
Abstract
Background:
Holmium laser enucleation of the prostate (HoLEP) has emerged as an alternative for benign prostatic obstruction (BPO), with fewer perioperative and functional complications. However, its comparative performance relative to robot-assisted simple prostatectomy (RASP) remains debated, requiring updated evaluation.
Methods:
A systematic review and meta-analysis of studies comparing HoLEP and RASP was performed using PubMed, Scopus, and Cochrane databases through August 2025. Outcomes were pooled using mean differences (MDs) and odds ratios (ORs) with random-effects models. Risk of bias assessment and trial sequential analysis were conducted to evaluate the robustness of evidence.
Results:
Thirteen studies, including 1993 patients, were analyzed. HoLEP was associated with shorter operative time (MD = −32.05 minutes), lower transfusion rates (OR = 0.34), fewer Clavien–Dindo grades III and IV complications (OR = 0.39), and earlier catheter removal (MD = −3.84 days). Postoperative International Prostate Symptom Score modestly favored RASP (MD = 0.96). No significant differences were observed in quality of life, maximum urinary flow rate, International Index of Erectile Function, prostate-specific antigen reduction, postvoid residual volume, estimated blood loss, specimen weight, hospital stay, minor complications, trifecta achievement, or postoperative urge and stress incontinence.
Conclusion:
HoLEP provides improved perioperative safety with largely comparable functional outcomes compared with RASP. Further high-quality comparative studies are needed to confirm long-term effectiveness.
Keywords
Introduction
Benign prostatic obstruction (BPO) is a common condition in urological practice worldwide, and its prevalence increased by 112% between 1990 and 2021, leading to a growing number of patients requiring surgical intervention. 1 In men with very large prostates, typically >80–100 g, surgical management has historically relied on open simple prostatectomy, a procedure associated with considerable perioperative morbidity.1,2 Robot-assisted simple prostatectomy (RASP) was introduced as a minimally invasive alternative designed to replicate the principles of anatomical adenoma enucleation while reducing surgical morbidity and is therefore primarily used for the management of large prostate glands in centers with robotic expertise. 3
More recently, attention has shifted toward endoscopic techniques that may offer comparable efficacy with lower surgical invasiveness. 4 Among these, holmium laser enucleation of the prostate (HoLEP) was developed as a transurethral technique capable of achieving anatomical adenoma enucleation while maintaining the advantages of endoscopic surgery, including reduced bleeding, shorter catheterization time, and faster postoperative recovery.5,6 Importantly, HoLEP has demonstrated effectiveness across all prostate sizes, including very large glands, and can also be performed concomitantly with procedures such as bladder stone treatment.4,7
Given that HoLEP is an effective minimally invasive technique applicable to prostates of any size, the role of RASP—typically reserved for prostates larger than 100 g and associated with higher procedural costs—has increasingly been questioned. 8 Two previous meta-analyses compared HoLEP and RASP for the surgical management of BPO.9,10 While the first was criticized for methodological limitations, the second was more robust; however, two recently published studies have expanded the available evidence, warranting an updated analysis.11,12 Therefore, this study integrates the most recent evidence with additional trial sequential analysis (TSA), meta-regression, and subgroup analyses to further clarify this debate.
Materials and Methods
This systematic review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, as outlined in Supplementary Table S1. 13 The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the identifier CRD420251123887. 14 Ethics committee approval and informed consent were not required because this study was based exclusively on previously published data.
Systematic search process
A comprehensive literature search was conducted in PubMed, the Cochrane Central Register of Controlled Trials, and Scopus to identify relevant studies published up to August 2025. The search strategy combined controlled vocabulary and free-text terms related to BPO (e.g., benign prostatic hyperplasia, lower urinary tract symptoms), HoLEP, and RASP. The full search strategies for each database are provided in Supplementary Table S2.
Study selection criteria
We included randomized controlled trials (RCTs) and observational studies that evaluated HoLEP versus RASP for BPO. Studies were excluded if they met any of the following: (1) evaluation of other surgical or minimally invasive modalities for BPO (e.g., photoselective vaporization, aquablation or open simple prostatectomy); (2) lack of a direct comparative group between HoLEP and RASP; (3) insufficient or unclear reporting of perioperative or functional outcomes relevant to comparison; (4) publication in non-original research formats (including single-arm trials, case reports, conference abstracts, meta-analyses, narrative reviews, or animal studies); (5) overlapping patient populations, in which case the most recent or most comprehensive dataset was retained.
Data extraction and endpoints
Two independent reviewers (G.L.G. and G.B.P.) independently screened the retrieved articles for eligibility and extracted data from studies that met the inclusion criteria. Any discrepancies were resolved through consensus, and when necessary, a third reviewer (B.F.P.) acted as an adjudicator. The following intraoperative and postoperative outcomes were assessed: (1) postoperative International Prostate Symptom Score (IPSS); (2) postprocedure Quality of Life index (QoL index); (3) postoperative Qmax, mL/s (maximum flow rate); (4) postoperative International Index of Erectile Function (IIEF); (5) postprocedure prostate-specific antigen (PSA) reduction, ng/mL; (6) postvoid residual (PVR), cm3; (7) operative time, min; (8) estimated blood loss, mL; (9) transfusion; (10) specimen weight, grams; (11) time to catheter removal, days; (12) Clavien–Dindo grades I–II; (13) Clavien–Dindo grades III and IV; (14) TRIFECTA (simultaneous achievement of: absence of postoperative complications, urinary continence at follow-up, and postoperative maximum urinary flow rate (Qmax) >15 mL/s); (15) postoperative urge incontinence; (16) postoperative stress incontinence; and (17) hospital stay, days.
Quality assessment
Two reviewers (B.F.P. and G.L.B.) independently assessed the risk of bias of the included RCTs using the Revised Cochrane Risk-of-Bias Tool (RoB 2). 15 Each trial was categorized as having low risk, high risk, or some concerns across five domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Disagreements were resolved through discussion, with arbitration by a third or senior reviewer when required. The same reviewers also evaluated the quality of the included non-randomized studies using the ROBINS-I tool, classifying each study as having critical, serious, moderate, or low risk of bias across seven domains: confounding, selection, classification, deviations from intended interventions, missing data, measurement of the outcome, and selection of reported results. 16
The certainty of evidence for each outcome was evaluated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach, which classifies the quality of evidence as very low, low, moderate, or high. Publication bias was explored through visual inspection of funnel plot symmetry and formally tested with Egger’s regression test when ≥10 studies were available for a given outcome. 17
Statistical analysis
Binary outcomes were summarized by calculating odds ratios (ORs) with their corresponding 95% confidence intervals (CIs), while continuous outcomes were analyzed using mean differences (MDs) with 95% CIs. When continuous data were reported as median and range or interquartile range (IQR), the corresponding mean and standard deviation (SD) were estimated using the methods proposed by Luo et al. (2018) and Wan et al. (2014), respectively.18,19 Pooled proportions were derived through inverse variance weighting following logit or logarithmic transformations when appropriate. All pooled estimates were derived using a random-effects model according to the DerSimonian and Laird method. 20 A P value <0.05 was considered statistically significant. Between-study heterogeneity was assessed using the Cochran Q test and the I2 statistic, with heterogeneity considered substantial when I2 exceeded 25% and the Q test P value was <0.10. All statistical analyses were conducted using R software, version 4.4.2, while TSA was performed using TSA software version 0.9.5.10. 21
Sensitivity analysis
For outcomes showing notable heterogeneity (I2 ≥ 25%), two complementary sensitivity analyses were performed. First, Baujat plots were generated to identify studies that contributed most to both the overall effect size and the observed heterogeneity. 22 Second, a leave-one-out analysis was conducted, systematically excluding each study in turn to assess the robustness of the results and the influence of individual studies. Additionally, a random-effects meta-regression analysis was performed exclusively for the operative time outcome to explore whether prostate volume could explain part of the observed heterogeneity. Regression coefficients with corresponding 95% CIs were calculated, and a P value of <0.05 was considered statistically significant.
Predefined subgroup analyses were conducted according to prostate size (≥150 versus <150 g) to explore potential effect modification. Finally, TSA was applied to account for random errors and to determine whether the cumulative evidence had reached the required information size. TSA was performed irrespective of the magnitude of statistical heterogeneity observed across studies. Analyses were interpreted using O’Brien–Fleming alpha-spending boundaries, with a two-sided alpha of 5% and beta of 20%, based on the pooled MD and between-study heterogeneity (D2) under a random-effects model.
Results
Study inclusion and baseline characteristics
As shown in Figure 1, the systematic search initially identified 1301 records. After removal of 530 duplicates, 771 records were screened based on titles and abstracts, resulting in the exclusion of 752 studies. Nineteen full-text articles were assessed for eligibility, and one additional study was identified through backward snowballing. Seven studies were excluded for predefined reasons detailed in Supplementary Table S3. Ultimately, 13 studies were included, comprising 12 observational comparative studies and 1 RCT.8,11,12,23–32
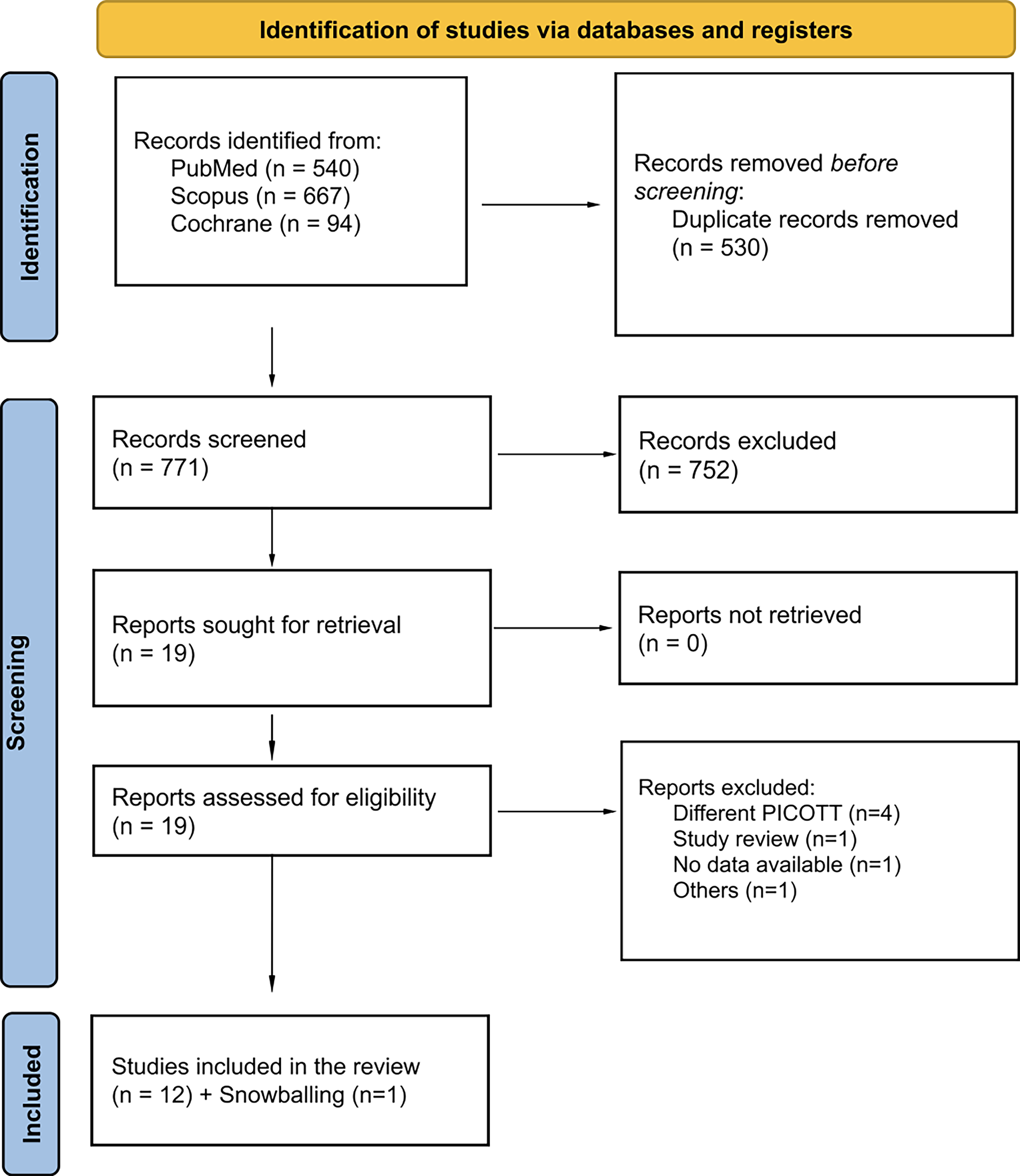
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of study screening and selection.
Overall, 1993 patients undergoing surgery for BPO were analyzed, including 1380 (69.2%) treated with HoLEP and 613 (30.8%) treated with RASP. Mean follow-up duration was 10.87 ± 12.02 and 14.46 ± 15.14 months, respectively. Among studies reporting baseline characteristics, mean age was 71.31 ± 8.19 versus 70.96 ± 7.84 years, while body mass index was 26.89 ± 4.47 and 27.19 ± 5.20 kg/m2, respectively. Preoperative PSA levels were 7.07 ± 6.58 and 8.13 ± 6.31 ng/mL, with comparable proportions of American Society of Anesthesiologists class III and IV patients (20.3% versus 20.5%). Mean prostate volume was 144.65 ± 54.57 and 152.72 ± 67.15 g, respectively.
Across studies, procedures were performed using holmium: YAG laser systems for endoscopic enucleation and contemporary da Vinci robotic platforms for robotic surgery. A 550 µm laser fiber with a 26 Fr resectoscope was the most commonly reported configuration for endoscopic procedures, whereas robotic surgery typically employed a four-arm setup. Patient positioning was generally lithotomy for endoscopic surgery and Trendelenburg for robotic procedures. The Gilling technique represented the predominant enucleation approach. Postoperative catheterization most frequently involved 20 Fr catheters after endoscopic surgery and 18 Fr Foley catheters after robotic surgery. Detailed characteristics are summarized in Tables 1 and 2
Baseline Characteristics of the Included Studies
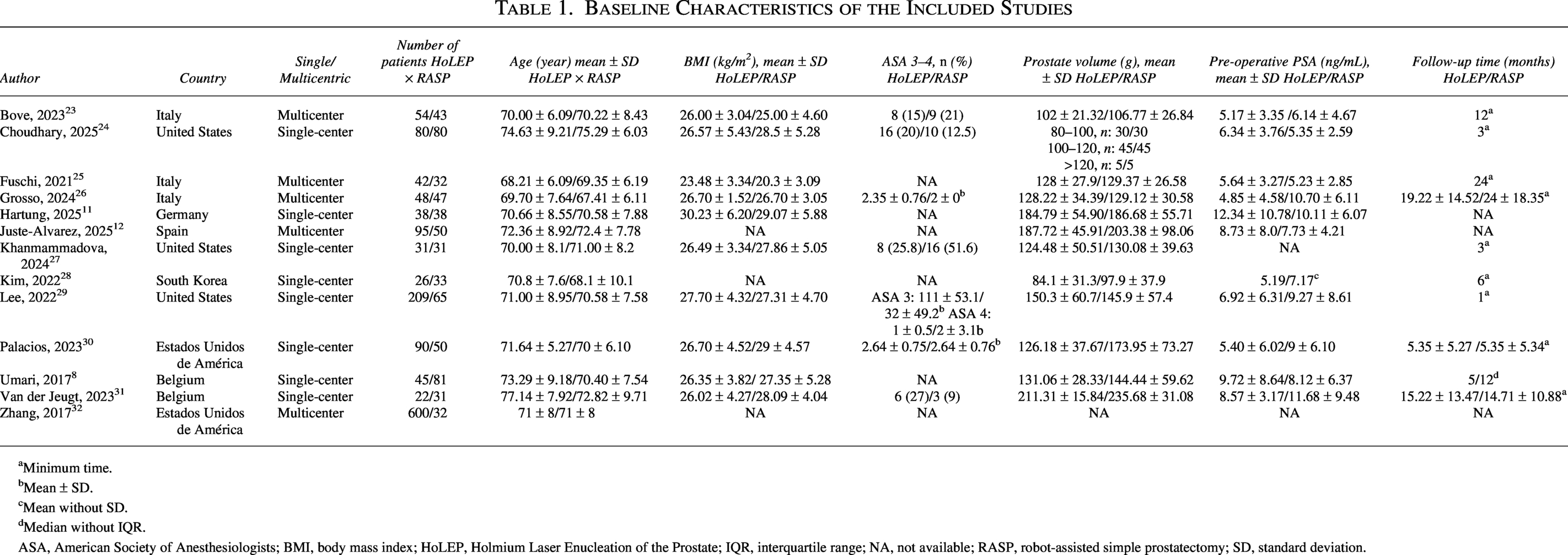
aMinimum time.
Mean ± SD.
Mean without SD.
dMedian without IQR.
ASA, American Society of Anesthesiologists; BMI, body mass index; HoLEP, Holmium Laser Enucleation of the Prostate; IQR, interquartile range; NA, not available; RASP, robot-assisted simple prostatectomy; SD, standard deviation.
Operative Technique and Perioperative Management across Included Studies
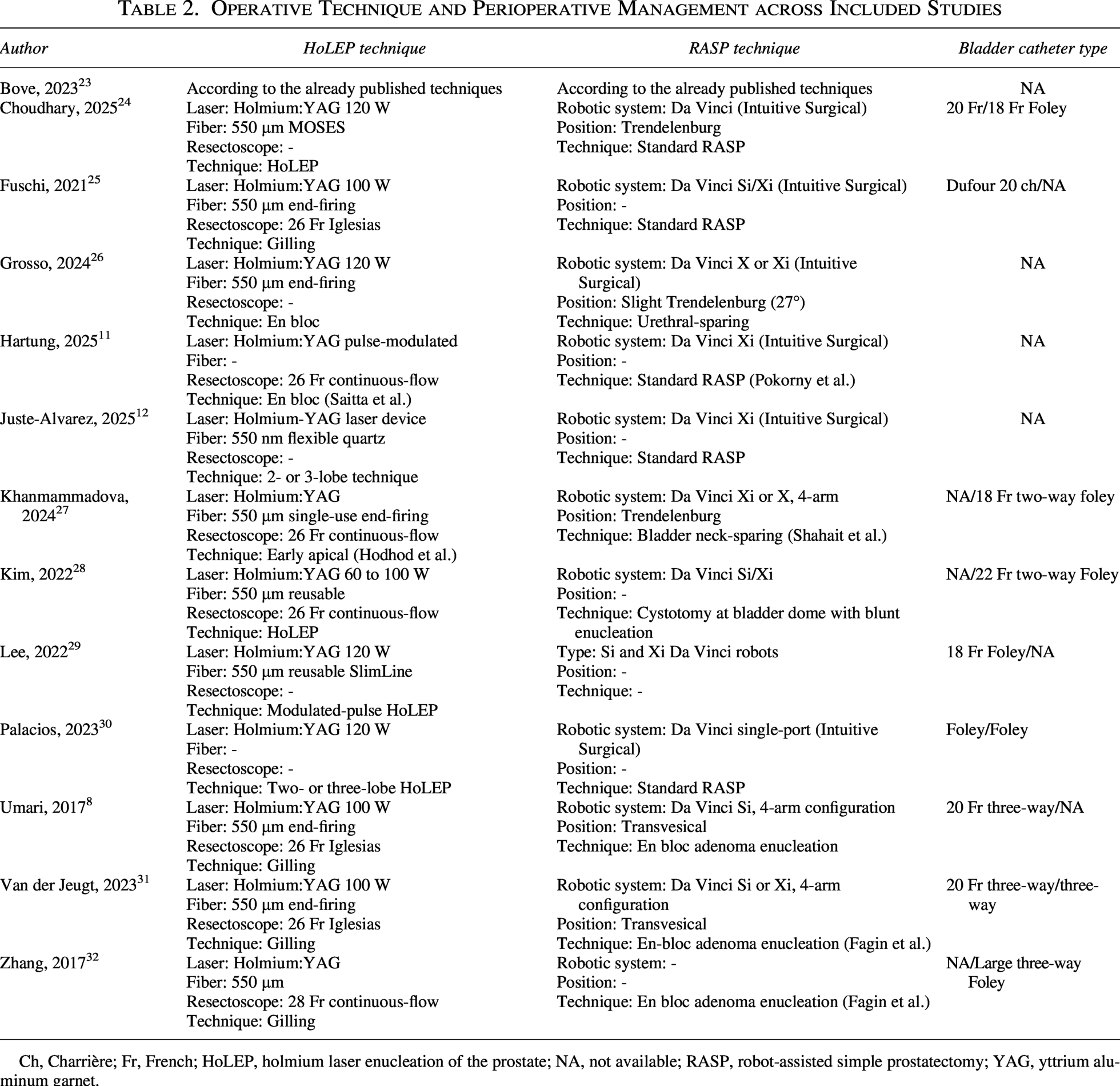
Ch, Charrière; Fr, French; HoLEP, holmium laser enucleation of the prostate; NA, not available; RASP, robot-assisted simple prostatectomy; YAG, yttrium aluminum garnet.
Pooled analyses of the included studies
Postoperative functional outcomes.
In pooled analysis, HoLEP was associated with a slightly higher postoperative IPSS score, indicating worse symptom improvement compared with RASP (MD = 0.96; 95% CI: 0.17–1.75; P = .018; I2 = 49.1%; Fig. 3A).8,12,23–26,30,31 No significant differences were observed for QoL score, Qmax, IIEF, postoperative PSA, or PVR (Figs. 3B–D and 4A, B).8,12,23,25–27,29–31 Substantial heterogeneity was observed across most functional outcomes, except for PVR, which showed low heterogeneity (I2 = 19.4%), suggesting variability in patient selection, follow-up duration, and reporting of functional measures among included studies.
Forest plots comparing holmium laser enucleation (HoLEP) and robot-assisted simple prostatectomy (RASP) approaches for benign prostatic obstruction:
Forest plots comparing holmium laser enucleation (HoLEP) and robot-assisted simple prostatectomy (RASP) approaches for benign prostatic obstruction:
Perioperative outcomes.
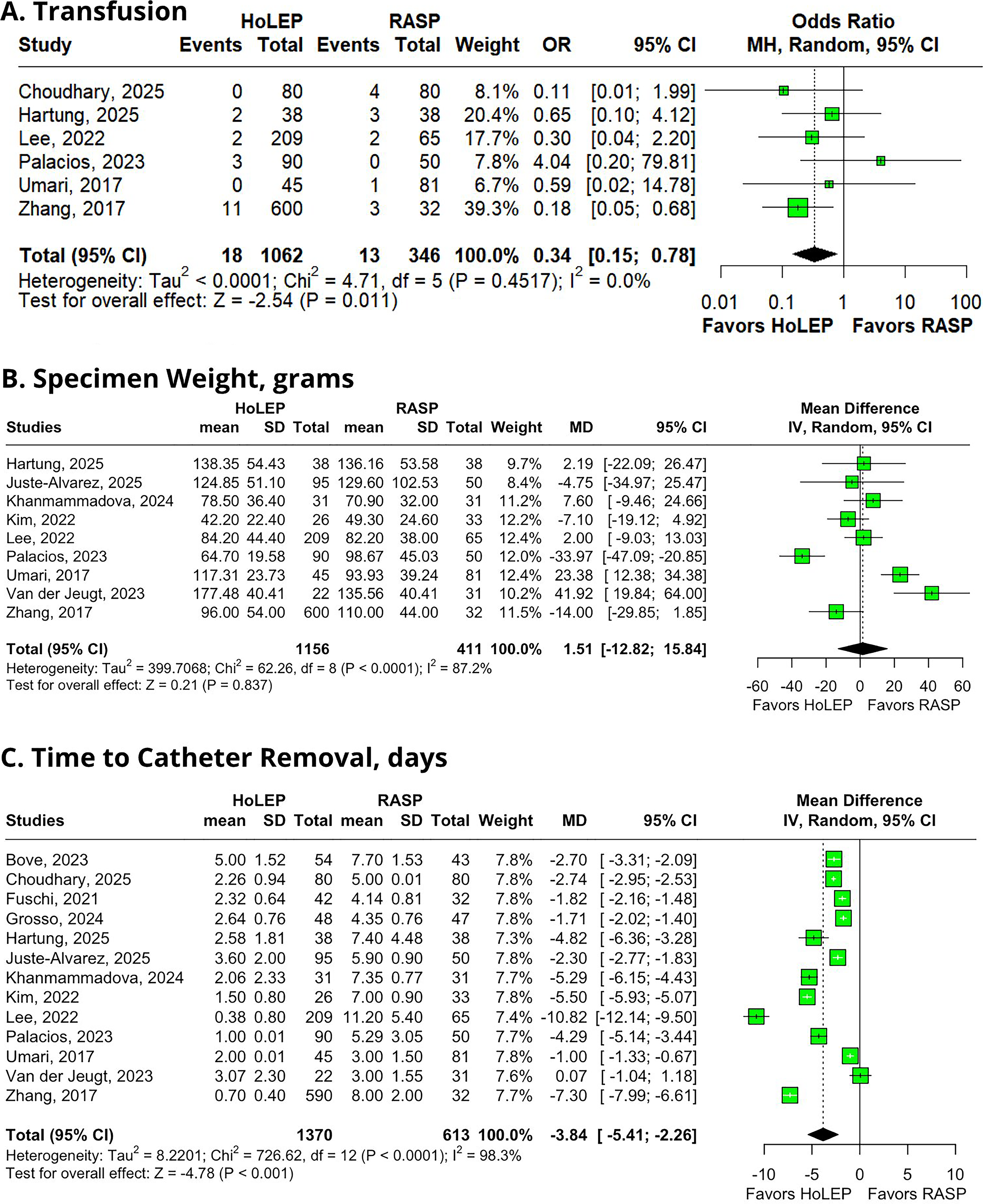
HoLEP was associated with a significant reduction in operative time (minutes) (MD = −32.05; 95% CI: −63.94 to −0.17; P = .049; Fig. 4C),8,11,12,23–32 lower transfusion rates (OR = 0.34; 95% CI: 0.15–0.78; P = .011; Fig. 5A),8,11,24,29,30,32 and earlier catheter removal (days) (MD = −3.84; 95% CI: −5.41 to −2.26; P < .001; Fig. 5C).8,11,12,23–32 No significant differences were observed for estimated blood loss (mL) or specimen weight (grams) (Figs. 4D and 5B).8,11,12,27–32 Heterogeneity was substantial for most outcomes, likely reflecting differences in surgical expertise, institutional volume, and perioperative protocols, except for transfusion rates, which showed no heterogeneity (I2 = 0%).
Forest plots comparing holmium laser enucleation (HoLEP) and robot-assisted simple prostatectomy (RASP) approaches for benign prostatic obstruction:
Postoperative complications and recovery.
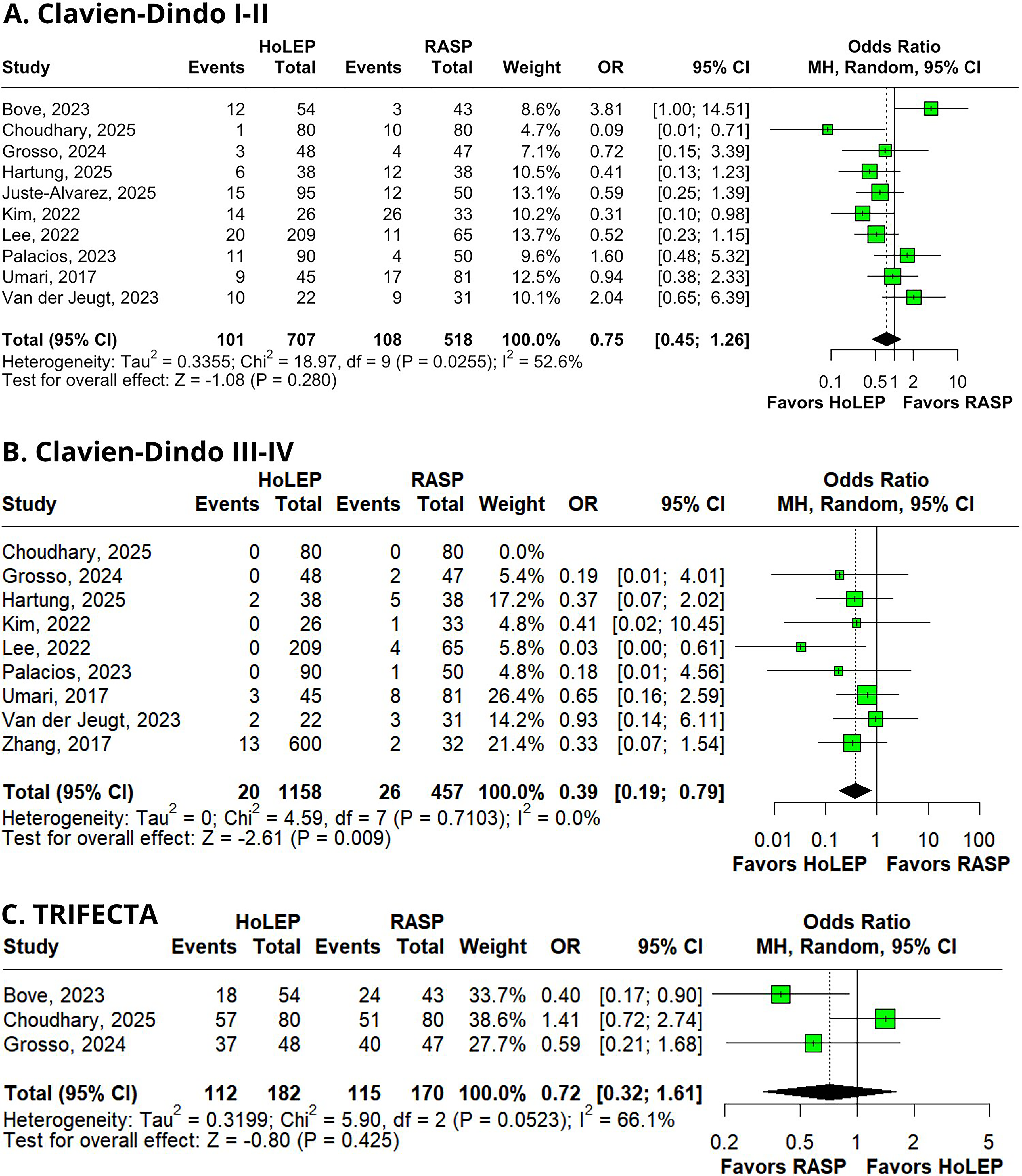
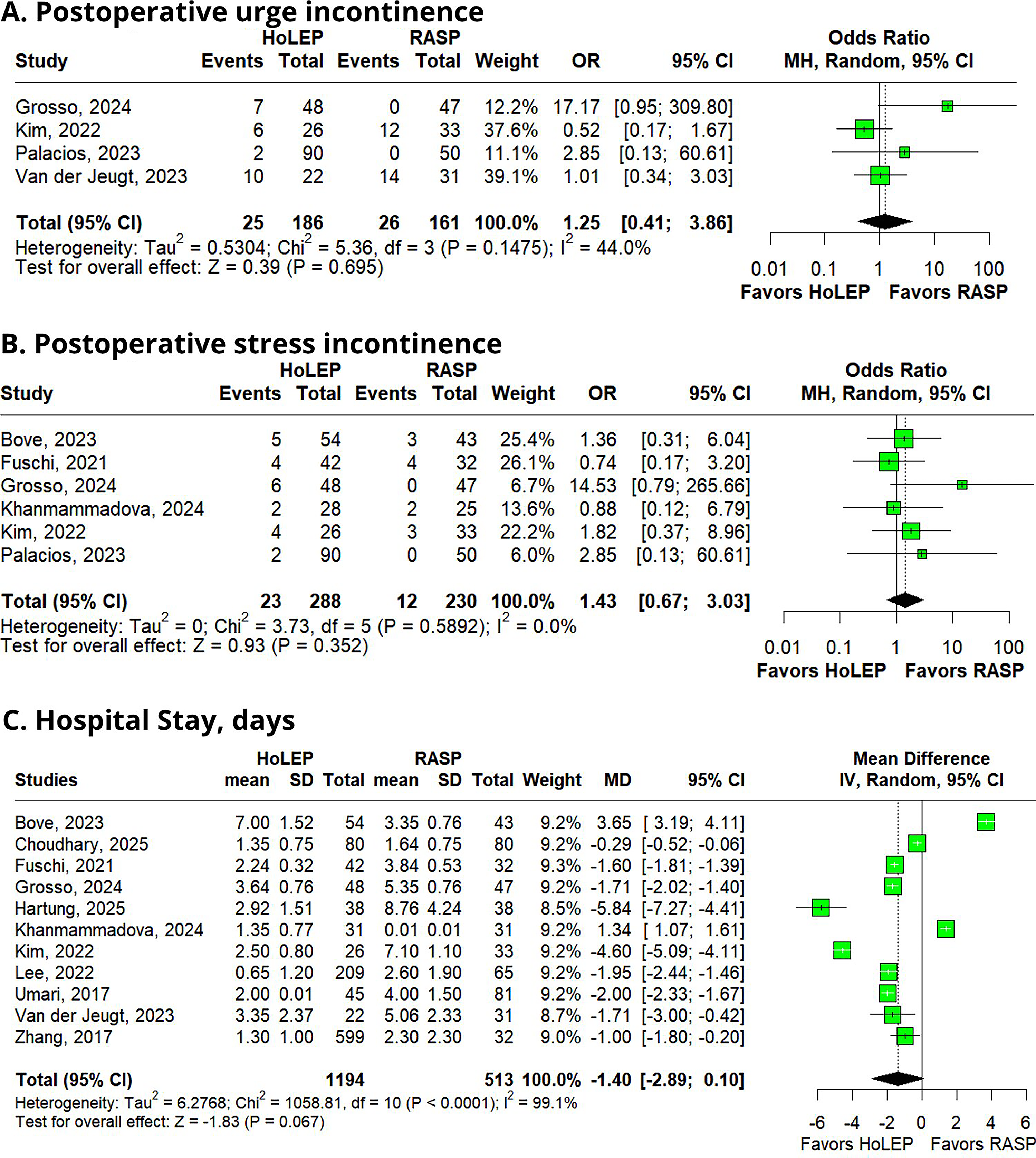
HoLEP showed no significant differences in minor complications (Clavien–Dindo grades I and II) (OR = 0.75; 95% CI: 0.45–1.26; P = .414; I2 = 52.6%; Fig. 6A),8,11,12,23,24,26,28–31 urge incontinence (OR = 1.25; 95% CI: 0.41–3.86; P = .695; I2 = 44.0%; Fig. 7A),26,28,30,31 stress incontinence (OR = 1.43; 95% CI: 0.67–3.03; P = .352; I2 = 0.0%; Fig. 7B),23,25–28,30 TRIFECTA achievement (OR = 0.72; 95% CI: 0.32–1.61; P = .425; I2 = 66.1%; Fig. 6C),23,24,26 or hospital length of stay (MD = −1.40 days; 95% CI: −2.89 to 0.10; P = .067; I2 = 99.1%; Fig. 7C).8,11,23–29,31,32
Meta-regression for operative time.
Risk of bias assessment of included studies according to the Cochrane RoB 2 and ROBINS-I tools. ROB 2, Revised Cochrane Risk-of-Bias Tool.
In contrast, HoLEP was associated with a significantly lower risk of major complications (Clavien–Dindo grades III and IV) (OR = 0.39; 95% CI: 0.19–0.79; P = .009; I2 = 0.0%; Fig. 6B).8,11,24,26,28–32 Heterogeneity ranged from moderate to considerable across postoperative outcomes, particularly for hospital stay, indicating variability in discharge practices and health care systems rather than procedural differences alone, while major complication outcomes remained highly consistent across studies.
Subgroup analysis
In the subgroup analysis according to prostate size (≥150 versus <150 g), postoperative IPSS remained significantly lower in the RASP group across both size categories. Notably, Qmax became significant in the ≥150 g subgroup, favoring HoLEP, suggesting a potential advantage of enucleation in larger prostates. Other outcomes largely mirrored the overall analysis across size categories (Supplementary Figures S48, S49, S50, S51, S52, S53, S54, S55, S56, S57, S58, and S59).
Sensitivity analyses
Baujat plot analysis was performed to identify studies contributing most to between-study heterogeneity. For postoperative functional outcomes, Juste Alvarez et al. 12 contributed most to variability in postoperative IPSS and Qmax analyses; however, exclusion of this study reduced heterogeneity without altering the direction or statistical significance of pooled estimates, confirming robustness of these outcomes (Supplementary Figs. S1 and S2 and S5 and S6).
For quality of life, Grosso et al. 26 showed the greatest influence, yet removal of this study did not modify the overall nonsignificant result (Supplementary Figs. S3 and S4). Similarly, erectile function outcomes were primarily influenced by Bove et al., 23 although pooled estimates remained unchanged after exclusion (Supplementary Figs. S7 and S8). Postoperative PSA variability was mainly driven by Van der Jeugt et al., 31 with sensitivity analysis reducing heterogeneity but not modifying the overall neutral effect (Supplementary Figs. S9 and S10).
Regarding perioperative outcomes, Zhang et al. 32 had the greatest influence on operative time heterogeneity; however, exclusion did not materially change the pooled effect favoring HoLEP (Supplementary Figs. S11 and S12). Estimated blood loss results were mainly influenced by Lee et al., 29 and removal of this study improved consistency without altering the statistical conclusions (Supplementary Figs. S13 and S14). Specimen weight analyses were influenced by Palacios et al. 30 and Umari et al., 8 although pooled estimates remained stable across sensitivity analyses (Supplementary Figs. S15 and S16).
For postoperative recovery metrics, Lee et al. 29 contributed most to variability in time to catheter removal; nevertheless, the benefit associated with HoLEP persisted after sequential exclusion, confirming robustness of this finding (Supplementary Figs. S17 and S18).
In complication outcomes, Bove et al. 23 influenced minor complication variability, but pooled estimates remained nonsignificant after exclusion (Supplementary Figs. S19 and S20). TRIFECTA outcomes were mainly influenced by Choudhary et al., 24 while urge incontinence variability was largely related to Grosso et al. 26 ; in both cases, exclusion did not modify pooled results (Supplementary Figures S21, S22, S23, and S24).
In contrast, hospital length of stay was mainly influenced by Bove et al., 23 and sensitivity analyses showed fluctuating effect estimates that remained nonsignificant, suggesting lower robustness for this outcome compared with other analyzed endpoints (Supplementary Figs. S25 and S26).
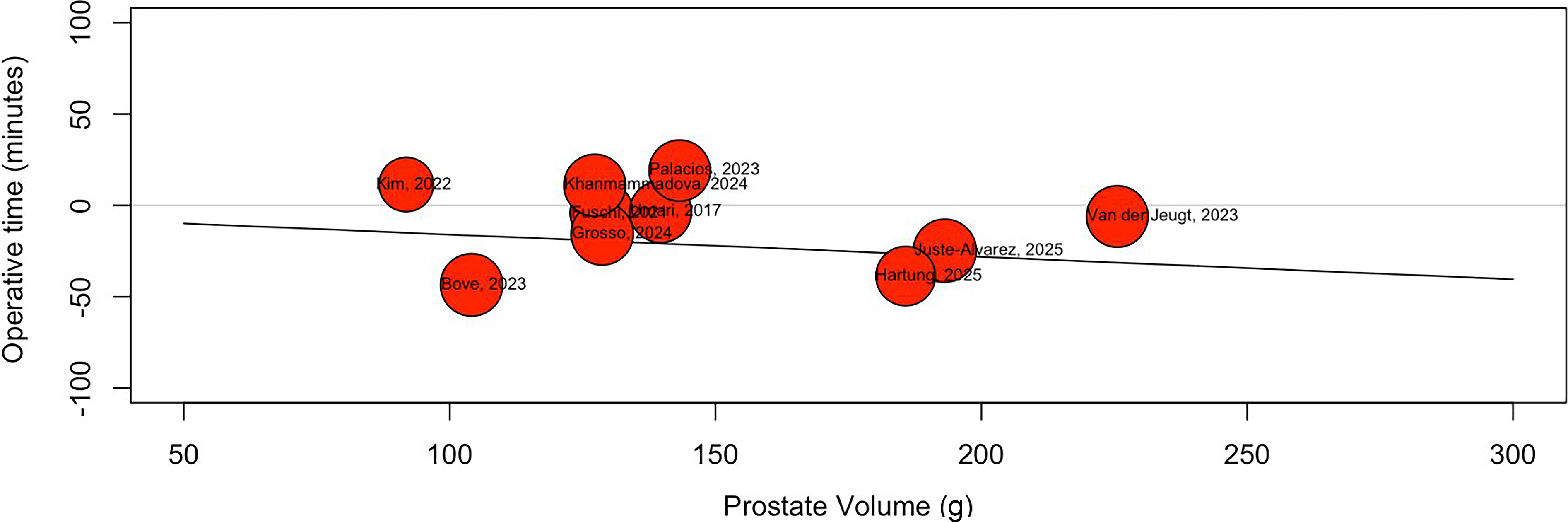
Meta-regression analysis (Fig. 8A) did not demonstrate a significant association between prostate volume and operative time. Although a slight negative trend was observed, the regression slope was minimal, and substantial between-study variability remained. These findings suggest that prostate volume did not significantly influence operative time across the included studies.
Meta-regression for operative time.
Trial-sequential analysis
TSA plots are presented in Supplementary Figures S31, S32, S33, S34, S35, S36, S37, S38, S39, S40, S41, S42, S43, S44, S45, S46, and S47. Overall, TSA was performed to evaluate the robustness of cumulative evidence and to control for potential risks of type I and type II random errors associated with repeated significance testing in cumulative meta-analysis.
For selected outcomes demonstrating statistically significant findings in the conventional meta-analysis, TSA provided confirmation of robust evidence. Specifically, outcomes such as transfusion rate, time to catheter removal, and Clavien–Dindo grades III and IV complications showed cumulative Z-curves crossing both the conventional significance boundary and the trial sequential monitoring boundary. In these analyses, the accumulated sample size exceeded the required information size, supporting a reliable treatment effect with a low probability of random error (Supplementary Figs. S39, S41, and S43).
In contrast, some outcomes that reached statistical significance in conventional meta-analysis did not demonstrate firm confirmation when evaluated using TSA. For operative time, the cumulative Z-curve crossed the conventional significance threshold but failed to clearly surpass the sequential monitoring boundary and did not achieve the required information size. For postoperative IPSS, the cumulative Z-curve did not cross either the conventional or sequential monitoring boundaries, and the required information size was not reached. These findings suggest that the available evidence for these outcomes remains inconclusive and potentially susceptible to random error, indicating that additional studies may modify the observed estimates (Supplementary Figs. S31 and S37).
For several secondary outcomes, including postoperative QoL index, Qmax, IIEF scores, postoperative PSA levels, PVR, specimen weight, minor complications (Clavien–Dindo grades I and II), TRIFECTA achievement, urinary incontinence outcomes, and length of stay, the cumulative Z-curves remained within the monitoring boundaries and did not reach the required information size. These results indicate that current evidence remains inconclusive, and that further adequately powered comparative studies are required (Supplementary Figures S32–S36, S40–S42, and S44, S45, S46, and S47).
Additionally, certain outcomes demonstrated discordance between conventional meta-analysis and TSA findings, such as estimated blood loss, where the cumulative Z-curve crossed monitoring boundaries despite nonsignificant pooled estimates. Such discrepancies may reflect differences in modeling assumptions or heterogeneity adjustments within TSA and therefore should be interpreted cautiously until further evidence becomes available (Supplementary Fig. S38).
Overall, TSA indicates that only a subset of evaluated outcomes currently provides firm and reliable evidence, whereas most functional and perioperative endpoints remain underpowered. Consequently, the present findings highlight the need for additional high-quality comparative studies to establish definitive conclusions regarding comparative effectiveness.
Quality assessment and certainty
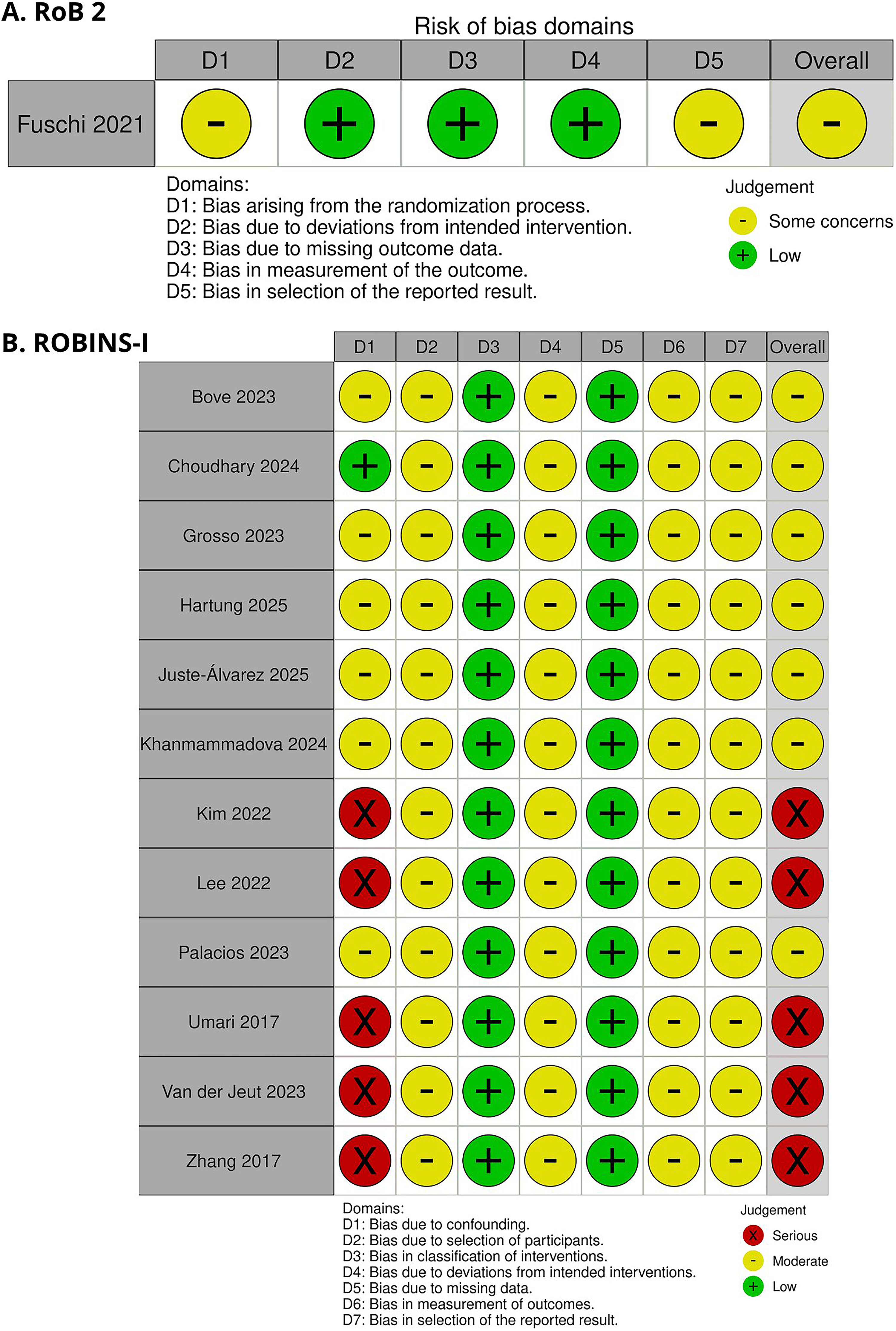
An overview of the study-specific risk-of-bias assessments is presented in Figure 9A and B. The RCT was evaluated using the RoB 2 tool and was judged to raise some concerns regarding risk of bias. These concerns were primarily related to insufficient reporting of the random sequence generation process, unclear allocation concealment, and the absence of a prespecified statistical analysis protocol. 25 Among the 13 observational studies, seven were classified as having a moderate risk of bias. The primary limitations were residual confounding due to reliance on multivariable adjustment without propensity score methods, retrospective study design with treatment decisions influenced by institutional practice, heterogeneity in perioperative management across centers, lack of blinded outcome assessment for functional endpoints, and absence of a prespecified protocol, potentially increasing the risk of selective reporting.11,12,23,24,26,27,30 The remaining studies were considered to be at high risk of bias, mainly due to the absence of adequate strategies to control for confounding. Specifically, no propensity score methods or multivariable adjustments were performed, and comparisons were based on unadjusted observational analyses without control for baseline imbalances or key prognostic variables. This lack of statistical control substantially compromises internal validity and increases the risk of biased effect estimates.8,28,29,31,32 None of the included studies were classified as being at low risk of bias.
Risk of bias assessment of included studies according to the Cochrane RoB 2 and ROBINS-I tools. ROB 2, Revised Cochrane Risk-of-Bias Tool.
According to the GRADE approach, moderate certainty of evidence was assigned to the outcomes of transfusion and Clavien–Dindo grades III and IV complications. In contrast, postoperative IPSS, time to catheter removal, and operative time were rated as low certainty. Detailed GRADE assessments for each outcome are provided in Supplementary Table S4.
Funnel plot inspection did not reveal substantial asymmetry for the assessed outcomes. Egger’s regression test showed no evidence of small-study effects for operative time (P = .330), hospital stay (P = .648), time to catheter removal (P = .102), and Clavien–Dindo grades I and II (P = .973), with all P values exceeding the predefined threshold for statistical significance. Overall, these findings indicate a low risk of publication bias, suggesting that the results of this meta-analysis are unlikely to be meaningfully influenced by selective reporting or small-study effects (Supplementary Figures S27, S28, S29, and S30; Supplementary Table S5).
Discussion
In this systematic review and meta-analysis of 13 studies including 1993 patients with BPO, the main findings were as follows: (1) HoLEP demonstrated improved perioperative efficiency, including shorter operative time, earlier catheter removal, and lower transfusion rates; (2) HoLEP was associated with a significantly lower risk of major complications (Clavien–Dindo grades III and IV); (3) most functional and continence outcomes were comparable between HoLEP and RASP; and (4) although postoperative IPSS statistically favored RASP, the MD was less than one point and therefore unlikely to represent a clinically meaningful difference given that the minimal clinically important difference for IPSS is approximately three points.33,34
HoLEP was introduced in the late 1990s as a minimally invasive endoscopic technique designed to reproduce the anatomical enucleation achieved by open prostatectomy while reducing surgical morbidity.5,7 By using the holmium:YAG laser, the procedure enables precise dissection along the prostatic surgical capsule while simultaneously coagulating small vessels during tissue separation, thereby maintaining continuous hemostasis throughout the enucleation process.6,7 In contrast to mechanical dissection or sharp excision techniques, the laser provides both cutting and coagulative effects, which may limit intraoperative vascular injury during adenoma removal. 6 Given these technical characteristics, HoLEP has been hypothesized to reduce perioperative bleeding and transfusion requirements compared with surgical approaches that rely on mechanical excision and reconstructive steps.6,35
HoLEP was associated with significantly lower transfusion rates in the present meta-analysis. These findings are consistent with early clinical series evaluating laser enucleation techniques. In large single-arm cohorts, HoLEP has consistently demonstrated very low transfusion requirements despite being performed in patients with large prostates. For example, Kuntz et al. 35 reported minimal intraoperative blood loss and negligible transfusion rates in their early experience with HoLEP for large glands, while Naspro et al. 6 observed similar findings in a prospective comparison between HoLEP and open prostatectomy. Subsequent observational studies have also reported transfusion rates typically below 1%–2% for HoLEP, even in glands exceeding 100 g, suggesting that the hemostatic properties of the holmium laser may play a central role in reducing perioperative bleeding.5,7 Together, these data support the hypothesis that laser-based enucleation provides effective vascular control during adenoma dissection, which may explain the lower transfusion rates observed in the present pooled analysis.
Reduced perioperative bleeding may contribute to this finding, since lower bleeding decreases clot formation and the risk of clot-related urinary retention, which may otherwise necessitate prolonged catheterization and bladder irrigation. In the present meta-analysis, HoLEP was associated with significantly earlier catheter removal compared with RASP. 6 For example, Kuo et al. reported a mean catheterization time of approximately 1 day following HoLEP in a large single-arm cohort, while Shah et al. described similarly short catheterization durations with minimal clot retention despite the treatment of large prostate glands.36,37 In contrast, RASP typically involves a transvesical incision with cystotomy closure, which often requires longer catheterization to ensure adequate bladder healing. 38 These procedural differences may explain the earlier catheter removal observed with HoLEP in our pooled analysis.
Moreover, it is well established that operative time is shorter in HoLEP compared with RASP, and our study is consistent with these findings. This difference may be explained by the technical steps required for robotic simple prostatectomy. RASP generally involves trocar placement, robotic docking, bladder incision, adenoma enucleation, and cystotomy reconstruction, all of which may prolong operative duration. 38 In contrast, HoLEP is performed through a transurethral approach without abdominal access or reconstructive suturing. 7 Although HoLEP has a well-recognized learning curve, operative efficiency improves substantially with surgical experience. El-Hakim et al. (2002) and Shah et al. (2007) have suggested that proficiency may be achieved after approximately 20–50 procedures, with progressive reductions in operative time thereafter.36,39 In the same way, large HoLEP series have consistently reported operative times comparable to or shorter than those of simple prostatectomy, even in patients with large prostate glands. These technical and experiential factors may explain the shorter operative time observed with HoLEP in our pooled analysis.
Shorter operative duration may partly explain the lower incidence of major complications (Clavien–Dindo grades III and IV) observed in the present analysis. Prolonged surgical procedures increase anesthetic exposure and physiological stress, factors associated with higher perioperative morbidity. 40 Consistent with this concept, HoLEP demonstrated significantly shorter operative time in our meta-analysis. Previous comparative studies have also reported favorable perioperative outcomes and comparable or lower postoperative complication rates with laser enucleation techniques.
This meta-analysis has several limitations that should be considered when interpreting the findings. First, although 13 studies were included, only one was an RCT, while the remaining were observational, which may increase the risk of bias and limit the overall strength of the evidence. To further assess the robustness of the findings despite this limitation, TSA was performed. Second, follow-up duration was variably reported across studies and was generally limited, restricting the ability to fully evaluate the long-term durability of functional outcomes, continence recovery, and delayed complications following HoLEP or RASP. Third, considerable variability in surgical techniques, perioperative management, and institutional protocols across studies, as well as differences in prostate size distribution among study populations, may have contributed to heterogeneity in perioperative outcomes. To explore this potential source of heterogeneity, meta-regression and subgroup analyses according to prostate size were performed.
Conclusions
HoLEP was associated with significantly lower transfusion rates, fewer Clavien–Dindo grades III and IV complications, shorter operative time, and reduced time to catheter removal. Postoperative IPSS modestly favored RASP. Overall, these findings support HoLEP as an effective and less invasive surgical option for the management of BPO, offering important perioperative advantages while maintaining comparable functional outcomes.
Footnotes
Acknowledgments
The authors thank all collaborators who contributed to this study.
Disclosure Statement
All authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this work.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.