
Abstract
Introduction:
Laparoscopic sleeve gastrectomy (LSG) is currently the most frequently performed bariatric surgery method worldwide. However, it includes the longest staple line (SL), remaining the major source of complications, with leak rates of 0.7% up to 5.7%. Because leaks occur just below the esophagogastric junction in up to 90% of cases, SL reinforcement is widely used, though its effect on failure locations remains insufficiently characterized.
Method:
This ex vivo study evaluated whether SL reinforcement affects mechanical resistance and leak localization. Sixty human LSG specimens (20/group) from routine resections were randomized to oversewing (Group 1), through-through suturing (Group 2), or no reinforcement (Group 3), using 3/0 polypropylene. Specimens were tested within 40 minutes by intraluminal insufflation via Veres needle and manometer while submerged; burst pressure and leak site were recorded.
Results:
Baseline characteristics were comparable across groups (P > .05). Leaks occurred distally in 70% and proximally in 30% of specimens. Reinforcement affected leak topography (P = .011): Distal leaks predominated in Groups 1 (85%) and 2 (80%), while Group 3 concentrated proximally (55%). Burst pressure differed significantly (P = .001): Highest with oversewing (mean 116.84 ± 16.35; median 120 [110–130] mm Hg), intermediate with through-through sutures (78.52 ± 14.27; median 80 [65–90] mm Hg), and lowest without reinforcement (41.00 ± 9.26; median 40 [30–50] mm Hg).
Conclusion:
Oversewing provides the greatest pressure safety window and shifts failure from the high-risk proximal region to distal SL, suggesting reinforcement strategies should anticipate distalized leak patterns, while in vivo validation remains necessary.
Introduction
While laparoscopic sleeve gastrectomy (LSG) was initially conceived as the first phase of a two-stage bariatric intervention to minimize surgical complications in high-risk, super-obese patients, studies have demonstrated its efficacy as a standalone procedure.1,2 The preservation of gastrointestinal continuity and absence of anastomosis contribute to the ease of execution of LSG. LSG has emerged as the most common bariatric surgical procedure globally over the past decade. Owing to technical intricacies, the extended staple line (SL) remains the main complication, with leakage rates between 0.7% and 5.7%. 3 This complication affects approximately 10% of patients following revision surgery for re-gain. 4
When stapling to create a smaller sleeve gastrectomy, passing close to the incisura angularis can cause functional obstruction in addition to the physiological obstruction mechanism of the pylorus. 5 The resulting intragastric hypertension constitutes a risk factor for leakage. Leaks can occur along the SL but typically appear below the esophagogastric junction (EGJ) in 90% of cases. 6
Studies have reported that different reinforcement materials and techniques used in the SL may increase resistance to intragastric pressure and reduce leakage risk.7,8 For ethical reasons, determining reinforcement techniques’ resistance to high pressure in vivo is difficult; however, burst pressure can be measured ex vivo. Additionally, how different reinforcement techniques affect leakage formation at the SL requires further investigation.
The aim of the present study is to evaluate the effects of different SL reinforcement methods (unreinforced, oversewing, and through-through) on mechanical strength (burst pressure) and topographic distribution of leak localization (proximal and distal) in ex vivo LSG specimens.
Method
All procedures were carried out in accordance with ethical standards and the 2008 revision of the 1975 Helsinki Declaration. Informed consent was obtained from all participants. The sample size was determined prior to the study using an a-priori power analysis based on previous literature.8,9 To achieve a statistical power of 80% (1-ß = 0.80) with a significance level of à = 0.05 and an anticipated large effect size (f = 0.40), a minimum total sample size of 52 patients (approximately 17–18 per group) was required. Thus, our inclusion of 60 patients (n = 20 per group) was deemed sufficient to provide adequate statistical power. Three groups were formed using simple randomization (coin tosses). Group 1 samples were reinforced with the SL oversewing suture technique, Group 2 with the through-through suture technique, and Group 3 received no reinforcement. Specimens were removed from the abdomen within 40 minutes after resection, and those with intact tissue integrity were included. A Veres needle with a cuff to create pressure at the distal end and a manometer were placed 0.5 cm distal to the specimen’s end. The Veres needle entry site was narrowed with a suture to prevent air leakage. Specimens were placed in a water-filled transparent container to visualize leakage. Intraluminal pressure was gradually increased using a manual insufflator, and pressure was monitored using a manometer. The pressure at which air leaked from the SL was recorded for each specimen. The leakage site was categorized as proximal or distal based on its anatomical location along the SL. This study used samples sent for postoperative pathology without additional patient procedures. The SL formed in the patient’s stomach was routinely reinforced with 3/0 polypropylene (Prolene; Doğsan, Turkey) sutures using different patterns per group. No interventions that would affect the pathological examination, damage the structure, or cause tissue loss were performed.
Statistical analysis
Statistical analysis used NCSS 2007 (Kaysville, Utah, USA). Descriptive statistics (mean, standard deviation, median, frequency, percentage, minimum, and maximum) evaluated study data. Data normality was tested using the Shapiro–Wilk test and graphical examinations. For normally distributed groups, One-way Anova and Bonferroni tests were used; for nonnormal distributions, Kruskal-Wallis and Bonferroni-Dunn tests were applied. Qualitative data were compared using Pearson’s Chi-Square and Fisher–Freeman–Halton tests. Statistical significance was P < .05.
Results
The study was conducted between 2023 and 2024 at the Gastroenterology Surgery Clinic of Sakarya University Hospital, with a total of 60 specimens, 20 in each group.
The study included 53 patients (88.3% female and 11.7% male). Patient ages ranged from 26 to 40 years (mean 33.48 ± 9.76). Average measurements were a height of 162.62 ± 7.24 cm, a weight of 120.33 ± 13.77 kg, and a BMI of 45.44 ± 4.17 kg/m2. Age, sex, height, weight, and BMI measurements showed no statistically significant differences between groups (P > .05; Table 1).
Evaluation of Descriptive Characteristics by Groups
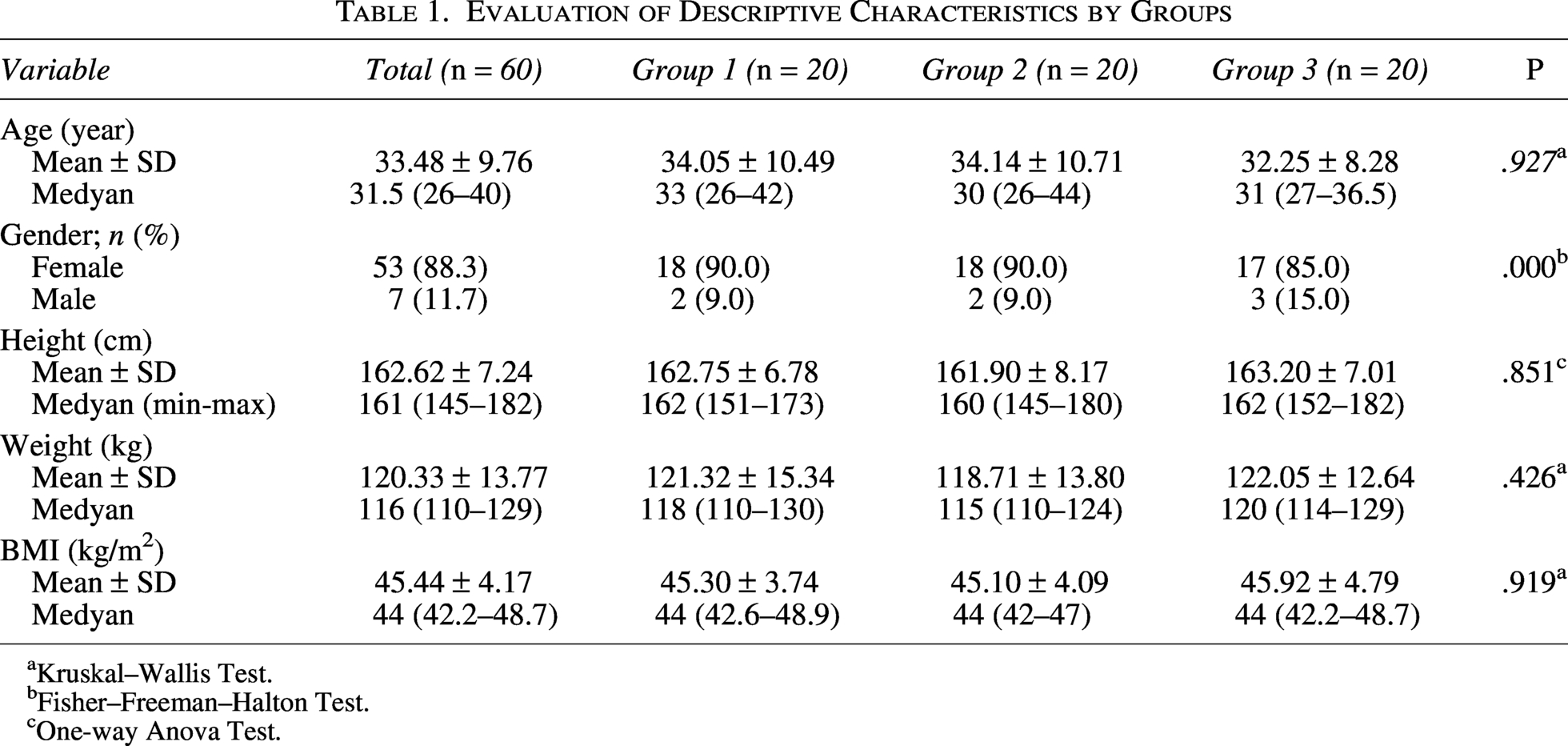
Kruskal–Wallis Test.
Fisher–Freeman–Halton Test.
One-way Anova Test.
In 30% of the leaks (n = 18), the leak occurred in the proximal region, and in 70% (n = 42), it occurred in the distal region. The mean leak pressure was 78.50 ± 33.90 mmHg (Table 2). There was a statistically significant difference in mean leak pressure between the three groups (P < .001). In suture groups 1 and 2, the vast majority of leaks (85% and 80%, respectively) occurred in the distal region, whereas in the control group (Group 3), leaks were more concentrated in the proximal region (55.0%). The suture technique applied was found to have a statistically significant effect on the location where the leak occurred (P = .011, P > .05).
Evaluation of Clinical Characteristics by Groups
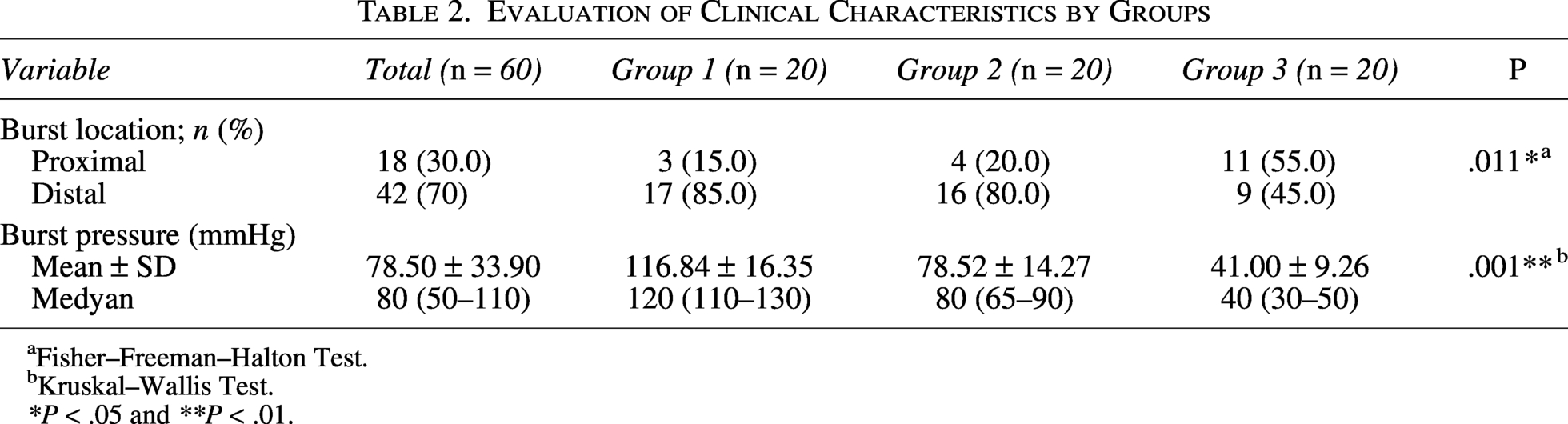
Fisher–Freeman–Halton Test.
Kruskal–Wallis Test.
*P < .05 and **P < .01.
A significant difference was observed between the leak pressures of the groups (P = .001; P < .01). Pairwise comparisons were performed to determine which group caused the significant difference; the pressure value of Group 1 was found to be higher than those of Groups 2 (P = .004) and 3 (P = .001) (P < .01). The pressure value of Group 2 was also found to be higher than those of Groups 3 (P = .001; P < .01).
Discussion
Leakage from the SL following LSG is considered the most concerning complication. Reinforcement of the SL through various methods enhances its structural integrity. Nevertheless, this reinforcement does not entirely eliminate the risk of leakage; rather, it modifies the dynamics of its occurrence. Reinforcing specific areas alters the pressure distribution along the SL, resulting in a scenario in which leakage may occur at a different location and under different pressure conditions compared with an unreinforced segment.
This study demonstrated that reinforcing the SL with sutures in LSG enhances its mechanical integrity. Furthermore, the choice of suture reinforcement technique can influence the specific anatomical region where leakage is likely to occur along the SL. The oversewing technique, in particular, provided substantial evidence of its ability to achieve the highest burst pressure and to shift the leakage localization from the proximal to the distal area. These topographical changes in the leakage point may also necessitate variations in the clinical approach.
Assessing the resistance of reinforcement techniques applied to SL under high pressure in vivo presents ethical challenges; however, resistance can be evaluated by measuring burst pressure ex vivo. Marie et al. 10 conducted an experimental study involving total gastrectomy and ex vivo sleeve gastrectomy in pigs. They observed that leakage frequently occurred at an average pressure of 26.3 ± 5.3 mm Hg in the proximal third of the SL when the intraluminal pressure increased within the sleeve stomach. Conversely, Natoudi et al. 11 reported that most leaks in the SG pig model occurred near the EGJ at a pressure of 24.5 (3–75) mm Hg. In ex vivo studies, burst pressure may exceed that under physiological and even pathological conditions. Yehoshua et al. 12 demonstrated in their in vivo study that intragastric pressure in a normal sleeve stomach ranged from an average of 18 mm Hg (basal) to 43 mm Hg (maximum). In this study, the median pressure at which leakage occurred was 40 mm Hg (30–50) in the group without reinforcement, 80 mm Hg (65–90) in the group reinforced with the through-through suture technique, and 120 mm Hg (105–130) in the group treated with the oversewing suture technique. The rupture pressure in SL reinforced with oversewing sutures was significantly higher than that in the other groups. The rupture pressure reaching 120 mm Hg with oversewing significantly reduces the risk of leakage under physiological conditions, according to the data from Yehoshua et al. 12
Tolone et al. 8 reported that the “chamber-like space” created by inverting the serosa with sutures functions as a secondary barrier to intraluminal pressure, and overcoming this barrier necessitates five times more pressure. In this study, pressures approximately three times higher than those in the nonreinforced group were recorded in the reinforced group (40 mm Hg → 120 mm Hg). This difference establishes a critical window for tissue healing, potentially offering a clinically significant advantage in preventing early postoperative complications, such as peritonitis. The consistency of these findings with previous ex vivo studies, including those by Karakoyun et al. 13 and Gönüllü et al., 9 further substantiates the reliability of suture reinforcement as an effective technique for enhancing the integrity of the SL. Both oversewing sutures and other suture patterns demonstrated a significant increase in burst pressure, underscoring that the decisive factor in augmenting the durability of the SL is the reinforcement method rather than a specific suture pattern. However, unlike other studies, this study observed not only an increase in pressure but also topographical displacement in the leakage area along with the suture pattern.
Post-LSG leakage can manifest at any location along the SL, but it predominantly occurs just below the fundus in 90% of cases. 6 This phenomenon is attributed to increased intragastric pressure resulting from ischemia and reduced peristalsis.14,15 Furthermore, this region demonstrates diminished resistance to elevated intraluminal pressure due to the thinner gastric wall layers. 16 In an ex vivo study, Timucin Aydin et al. 17 compared unreinforced SL with three different SL reinforcement techniques (Peri-Strip Dryon, fibrin glue, and suture) in sleeve gastrectomy samples. The burst pressure of the unreinforced group was significantly lower than that of the reinforced groups, with all leaks occurring in the proximal third of the SL. This observation suggests that the higher incidence of leaks in the proximal stomach may be due to tissue ischemia caused by the ligation of short gastric arteries during surgery, in addition to increased intragastric pressure. 17 In accordance with the Delphi consensus, it is recommended that resection be performed 1 cm lateral to the his (esophagogastric angle) of angle to protect the proximal stomach from ischemia. 18
Additionally, the thickness of the stomach varies along the SL. Anatomically, the gastric wall thickness increases from the lesser curvature to the greater curvature and from the fundus to the antrum. 19 Variations in tissue elasticity across different stomach regions and the differing expansion capacities of areas such as the fundus and antrum limit the applicability of ex vivo studies to real-life scenarios. Therefore, it is not feasible to extend beyond mechanical studies such as burst pressure measurement. Reinforcing the SL with sutures enhances the proximal SL, which was previously the most vulnerable point for leakage due to mechanical stress and ischemic factors. 20 This reinforcement distributes stress more evenly and effectively seals the SL, particularly near the EGJ, thereby fortifying the proximal area, which was previously weak and a potential risk for leakage. 21 This explanation aligns with clinical studies indicating that suture reinforcement of the SL reduces proximal leak rates.16,22,23 Although studies suggest that reinforcement applied to the SL increases safety near the hiatus, data regarding the localization of leakage under higher pressure conditions, including ex vivo studies, are limited. Suture reinforcement prevents leaks in the proximal SL at lower pressures by strengthening this region; however, leaks can still be observed in this area only under higher intragastric pressure.24,25
In this study, leakage was more frequently observed in the proximal section of the group without reinforcement, in the distal section of the through-and-oversewing groups, and at increasing pressures. This suggests that suture reinforcement shifts the weakest point in the SL from proximal to distal, thereby transferring the risk of leakage distally. The distal SL, which was previously subjected to higher lumen pressures that would cause proximal leakage, became the new site of leakage. This finding underscores that reinforcement enhances the overall integrity of the SL but does not completely eliminate leaks; rather, it alters the location and pressure at which leaks occur. Reinforcing the SL with the oversewing suture technique shifts the typical leak point from the proximal portion near the EGJ to the distal portion. 9 This indicates that postoperative monitoring and diagnostic attention should be adjusted accordingly, focusing not only on the proximal SL but also on the distal regions where leaks may occur under higher pressures. The change in leak location and pressure suggests a complex interaction between the mechanical properties of the reinforcement and the SL, highlighting the need for a comprehensive leak prevention approach that accounts for these changing stress patterns. Therefore, reinforcement increases durability and resistance to leakage but also necessitates careful evaluation of the new pressure points that may result. Considering the change in leakage location in the study, in clinical practice, reinforcement approaches tailored to the patient’s risk factors and anatomical characteristics may be beneficial by optimizing both proximal and distal SL integrity. Clinically, this change may affect patient outcomes by potentially reducing the frequency and severity of leaks in sensitive areas, thereby reducing related complications such as infection, delayed healing, or the need for reoperation.23,24 Proximal leaks are the most challenging to treat due to their high-pressure nature and ischemic characteristics. The study by Sakran et al. 26 clearly demonstrated that proximal leaks lead to a more complex clinical picture (septic shock, multiple organ failure, and prolonged hospital stay). The migration of the leak distally creates a technically more manageable area for endoscopic stenting, percutaneous drainage, and even surgery. 27 However, the emergence of leaks in new areas or under different pressure conditions can lead to unforeseen difficulties in postoperative management, and this change may fundamentally alter leak management strategies, requiring specialized intervention approaches.
The present study has some limitations. First the sample size is small, and second, we cannot definitively claim that these ex vivo results will yield similar in vivo results. However, we believe that we have created a new and different perspective for future studies in this area.
Conclusion
Oversewing suture technique ex vivo showed superior mechanical strength in reinforcing the SL compared with other methods. This technique enhanced the SL mechanical strength and modified the anatomical distribution of leaks, shifting their frequency from proximal to distal regions. These findings have significant implications, indicating that reinforcement strategies should address both overall leakage risk and anticipated changes in leak localization that could impact postoperative management. The distal shift of leakage zones may affect clinical protocols, imaging focus, and intervention planning. Therefore, understanding how different reinforcement techniques alter the mechanical and topographical properties of the SL is essential. Although these ex vivo results are promising, the biological response to reinforcement with the oversewing suture technique and its long-term clinical outcomes must be validated using in vivo models consisting of larger series. Integrating biomechanical data with clinical evidence will facilitate the development of optimized reinforcement protocols that enhance SL durability and the effectiveness of postoperative care.
Authors’ Contributions
K.K., A.Y., and G.F.: Consept and design; A.Y. and K.K.: Supervision; G.F. and O.İ.: Providing; G.F. and E.G.: Data colectiom or processing; G.F.: Analysis or interpretation, G.F. and O.İ.: Literature review, G.F.: Article writing, A.Y. and K.K.: Critical review. All authors have read and approved the final version of the article to be published.
AI Statement
The authors used Artigicial intelligence (AI) and AI-assisted technologies (Grammarly and MS Word Editor) in the writing process. These technologies improved the readability and language of the work. Still, they did not replace key authoring tasks such as producing scientific or medical insights, drawing scientific conclusions, or providing clinical recommendations. The authors are ultimately responsible and accountable for the contents of the whole work.
Consent for Publication
The original article is not under consideration by another publication, and its substance, tables, or figures have not been published previously and will only be published elsewhere.
Data Availability
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethical Declaration
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Our institution has granted ethics committee approval with protocol number E-16214662-050.01.04-237374. As this was retrospective research, no informed consent was obtained from participants.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
There is no specific funding related to this research.