
Abstract
Background:
Laparoscopic intraperitoneal onlay mesh repair with defect closure (intraperitoneal onlay mesh repair with fascial defect [IPOM Plus]) is widely practiced for ventral hernia repair but remains associated with significant postoperative pain and intraperitoneal mesh-related complications. Transabdominal preperitoneal mesh repair with defect closure (vTAPP Plus) offers an anatomical, extraperitoneal alternative that may reduce postoperative pain along with reduced mesh-related complications. High-quality randomized evidence directly comparing these techniques is limited.
Methods:
This prospective, single-center, randomized controlled trial was conducted at a tertiary care institute. Adults with small-to-medium primary ventral hernias (2–4 cm) were randomized to undergo laparoscopic IPOM Plus or vTAPP Plus repair. The primary outcome was mean postoperative pain score (Visual Analogue Scale [VAS]) within the first 24 hours. Secondary outcomes included serial pain scores up to 6 months, operative duration, length of hospital stay, postoperative complications, and recurrence. Statistical analysis was performed using appropriate statistical tests.
Results:
In total, 68 patients were analyzed (IPOM Plus: n = 36; vTAPP Plus: n = 32). Baseline demographic and clinical variables were comparable between groups. vTAPP Plus demonstrated significantly lower postoperative pain at 6, 12, 24, and 48 hours, as well as at 14 and 30 days (P < .001). Differences diminished at 3 months and were not significant at 6 months. Operative time was marginally longer for vTAPP Plus, the hospital stay was significantly lower. Postoperative complication rates were comparable. No mesh infection or hernia recurrence was observed during follow-up.
Conclusion:
vTAPP Plus repair significantly reduces early and intermediate postoperative pain compared with IPOM Plus, without compromising safety or short-term efficacy. Thus, vTAPP Plus represents a better option for selected primary midline ventral hernias.
Introduction
Ventral abdominal wall hernias represent one of the most frequently encountered conditions in general surgical practice and are associated with pain, functional limitation, cosmetic deformity, and impaired quality of life. The prevalence of abdominal wall hernias is estimated at approximately 1.7% in the general population, increasing to nearly 4% in individuals over 45 years of age. 1 Over the past two decades, laparoscopic repair has emerged as the preferred approach owing to reduced wound morbidity, shorter hospital stays, and faster postoperative recovery compared with open techniques. 2 Among laparoscopic methods, intraperitoneal onlay mesh repair with fascial defect closure (IPOM Plus) has gained widespread acceptance due to its technical simplicity and reproducibility.
However, IPOM Plus is associated with significant postoperative pain, largely attributable to intraperitoneal mesh fixation using transfascial sutures and tacks. Previous studies have reported mean Visual Analogue Scale (VAS) pain scores as high as 5 to 6/10 on postoperative day one, with persistent pain reported in a subset of patients during early recovery. 1 In addition, the requirement for composite meshes and fixation devices increases procedural cost and exposes patients to potential mesh–viscera complications, including adhesions and bowel injury. 3
Transabdominal preperitoneal repair with defect closure (vTAPP Plus) adapts the principles of extraperitoneal mesh placement, restoring abdominal wall anatomy while isolating the mesh from intra-abdominal viscera. Despite encouraging outcomes, comparative evidence between IPOM Plus and vTAPP Plus remains largely retrospective, and randomized trials focusing on patient-centered outcomes such as postoperative pain are scarce. The present study was designed to address this evidence gap through a prospective randomized controlled comparison of these two techniques.
Methodology
Study design and setting
This study was designed as a prospective, randomized, single-blinded controlled trial conducted in the Department of Surgical Disciplines at the All India Institute of Medical Sciences, New Delhi, a tertiary care referral center. The study period extended from December 2023 to May 2025.
The trial was conducted following approval from the Institutional Ethics Committee and was registered with the Clinical Trials Registry of India. All procedures adhered to the principles outlined in the Declaration of Helsinki (2013 revision), Indian Council of Medical Research ethical guidelines, and Good Clinical Practice standards. The reporting of this trial conforms to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized controlled trials.
The study employed a parallel-group design comparing two established minimally invasive techniques for ventral hernia repair: Laparoscopic Intraperitoneal Onlay Mesh repair with fascial defect closure (IPOM Plus) and laparoscopic Transabdominal Preperitoneal mesh repair with fascial defect closure (vTAPP Plus).
Study population
Adult patients presenting with primary midline ventral abdominal wall hernias to outpatient clinics or surgical wards were screened for eligibility. Only patients with small-to-medium-sized hernias were considered in order to ensure the technical feasibility of both procedures and minimize confounding related to hernia complexity.
Inclusion criteria
Patients were included if they fulfilled all of the following criteria:
Age ≥18 years. Primary midline ventral hernia with a defect size between 2 and 4 cm, as measured by preoperative ultrasonography or intraoperative assessment. Fitness for general anesthesia and laparoscopic surgery. Willingness to provide written informed consent and comply with a structured 6-month follow-up protocol.
Exclusion criteria
Patients were excluded if they had:
Recurrent, incisional, parastomal, or multiple hernias. Large hernia defects (>4 cm), loss of domain, or complex abdominal wall defects. Emergency presentations such as strangulated or obstructed hernias. Severe cardiopulmonary comorbidities precluding laparoscopy. Pregnancy. Inability or unwillingness to complete follow-up.
Sample size calculation
Sample size estimation was performed using postoperative pain score data from previously published comparative studies. Based on reported mean VAS scores at 24 hours of 3.29 ± 1.44 for IPOM and 2.26 ± 1.75 for vTAPP repairs, 4 a noninferiority margin of 1 unit on the VAS scale was selected. With a power of 90% and a two-sided alpha of 0.05, the calculated minimum sample size was 65 patients. To compensate for potential dropouts, a total of 72 patients were recruited, with 36 patients allocated to each arm.
Randomization and blinding
Randomization was carried out using computer-generated random numbers prepared by an independent biostatistician. Block randomization with variable block sizes was employed to maintain balanced allocation and prevent predictability. Allocation concealment was ensured using sealed, opaque, sequentially numbered envelopes opened in the operating theater immediately prior to surgery.
The study was single-blinded: Operating surgeons were aware of the allocated procedure, while patients were blinded to the type of repair performed. This approach was chosen to minimize subjective bias during postoperative pain assessment, the primary outcome of the study.
Preoperative evaluation
All patients underwent standardized preoperative assessment, including detailed clinical history, physical examination, and evaluation of hernia characteristics such as location, size, reducibility, and duration. Baseline investigations included complete blood counts, renal and liver function tests, fasting blood glucose, electrocardiography, and chest radiography as required for anesthetic clearance. Abdominal ultrasonography was performed in all patients to assess defect size and contents.
Patients were educated preoperatively regarding the VAS for pain assessment to ensure accurate and consistent reporting postoperatively.
Operative technique
All procedures were performed under general anesthesia by surgeons experienced in advanced laparoscopic hernia repair. Inj. Cefuroxime 1.2 g intravenously was administered preincision as standard antibiotic prophylaxis. Patients were positioned supine with both arms by the side. The surgeon stood on the left side, and the assistant with the camera stood beside the surgeon. The monitor was placed on the right side of the patient for optimal ergonomics.
After standard sterile preparation, Foley’s catheterization was done, and pneumoperitoneum was established using a Veress needle at Palmer’s point. The intra-abdominal pressure was maintained at 14 mmHg. A standard three-port technique was used, with a 12-mm camera port—mid-axillary line and two 5-mm working ports—placed in the anterior axillary line on either side, approximately 7.5 cm from the camera port. Intra-abdominal pressure was maintained at 14 mmHg.
IPOM plus group
Following adhesiolysis and reduction of hernia contents, the fascial defect was closed using a continuous barbed suture. A composite dual-layer mesh was placed intraperitoneally with a minimum overlap of 5 cm beyond defect margins. Mesh fixation was achieved using a combination of transfascial sutures and absorbable tacks in a double-crown configuration. Figure 1a–c shows the standard steps of the IPOM plus procedure:
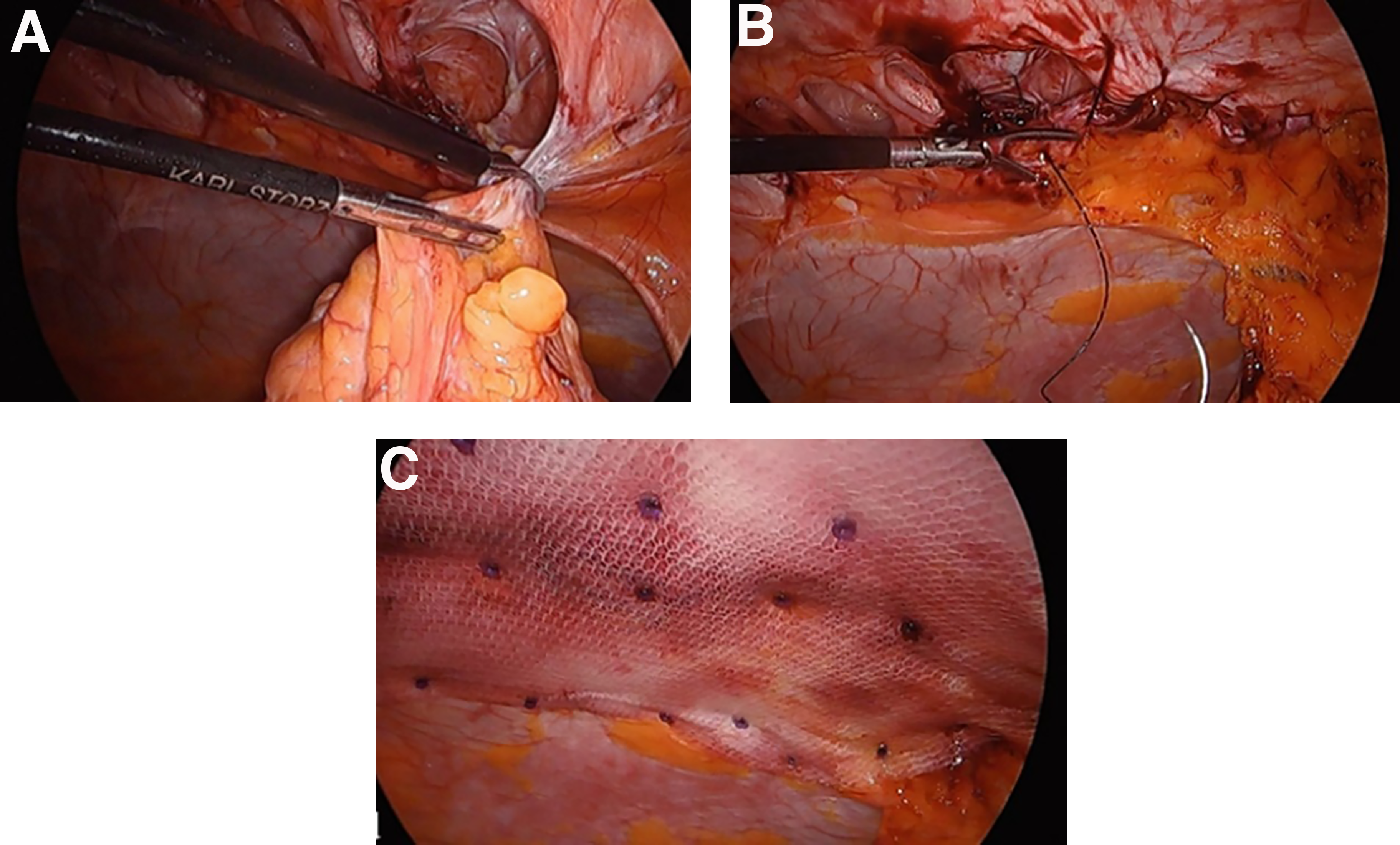
Steps of IPOM Plus repair.
vTAPP plus group
A peritoneal incision was made at least 5 cm from the defect margin, and a preperitoneal plane was developed. After defect closure using a continuous barbed suture, a polypropylene mesh was placed in the preperitoneal space with adequate overlap. The peritoneal flap was then meticulously closed over the mesh, completely isolating it from the intra-abdominal cavity. Figure 2a–f shows the steps involved in TAPP plus repair for ventral abdominal hernias (vTAPP):
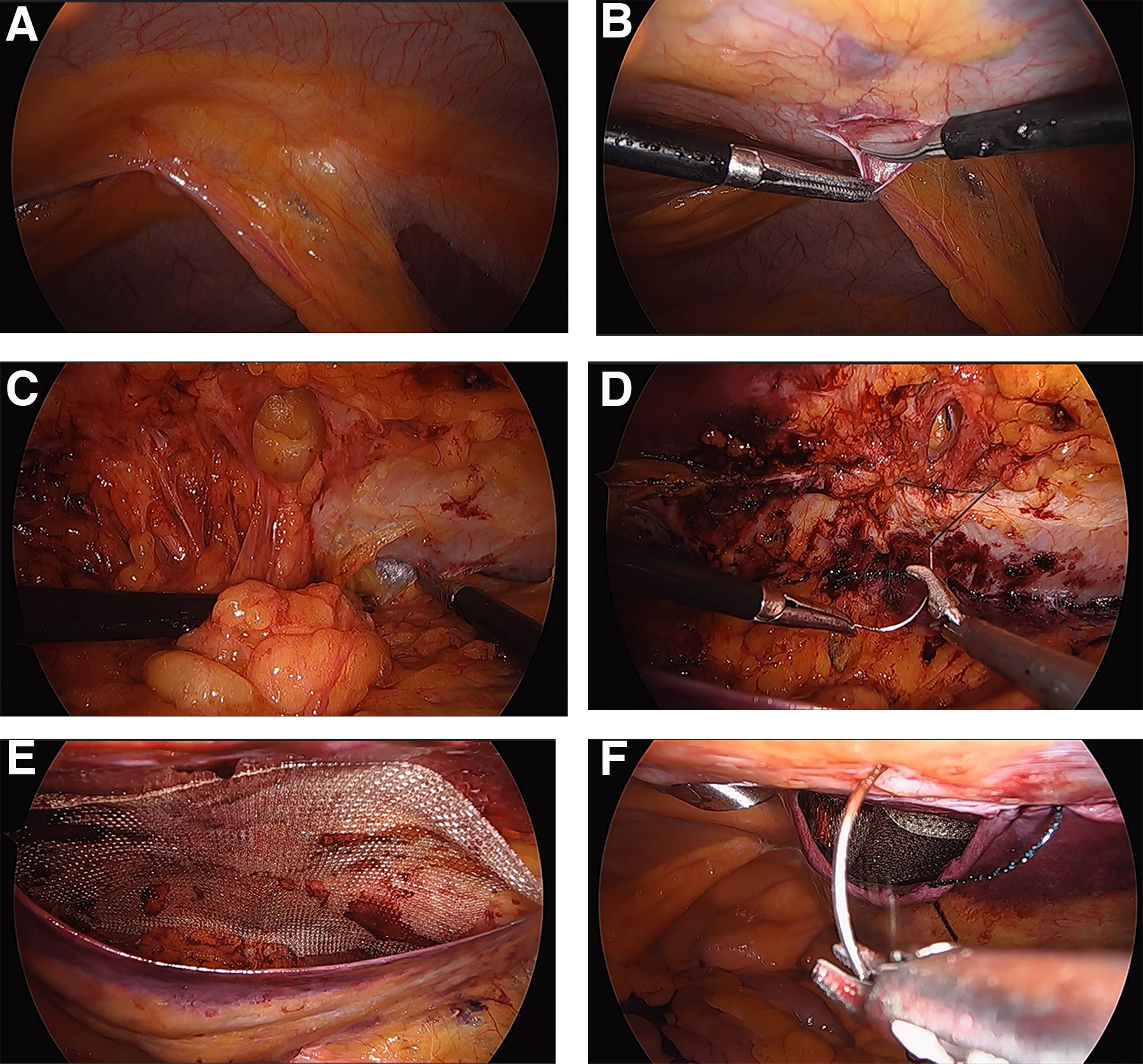
Steps of vTAPP Plus repair.
Postoperative care and follow-up
Postoperative analgesia followed a standardized protocol. Pain was assessed using VAS at predefined intervals: 6, 12, 24, and 48 hours, and at 2 weeks, 1 month, 3 months, and 6 months. Patients were followed clinically at each visit for complications, chronic pain, and recurrence.
Statistical analysis
Data were analyzed using SPSS v20. Continuous variables were expressed as mean ± SD and compared using Student’s t-test or Mann–Whitney U test as appropriate. Categorical variables were compared using Chi-square or Fisher’s exact test. A P value <0.05 was considered statistically significant.
Results
Study population and CONSORT flow
During the study period, a total of 79 patients presenting with primary ventral abdominal wall hernias were assessed for eligibility. Of these, 72 patients met the inclusion criteria and were randomized to one of the two intervention arms: Laparoscopic IPOM Plus repair or laparoscopic vTAPP Plus repair. Randomization was performed in a 1:1 allocation ratio, resulting in 36 patients assigned to each group.
Intraoperatively, four patients (11.1%) in the vTAPP Plus arm required conversion to IPOM Plus repair due to technical limitations encountered during surgery. The primary reason for conversion was the inability to create an adequate and safe preperitoneal flap, most commonly due to dense peritoneal adhesions or peritoneal fragility. These conversions were anticipated risks inherent to the vTAPP technique and were not associated with any intraoperative complications or adverse events.
As per the predefined statistical plan, a per-protocol analysis was undertaken to accurately assess outcomes related to the intended surgical technique. Consequently, the four converted patients were excluded from the final analysis. Thus, 68 patients were included in the per-protocol analysis, comprising 36 patients in the IPOM Plus group and 32 patients in the vTAPP Plus group.
All patients completed in-hospital follow-up, and follow-up data up to 3 months were available for all analyzed participants. At 6 months, a small degree of attrition was observed, consistent with real-world clinical follow-up; however, this did not affect the analysis of primary or early secondary outcomes. The overall patient flow through the study is summarized in the CONSORT diagram (Fig. 3).
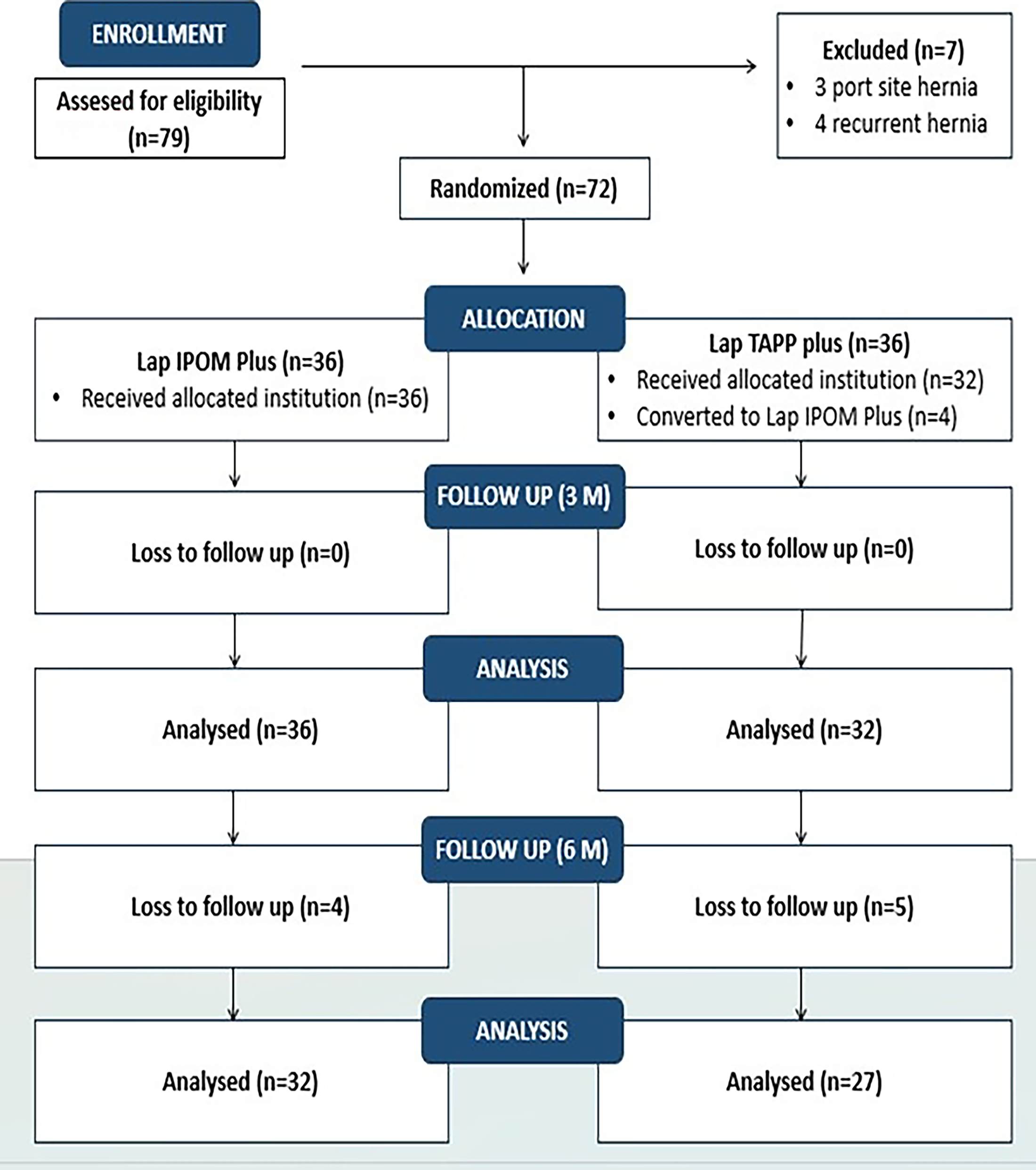
CONSORT diagram.
Baseline demographic and clinical characteristics
Baseline demographic and clinical characteristics of the study population are summarized in Table 1. The two groups were well matched across all measured baseline parameters, confirming the effectiveness of the randomization process and ensuring the internal validity of the comparative analysis.
Baseline Characteristics of the Two Groups
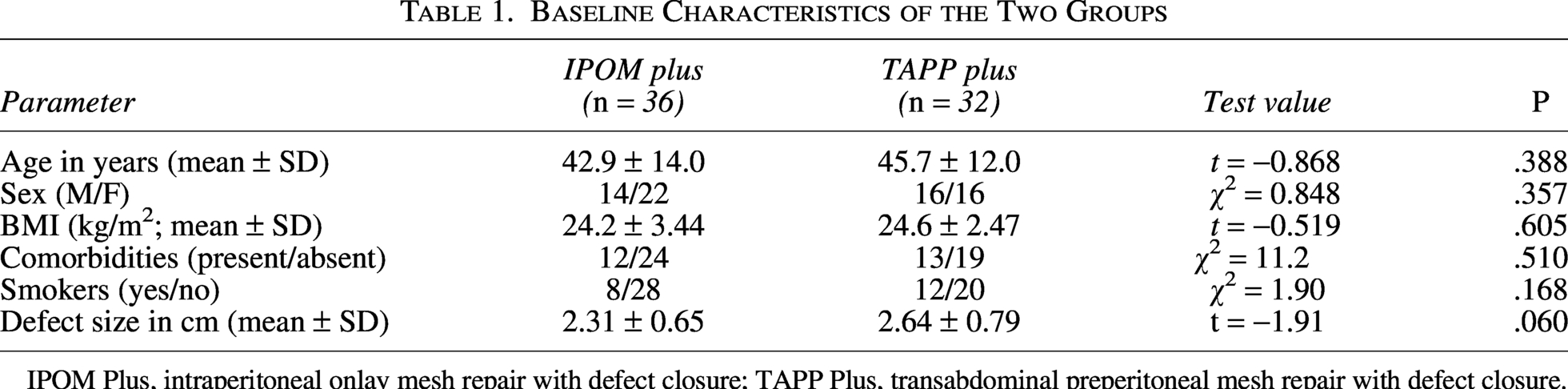
IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure.
The mean age in the IPOM Plus group was 42.9 ± 14.0 years, compared with 45.7 ± 12.0 years in the vTAPP Plus group, with no statistically significant difference (P = .388). Sex distribution was similar, with 14 males and 22 females in the IPOM Plus group and 16 males and 16 females in the vTAPP Plus group (P = .357).
Mean body mass index was 24.2 ± 3.44 kg/m2 in the IPOM Plus group and 24.6 ± 2.47 kg/m2 in the vTAPP Plus group, without significant difference (P = .605). The prevalence and distribution of associated comorbidities were comparable (P = .510), with hypertension being the most common, followed by diabetes mellitus and hypothyroidism.
Smoking status did not differ significantly between groups, with smokers comprising 22.2% of the IPOM Plus group and 37.5% of the vTAPP Plus group (P = .168). The mean hernia defect size was 2.31 ± 0.65 cm in the IPOM Plus group and 2.64 ± 0.79 cm in the vTAPP Plus group, with no statistically significant difference (P = .060).
Overall, baseline homogeneity was achieved, allowing postoperative outcomes to be attributed primarily to the surgical technique rather than patient- or hernia-related factors.
Postoperative pain scores
The primary outcome of the study was the mean postoperative pain score during the first 24 hours, assessed using the VAS. Pain scores at 6, 12, and 24 hours were recorded systematically and analyzed both individually and as a composite measure.
As shown in Table 2, patients in the vTAPP Plus group experienced significantly lower postoperative pain compared with those in the IPOM Plus group at all early time points. At 6 hours postoperatively, the mean VAS score was 3.75 ± 1.32 in the IPOM Plus group, compared with 2.66 ± 0.83 in the vTAPP Plus group. This difference was statistically significant (P < .001).
Comparison of Postoperative Visual Analogue Scale Pain Scores at Multiple Time Intervals Between Intraperitoneal Onlay Mesh Repair with Defect Closure-Plus and Transabdominal Preperitoneal Mesh Repair with Defect Closure Groups
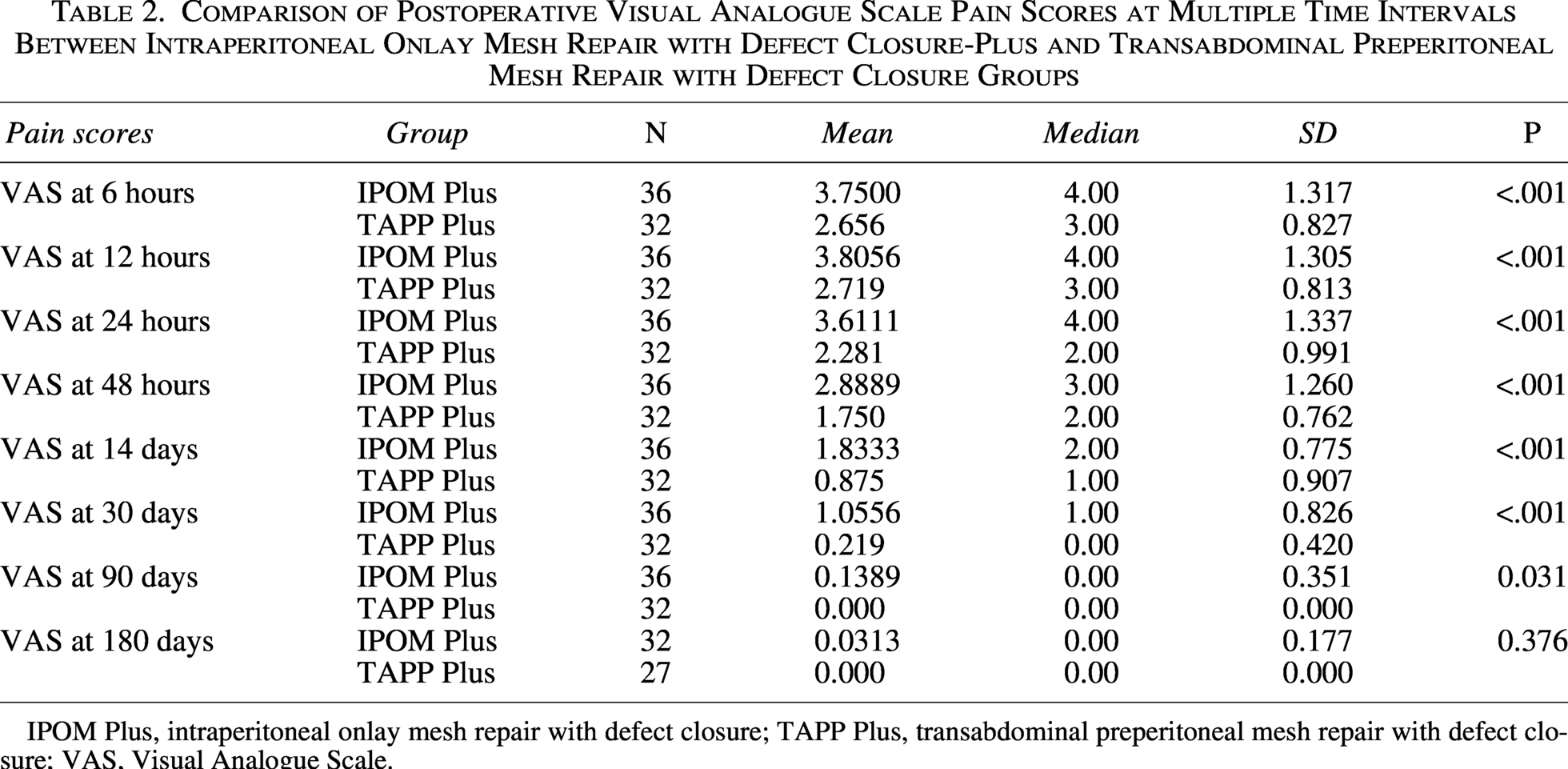
IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure; VAS, Visual Analogue Scale.
At 12 hours, the mean VAS score remained higher in the IPOM Plus group (3.81 ± 1.31) compared with the vTAPP Plus group (2.72 ± 0.81), again demonstrating a statistically significant difference (P < .001). Similarly, at 24 hours, patients undergoing IPOM Plus repair reported a mean VAS score of 3.61 ± 1.34, whereas those undergoing vTAPP Plus repair reported a substantially lower mean score of 2.28 ± 0.99 (P < .001).
The consistently lower pain scores in the vTAPP Plus group across all early postoperative assessments resulted in a significantly lower composite 24-hour pain score, thereby meeting the primary endpoint of the study (Table 3). These findings indicate a clear and clinically meaningful reduction in early postoperative pain following vTAPP Plus repair.
Distribution of Patients According to Operative Time in the Two Study Groups

IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure.
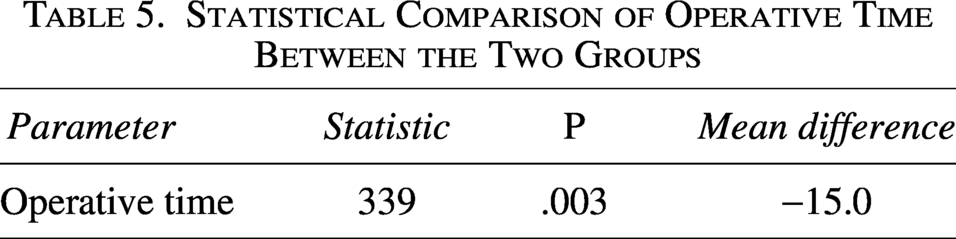
Statistical Comparison of Operative Time Between the Two Groups
Comparison of Average Visual Analogue Scale Pain Scores During the First 24 hours Between Intraperitoneal Onlay Mesh Repair with Defect Closure and Transabdominal Preperitoneal Mesh Repair with Defect Closure Groups
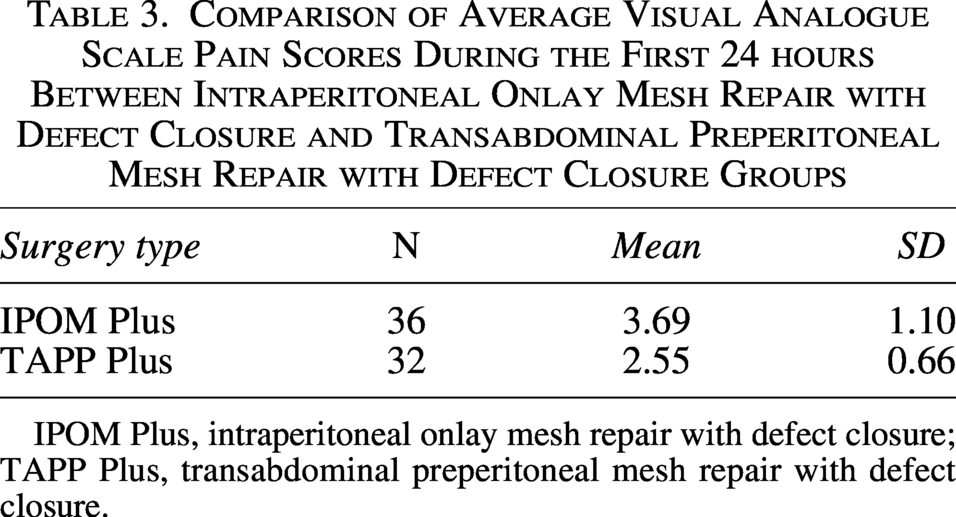
IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure.
Serial assessment of postoperative pain revealed a distinct and sustained divergence in pain trajectories between the two groups during the early and intermediate postoperative periods (Table 2).
At 48 hours, pain scores declined in both groups; however, the difference between techniques remained significant. The mean VAS score at this time point was 2.89 ± 1.26 in the IPOM Plus group compared with 1.75 ± 0.76 in the vTAPP Plus group (P < .001). This finding suggests that the pain-reducing effect of vTAPP Plus extends beyond the immediate postoperative period.
At 14 days, most patients reported mild pain or discomfort. Nevertheless, the IPOM Plus group continued to demonstrate higher pain scores (1.83 ± 0.78) compared with the vTAPP Plus group (0.88 ± 0.91), and this difference remained statistically significant (P < .001).
By 30 days, pain levels were low in both groups, yet a statistically significant difference persisted. The mean VAS score was 1.06 ± 0.83 in the IPOM Plus group compared with 0.22 ± 0.42 in the vTAPP Plus group (P < .001). This indicates more rapid resolution of postoperative discomfort following vTAPP Plus repair.
At 90 days, pain had resolved in nearly all patients. A minimal residual pain score was observed in the IPOM Plus group (0.14 ± 0.35), whereas no patient in the vTAPP Plus group reported persistent pain, resulting in a small but statistically significant difference (P = .031).
At 180 days, pain outcomes were comparable between groups, with negligible VAS scores and no statistically significant difference (P = .376). This suggests that while both techniques yield similar long-term pain outcomes, vTAPP Plus offers a substantial advantage during early and intermediate recovery.
Operative parameters
The operative duration was marginally longer in the vTAPP Plus group compared with the IPOM Plus group. This difference reflects the additional technical steps involved in vTAPP Plus repair, including creation of a preperitoneal flap, meticulous dissection, and closure of the peritoneum over the mesh. Despite the longer operative time, there were no intraoperative complications attributable to prolonged surgery, and no procedure required conversion to open repair.
Postoperative outcomes and complications
The length of hospital stay, as shown in Table 6, was significantly lower in the vTAPP plus group as compared with the IPOM plus group (1.31 ± 0.471 versus 2 ± 0.756; P < .001).
Comparison of Early Post-Operative Complications at 3 Days Between Intraperitoneal Onlay Mesh Repair with Defect Closure and Transabdominal Preperitoneal Mesh Repair with Defect Closure Groups
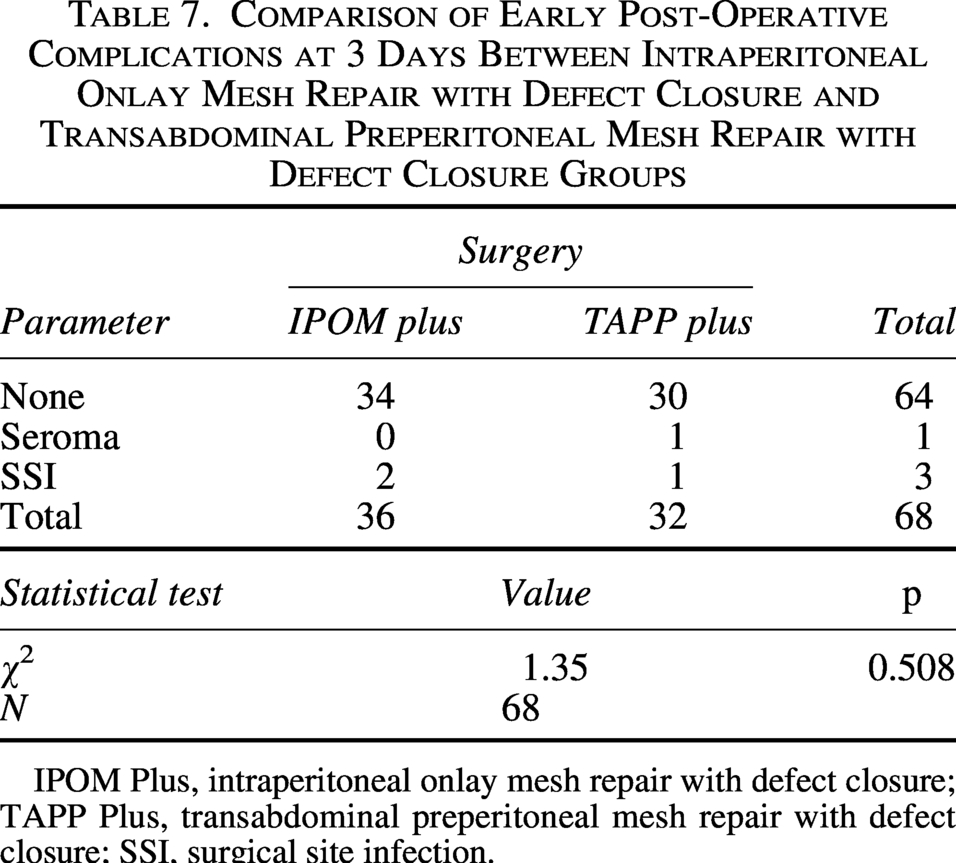
IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure; SSI, surgical site infection.
Comparison of Post-Operative Complications at 7 Days Between Intraperitoneal Onlay Mesh Repair with Defect Closure and Transabdominal Preperitoneal Mesh Repair with Defect Closure Groups
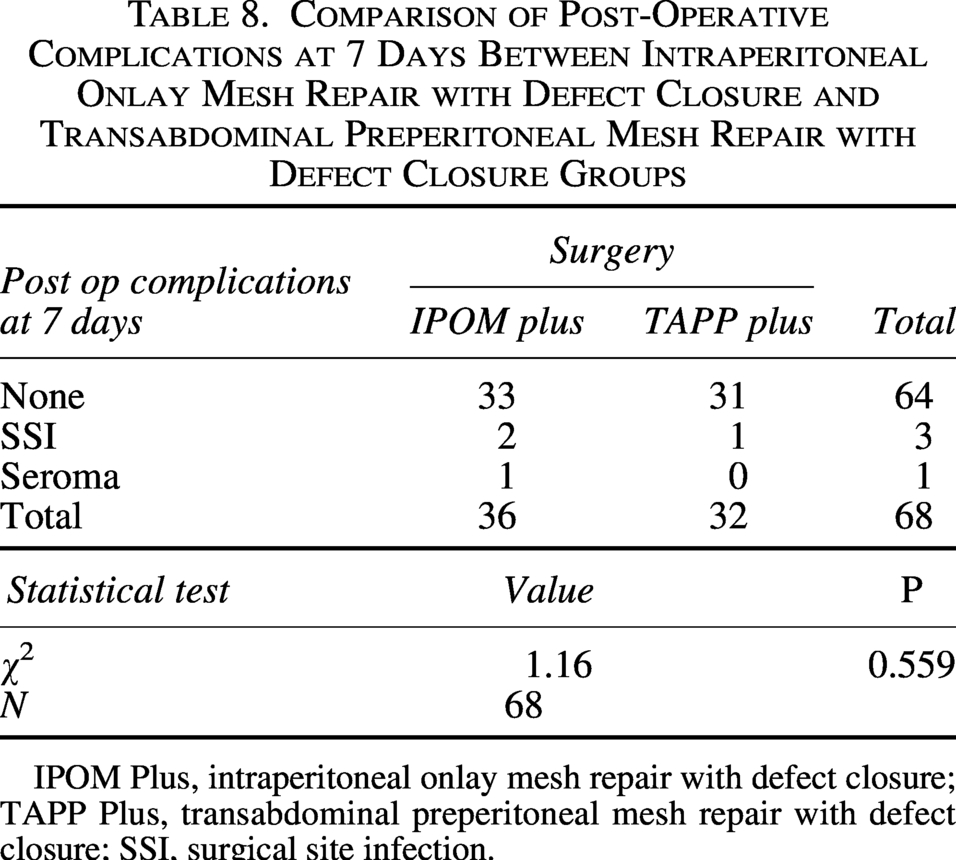
IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure; SSI, surgical site infection.
Comparison of Length of Hospital Stay (Days) in Between the Two Groups

IPOM Plus, intraperitoneal onlay mesh repair with defect closure; TAPP Plus, transabdominal preperitoneal mesh repair with defect closure.
Postoperative complications were infrequent and comparable between groups. Seroma formation, hematoma, and surgical site infection occurred at low rates, with no statistically significant differences observed. All complications were minor (Clavien–Dindo Grade I–II) and managed conservatively.
Post-operative complications at 21, 90, and 180 days
Follow-up assessments were conducted at 21 days, 90 days, and 180 days postoperatively to evaluate for late or delayed complications in both study groups. Parameters assessed included seroma formation, superficial surgical site infection (SSI), hematoma, urinary retention, neuralgic pain, mesh infection, and hernia recurrence.
No complications were observed at any of these follow-up intervals in either the IPOM Plus or TAPP Plus groups. All patients remained asymptomatic, and no clinical or radiological evidence of mesh-related morbidity or hernia recurrence was identified during the entire follow-up period.
Discussion
This prospective randomized controlled trial provides robust evidence that laparoscopic transabdominal preperitoneal mesh repair with fascial defect closure (vTAPP Plus) is associated with significantly reduced postoperative pain compared with intraperitoneal onlay mesh repair with defect closure (IPOM Plus) in patients with small-to-medium primary midline ventral hernias. The observed reduction in pain was most pronounced in the immediate postoperative period and persisted through the early and intermediate phases of recovery, extending up to 3 months. These findings directly address one of the most clinically relevant limitations of IPOM-based repairs and reinforce the growing interest in extraperitoneal approaches for ventral hernia management,3,5 where postoperative pain scores on day one have been reported to range between VAS 4 and 7 following conventional IPOM repairs.
Postoperative pain remains a critical determinant of patient satisfaction, early mobilization, return to daily activities, and overall quality of recovery following hernia surgery. Despite widespread adoption of IPOM Plus, postoperative pain—both acute and chronic—continues to be a significant concern, with chronic pain reported in approximately 10–20% of patients after laparoscopic ventral hernia repair in long-term series. 6 Multiple mechanisms have been proposed to explain pain following IPOM repair, the most prominent being traumatic mesh fixation. Transfascial sutures and tacks traverse the abdominal wall musculature and may irritate or entrap intercostal nerves, resulting in nociceptive and neuropathic pain; nerve-related pain symptoms have been described in up to 32% of patients following tack fixation.7,8 In addition, intraperitoneal mesh placement may provoke a heightened inflammatory response due to direct contact with visceral and parietal peritoneum, contributing to persistent discomfort. 9
In contrast, vTAPP Plus places the mesh in the preperitoneal plane, a relatively aneural and well-vascularized space. 9 This anatomical positioning allows the mesh to be stabilized by the physiological “sandwich effect” created by intra-abdominal pressure between the posterior rectus sheath and peritoneum, thereby substantially reducing or eliminating the need for traumatic fixation. 10 Studies evaluating defect closure and extraperitoneal mesh placement have demonstrated a 30%–50% reduction in early postoperative pain scores compared with intraperitoneal repairs. 11 The consistently lower pain scores observed in the vTAPP Plus group across all early time points in the present study strongly support this mechanistic rationale. Importantly, the magnitude of pain reduction observed is not only statistically significant but also clinically meaningful, particularly during the first 48 hours when pain most influences postoperative recovery. 11
Our findings align with those of several retrospective and observational studies suggesting reduced postoperative pain with extraperitoneal ventral hernia repairs.12–14 Propensity-matched analyses comparing IPOM and vTAPP have demonstrated lower early pain scores, reduced analgesic requirements by nearly 40%, and faster functional recovery with extraperitoneal techniques. However, most existing studies are limited by nonrandomized designs, heterogeneity in operative technique, and lack of standardized pain assessment. 15 By employing a randomized controlled design with predefined pain assessment intervals and standardized operative protocols, the present study significantly strengthens the evidence base supporting vTAPP Plus.
To our knowledge, this study represents one of the first randomized controlled trials directly comparing IPOM Plus and vTAPP Plus with postoperative pain as the primary outcome. This distinction is important, as many prior investigations have focused primarily on recurrence or complication rates with pain often reported as a secondary or subjective outcome.16,17 By prioritizing pain as the primary endpoint, our study adopts a patient-centered perspective increasingly emphasized in contemporary hernia research, where pain control is recognized as a key determinant of surgical success. 18
The persistence of pain differences beyond the immediate postoperative period and up to 30 days—and to a lesser extent at 3 months—deserves particular attention. While acute postoperative pain is expected following any surgical intervention, prolonged or intermediate pain can delay return to work by 1–3 weeks, impair physical function, and negatively affect quality of life. 19 The more rapid pain resolution observed following vTAPP Plus repair suggests a smoother convalescence and potentially superior functional recovery, even though formal quality-of-life instruments were not used. 20
By 3 months postoperatively, pain had resolved in nearly all patients in both groups, with only minimal residual discomfort observed in a small subset of IPOM Plus patients. At 6 months, pain outcomes were comparable. This finding is consistent with previous reports indicating that long-term pain after laparoscopic ventral hernia repair decreases to <5% by 6 months. Thus, while both techniques achieve similar long-term pain resolution, the principal advantage of vTAPP Plus lies in the early and intermediate recovery phases—an aspect highly valued by patients. 21
Table 4 and 5 shows that the operative duration was significantly lower in the IPOM plus group as compared to the vTAPP plus group with a mean difference of around 15-20 minutes. Operative duration was marginally longer in the vTAPP Plus group, reflecting the additional steps required for peritoneal flap creation and closure. Published learning curve analyses suggest that operative time may initially be 20–30 minutes longer for extraperitoneal repairs.22,23 Importantly, the increased operative time did not translate into higher complication rates, or increased morbidity, indicating that vTAPP Plus is safe when performed by experienced surgeons. 24
The learning curve associated with vTAPP Plus warrants consideration. Previous studies suggest operative efficiency improves significantly after approximately 20–30 cases, with operative times approaching those of IPOM repairs thereafter. 25 In this context, the marginally longer operative duration should be considered an acceptable trade-off for the substantial reduction in postoperative pain. 26
An important secondary advantage of vTAPP Plus is its economic profile. IPOM repair requires composite meshes and fixation devices, which have been shown to increase procedural costs by 30%–50% compared with extraperitoneal repairs. 27 In contrast, vTAPP Plus allows the use of conventional polypropylene mesh without intraperitoneal fixation, offering a cost-effective alternative—particularly relevant in low- and middle-income countries, where hernia surgery accounts for a significant proportion of general surgical workload. 28
From a safety perspective, both techniques demonstrated comparable short-term outcomes. Rates of seroma, hematoma, and surgical site infection were low and similar between groups, consistent with large series reporting overall complication rates of 5%–10% following laparoscopic ventral hernia repair. 29 No mesh infections, bowel injuries, or hernia recurrences were observed during follow-up, supporting the short-term safety and efficacy of vTAPP Plus. 30
Table 7 shows that most patients had no complications (34/36 in IPOM plus and 30/32 in TAPP plus). Seroma occurred in one TAPP plus patient only, while surgical site infection (SSI) occurred in 2 IPOM plus and 1 TAPP plus patient. The overall complication rates were low, and there was no statistically significant difference between the groups (χ² = 1.35, p = 0.508). Table 8 compares postoperative complications at 7 days between the IPOM plus (n = 36) and TAPP plus (n = 32) groups. Most patients remained free of complications, with 33 patients in the IPOM plus group and 31 patients in the TAPP plus group reporting no adverse events. Surgical site infection (SSI) occurred in 2 patients in the IPOM plus group and 1 patient in the TAPP plus group, while seroma was observed in 1 patient in the IPOM plus group only. Overall, complication rates were low and comparable between the two groups, with no statistically significant difference observed (χ² = 1.16, p = 0.559). The absence of recurrence should be interpreted cautiously given the limited follow-up duration. Hernia recurrence rates after laparoscopic repair are typically reported between 2 and 10% over long-term follow-up. However, extraperitoneal mesh placement may offer biomechanical advantages by facilitating mesh integration on both surfaces, potentially enhancing long-term durability. 31 This theoretical benefit further supports the shift toward extraperitoneal repairs.
In summary, this randomized controlled trial demonstrates that vTAPP Plus repair offers significant advantages over IPOM Plus in reducing early and intermediate postoperative pain without compromising safety or short-term efficacy. By addressing a key patient-centered outcome, this study contributes meaningfully to the evolving paradigm favoring extraperitoneal mesh placement in ventral hernia surgery. 32
Conclusion
In conclusion, laparoscopic vTAPP Plus repair is associated with a significant reduction in early and intermediate postoperative pain compared with IPOM Plus repair, with this advantage persisting for up to 3 months. By avoiding intraperitoneal mesh placement and fixation-related morbidity, vTAPP Plus offers important physiological and clinical advantages. Furthermore, extraperitoneal mesh placement allows the use of cost-effective polypropylene mesh without compromising outcomes. Taken together, these findings support vTAPP Plus as a preferred minimally invasive approach for appropriately selected patients with small-to-medium primary ventral hernias.
Authors’ Contributions
All authors have made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation of data. All authors were involved in drafting the article or revising it critically for important intellectual content. Each author has approved the final version of the article and agrees to be accountable for all aspects of the work in accordance with the recommendations of the International Committee of Medical Journal Editors.
Footnotes
Acknowledgments
The authors would like to thank the surgical team, nursing staff, and research personnel who contributed to patient care and data collection during the conduct of this study. They also express their sincere gratitude to all the patients who consented to participate in this randomized controlled trial as, their cooperation made this research possible.
Author Disclosure Statement
The authors declare that they have no conflicts of interest related to this study.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.