
Abstract
Introduction:
Sleeve gastrectomy (SG) is currently the most commonly performed bariatric procedure worldwide. However, the development or persistence of gastroesophageal reflux disease (GERD) remains a significant concern, particularly in patients with preexisting reflux symptoms. In selected bariatric patients affected by symptomatic GERD, alternative surgical strategies may be required. This prospective observational study aimed to evaluate the long-term outcomes of SG combined with Rossetti fundoplication (SGRF) in a selected population of patients with morbid obesity and documented GERD.
Methods:
Patients with obesity and preoperative GERD symptoms, chronic proton pump inhibitor (PPI) use, and endoscopic evidence of esophagitis were prospectively enrolled, underwent SGRF, and were followed for more than 5 years. Unlike SG combined with Nissen fundoplication, the Rossetti technique requires a smaller portion of the gastric fundus to construct the antireflux wrap. This aspect may be particularly relevant in bariatric surgery, as SG is based on the resection of most of the gastric fundus, which contains ghrelin-producing orexigenic cells.
Results:
In total, 38 out of 58 patients enrolled (65.5%) completed long-term follow-up (mean 68.5 months). Of all, 92.1% of patients had discontinued PPIs and reported resolution of reflux symptoms. Among the 24 patients who underwent long-term gastroscopy, 96.6% showed no evidence of esophagitis. The adjusted total weight loss (%TWL) was 26.1%.
Conclusion:
These findings suggest that SGRF may represent a promising surgical option for carefully selected bariatric patients with GERD. Further prospective studies, including objective functional assessments such as esophageal manometry and pH monitoring, are needed to better define the role of this technique.
Keywords
Introduction
It is estimated that around 30% of the world’s population (2.1 billion people) is overweight or affected by obesity, 1 which significantly increases the risk of numerous medical conditions, including gastroesophageal reflux disease (GERD).2–4 Effective weight loss and reduction in body mass index (BMI) have been demonstrated, by systematic review and meta-analysis, to improve GERD symptoms and decrease esophageal acid exposure. 5 Metabolic and bariatric surgery (MBS) represents the most effective long-term treatment for severe obesity and its related comorbidities. However, despite consistent weight loss, MBS may induce de novo GERD or worsen preexisting reflux, which is a critical long-term complication. In particular, the prevalence of GERD after the most common bariatric procedure, sleeve gastrectomy (SG), is a significant concern, with reported rates for reflux symptoms ranging from 2% to 20%.6,7 This is a significant issue, as long-term studies like the multicenter clinical trials SM-BOSS 8 and SLEEVEPASS 9 have shown that the prevalence of esophagitis and GERD is significantly higher after SG compared with Roux-en-Y gastric bypass (RYGB).
This persistent risk highlights an unmet need for technical modifications to SG to mitigate postoperative GERD. Various antireflux surgical techniques have been developed.10–14 Among these, fundoplication is considered a valid option because it directly addresses the underlying pathophysiology of reflux by creating a new barrier at the gastroesophageal junction. The Rossetti fundoplication (RF) is a specific variant of the Nissen technique that creates a 360° wrap using only the anterior wall of the gastric fundus. 15 This modification is hypothesized to maintain the antireflux effect while minimally involving the gastric fundus, whose resection is a crucial factor in achieving weight loss success after SG.
Given the prevalent long-term issue of GERD after SG and the potential benefits of adding an antireflux mechanism, this study aims to evaluate the durability and long-term performance of the combined procedure. We hypothesized that the addition of the RF would provide favorable long-term outcomes.
Specifically, in patients with obesity undergoing SG, does the concomitant addition of the RF ensure, over a 5-year follow-up period, effective weight loss maintenance and durable resolution of GERD?
This paper reports the 5-year follow-up data of a prospective cohort study, extending the results previously published at 1-year. 16
Methods
Study design and setting
This work presents the long-term (≥60 months) follow-up of a prospective, observational cohort study carried out through a collaboration between a high-volume bariatric center and an independent data management and analysis unit. This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. All surgical procedures were performed between June 2017 and September 2018 by the same surgical team at Policlinico San Marco (Zingonia, Italy), a high-volume bariatric center. Clinical data were prospectively collected in a dedicated database designed and maintained by the Center for Public Health Research (University of Milano-Bicocca, Monza, Italy), an independent data management and analysis unit. All participants provided written informed consent. The study was approved by the Ethics Committee of Bergamo (final resolution issued on March 7, 2017) and conducted in accordance with the ethical standards of the institutional research board and the Declaration of Helsinki (1964) and its later amendments.
Patients population, inclusion and exclusion criteria
Patients were enrolled in the study if they were affected by obesity suitable for surgery according to bariatric guidelines 17 and associated with GERD. All patients met the criteria for bariatric intervention (i.e., BMI > 40 kg/m2, or BMI 30 to 40 kg/m2 and at least one comorbidity, such as hypertension, type 2 diabetes, arthropathies, or obstructive sleep apnea syndrome). GERD was defined according to the Montreal definition, 18 and was based on endoscopic findings of esophagitis according to the Los Angeles classification system. 19
All enrolled patients had both GERD symptoms that required PPIs and esophagitis, demonstrated by Esophago-Gastro-Duodenoscopy (EGDS) performed no more than 3 months before enrollment.
The exclusion criteria were: age <18 or >65 years; presence of esophageal motility disorders; history of previous bariatric surgery or procedures involving the gastroesophageal junction; contraindications to laparoscopic surgery; or a performance status of 3–4. All patients were assessed by a multidisciplinary team including a trained psychologist, dietitian, and anesthesiologist.
Assuming that the prevalence of GERD (main outcome) was 3% at 1 year after antireflux surgery, 20 with a 5% margin of error and a 95% confidence level (CI), the calculated sample size required for this observational study was 45 patients.
Surgical technique
Four trocars were used: a 10 mm trocar in the left subcostal space for the optic view, a 5 mm trocar in the epigastrium for liver retraction, and two operative trocars in the right hypochondrium (5 mm) and above the navel (15 mm). We started by dissecting the gastrocolic and gastrosplenic ligaments at the gastric margin using the LigaSure™ Maryland laparoscopic sealer/divider (Medtronic, Colorado, USA). After mobilizing the gastric fundus, we dissected the crura, creating a small passage behind the cardia and the distal esophagus.
Through this passage, we built the fundoplication on a 38 Fr oro-gastric bougie. It is a 1.5 to 2 cm long, floppy, anterior 360° fundoplication, according to Rossetti’s modification to Nissen’s technique. 15 This modification is hypothesized to maintain the antireflux effect while minimally involving the gastric fundus, whose near-complete resection is a crucial factor in achieving weight loss success after SG due to its role in appetite regulation. RF is built with two interrupted, nonabsorbable, extracorporeal Roeder knots (Ethibond 0, Ethicon, Somerville, NJ). A linear stapler is then used to cut the stomach over the 38 Fr bougie (Tristaple Signia stapling system, Medtronic, Dublin, Ireland), choosing different staple heights for different tissue thicknesses. An indocyanine green (ICG) fluorescence imaging (SPIES, Storz) test was performed at the end of the operation to demonstrate the proper vascularization of the staple line.
Postoperative management and follow-up
Patients started an oral diet on postoperative day 2 after performing an upper gastrointestinal (UGI) series with oral water-soluble contrast (Gastrografin, Bracco Diagnostics, Italy) to check for staple line leaks. Blood analyses were performed on the first and third postoperative days as part of a routine postoperative protocol. If the postoperative course was regular, the patient was discharged on the third postoperative day. The patients continued with low molecular weight heparin for 24 days and PPIs for 60 days after surgery at 40 mg per day.
Follow-up visits were scheduled at 1, 3, 6, 12 months, and annually thereafter, for a total of 5 years. Patients underwent EGDS at 1 and 5 years after surgery. Long-term follow-up data on weight and GERD symptoms were collected through structured telephone interviews.
Statistical analysis
Statistical analyses were performed by an independent data management and analysis unit, ensuring statistical expertise was available for all analyses. Descriptive statistics were used to summarize patients’ demographic and clinical characteristics, using mean ± standard deviation (SD) for continuous variables and counts/percentages for categorical variables. Group comparisons were performed using Student’s t-test for normally distributed continuous variables and Pearson’s chi-square test or Fisher’s exact test, as appropriate, for categorical variables. To evaluate changes in GERD outcomes between baseline and long-term follow-up (≥60 months), paired proportions were compared using McNemar’s test. Longitudinal changes in BMI and percentage of total weight loss (%TWL) over time were analyzed using linear mixed-effects models (LMM) with random intercepts for each patient to account for intra-subject correlation. Time was modeled as a categorical variable (baseline, 1, 3, 6, 12, and ≥60 months). 16 Models were adjusted for baseline BMI, age, and sex. Robust standard errors clustered at the patient level were used. Adjusted marginal means with 95% CI were estimated for each follow-up point. Pairwise comparisons between time points were corrected for multiple testing using the Bonferroni adjustment. A P value <0.05 was considered statistically significant. Statistical analyses were performed using Stata 19.5 (StataCorp, College Station, USA).
Results
Demographic and clinical characteristics
Of the 58 patients included in the sister study, 16 38 completed long-term follow-up: given the variability in the duration of long-term follow-up among the limited number of patients (mean: 68.5 ± 4.1 months), all assessments beyond 60 months were grouped as ≥60 months. The characteristics of the study population are reported in Table 1.
Study Population (N = 38)
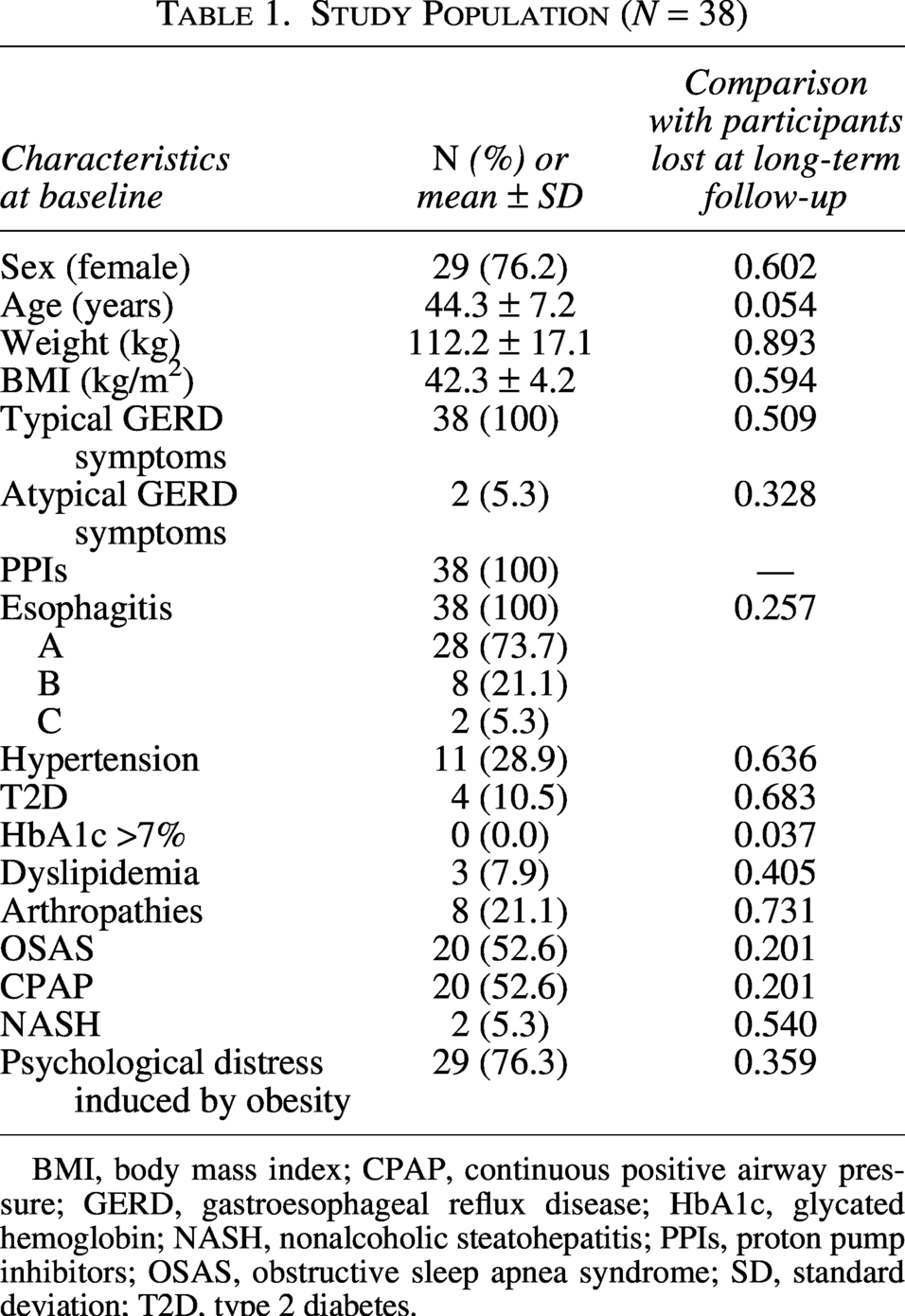
BMI, body mass index; CPAP, continuous positive airway pressure; GERD, gastroesophageal reflux disease; HbA1c, glycated hemoglobin; NASH, nonalcoholic steatohepatitis; PPIs, proton pump inhibitors; OSAS, obstructive sleep apnea syndrome; SD, standard deviation; T2D, type 2 diabetes.
All patients had confirmed GERD with typical symptoms (heartburn and regurgitation) and were receiving PPI therapy at baseline. Two patients (5.3%) also presented atypical symptoms (cough, dysphonia, or sore throat). Preoperative EGDS revealed esophagitis in all cases: grade A in 28 patients (73.7%), grade B in 8 (21.1%), and grade C in 2 (5.3%).
All patients underwent laparoscopic SGRF.
Long-term surgical outcomes
Complications requiring surgical revision (Clavien–Dindo Grade ≥ IIIb) occurred in seven patients (12.1% of the long-term cohort). Detailed characteristics of these reinterventions are summarized in Table 2. In the early postoperative period, two patients (3.4% of the total n = 58 cohort) underwent urgent revision due to valve perforations. Among the 38 patients who completed the long-term follow-up, five (13.2%) required secondary surgical procedures. The primary indications for reintervention were categorized into mechanical failure of the fundoplication (n = 2; 5.3%) and bariatric failure (n = 3; 7.9%). Specifically, mechanical failures included one case of wrap disruption and one hiatal hernia recurrence with valve slippage. Conversely, three patients underwent revision primarily due to weight regain: two of these presented with an intact fundoplication, while one presented with concomitant wrap disruption. Consequently, a total of 7.9% of the long-term cohort required surgical revision for weight regain.
Early and Late Surgical Complications
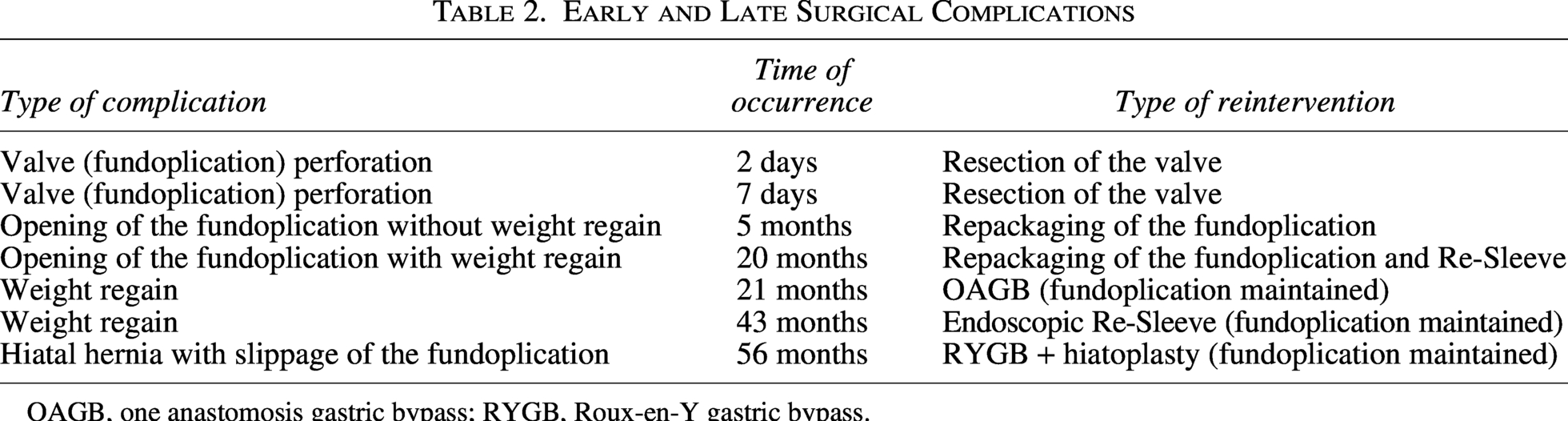
OAGB, one anastomosis gastric bypass; RYGB, Roux-en-Y gastric bypass.
Gastroesophageal reflux outcomes
At baseline, all patients were receiving PPI therapy. At long-term follow-up (≥60 months), the majority of patients had discontinued therapy, with only 6 patients (15.8%) remaining on treatment (two of whom used PPIs on an as-needed basis). This decline in PPI use was statistically significant (McNemar’s test, P < .001). The remaining patients reported no reflux symptoms.
Among the 24 patients who underwent long-term EGDS, only one (4.2%) presented with grade A esophagitis (McNemar’s test, P < .001); this patient was asymptomatic, required no medication, and had already shown grade A esophagitis before SGRF.
Weight loss
From the initial cohort of 58 patients with a preoperative BMI of 42.1 ± 4.7 kg/m2, weight data at long-term follow-up (≥60 months) were available for 32 patients (55.2%). The LMM, adjusted for baseline BMI, age, and sex, demonstrated a significant BMI reduction as early as 1 month (37.1 kg/m2, 95% CI: 36.5–37.7 vs. kg/m2, 95% CI: 41.7–42.6 at baseline). Weight loss continued to progress until 12 months (28.5 kg/m2, 95% CI: 27.7–29.2). At ≥60 months, a partial regain was observed (30.9 kg/m2, 95% CI: 29.6–32.2); however, BMI remained significantly lower than at baseline. In addition to the effect of time, several baseline covariates were independently associated with BMI trajectories. Baseline BMI was positively correlated with BMI throughout follow-up (β = 0.70; P < .001), indicating that individuals with higher starting values tended to maintain higher BMI levels after surgery. Age also showed a modest but significant effect (β = 0.09 per year; P < .01), suggesting that older patients tended to have slightly higher BMI values during follow-up. Finally, sex was a significant predictor (β = 0.88; P = .04), with women exhibiting on average nearly one BMI point higher than men, after adjustment for baseline BMI and age (Table 3 and Fig. 1). Adjusted mean differences in BMI between pairs of time points derived from the LMM are presented in Supplementary Table S1 (Supplementary Data). The adjusted %TWL calculated at LLM was 32.1 (95% CI: 30.6–33.5) at 1-year follow-up and 26.1 (95% CI, 22.9 to 29.2) at long-term follow-up. Higher baseline BMI was associated with greater %TWL (β = 0.28; P = .001), while older age (β = −0.20; P = .001) and female sex (β = −2.37; P = .018) predicted lower weight loss over time (Table 4 and Fig. 2). Adjusted mean differences in %TWL between pairs of time points derived from the LMM are presented in Supplementary Table S2.
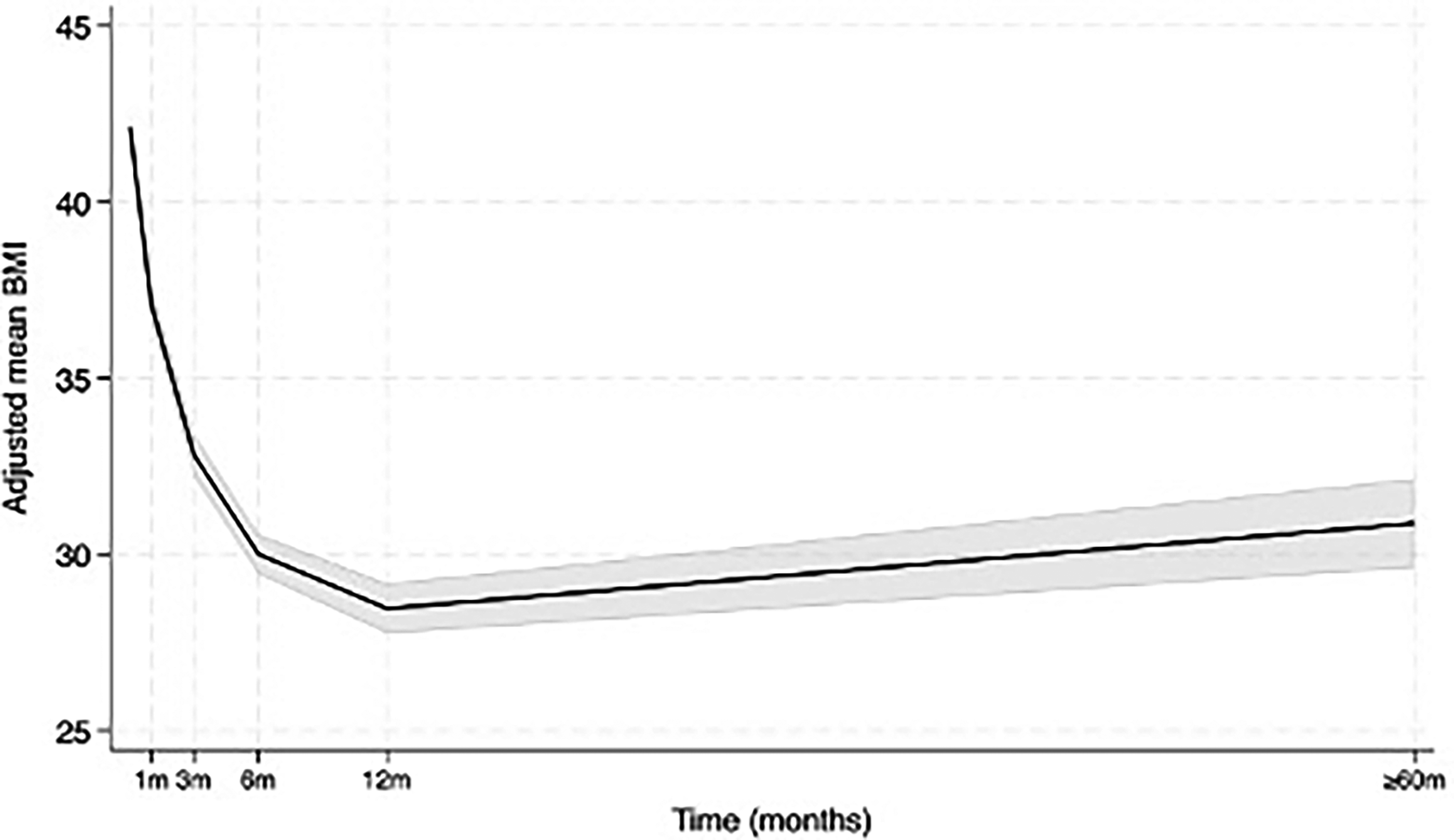
Trajectories of body mass index (BMI), with 95% confidence intervals (CI). Due to heterogeneity in long-term follow-up timing, the “≥60 months” category summarizes the mean values observed at each patient’s last clinical contact beyond 60 months. BMI is expressed in kg/m2.
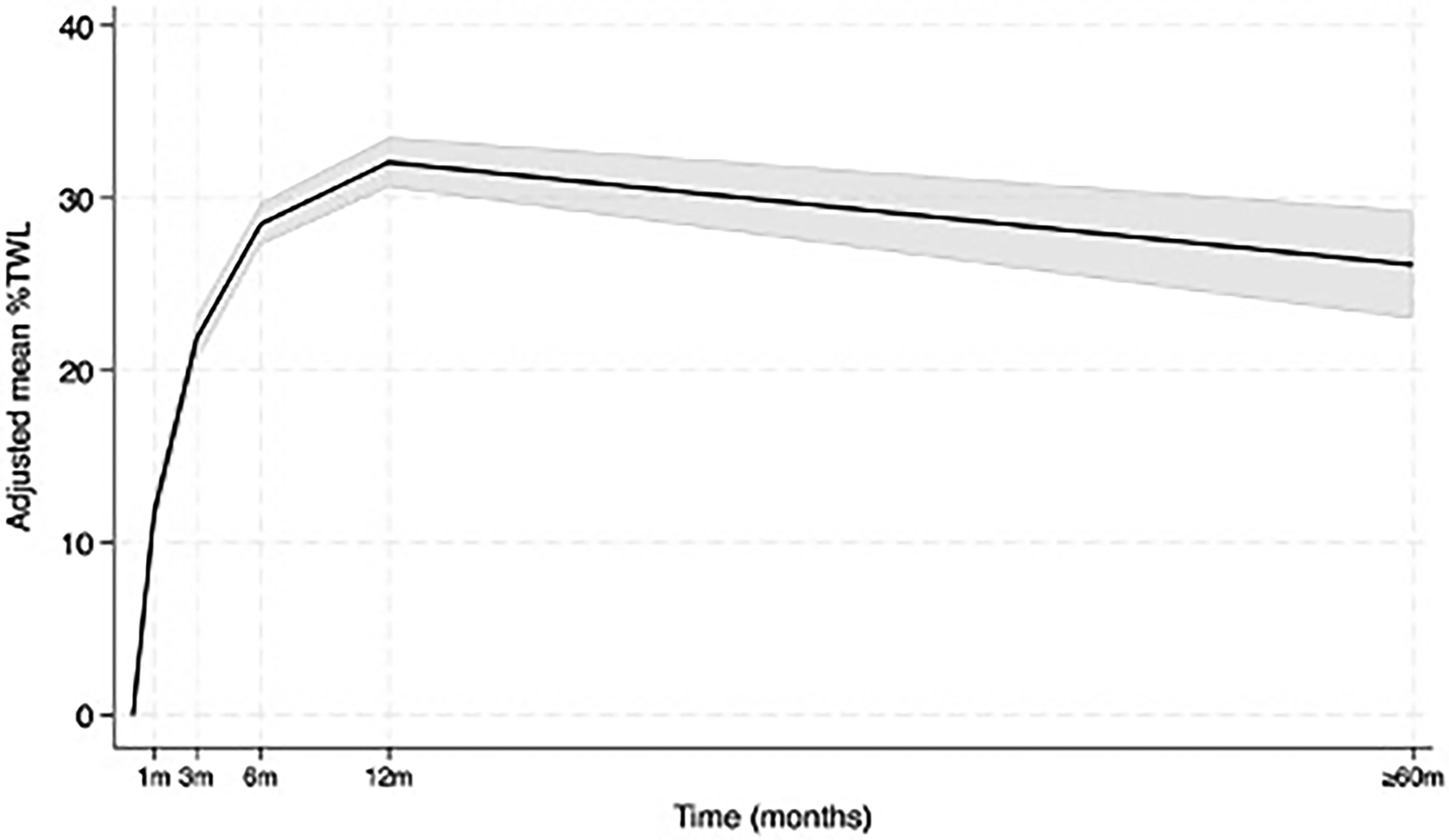
Trajectories of percentage total weight loss (%TWL), with 95% confidence intervals (CI). Due to heterogeneity in long-term follow-up timing, the “≥60 months” category summarizes the mean values observed at each patient’s last clinical contact beyond 60 months.
Linear Mixed-Effects Model for BMI Trajectories at Long-Term Follow-Up
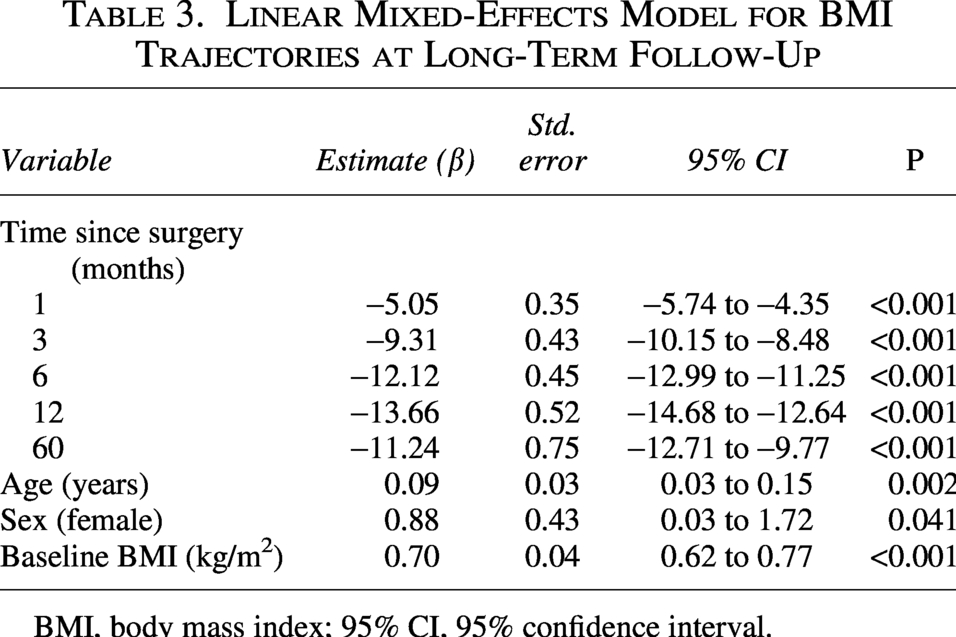
BMI, body mass index; 95% CI, 95% confidence interval.
Linear Mixed-Effects Model for Percentage Total Weight Loss Trajectories at Long-Term Follow-Up
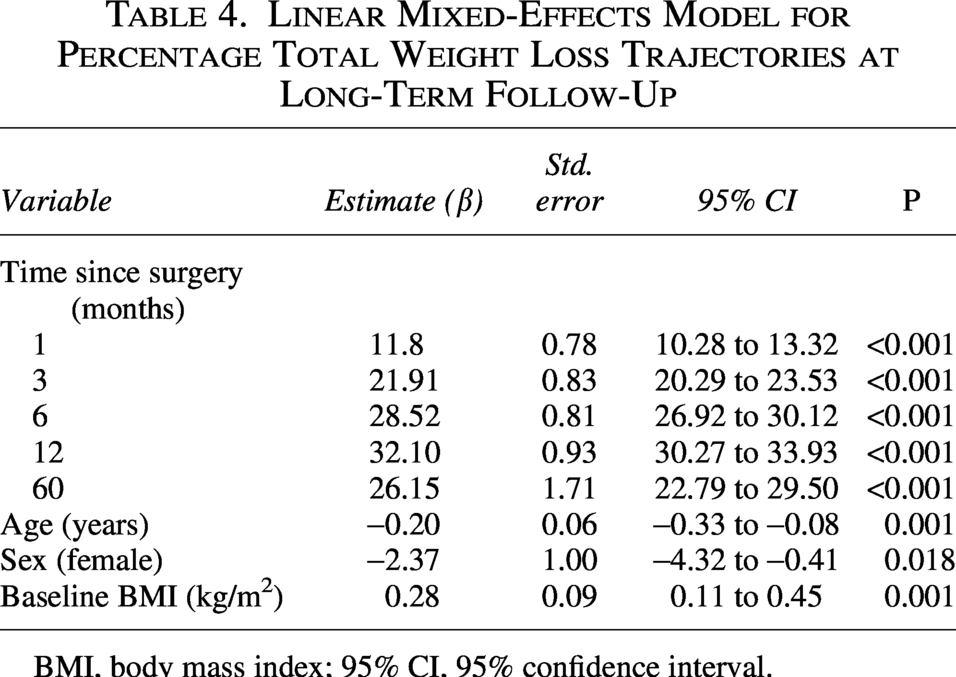
BMI, body mass index; 95% CI, 95% confidence interval.
Discussion
This prospective, observational study, with a long follow-up of over 5 years, demonstrates that SGRF may be an effective procedure for patients with both obesity and coexisting GERD.
The primary success of the procedure lies in its significant and sustained improvement in GERD symptoms. Five years after the operation, 92.1% of patients had discontinued PPIs and were asymptomatic, with 96.6% showing no evidence of esophagitis on endoscopic evaluation. This finding is particularly notable given that SG alone is often associated with the worsening or onset of GERD.6–9 The excellent reflux control demonstrated by SGRF could make it a valuable alternative to other bariatric procedures, such as RYGB, for patients with obesity and established GERD.
The procedure also showed promising results regarding weight loss. The mean 5-year %TWL of 26.2% is comparable to the outcomes of standard SG, 21 supporting the hypothesis that the Rossetti modification preserves the essential antiobesity mechanisms of the gastric fundus.
Regarding perioperative safety, our series reported an early perforation rate of 3.4%. While this incidence is higher than the leakage rates typically associated with standard SG, it must be interpreted within the context of the surgical learning curve. Bariatric surgeons are traditionally less accustomed to the specific maneuvers of antireflux surgery, such as hiatal dissection and fundoplication wrapping. Notably, we observed that the incidence of perforation decreased significantly as technical proficiency with the RF increased. 16 This suggests that with standardized training and increased volume, the safety profile of SGRF can be further optimized to match conventional bariatric standards.
Furthermore, the long-term reintervention profile of SGRF provides a compelling argument for its durability. In our cohort, the rate of revision for weight regain (7.9%) compares favorably with the revision rates reported for standard SG over a 10-year period. 22 More significantly, while long-term data for standard SG indicate that 7% of patients eventually require conversion to RYGB specifically for refractory GERD, 23 our series showed a distinctively low rate of mechanical failure. Only one patient (2.6%) required revision due to a hiatal hernia recurrence, and none required conversion specifically for uncontrolled reflux. This suggests that the SGRF wrap provides a robust and lasting antireflux barrier that may mitigate the need for the late “reflux-driven” conversions often seen after standard SG.
Despite these positive findings, our study has some inherent limitations. First, while the final sample size of 38 patients represents a drop from the initial cohort of 58, it still constitutes 84% of the minimum required sample size of 45 subjects, as determined by the statistical power calculation. Furthermore, this long-term patient attrition (∼35% at 5 years) must be interpreted within the context of bariatric surgery: high drop-out rates are a widely acknowledged issue in long-term bariatric follow-up, often exceeding 50%, particularly in patients who have achieved positive outcomes and are asymptomatic. 24 These patients frequently cease attending routine check-ups, especially for procedures like endoscopy.
Second, the assessment of GERD symptoms relied on patient self-reports, which are subjective. However, the symptomatic data were robustly supported by objective measures, including the discontinuation of PPI therapy and endoscopic findings (EGDS), which showed minimal esophagitis recurrence. While gold-standard objective tests like manometry and pH-metry were not systematically performed, their inclusion is often challenging to achieve in a long-term bariatric follow-up setting.
Conclusions
In conclusion, our findings suggest that SGRF appears to be a safe and potentially effective surgical option for patients with obesity and comorbid GERD. Despite the inherent limitations of this study, it is important to highlight that our analysis was conducted on a highly selected patient population, all of whom presented with symptomatic reflux requiring PPI therapy and had endoscopic evidence of esophagitis at the preoperative work-up. Furthermore, the extended follow-up period provides valuable insights into the durability of these results. Future prospective, ideally randomized controlled trials, are warranted to further investigate these trends. Larger patient cohorts and the systematic implementation of objective functional assessments (such as pH-manometry) remain essential to more definitively establish the role of SGRF as a primary therapeutic alternative for this specific patient subset.
Authors’ Contributions
All authors contributed to the study’s conception, design, data collection, analysis, and interpretation. The first draft of the article was written by the corresponding author, and all authors critically reviewed and approved the final version of the article. All authors agree to be accountable for the accuracy and integrity of the work.
Ethics Approval
This study was conducted in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments. The study protocol was approved by the Ethics Committee of Bergamo (final resolution issued on March 7, 2017).
Informed Consent
Written informed consent was obtained from all individual participants included in the study prior to enrollment. Participants consented to the use of their anonymized clinical data for research purposes.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. No public repository is available due to privacy restrictions.
Footnotes
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding Information
No funding was received to assist with the preparation of this article or for conducting this study.
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.