-related differences in wound healing capacity may have influenced outcomes.
In conclusion, although statistical significance was not achieved, all postoperative wound-related complications occurred in the umbilical incision group, whereas none were observed in the nonumbilical incision group. In obese patients undergoing LC, avoiding an umbilical incision appears to be a safe and clinically reasonable surgical strategy, although the findings should be interpreted as hypothesis generating. Larger prospective studies are warranted to confirm these findings.
Authors’ Contributions
Y.U.: Conceptualization, data curation, formal analysis, and writing—original draft. S.I.: Supervision and writing—review and editing.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study was approved by the institutional review board of Ohama Daiichi Hospital (approval number: 276).
Consent to Participate
The requirement for informed consent was waived due to the retrospective nature of the study.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research received no external funding.