
Abstract
Introduction:
Superior mesenteric artery syndrome (SMAS) is an uncommon cause of abdominal pain, emesis, and weight loss in children. While there are many surgical options, we previously reported a small series of laparoscopic duodenal lowering (DL), which became our standard first approach. Here, we report our expanded experience on the surgical management of patients with SMAS.
Methods:
We conducted a retrospective chart review of patients who underwent surgical management of SMAS between January 2008 and December 2023 at our institution.
Results:
22 patients underwent surgical management for SMAS during this study period. The majority of patients were female (n = 19, 86%), and median age at time of surgery was 17 years (interquartile ranges: 16.0, 18.4). The median measured aorto-SMA angle was 16° (12, 20), with 3 patients having an aorto-SMA angle as narrow as 10°. Twenty patients underwent laparoscopic DL, and 2 patients underwent laparoscopic duodenojejunostomy, as they had previously undergone surgical procedures for SMAS at another institution (open duodenal de-rotation, open DL, and median arcuate ligament release). Of the 20 patients who underwent DL, 12 patients (60%) had resolution of their symptoms. Two of these patients had recurrence of symptoms within 6 months and underwent subsequent LDJ. Of the 8 patients without improvement after DL, 2 underwent subsequent LDJ with improvement of symptoms. The median follow-up for all patients was 51 days (33, 321). In both univariate and multivariate statistical analyses, having a diagnosis of Ehlers–Danlos syndrome was predictive of failure to achieve symptom resolution after DL (P = .004). No other clinical or demographic characteristics were found to be predictive of successful resolution of symptoms from surgery.
Conclusions:
Patients with SMAS are a complex population. The more conservative DL can be an efficacious first step when approaching surgical management of SMAS. Future investigation is warranted to characterize which patients are more likely to fail operative intervention or require repeat operations.
Keywords
Introduction
Superior mesenteric artery syndrome (SMAS) is an uncommon cause of abdominal pain, emesis, and weight loss with an estimated incidence of 0.01%−0.3%. 1 This disease more commonly affects women and patients aged 10–39 years old. 2 The rational explanation is that the third portion of the duodenum is obstructed by compression between the aorta and superior mesenteric artery (SMA) as it courses between them. The mesenteric fat pad between the SMA and aorta is thought to act as a cushion keeping the SMA off the third portion of the duodenum. A normal angle of the aorta and SMA, the aortomesenteric angle, is 38°–65°, and loss of the mesenteric fat pad causes a more acute aortomesenteric angle, resulting in SMAS.
First-line treatment is nutritional support, sometimes with enteral feeding beyond the obstruction with the goal of weight gain to increase the fat pad size separating the duodenum and SMA. Nonoperative management is successful in over 80% of patients.1,3 If this treatment fails, surgical options include duodenojejunostomy (LDJ) to bypass the obstruction, anterior transposition of the duodenum, derotation, or extensive mobilization of the duodenum.2,4,5 However, our institution has previously studied laparoscopic duodenal lowering (DL), which has become our standard first-line therapy, as it avoids both an anastomosis and derotation. 2 Our prior report has shown this technique to be efficacious in 7 patients. Here, we report the larger experience with SMAS.
Materials and Methods
Institutional review board approval was obtained (#00002970), and a waiver of informed consent was granted. A list of patients with the diagnosis code of SMAS that underwent surgical treatment at our freestanding children’s hospital from January 2008 to December 2023 was created. A retrospective review was conducted. The primary outcome of interest was resolution of symptoms after the DL procedure. Secondary outcomes included need for repeat operations, return of symptoms, length of stay (LOS), operative time, and duration of symptom relief.
Demographic data, LOS, radiographical findings, and operative details were abstracted from the electronic medical records and stored in a secure database. Results are reported in percentages for categorical variables and medians with interquartile ranges (IQR) for continuous variables. Statistical analysis, including univariate and multivariate analyses, was performed in STATA (StataCorp 2017) using the chi-square test for categorical variables and the Wilcoxon rank sum test for continuous variables. We used a level of significance of alpha = 0.05.
Operative Techniques
Laparoscopic DL
Standard prepping and draping were completed with the patient kept supine, and a 5 mm infraumbilical port was placed. Additional stab incisions x3 were placed, one in the right mid-abdomen, one in the right lower quadrant, and one in the left mid-abdomen. The transverse colon was reflected cephalad to identify the ligament of Treitz. The ligament of Treitz was incised, carefully avoiding the mesenteric vessels, and dissection was continued medially. Monopolar cautery was used when necessary, but most of the dissection was blunt. Next, the duodenum was mobilized while preserving the mesentery, and dissection was continued until we were across the aorta and could usually look from the patient’s left to right underneath the base of the mesentery clear to the liver. At this point, the IVC and superior mesenteric vessels were fully visualized. The relationship of the duodenum to the SMA was inspected to confirm that the duodenum had lowered down away from the SMA angle, relieving any obstruction (Fig. 1).
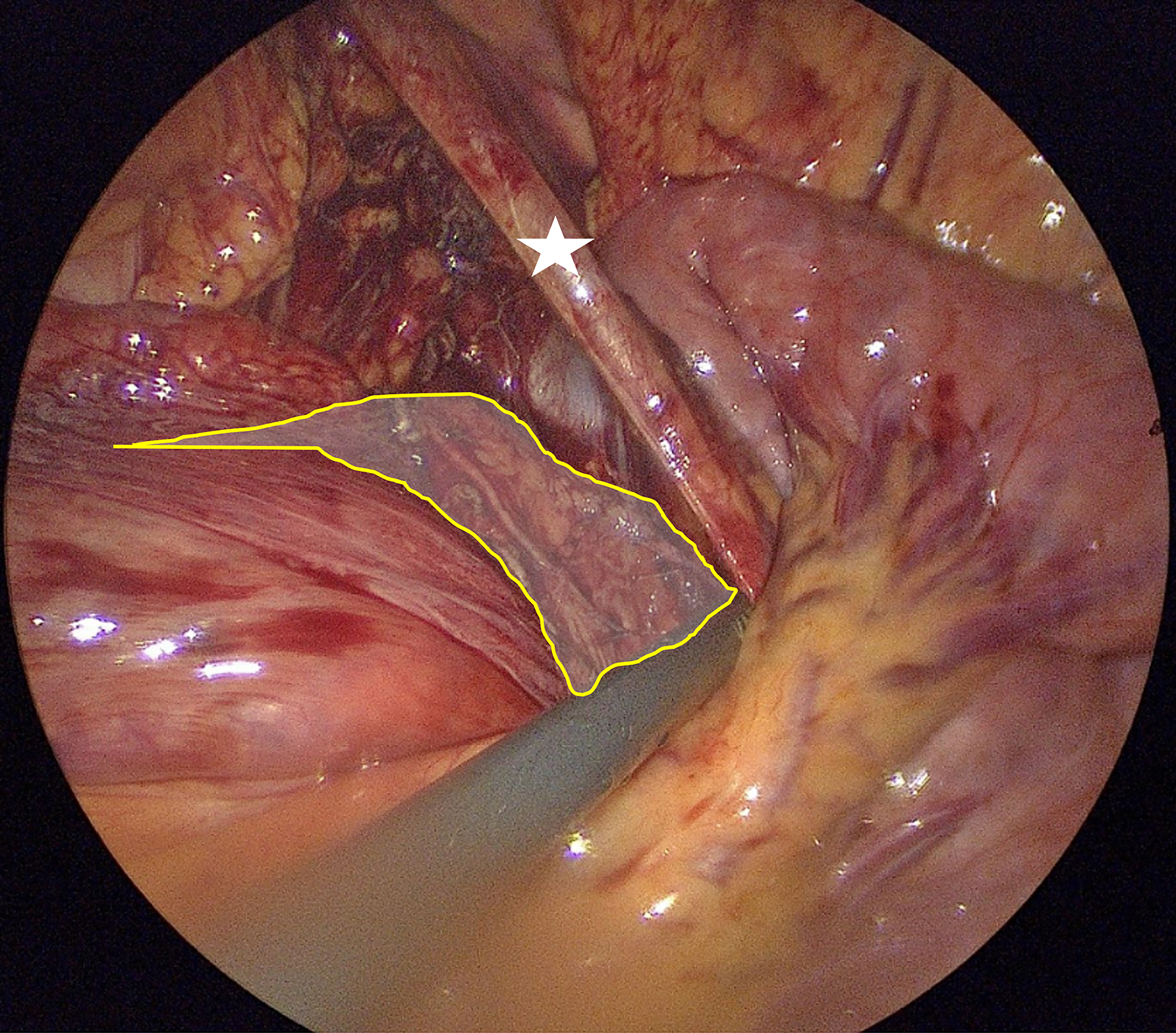
Intraoperative photo showing completion of laparoscopic duodenal lowering. The SMA is shown (white star). After dissection, the duodenum is lowered below the angle of the SMA, avoiding any compression (highlighted yellow area). SMA, superior mesenteric artery.
Laparoscopic LDJ
If laparoscopic DL was unsuccessful, our next approach was LDJ. We approached the next operation with the same setup as before, except we introduced a 12 mm port in the umbilicus. We divided the bowel ∼6–8 cm from the ligament of Treitz with a stapler. Next, we used a LigaSure to resect the mesentery of the proximal jejunum/distal duodenum back to near the head of the pancreas. We brought the distal limb of jejunum retrocolic for a stapled anastomosis to the duodenum. The jejunal limb was placed to the left of the duodenum, and then the jejunal end was curved back so both staple lines face the camera (Fig. 2). We opened the corners of each staple line and fired the stapler twice longitudinally and transected the common opening. This process eliminates the “C” loop of the duodenum, ensuring that the SMA angle and point of obstruction are bypassed.
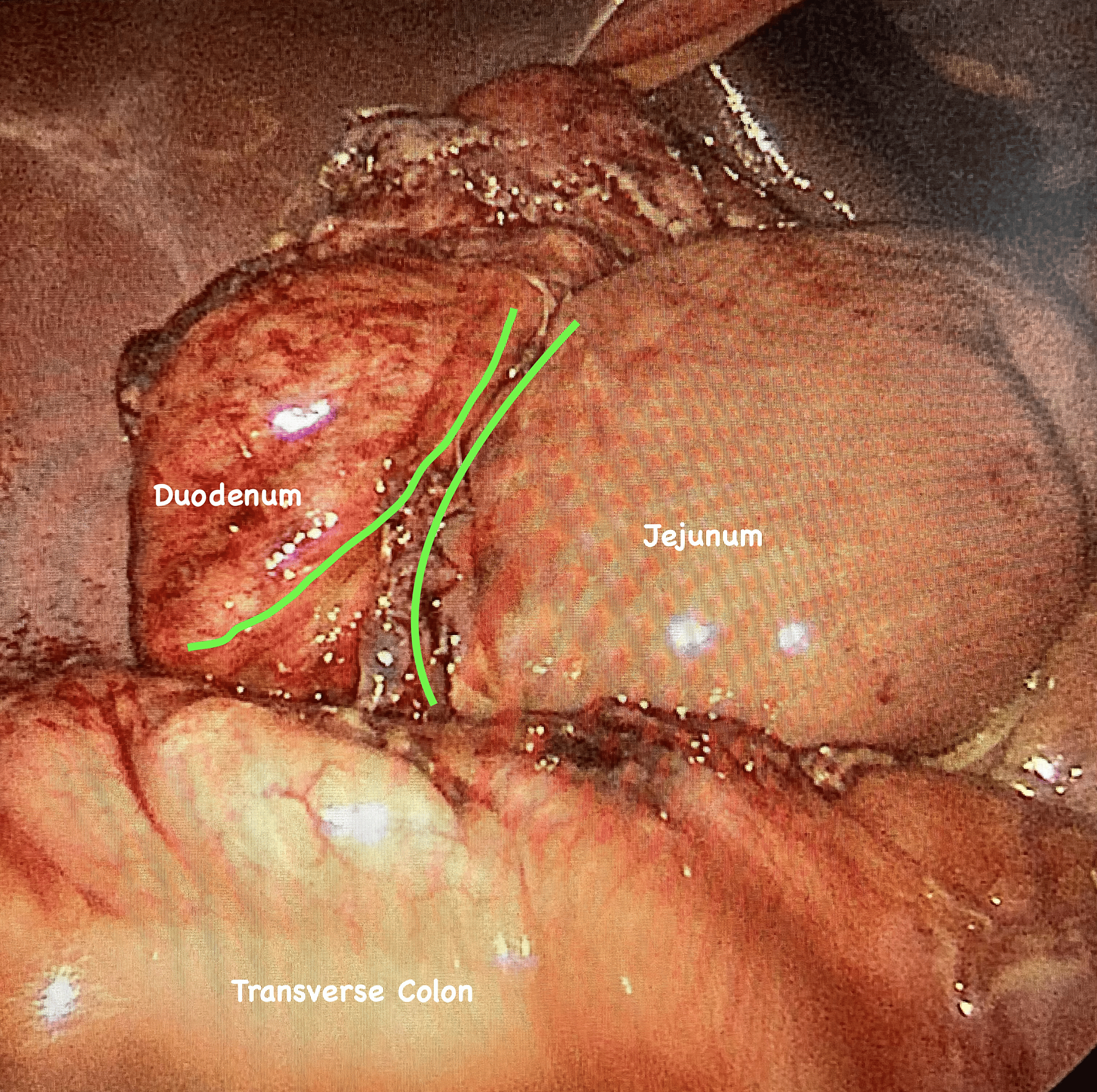
Intraoperative photo showing the retro-colic lay of the duodenum and jejunum, lining up the staple lines (green lines) prior to completing stapled anastomosis.
Case 1
A 16-year-old female diagnosed with SMA syndrome 2 years prior to surgical evaluation after being diagnosed by CT angiogram (CTA) for progressive emesis. She was treated conservatively with nasojejunal (NJ) feeds for ∼1 month and then was able to have the NJ tube removed and tolerate PO intake. She had a relapse 1.5 years later, eventually requiring replacement of the NJ tube, and Esophagogastroduodenoscopy (EGD) at that time showed pulsatile extrinsic compression of the third portion of the duodenum and duodenitis (Fig. 3). Repeat CTA showed a severely narrowed aortomesenteric angle of 10° (Fig. 4). She was tolerating NJ feeds but only able to eat soft candies prior to surgery. She underwent a laparoscopic DL procedure without complication. She was unable to be advanced to solid foods during admission and required the NJ tube to be replaced on post-operative day (POD) 5 and was discharged on NJ feeds with a clear liquid diet. Patient returned 4 months later and underwent laparoscopic LDJ without complication and was discharged on regular diet on POD 6. She presented to the emergency department 3 weeks after LDJ and was diagnosed with small bowel obstruction due to stricture at the LDJ anastomosis. She underwent EGD with serial dilations of this stricture a total of four times over the next 3 months. She was tolerating a regular diet after her fourth dilation and has not required intervention since.
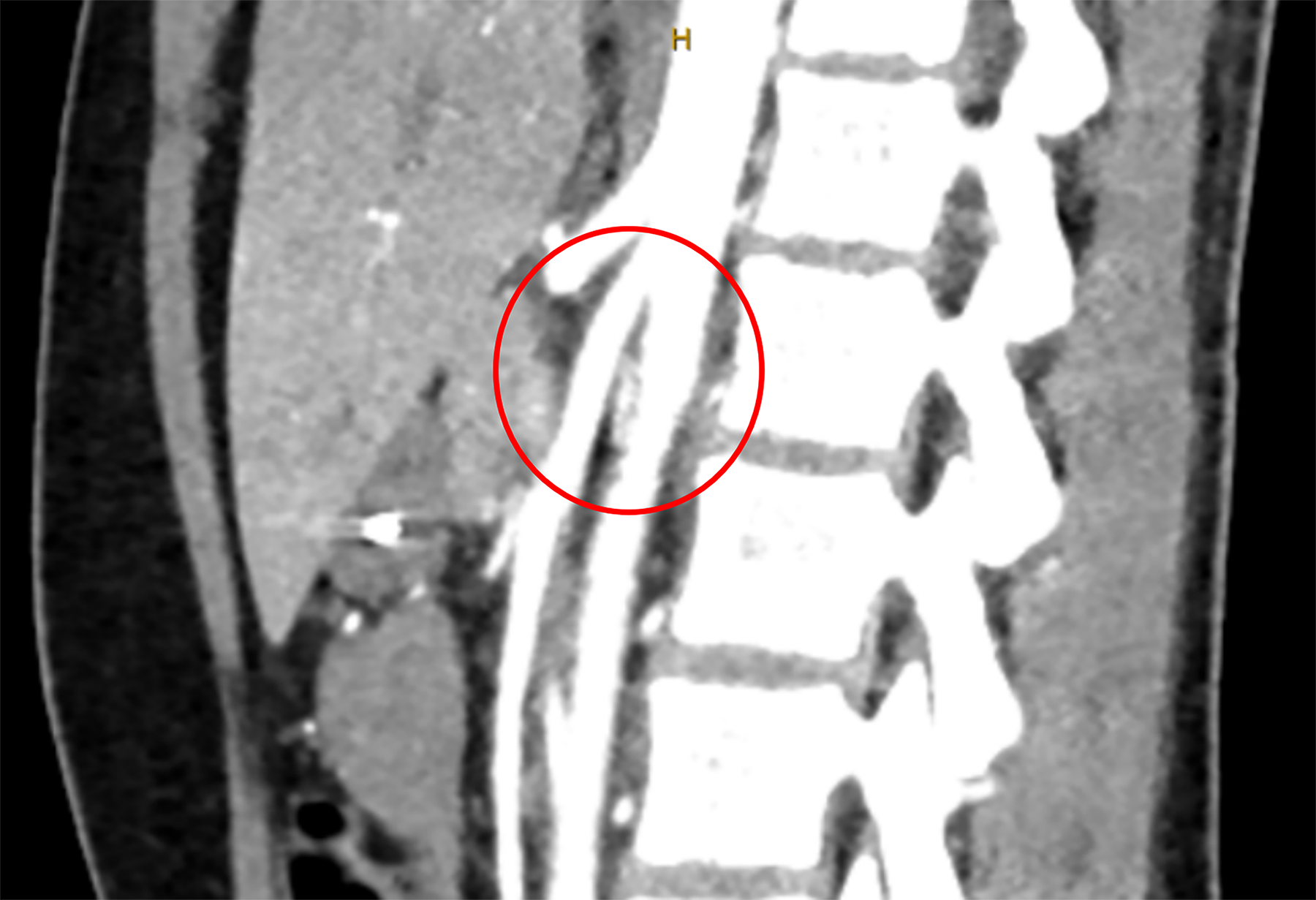
Preoperative CT abdomen showing narrowed aorto-SMA angle with compression of the duodenum (red circle). SMA, superior mesenteric artery.
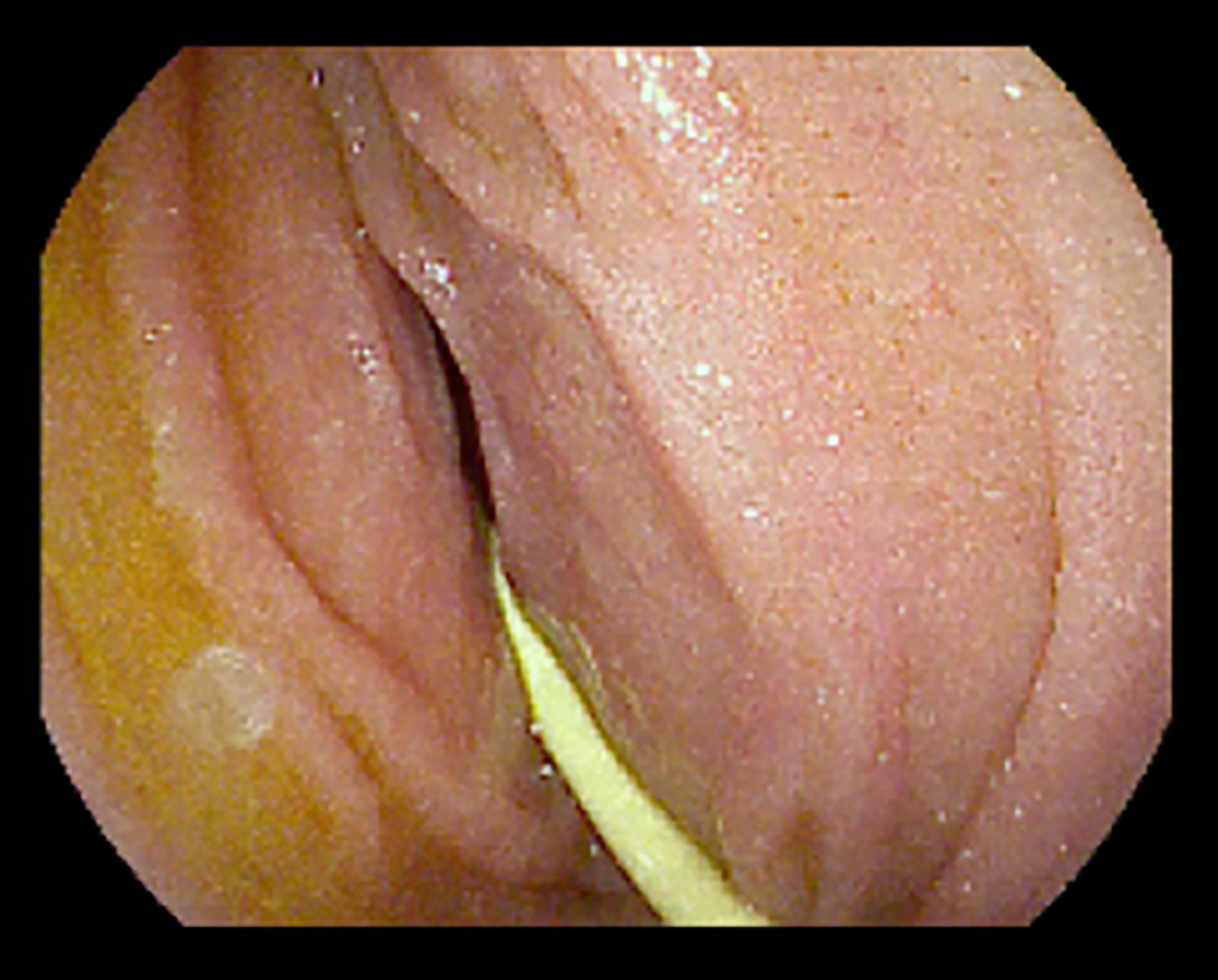
Preoperative endoscopy with the nasojejunal tube in place at the third portion of the duodenum showing external compression of the duodenum by the SMA with narrowing of the bowel lumen. SMA, superior mesenteric artery.
Case 2
Sixteen-year-old female presenting with 4 months of progressive abdominal pain, nausea, and disruptive borborygmi—a loud and repetitive gurgle every ∼10 seconds, preventing her from attending class. A CT abdomen was obtained to investigate her symptoms and revealed her aortomesenteric angle was 13°. The patient tolerated a regular diet. She underwent laparoscopic DL without complication and was discharged POD 1. She had resolution of symptoms for ∼4 weeks, and then symptoms recurred, prompting laparoscopic duodenectomy (distal second to fourth portion) and LDJ 2 months after DL. She did well without symptoms for 5 months, but again, her symptoms, including bloating, abdominal pain, and borborygmi, recurred. Evaluation, including an upper gastroenterology (GI) series and EGD, revealed a widely patent DJ anastomosis with easy passage of scope and contrast; however, it was noted that the patient’s stomach was abnormally large and J-shaped, extending down into her pelvis (Fig. 5).
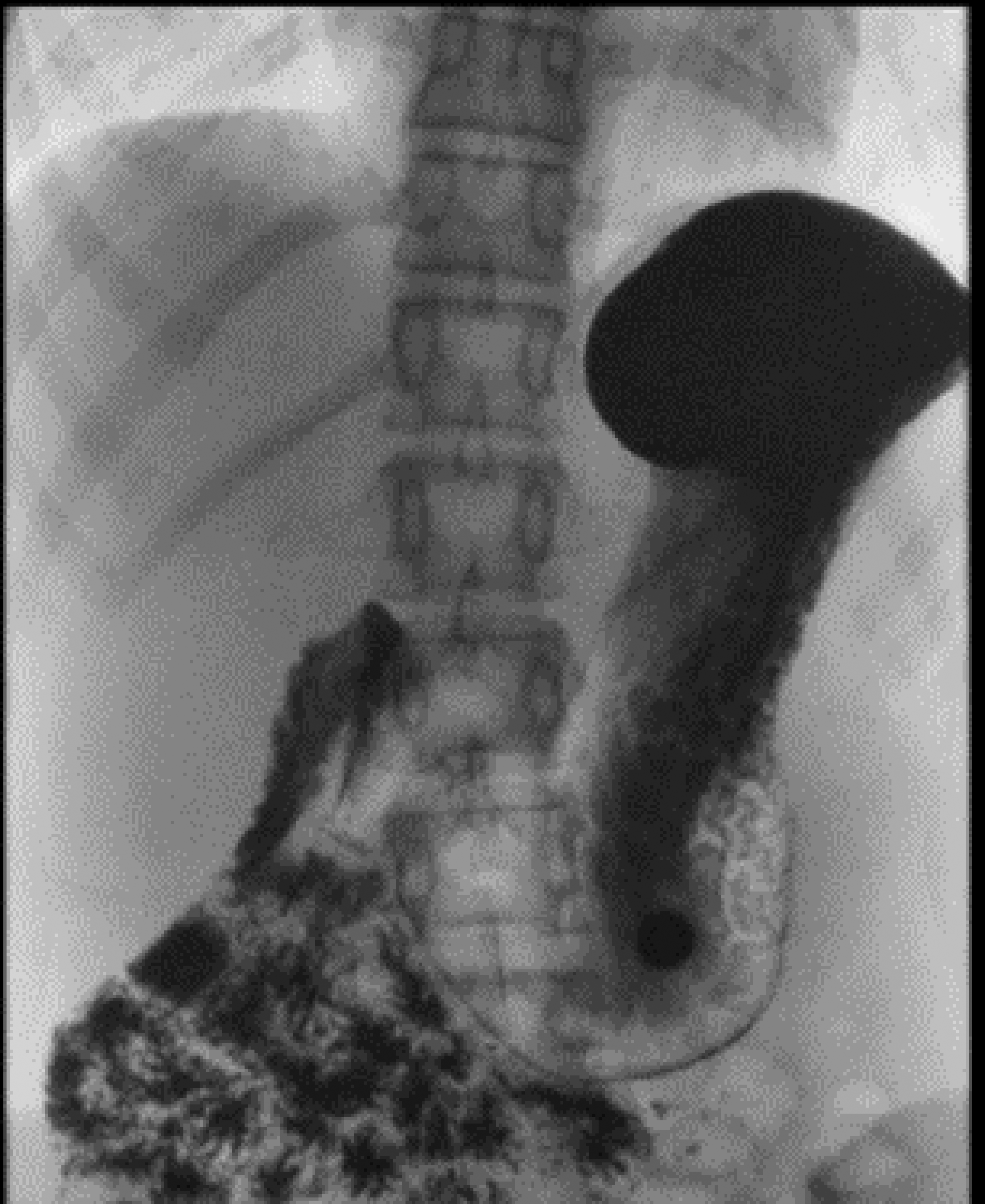
Upper GI contrast study showing passage of contrast through prior duodenojejunal anastomosis. The stomach is large and abnormally J-shaped.
Case 3
A 17-year-old female presents with 5 years of daily nausea, intermittent abdominal pain, lightheadedness, and more recently drastic weight loss over the last 6 months. She was originally diagnosed with cyclic vomiting syndrome, but after her weight loss, further evaluation was pursued, and CTA revealed an aortomesenteric angle of 16°, and the patient was referred. She opted for surgical management and underwent laparoscopic DL 1 month after surgical consultation. She discharged on POD 1 with full relief of symptoms and remained symptom-free on outpatient follow-up 4 weeks later.
Case 4
A 17-year-old male presents with rapid-onset upper abdominal pain, distension, and several episodes of emesis. Of note, the patient was preparing to play collegiate basketball and had intentional weight loss of ∼40 lbs from diet/exercise over the past 5 months. A CT scan revealed a severely distended stomach and portion of the duodenum with an aortomesenteric angle of 12° (Fig. 6). NJ tube placement for decompression greatly improved symptoms, and the patient was discharged from the index admission in 10 days on tube feeds with a follow-up surgery clinic appointment 2 days later. Patient elected to pursue surgical management and underwent DL 2 weeks later (25 days after onset of symptoms). He was discharged on the same day as surgery, and on a 4-week follow-up, he had complete resolution of symptoms.

CT showing severe gastric distension with decompressed distal small bowel from rapid onset SMA syndrome. SMA, superior mesenteric artery.
Results
Briefly, 22 patients underwent surgical management for SMAS during this study period. The majority of patients were female (n = 19, 86%), and the median age at the time of surgery was 17 years (IQR: 16.0, 18.4). The median measured aorto-SMA angle was 16° (12, 20), with 3 patients having an aorto-SMA angle as narrow as 10°.
All patients reported nausea as a symptom, with the next most common symptoms being vomiting (73%), abdominal pain (68%), and weight loss (45%). The most common co-morbidities included Ehlers–Danlos syndrome (23%), postural orthostatic tachycardia syndrome (18%), median arcuate ligament syndrome (14%), and Nutcracker syndrome (14%). Moreover, 13 of the 22 patients were receiving some form of post-pyloric tube feeds, either through the NJ tube or surgical gastrojejunal (GJ) tube prior to their operation.
In total, 20 patients underwent laparoscopic DL, and 2 patients underwent laparoscopic LDJ, as they had previously undergone surgical procedures for SMAS at another institution (open duodenal de-rotation, open DL, and median arcuate ligament release). Of the 20 patients who underwent DL, 12 patients (60%) had resolution of their symptoms. Two of these patients had recurrence of symptoms within 6 months and underwent subsequent LDJ. Of the 8 patients without improvement after DL, 2 patients underwent subsequent LDJ with improvement of symptoms. Median follow-up for all patients was 51 days (33, 321). On both univariate and multivariate statistical analyses, having a diagnosis of Ehlers–Danlos syndrome was predictive of failure to achieve symptom resolution after DL (P = .004). No other clinical or demographic characteristics were found to be predictive of successful resolution of symptoms from surgery.
Of the 6 patients without improvement after DL, 1 was considering DJ in the future, 1 patient was diagnosed at another facility with exocrine pancreas dysfunction without future plans for surgery, 1 patient was undergoing manometry studies at another facility, and 3 patients were lost to follow-up.
Discussion
SMAS is a rare cause of proximal small bowel obstruction in children, and the need for surgical intervention is even more uncommon. For that reason, the literature on optimal surgical management for these complex patients is limited. Most studies consist of small cohorts of patients and limited long-term follow-up.
The surgical approach to SMAS has evolved from open gastrojejunostomy to now include several laparoscopic options, including LDJ and the Strong procedure (release of the ligament of Treitz with complete duodenal de-rotation). The success rate of these procedures is reportedly around 80%, with most surgeons preferring LDJ.5,6 However, potential complications of LDJ include issues with the anastomosis, such as leaks or strictures and blind loop syndrome from bypassing a portion of the duodenum. 2 While the Strong procedure avoids the need for creating an anastomosis, this technique requires extensive mobilization of the duodenum and entire bowel, risking subsequent volvulus. 7 For these reasons, we developed the laparoscopic DL technique as a less invasive and more conservative initial surgical approach. This operation requires no anastomosis and uses a simple mobilization of the duodenum with a median operation time of 40 minutes.
In our previous report, DL resulted in symptom relief in over half of patients with a recurrence rate comparable to the Strong procedure, making it an effective first option for patients with SMAS. 2 In our updated cohort of patients in this study, these findings remained consistent with 60% of patients having resolution of symptoms after DL, with 17% of these patients having eventual recurrence of symptoms within 6 months. This updated study also highlights the safety of the DL technique, as no operative complications were recorded. Patients had a median hospital LOS of 29 hours (interquartile range: 23, 76), and average follow-up after discharge was 12.6 months. We present four of our cases to highlight the variation in outcomes.
Overall, these cases highlight the complexity of SMA syndrome patients and some of the challenges of surgically managing them. While the diagnosis of SMA syndrome is straightforward with imaging, the wide array of possible symptoms could be representative of other co-morbidities. A collaborative approach to these patients with a multidisciplinary team is paramount to optimize outcomes.
When the diagnosis is made, patients undergo nonoperative management with nutrition support to regain weight and resolve symptoms. In situations where patients fail nonoperative management, have a recurrence of symptoms or, for some reason, are not comfortable with the extended length of time of nonoperative treatment, surgical intervention is offered. The diagnosis of SMA syndrome is confirmed with an SMA angle of <25° on CT imaging and the presence of symptoms, but we do not use a more specific cutoff of SMA angle when selecting patients for surgical intervention. The severity of angle narrowing was not predictive of successful response to surgery. After completion of DL, we visualize intraoperatively that the duodenum is lowered away from any potential compression by the SMA, and thus success would be expected to be independent of angle severity. In cases where patients fail treatment by DL, our next approach is LDJ, in which we resect the involved portion of the duodenum to assure there is no longer a “C-loop” remaining for future symptoms.
We observed a statistically significant failure rate after DL in patients diagnosed with Ehlers–Danlos syndrome. All 4 patients (100%, P = .004) had persistent symptoms of abdominal pain and nausea/vomiting after DL. Moreover, 2 patients proceeded with subsequent LDJ, and both continue to be symptomatic after surgery, with 1 patient reporting improvements in abdominal pain but still being unable to tolerate PO intake. Ehlers–Danlos syndrome involves mutations in collagen synthesis/processing that can have a wide variety of phenotypic presentation. 8 Some of the more common manifestations of Ehlers–Danlos syndrome include delayed wound healing and atrophic scarring. 9 Other manifestations of tissue collagen dysfunction can include hernias and prolapse (vaginal and rectal).10–11 Although we did not observe any issues with postoperative wound healing in these patients, it is possible that collagen dysfunction and wound healing played a role in the failure to resolve symptoms after surgery. When the dissection is completed and the duodenum falls away from the SMA pedicle, we expect some degree of scarring to occur in that dissection plane to help keep the duodenum in its lowered position. If these patients do not form adequate postoperative scar tissue, then this could potentially contribute to the observed failure rate.
No other clinical characteristics were predictive of surgical success but could be due to the limited sample size of this rare problem. Other studies have suggested potential causes of treatment failure, such as neuropathic components of the disease or concomitant motility disorders.9–11 While some of our patients were also diagnosed with gastrointestinal motility disorders (both in the pre- and postoperative periods), we are not able to draw conclusions with our current cohort of patients.
Limitations include that this is a retrospective review and a small patient cohort. Given the rarity of this problem and the need for surgical management, we have patients that travel from various parts of the country for their surgery, which limits the ability for consistent follow-up. However, compared with the available literature, this is a significant number of pediatric and young adult patients with SMAS managed surgically and continues to highlight DL as a viable option that is safe and effective.
Conclusion
The more conservative DL can be an efficacious first step when approaching surgical management of SMAS, as it continues to have an adequate rate of success with minimal operative risk. Patients with SMAS are a complex population, and for those requiring surgical management, further study is warranted to characterize which patients are more likely to fail operative intervention or require repeat operations.
Authors’ Contributions
S.S. and S.S.P.: Study concept and design, analysis and data interpretation, and critical revision. S.S.: Data acquisition and drafting of the article.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interests or competing interests to declare.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.