
Abstract
Background:
Intrathoracic wrap migration (IWM) is a relatively infrequent but clinically significant complication following laparoscopic fundoplication (LF). This meta-analysis aimed to synthesize the available evidence comparing the incidence of IWM after primary cruroplasty with or without mesh reinforcement.
Methods:
A systematic search of PubMed, Embase, Scopus, Web of Science, and Cochrane Library was performed through February 2026. The primary outcome was the incidence of IWM following LF with mesh reinforcement versus simple suture repair. Secondary outcomes included operative time and postoperative dysphagia. The random-effects model was used to calculate the pooled odds ratios (OR) and mean difference (MD) with 95% confidence intervals (CI).
Results:
Of 507 studies screened, 7 cohort studies comprising 1171 patients were included. The mesh group represented 43.5% of patients (n = 510). Overall, 43% were female (n = 504) with a mean age of 54.3 years. There was no significant difference in age or sex distribution between groups. Mesh reinforcement during LF was associated with a significantly lower risk of IWM (OR = 0.21; 95% CI = 0.10 to 0.42; I2 = 0%). Sensitivity analyses confirmed the robustness of the IWM findings across prospective studies and polypropylene mesh subgroups. There was no statistically significant difference in operative time (MD =+14.22 minutes; P = .05). Mesh reinforcement was associated with a higher risk of dysphagia at 3 months (OR = 2.22; 95% CI = 1.60 to 3.09; I2 = 0%), with no significant difference observed at 1-year follow-up.
Conclusion:
Mesh reinforcement during LF was associated with a significantly lower risk of IWM compared with simple suture repair, without significant differences in operative time and long-term dysphagia.
Keywords
Introduction
The laparoscopic approach to antireflux surgery has revolutionized surgical treatment for gastroesophageal reflux disease and hiatal hernia repair (HHR) since it was introduced in the early 1990s. 1 The standard surgical technique involves reduction in hernia contents, closure of the hiatal defect, and fundoplication. However, primary suture repair of the hiatus alone has been associated with an increased risk of anatomical recurrence, sometimes manifesting as intrathoracic migration of the fundoplication wrap.2,3
This complication, often referred to as a “slipped” fundoplication, may result in clinically significant symptoms, including recurrent gastroesophageal reflux, dysphagia, or both, frequently requiring reintervention.4–6 Intrathoracic wrap migration (IWM) has been identified as a major mechanism of anatomical failure after laparoscopic fundoplication (LF), highlighting the importance of durable hiatal closure techniques in preventing recurrence.4–6
While prior studies have predominantly focused on overall recurrence rates after HHR, limited attention has been given to the specific impact of surgical techniques on the development of IWM. In particular, the role of mesh reinforcement in reducing this complication remains incompletely defined. Therefore, this systematic review and meta-analysis aimed to compare the incidence of IWM in patients undergoing LF with mesh-reinforced versus primary suture repair during HHR.
Materials and Methods
Study design
A systematic review and meta-analysis were conducted to investigate differences in frequency of IWM after LF with mesh reinforcement versus primary suture repair. We registered this systematic review protocol in the International Prospective Register of Systematic Reviews under the number CRD420261357182. The study was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P 2020) guidelines, 7 adhering to established methodological standards. We did not seek formal ethical approval as the study used data from published primary studies. The central question driving the study is: Does the placement of mesh during LF reduce the incidence of IWM when compared with simple suture repair?
Information sources and search strategy
A comprehensive search strategy was developed to search the following databases: PubMed, Embase, Cochrane Library, Scopus, and Web of Science. We systematically searched in these databases from inception to February 2026. The search terms were derived from the keywords “fundoplication” AND “wrap migration.” A complete list of search terms and a detailed search strategy are provided in Supplementary Table S1.
Study selection
Two independent reviewers screened the titles and abstracts of identified studies for relevance based on predefined inclusion and exclusion criteria. The full text of potentially relevant studies was then assessed for final eligibility. Any discrepancies between reviewers were resolved through discussion or consultation with a third reviewer. Inclusion criteria were as follows: (1) studies of patients undergoing LF comparing surgical outcomes in mesh placement versus primary suture repair group; (2) studies with adult patients (≥18 years old; (3) studies reporting at least one of the clinical outcomes of interest; and (4) randomized control trials (RCT), cohort, case-control, cross-sectional studies. Exclusion criteria were as follows: (1) studies with incomplete data or insufficient information about patient follow-up after surgery; (2) case reports, case series, reviews, commentaries, conference abstracts, and editorials; (3) studies with overlapping populations; and (4) studies published in languages other than English. There were no restrictions based on study sample size or publication date.
Data extraction
Two independent reviewers extracted data from eligible studies using a standardized data collection form in an Excel template. The extracted data included study characteristics such as year of publication, country of origin, sample size, study design, study period, follow-up duration, type of fundoplication, and mesh use; patient characteristics such as age and sex; and surgical outcomes such as operative time, IWM, and dysphagia.
Bias and quality assessment
Two reviewers performed the risk of bias assessment by using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized studies and the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool for observational studies.8,9 We used an electronic program, Robvis, to create risk-of-bias summary plots and weighted bar plots for visualization of individual studies. 10 We assessed the certainty of evidence by applying “The Grading of Recommendations Assessment, Development and Evaluation (GRADE)” approach. 11 Any discrepancies between reviewers were resolved through discussion or consultation with a third reviewer.
Statistical analysis
Exposure effects for binary endpoints were compared using pooled odds ratios (OR) with 95% confidence intervals. The findings were displayed in tables summarizing the primary study and patient characteristics, along with forest plots illustrating the aggregated results. The DerSimonian and Laird random-effects model was used. 12 Statistical significance was defined as a P value < 0.05. We assessed heterogeneity for each outcome using I2 and defined I2 of 75% and greater as substantial heterogeneity, 25%−75% as moderate heterogeneity, and below 25% as low heterogeneity, as defined by Higgins et al. 13 ; P < .10 and I2 > 25% were considered significant for heterogeneity. Review Manager 5.4 (Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) and SPSS V.29 were used for statistical analysis. A leave-one-out sensitivity analysis was performed to ensure the results were not dependent on a specific study. Publication bias was evaluated by visual inspection of funnel-plot graphs to assess for symmetrical distribution of trials with similar weights. Egger’s test was not used due to the small number of included studies. 14
Results
Study selection
From five different databases, we identified 507 records during the initial literature search, of which seven studies were ultimately included. Details about final eligibility are presented in the PRISMA flowchart, Figure 1, generated using the Haddaway et al. online tool. 16
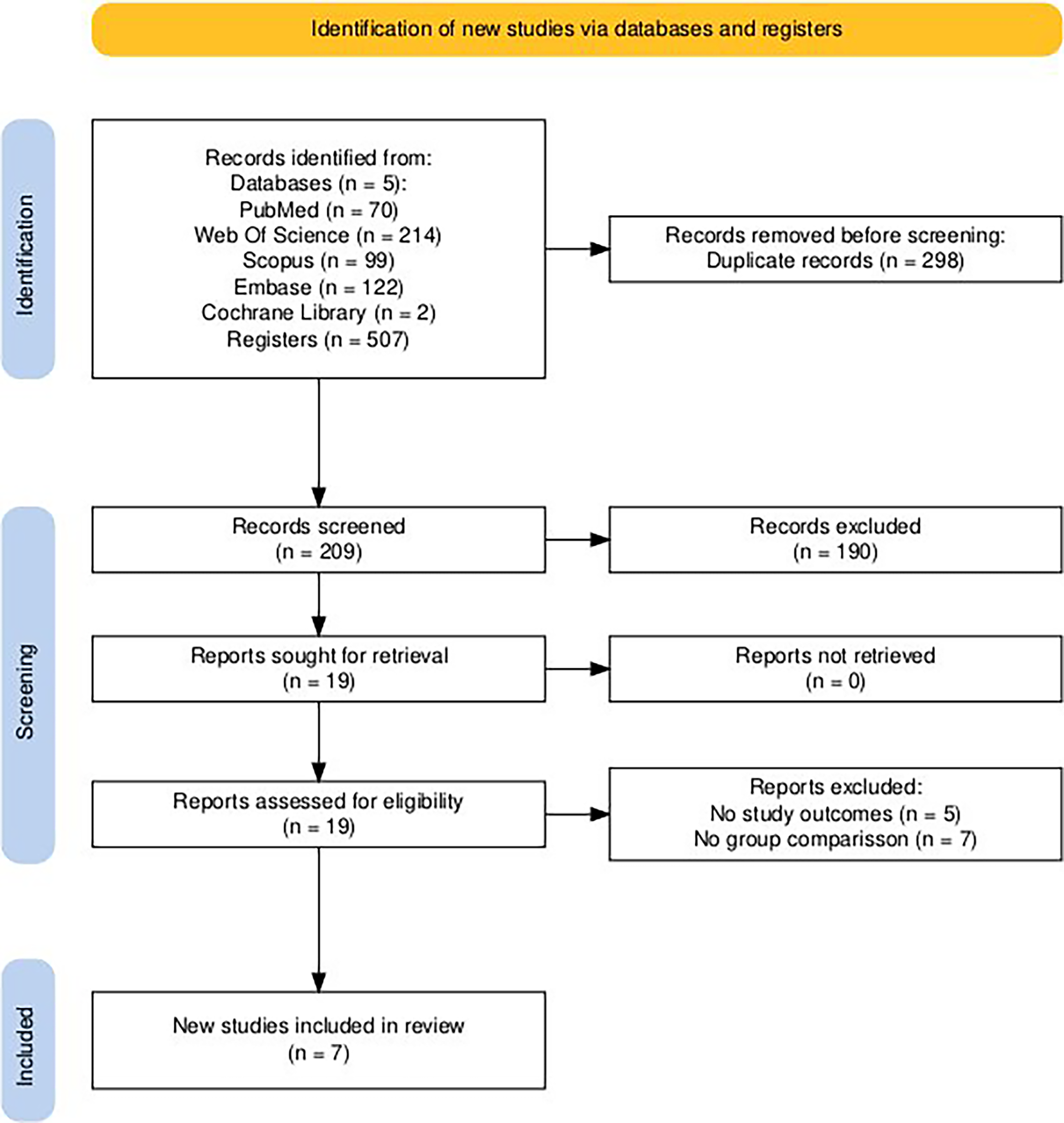
Search outputs based on PRISMA guidelines. 15 PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols.
Study characteristics
From the included studies, two were prospective and the remaining were retrospective cohort studies. Only one study was conducted in the United States. The detailed characteristics of the included studies and study populations are presented in Table 1.
Study Characteristics
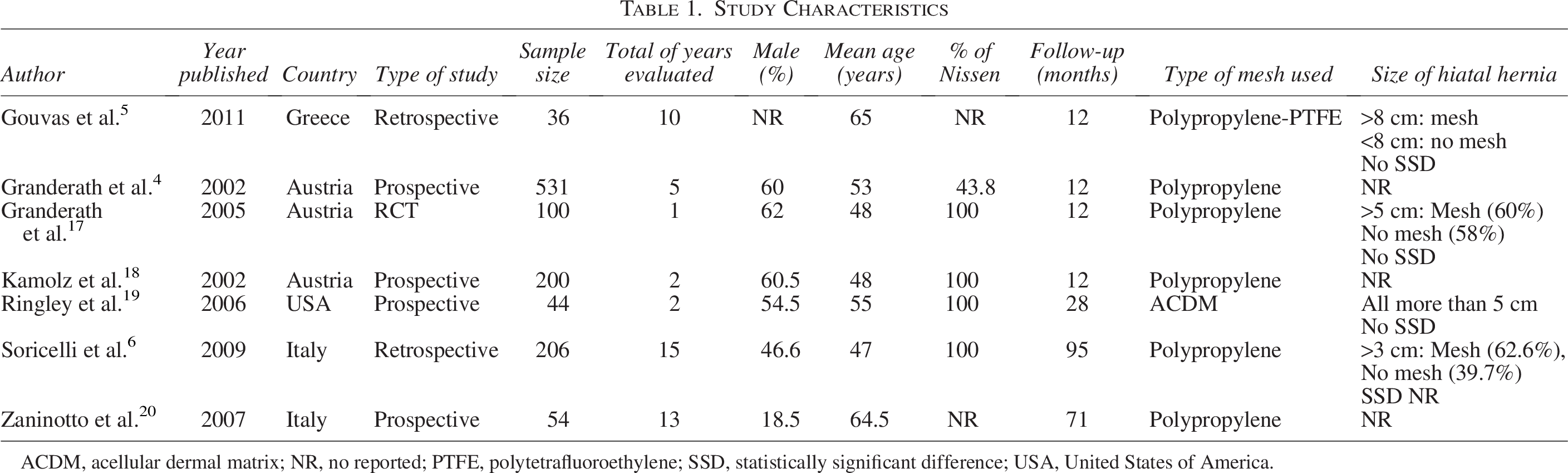
ACDM, acellular dermal matrix; NR, no reported; PTFE, polytetrafluoroethylene; SSD, statistically significant difference; USA, United States of America.
Results of syntheses
The total sample included 1171 patients. Among them, 43% were female (n = 504), with a mean age of 54.3 years. Baseline characteristics were similar between groups with respect to age and sex. Details are presented in Figure 2.
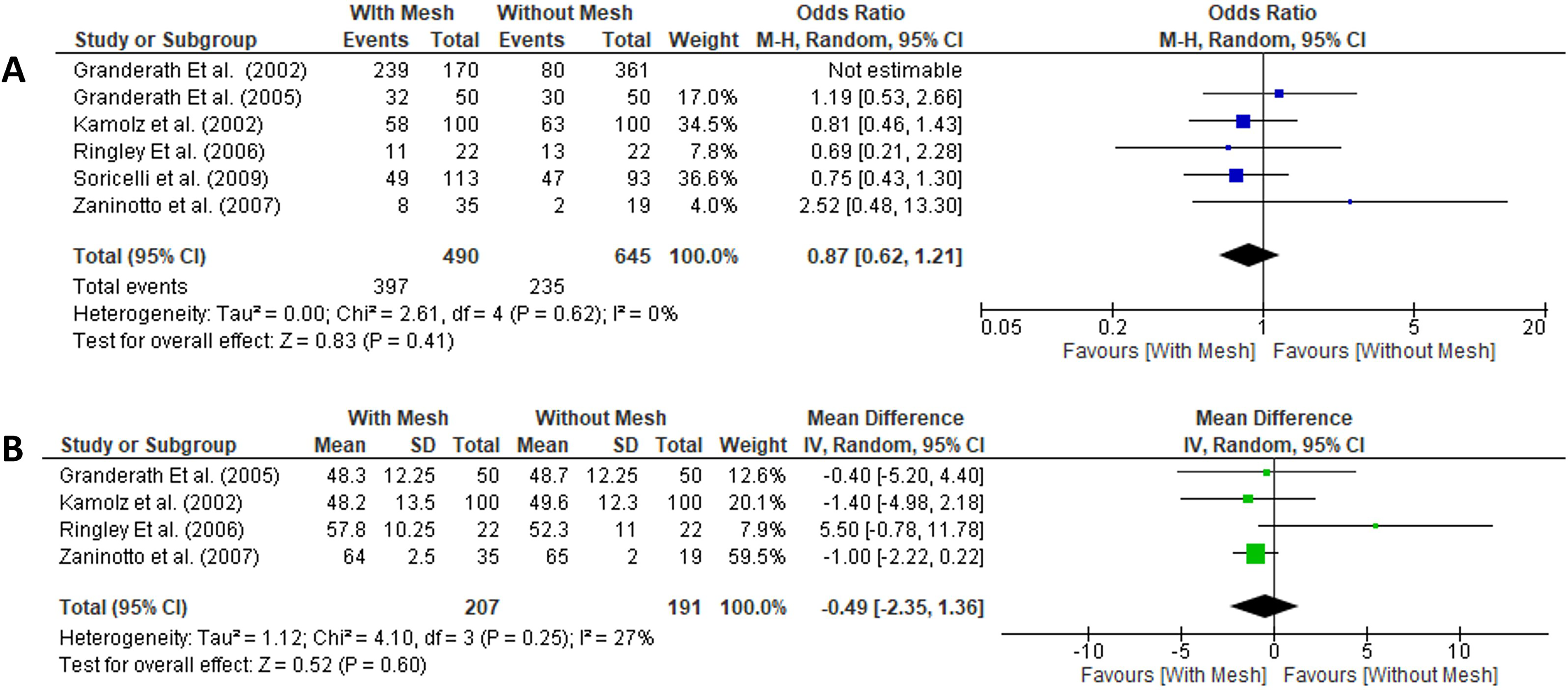
The pooled clinical characteristics.
Surgical outcomes
The mesh group had a longer operative time (mean difference = + 14.22, P = .05), with a significantly lower incidence of IWM (OR = 0.21; 95% CI = 0.10 to 0.42; P < .001), but a higher frequency of dysphagia at 3 months post-procedure (OR = 2.22; 95% CI = 1.60 to 3.09; P < .001). However, at 1-year follow-up, there was no significant difference in dysphagia between groups. Details are presented in Figure 3.
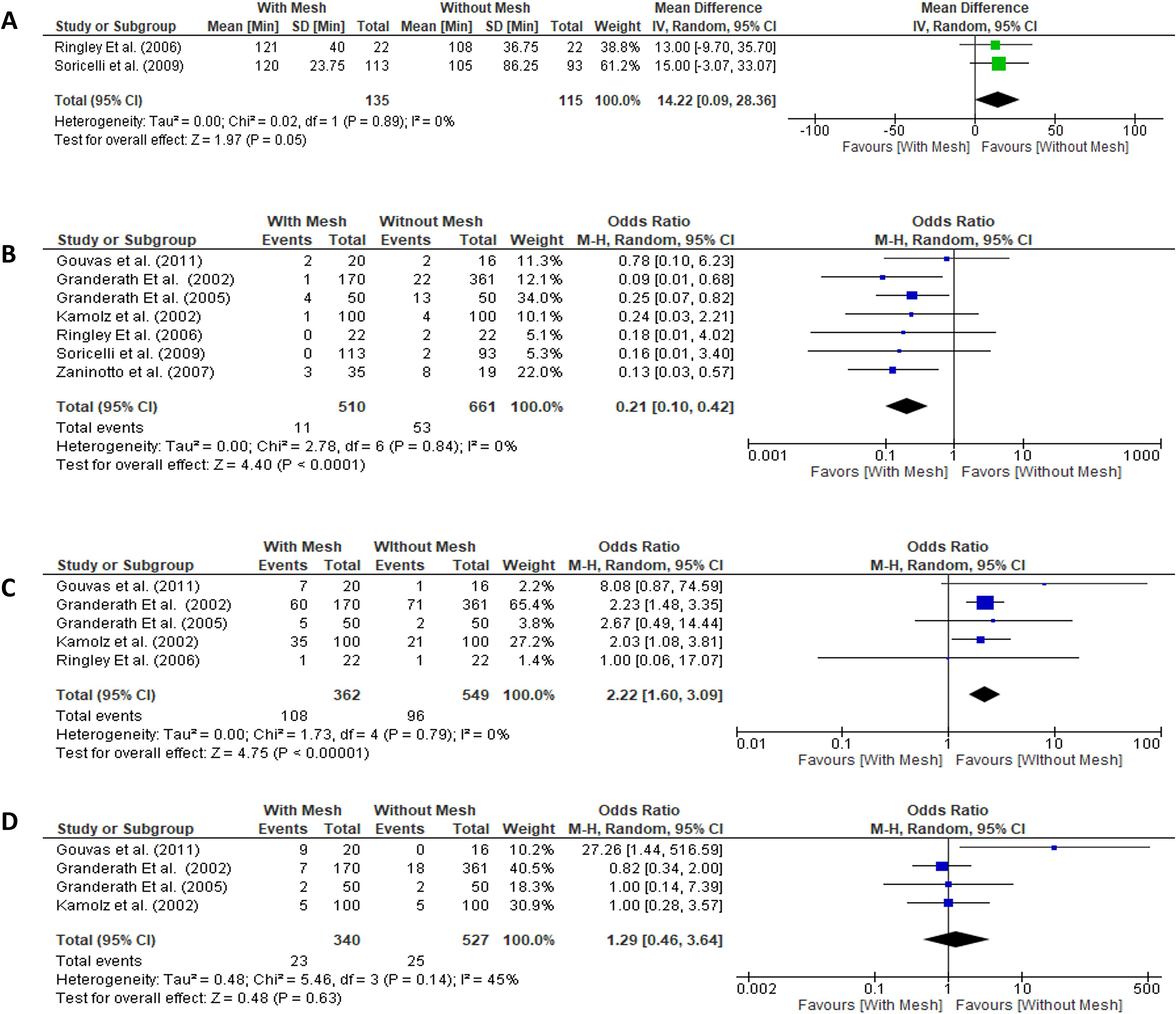
Pooled intraoperative and postoperative outcomes.
Sensitivity analysis
A leave-one-out sensitivity analysis was performed by iteratively removing one study at a time to assess the robustness of the pooled IWM estimates. The overall effect remained stable regardless of which study was excluded, indicating that no single study disproportionately influenced the results. Details are presented in Figure 4. Similar findings were observed when the analysis was restricted to prospective studies only. Furthermore, subgroup analysis restricted to polypropylene mesh yielded consistent results.
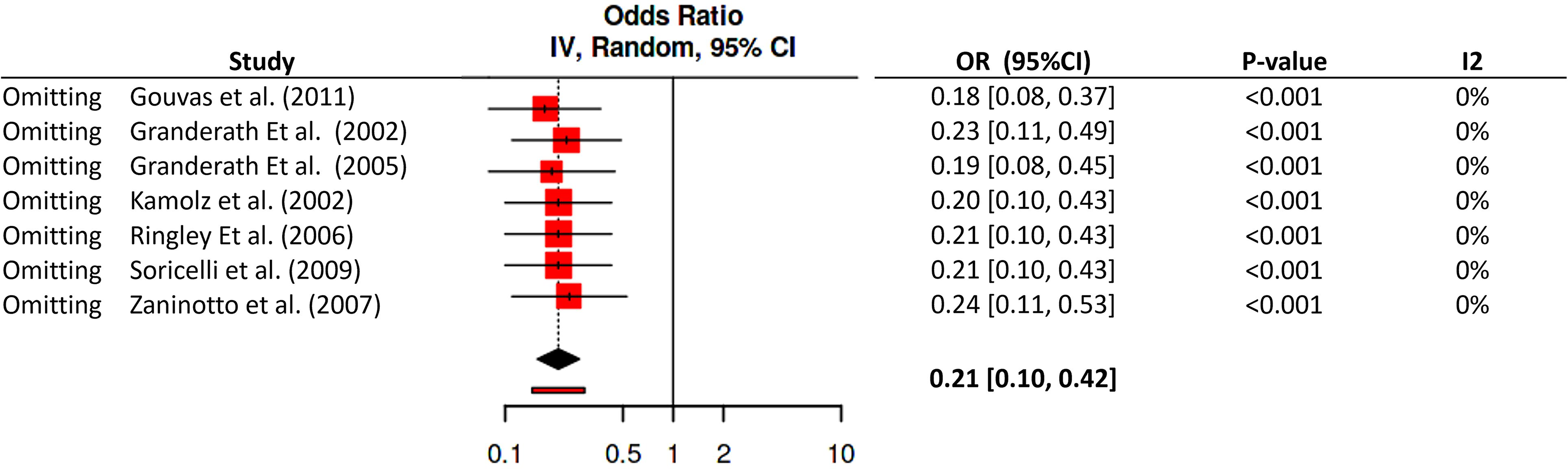
Leave-one-out sensitivity analysis for intrathoracic wrap migration.
Heterogeneity and risk of bias across studies
Heterogeneity was low for most of the surgical outcomes evaluated (I2 = 0%) except for dysphagia at 1 year with a 12 = 45%. Funnel plot analysis for IWM and dysphagia at 3 months demonstrated a symmetric distribution, suggesting no publication bias, whereas the funnel plot for dysphagia at 1 year demonstrated asymmetry, suggesting possible publication bias (Fig. 5).
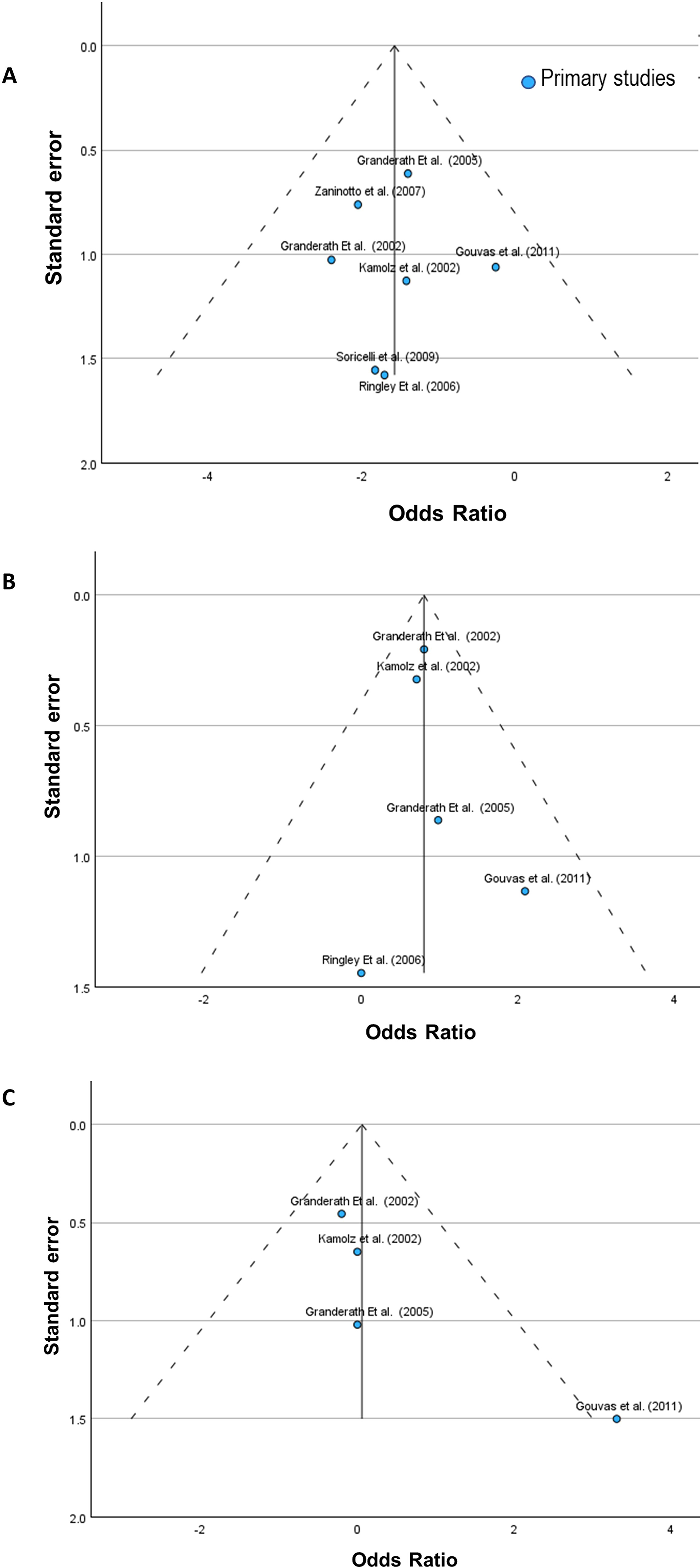
Funnel plots of the main surgical outcomes.
The results of the ROBINS-I and Rob2 scale, are shown in Supplementary Figures S1 and S2. For the observational studies, the overall assessment reported a serious risk of bias mainly based on bias due to confounding and missing data.
GRADE (quality of evidence)
The quality of evidence, assessed using the GRADE approach, was high for IWM and for dysphagia at 3 months. Although the risk of bias was serious, the certainty was upgraded due to a large effect size and the absence of imprecision, indirectness, inconsistency, and publication bias. In contrast, the quality of evidence for dysphagia at 1 year was low, mainly due to serious risk of bias, heterogeneity, and imprecision (Supplementary Table S2).
Discussion
This systematic review and meta-analysis comparing the incidence of IWM following LF in patients undergoing mesh reinforcement versus suture repair alone demonstrated a significantly lower incidence of IWM in the mesh group, with an increased incidence of dysphagia at 3 months; however, no significant difference in dysphagia was observed at 1 year postoperatively.
IWM after fundoplication
IWM is a significant complication following fundoplication, occurring in 7% to 30% of patients, with rates varying according to surgical technique and duration of follow-up.21,22 In this meta-analysis, the overall incidence was 5.5%, which may reflect the inclusion of patients undergoing mesh reinforcement. These findings highlight a tradeoff between structural durability and early postoperative function.
Its clinical relevance lies primarily in long-term surgical failure rather than acute complications. Migration leads to recurrent reflux symptoms, dysphagia, or both, frequently necessitating reoperation. 21 Reoperation rates following fundoplication range from 0% to 15%, with breakdown of the hiatal closure and subsequent wrap herniation representing the most common morphological cause, 23 and are associated with increased morbidity and mortality that reoperation carries when compared with primary surgery. 24
Several factors increase the risk of wrap migration. Technical factors include inadequate crural closure and insufficient esophageal mobilization, while patient-related factors include large hiatal hernias, early postoperative vomiting, and other diaphragmatic stressors.21,25 Notably, in this meta-analysis, hernia size was inconsistently reported across the analyzed studies, precluding adjustment for this variable. This limitation may introduce confounding, as hernia size is a known predictor of recurrence and wrap migration. However, among the studies that reported hernia size, no statistically significant difference in hiatal hernia dimensions was observed between the mesh and no-mesh groups.
Hiatal hernia recurrence versus IWM
Most studies on mesh reinforcement following fundoplication have focused on hiatal hernia recurrence rates, with no conclusive evidence that mesh reinforcement significantly reduces hiatal hernia recurrence when compared with suture-only repair,26–28 while mesh use has been associated with increased dysphagia in some studies. Notably, none of these studies specifically evaluated the effect of mesh reinforcement on IWM specifically, while our results suggest that despite the absence of a demonstrated benefit on overall recurrence, mesh reinforcement may play a role in reducing the incidence of IWM.
The apparent paradox in which mesh reinforcement does not reduce the overall incidence of hiatal hernia recurrence but is associated with a lower rate of IWM may be explained by distinct biomechanical mechanisms. Hiatal hernia recurrence reflects a failure of the crural repair—a process driven by tissue tension, poor tissue quality, and mechanical stress at the diaphragmatic hiatus during respiration and increases in intra-abdominal pressure. These forces act directly on the crural closure and may not be sufficiently mitigated by mesh reinforcement alone, particularly when the defect is large or the surrounding tissue is attenuated.
The IWM, in contrast, represents a distinct failure mode in which an intact or partially intact wrap displaces superiorly through the hiatus into the mediastinum. In this context, mesh may confer a more targeted benefit: By reinforcing the hiatal aperture and providing a more rigid scaffold around the gastroesophageal junction, it may mechanically impede cephalad migration of the wrap even in cases where some degree of hiatal laxity persists. Thus, while mesh may not prevent progressive widening of the hiatus, it may provide sufficient resistance to limit wrap herniation, effectively decoupling the two failure modes and explaining why its protective effect is selectively observed for migration rather than for recurrence overall.
Dysphagia
The existing evidence remains inconclusive, although some studies suggest a higher rate of dysphagia with mesh-reinforced fundoplication. The 13-year JAMA Surgery trial found that patients receiving suture-only repair experienced significantly less dysphagia for solids throughout the entire follow-up period (P = .013). 28 Similarly, a 2020 RCT reported a higher dysphagia score for solid food at 3 years in the mesh group compared with the suture-only group. 29 In contrast, a 2024 meta-analysis found no difference between groups in terms of new-onset early or late dysphagia, 27 while a network meta-analysis suggested that nonabsorbable mesh with fundoplication was associated with the lowest dysphagia rates when compared with primary suture repair with fundoplication, based on rankogram analysis. 26
In this meta-analysis, dysphagia was more frequent at 3 months postoperatively in the mesh group; however, no significant difference in dysphagia was observed at 1 year. The increased incidence of dysphagia at 3 months in the mesh group is likely attributable to local postoperative edema and the inflammatory reaction secondary to mesh placement, which transiently narrows the hiatal opening. The resolution of this difference at 1 year suggests that once the acute inflammatory response subsides and the surrounding tissues adapt, the mechanical impact of the mesh on esophageal transit normalizes, resulting in dysphagia rates comparable to those of the suture-only group.
Mesh reinforcement after fundoplication for selected patients and for selected outcomes?
While current evidence does not support a routine recommendation for mesh reinforcement during fundoplication—given the lack of demonstrated benefit in reducing hiatal hernia recurrence and the possible risk of mesh-related dysphagia—a more detailed, risk-stratified approach may be considered in selected patients. Specifically, in individuals with risk factors for IWM, such as a large hiatal defect, a short esophagus, elevated intra-abdominal pressure, or prior failed fundoplication, 21 selective mesh reinforcement may offer a clinically meaningful protective effect.
Importantly, the concern regarding dysphagia as a deterrent to mesh use may be overstated in this context: Our results demonstrated that although the incidence of dysphagia was higher in the mesh group during the first three postoperative months, this difference did not persist at 1 year, suggesting that mesh-related dysphagia could be largely a transient phenomenon rather than a persistent complication.
Taken together, these findings suggest that while mesh should not be routinely used for the prevention of hiatal hernia recurrence, its use may be justifiable—and potentially beneficial—in patients at heightened risk for IWM, provided that patients are counseled about the likelihood of early postoperative dysphagia, which is expected to resolve with time.
Limitations and strengths
Our study has important limitations as follows: (1) Most of our studies are observational in design, with an overall serious risk of bias; however, despite this, the level of evidence was considered high for the primary outcome. (2) Important clinical variables such as hiatal hernia size, BMI, or type of fundoplication were not uniformly reported, introducing clinical heterogeneity that may have influenced the observed outcomes. (3) The small number of included studies limits the possibility to perform a more robust subgroup analysis or meta regression. (4) Most included studies were published before 2010; however, they represent the only available comparative evidence specifically reporting IWM. More recent meta-analyses on HHR have focused primarily on overall anatomical recurrence, leaving this specific complication largely unaddressed in contemporary literature.
To the best of our knowledge, this is the first meta-analysis to systematically evaluate the effect of mesh reinforcement on IWM following fundoplication. Our findings suggest that mesh reinforcement may reduce the risk of IWM and may be considered in selected patients at elevated risk for this complication.
Conclusion
This meta-analysis demonstrates that mesh reinforcement is associated with a significantly lower incidence of IWM, along with a transient increase in dysphagia at 3 months that did not persist at 1 year. Although mesh reinforcement cannot be routinely recommended for the prevention of hiatal hernia recurrence, its selective use may be justified in patients at high risk for IWM. Further prospective randomized controlled trials are warranted to confirm these findings and to better define the role of mesh reinforcement in reducing IWM and its impact on both short- and long-term dysphagia.
Authors’ Contributions
Study conception and design, as well as analysis and interpretation of data, were performed by Y.R.-M. Data acquisition was conducted by Y.R.-M. and J.A. The article was drafted by Y.R.-M. Critical revision of the article was carried out by T.A., Y.Z., J.C., and E.M-A.
Footnotes
Author Disclosure Statement
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.