
Abstract
Background:
Pediatric noncommunicating hydrocele (NCH) requires surgical treatment when spontaneous resolution does not occur. Although communicating hydrocele is typically treated with high ligation alone, NCH traditionally requires hydrocelectomy with high ligation. Evidence comparing laparoscopic hydrocelectomy and simple aspiration in children remains limited.
Methods:
We retrospectively analyzed 2500 children under 10 years who underwent laparoscopic management for NCH between 2016 and 2024. Patients were categorized into scrotal hydrocele (SH) and encysted spermatic cord hydrocele (ESCH), and surgical methods were classified as hydrocelectomy or aspiration, both combined with high ligation. Operative outcomes and recurrence were compared between subtypes and surgical techniques.
Results:
Among 2500 patients (SH: 862; ESCH: 1638), ESCH had a significantly higher association with inguinal hernia (13.6% versus 9.2%; P < .001). Most patients underwent hydrocelectomy (n = 2449, 98%), while 51 (2%) underwent aspiration. Recurrence was markedly higher after aspiration than hydrocelectomy (5.9% versus 0.3%, P < .001). Complications were infrequent and comparable between groups.
Conclusion:
Laparoscopic hydrocelectomy with high ligation is a highly effective and safe treatment for pediatric NCH, with an exceptionally low recurrence rate. Aspiration showed inferior and inconsistent outcomes, suggesting that it should be reserved for very select cases. These findings support complete laparoscopic hydrocelectomy as the preferred minimally invasive technique for pediatric NCH.
Keywords
Introduction
Pediatric hydrocele is a common condition characterized by the accumulation of fluid within the tunica vaginalis or along the spermatic cord, typically arising from incomplete obliteration of the processus vaginalis (PV). 1 Hydroceles are broadly classified as communicating or noncommunicating depending on the presence or absence of a patent peritoneal connection. Noncommunicating hydroceles (NCH) are further subdivided into scrotal hydrocele (SH), in which fluid surrounds the testis, and encysted spermatic cord hydrocele (ESCH), in which fluid becomes loculated along the spermatic cord separate from the testis.1,2 Although these subtypes are well recognized, their clinical and anatomical differences remain underexplored, and the implications of these differences for surgical planning are not well established.
Traditionally, pediatric hydrocele repair has been performed through an inguinal or scrotal open approach.2,3 With advances in minimally invasive pediatric surgery, laparoscopy has become widely used for inguinal hernia, undescended testis, and hydrocele,4–7 offering advantages such as superior visualization of the internal ring, reduced tissue disruption, and the ability to diagnose and manage contralateral PV patency simultaneously.4,8,9 The efficacy of laparoscopy for communicating hydrocele is well established.10,11 Despite these advantages, consensus regarding the optimal laparoscopic management of NCH—particularly the extent of distal sac dissection—remains lacking.2,4,12 Reported laparoscopic techniques range from simple aspiration with high ligation to marsupialization or complete hydrocelectomy.4,5,13–15 However, available evidence consists predominantly of small case series, heterogeneous techniques, and limited comparative data, especially for SH and ESCH individually.
Given these limitations, high-quality data comparing NCH subtypes and laparoscopic treatment modalities are needed to guide clinical decision-making. The present study aims to address this gap by analyzing a large single-institution cohort of 2500 children who underwent laparoscopic management for SH or ESCH. We sought to (1) compare the clinical characteristics and operative outcomes of SH and ESCH and (2) evaluate the effectiveness of laparoscopic hydrocelectomy versus aspiration, both performed with high ligation. Through this analysis, we aimed to provide evidence supporting a standardized and reproducible laparoscopic approach for pediatric NCH.
Materials and Methods
This retrospective cohort study was conducted at Damsoyu Hospital, Seoul, Republic of Korea. Medical records of pediatric patients who underwent laparoscopic surgery for hydrocele between January 2016 and December 2024 were reviewed. The study protocol was approved by the institutional review board of Damsoyu Hospital (DSY-2025-005), and all procedures were performed in accordance with the Declaration of Helsinki. The study adhered to STROBE guidelines for observational research.
A total of 2995 children under the age of 10 years were evaluated during the study period (Fig. 1). Patients with communicating hydrocele, defined as a persistent patency of the PV communicating with the peritoneal cavity, were excluded (n = 495). After exclusions, 2500 patients with NCH formed the final study cohort. NCH was subclassified into SH or ESCH based on combined ultrasonographic and intraoperative findings (Fig. 2). Intraoperatively, a patent PV was identified in almost all cases. The hydrocele was a distal fluid collection anatomically separated from the proximal PV (hernia sac), without functional communication with the peritoneal cavity. In some patients, the PV appeared proximally obliterated; however, it was carefully opened during dissection to allow the complete removal of the hydrocele sac and was subsequently ligated. SH was diagnosed when an anechoic fluid collection surrounded the testis within the tunica vaginalis. ESCH was defined as a well-circumscribed, fusiform, or oval fluid collection located along the spermatic cord, completely separated from the testis and tunica vaginalis. Abdominoscrotal hydrocele was recorded separately but included in the respective classification based on its distal component.
Patients were excluded if they had (1) prior inguinal or scrotal surgery, (2) incomplete medical records, (3) associated urogenital anomalies requiring alternative surgical approaches (e.g., hypospadias, intersex disorders, complex undescended testis), or (4) concurrent conditions warranting different operative priorities.
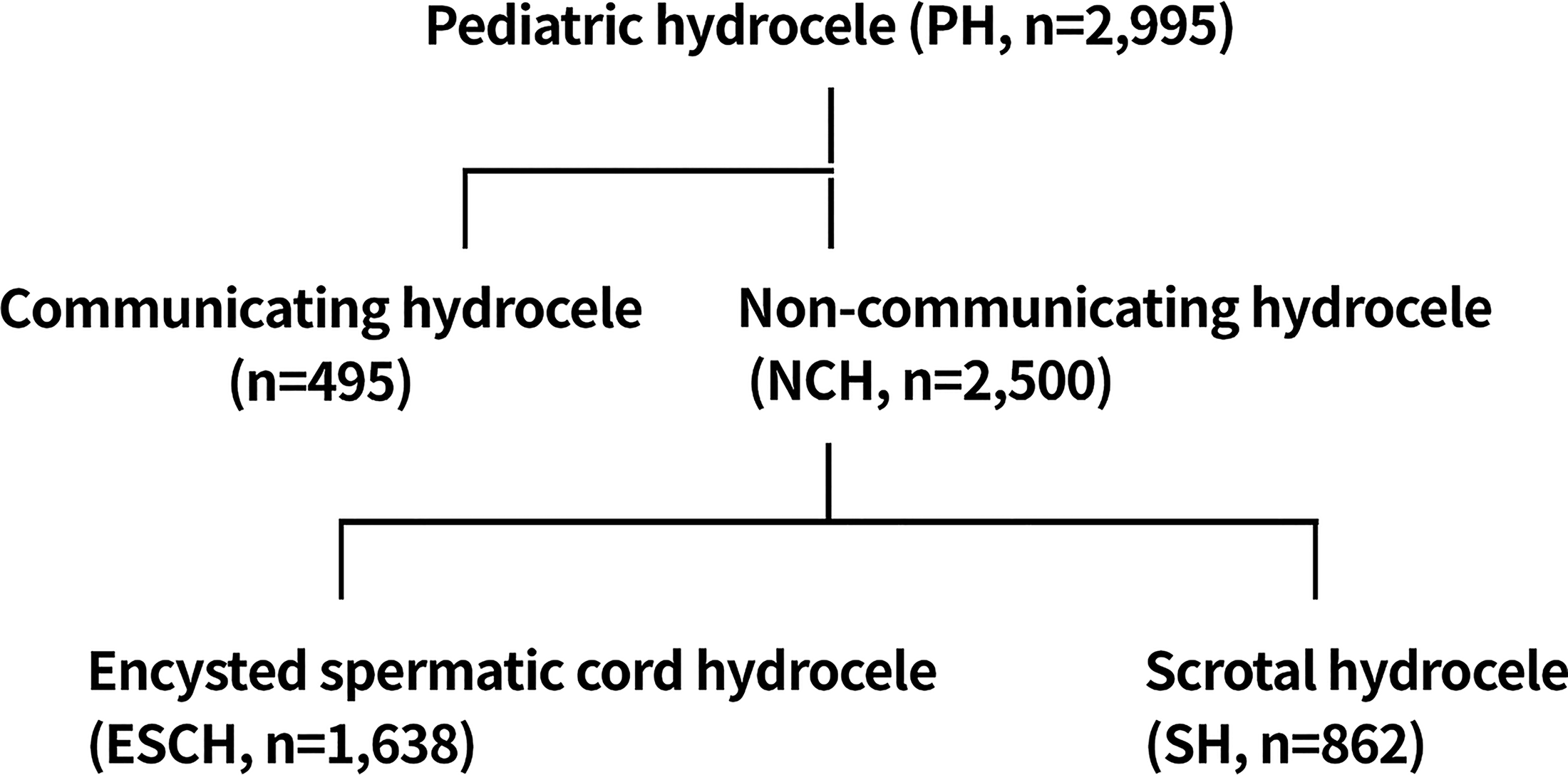
Flowchart demonstrating patient selection and classification of pediatric hydrocele. Cases are categorized as communicating hydrocele, noncommunicating hydrocele (NCH), encysted spermatic cord hydrocele (ESCH), and scrotal hydrocele (SH).
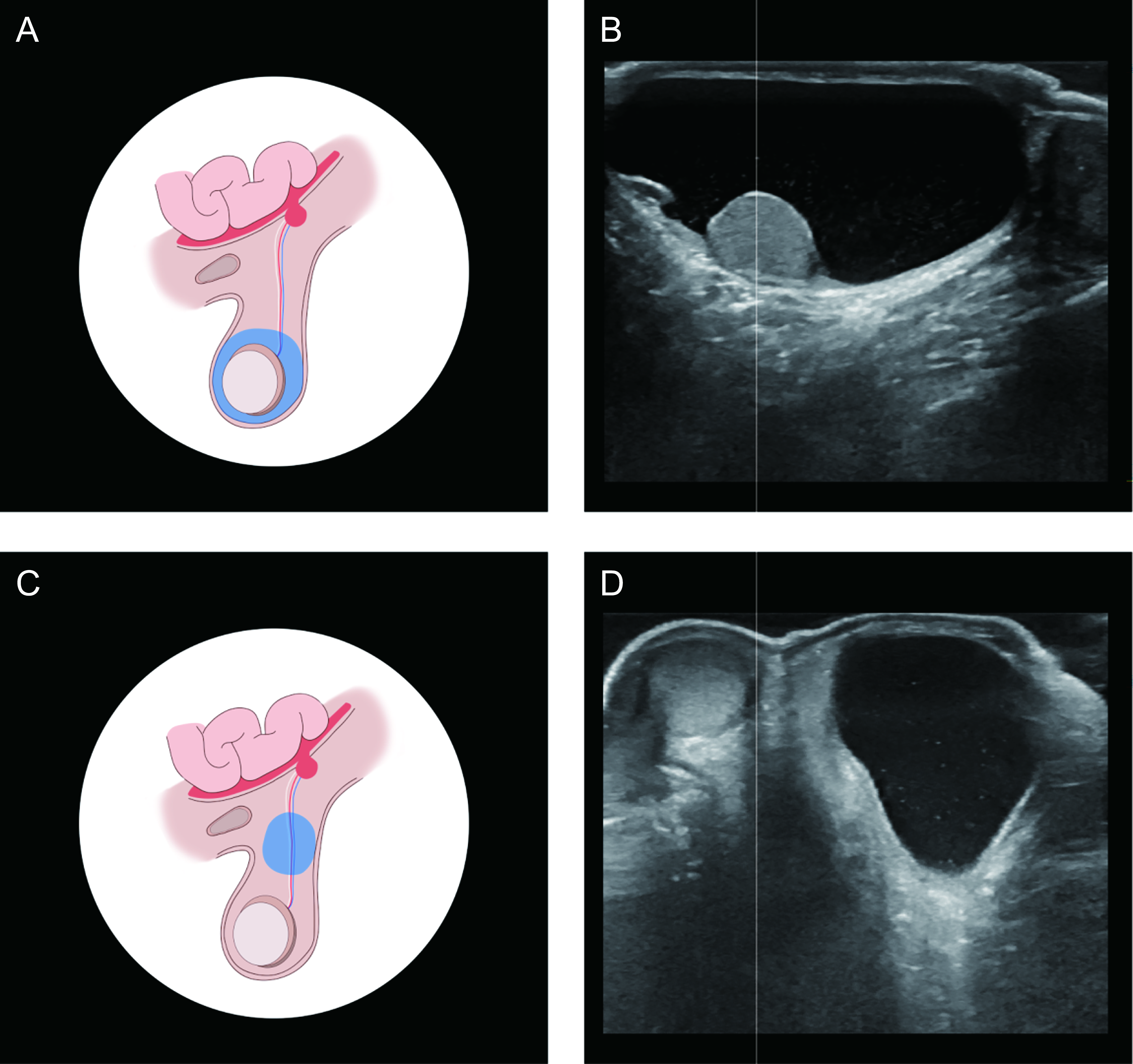
Types of inguinal and scrotal hydroceles with corresponding ultrasonographic findings.
Surgical procedure
All operations were performed under general anesthesia by one experienced laparoscopic surgeon (S.R.L.) using a standardized laparoscopic approach. Pneumoperitoneum was established through a 3-mm transumbilical trocar, and intraabdominal pressure was maintained at 6–8 mmHg. Two additional 2.7-mm instruments were inserted through lateral stab incisions under direct vision. High ligation of the patent PV was performed intracorporeally under direct laparoscopic visualization, with removal of both the hernia sac and the distal hydrocele sac. Distal hydrocele management consisted of either complete laparoscopic hydrocelectomy or fine-needle aspiration. Hydrocelectomy involved circumferential dissection and removal of the parietal tunica vaginalis (for SH, Fig. 3) or complete excision of the loculated cystic lesion (for ESCH, Fig. 4). Aspiration was selected only when distal excision posed increased risk to adjacent structures or when operative priority required minimal dissection (Fig. 5). Specifically, this included cases in which the hydrocele sac was located deep in the scrotum or distal spermatic cord, where dissection risked injury to the vas deferens or testicular vessels, as well as cases with small lesions in which extensive dissection was considered unnecessary. All patients were followed for at least 12 months, and recurrence was defined as reaccumulation of fluid requiring intervention.
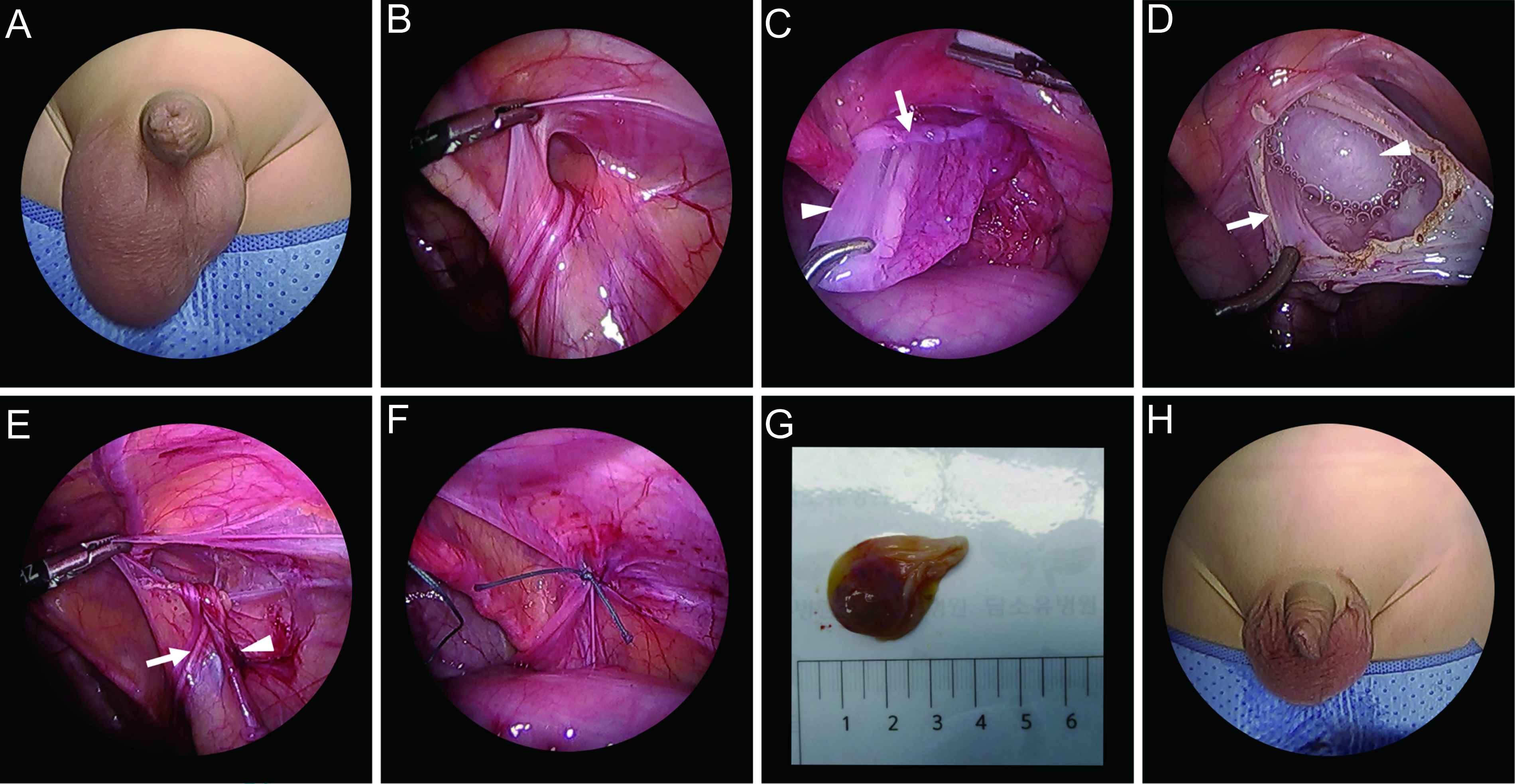
Laparoscopic procedure for scrotal hydrocele (SH).
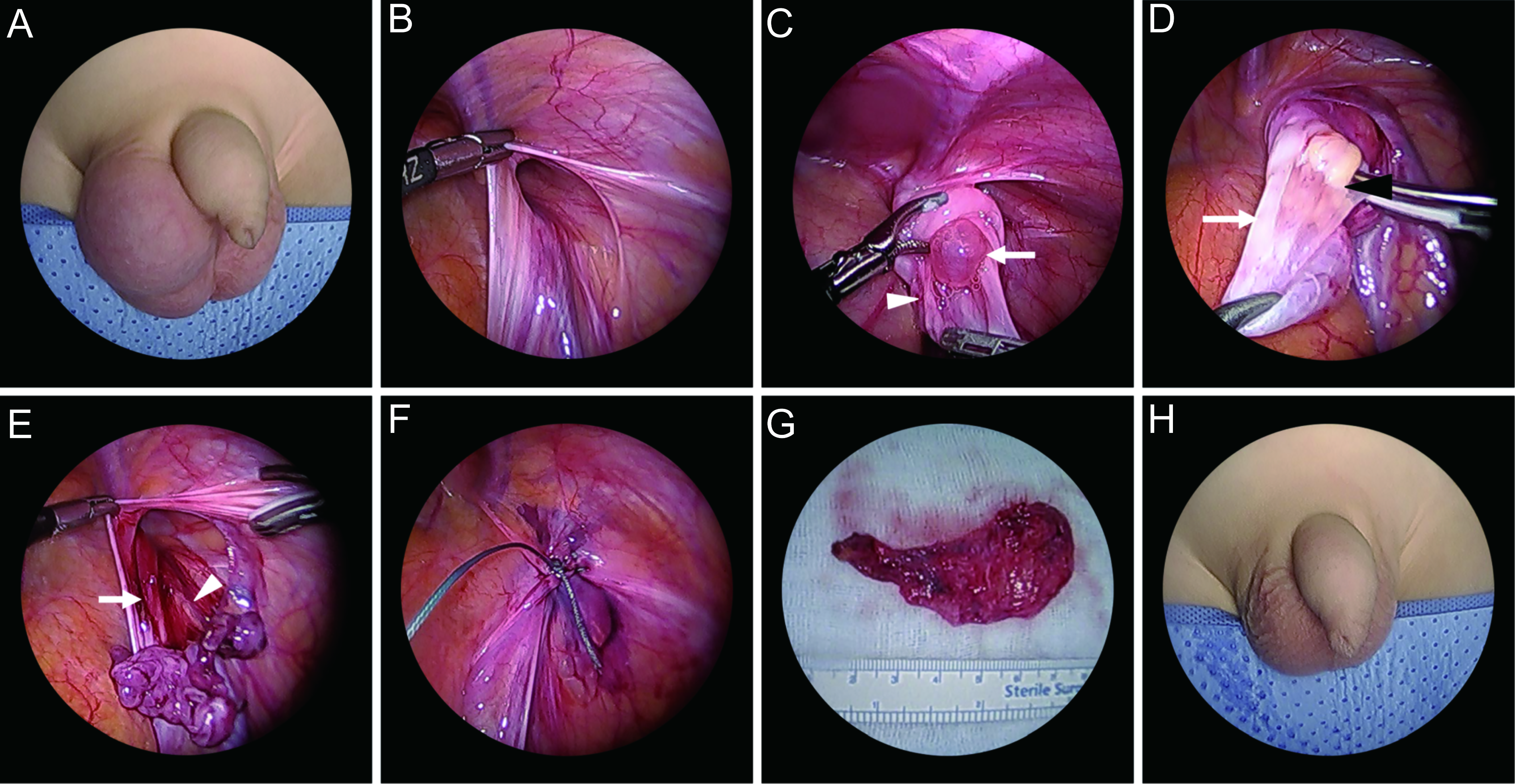
Laparoscopic procedure for encysted spermatic cord hydrocele (ESCH).
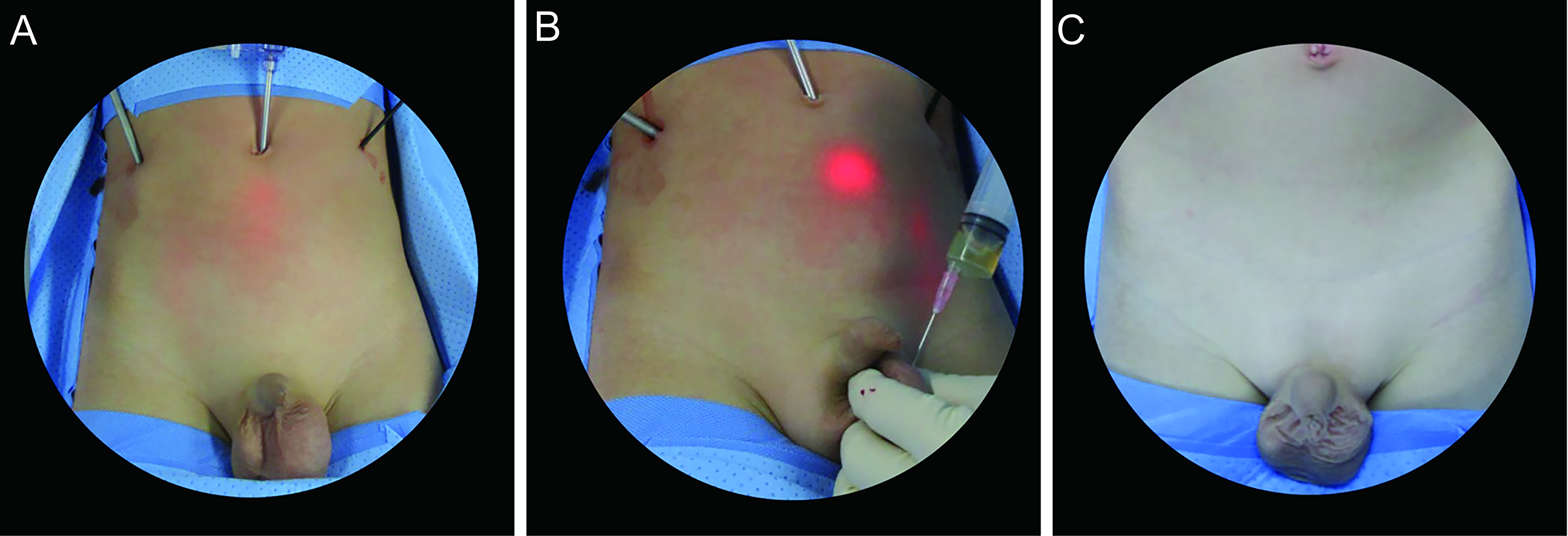
Technical considerations during laparoscopic hydrocelectomy.
Clinical variables and outcomes
Demographic and clinical data included age, body weight, hydrocele subtype, laterality, presence of associated inguinal pathologies (e.g., inguinal hernia, undescended testis), and intraoperative findings. Operative time, hospital stay, intraoperative and postoperative complications (hematoma, seroma, infection, port-site hernia, vas or vessel injury), and recurrence were recorded. When recurrence was suspected, simple aspiration treatment was performed for up to 6 months, and reoperation was performed thereafter. Recurrence was defined as reaccumulation of hydrocele fluid after an initial symptom-free period and requiring clinical intervention. Early postoperative fluid collections consistent with transient seroma were managed with simple aspiration and were not considered a recurrence. This definition was used to distinguish between true recurrence and subjective or transient postoperative reenlargement. All patients were routinely followed at 1 month, 1 year, and annually thereafter, with a minimum follow-up of 12 months. The overall follow-up range was 12–119 months, consistent with Table 1.
Comparison of the Clinical Factors Between SH and ESCH
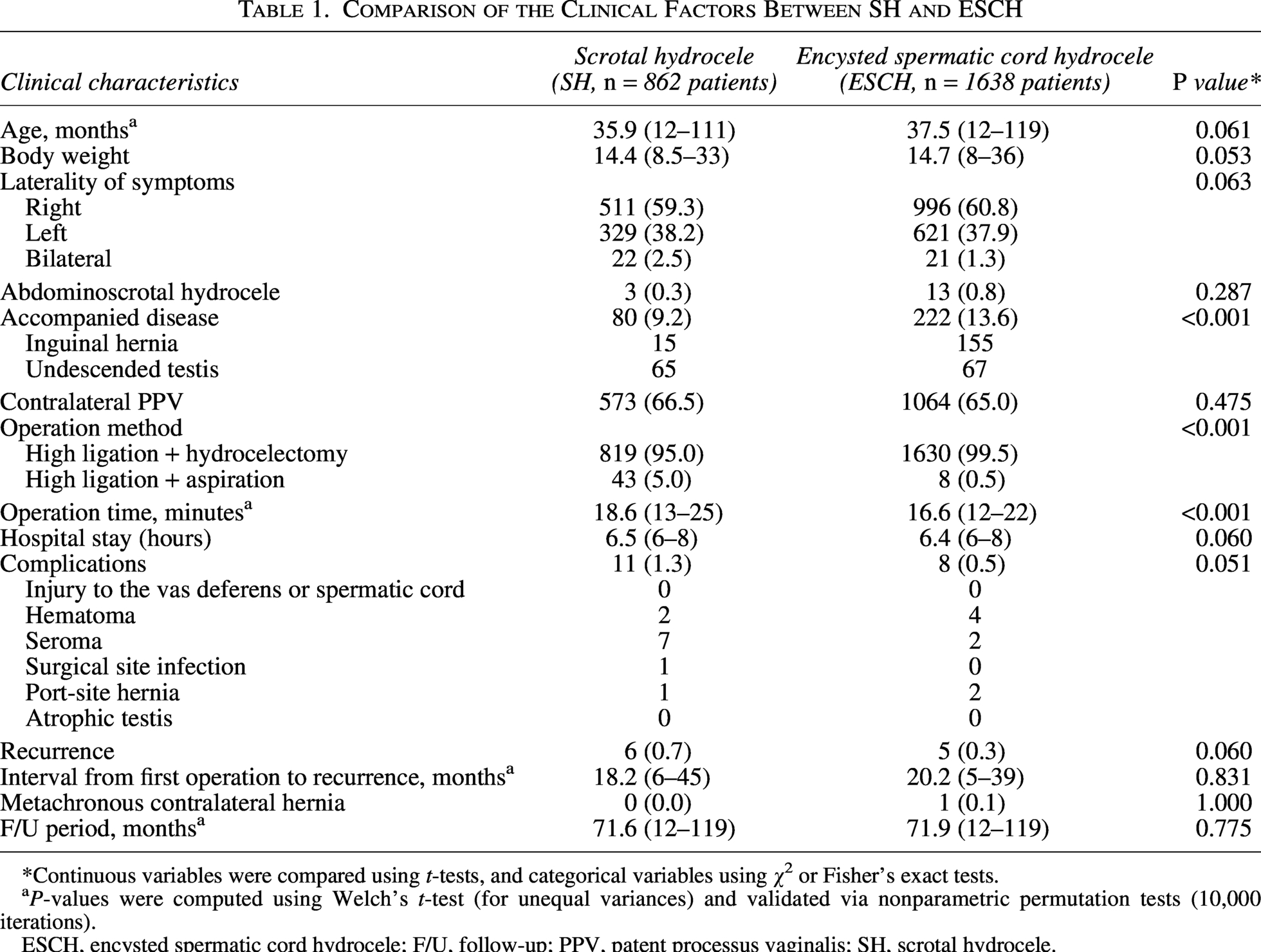
*Continuous variables were compared using t-tests, and categorical variables using χ² or Fisher’s exact tests.
P-values were computed using Welch’s t-test (for unequal variances) and validated via nonparametric permutation tests (10,000 iterations).
ESCH, encysted spermatic cord hydrocele; F/U, follow-up; PPV, patent processus vaginalis; SH, scrotal hydrocele.
Comparison of the Clinical Factors Between Laparoscopic Hydrocelectomy and Aspiration
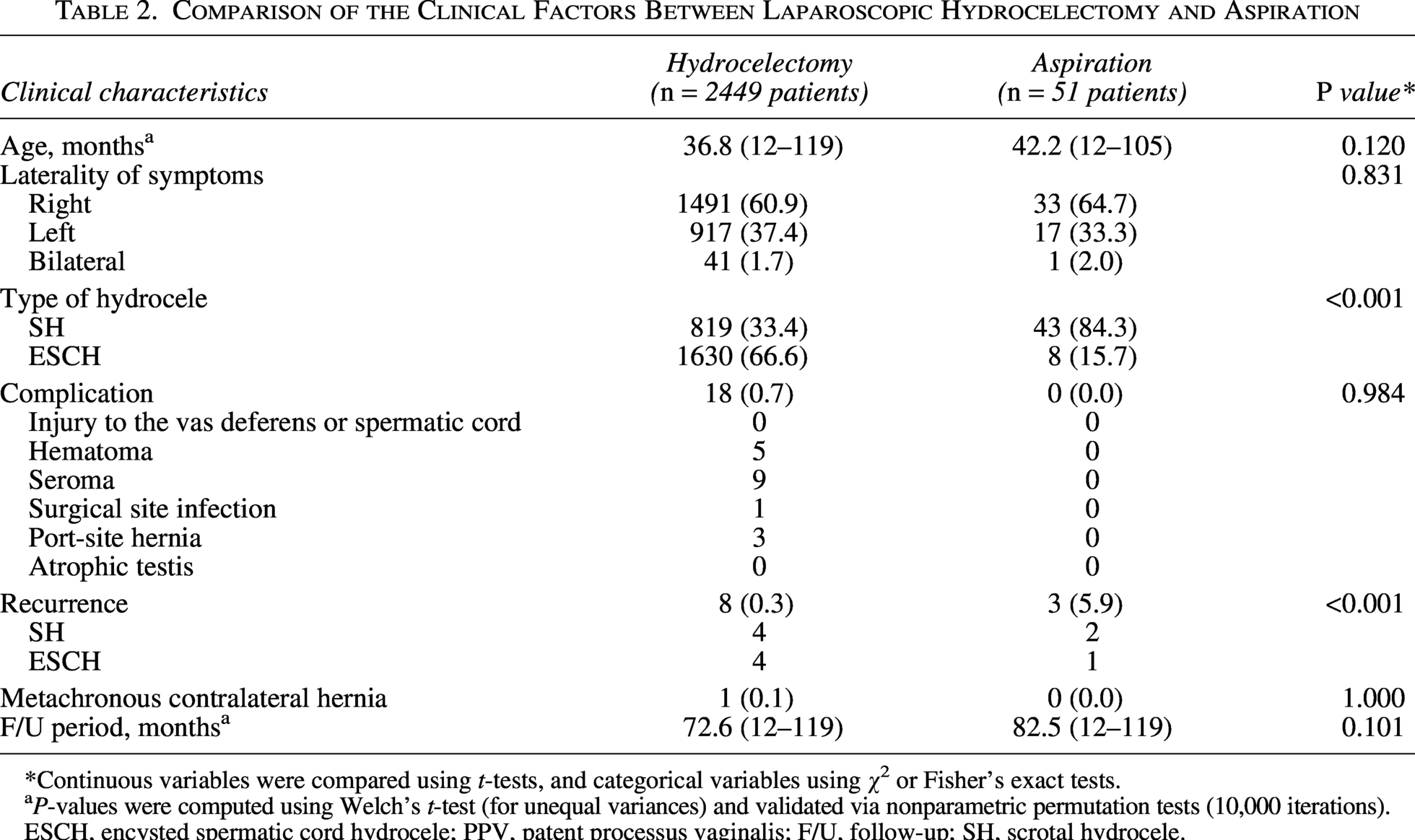
*Continuous variables were compared using t-tests, and categorical variables using χ² or Fisher’s exact tests.
P-values were computed using Welch’s t-test (for unequal variances) and validated via nonparametric permutation tests (10,000 iterations).
ESCH, encysted spermatic cord hydrocele; PPV, patent processus vaginalis; F/U, follow-up; SH, scrotal hydrocele.
Statistical methods
Statistical analyses were performed using R software (version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were presented as mean ± standard deviation and compared using Welch’s t-test. Effect sizes for continuous variables were reported as mean differences with 95% confidence intervals. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate.
Results
Comparison of clinical characteristics between SH and ESCH (Table 1)
A total of 2500 children with NCH were included, consisting of 862 patients with SH and 1638 with ESCH. Age, body weight, and laterality did not differ significantly between groups.
The prevalence of accompanied disease was significantly higher in the ESCH group (13.6%) compared with the SH group (9.2%, P < .001), with inguinal hernia being more frequently identified in ESCH (155 cases versus 15 cases). There was no significant difference in the incidence of contralateral patent processus vaginalis.
Operation time differed significantly between groups, with SH requiring a longer median operative duration (18.6 minutes) than ESCH (16.6 minutes, P < .001). Hospital stay, overall complication rate, and recurrence rate showed no statistically significant difference.
The mean interval from primary surgery to recurrence was 18.2 months for SH and 20.2 months for ESCH. All recurrent cases were successfully corrected surgically, with no postoperative complications or subsequent recurrences noted during follow-up.
Comparison of outcomes according to surgical method (Table 2)
Among all patients, 2449 underwent laparoscopic hydrocelectomy, whereas 51 patients (2.0%) were treated with aspiration following high ligation. Aspiration was performed significantly more often in SH (81.0%) than in ESCH (19.0%, P < .001).
Postoperative complications were rare, occurring in only 0.7% of the total cohort (19/2500). There was no statistically significant difference in complication rates between the hydrocelectomy and aspiration groups (0.7% versus 0.0%, P = .984). Notably, no cases of vas deferens injury, testicular vessel damage, or testicular atrophy occurred in either group. Notably, the recurrence rate was markedly higher in the aspiration group (5.9%, 3/51) compared with the hydrocelectomy group (0.3%, 8/2449, P < .001).
Characteristics of recurrent cases (Table 3)
A total of 11 patients (0.44%) experienced recurrence. Table 3 summarizes their clinical characteristics. Initial diagnoses included SH in 6 patients and ESCH in 5 patients. In all patients with recurrence, the PV that was high-ligated at the time of the first surgery was confirmed to be occluded.
Clinical Characteristics of Recurrence
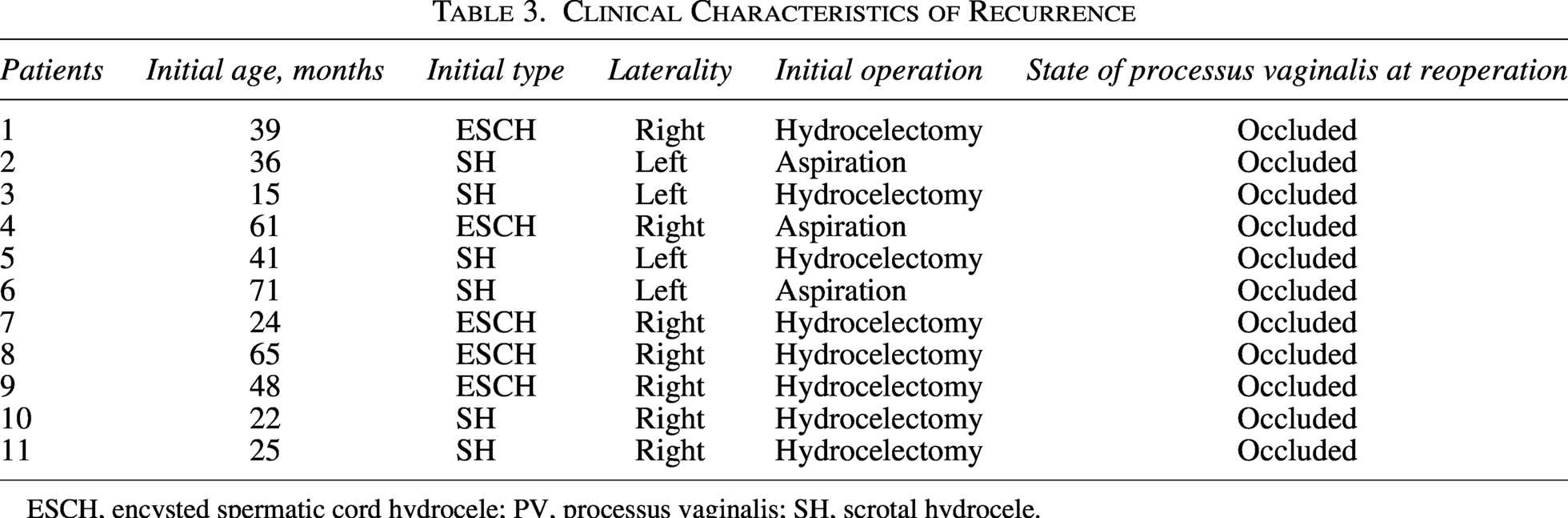
ESCH, encysted spermatic cord hydrocele; PV, processus vaginalis; SH, scrotal hydrocele.
Discussion
This study represents one of the largest single-institution series evaluating laparoscopic management of pediatric NCH, including a detailed comparison of SH and ESCH, as well as a direct evaluation of hydrocelectomy versus aspiration for management of the distal hydrocele sac. Our findings provide important insights into the clinical characteristics of NCH subtypes and support the effectiveness of laparoscopic hydrocelectomy with high ligation as a reliable minimally invasive approach.
The first key finding of this study is that SH and ESCH differ significantly in their association with other inguinal pathologies. ESCH demonstrated a significantly higher rate of accompanied diseases, particularly inguinal hernia, compared with SH. This supports the embryologic concept that ESCH often arises from partial persistence of the PV rather than a fully isolated lesion, which may explain the higher observed prevalence of occult or concurrent hernias.16,17 This partial persistence may result in incomplete proximal obliteration, thereby increasing the likelihood of the occurrence of an associated inguinal hernia. These findings underscore the need for careful laparoscopic evaluation of the internal ring in ESCH, even when preoperative ultrasound does not indicate a communicating component.
Operative complexity also differed between subtypes. The longer operative time observed in SH is likely attributable to the broader extent of tunica vaginalis involvement surrounding the testis, requiring a more extensive distal dissection. In contrast, ESCH was typically more localized along the spermatic cord, allowing for faster excision. Although not statistically significant (P = .051), the complication rate was marginally higher in the SH group (1.3%) compared with the ESCH group (0.5%). This trend is likely due to the more extensive dissection required to detach the tunica vaginalis from the testis in SH cases, which creates a larger raw surface area prone to minor seroma formation. Importantly, despite these anatomical and technical differences, both groups demonstrated similarly low complication rates and excellent postoperative outcomes, supporting the safety and consistency of the laparoscopic approach across NCH subtypes.
The most clinically significant finding concerns the marked difference in outcomes between hydrocelectomy and aspiration. Although aspiration was performed selectively in only 2% of patients, its recurrence rate (5.9%) was substantially higher than that of hydrocelectomy (0.3%). This disparity is unsurprising, as aspiration does not remove the epithelial lining of the distal sac, allowing the potential for continued fluid secretion and reaccumulation. Therefore, recurrence patterns in the aspiration group may differ mechanistically from those in the hydrocelectomy group. Prior studies in adults have reported similar limitations of aspiration-based techniques,18,19 but pediatric evidence has been sparse. Our large cohort provides robust confirmation that aspiration is generally insufficient as a primary treatment for pediatric NCH.
Nonetheless, aspiration may still have a role in highly selected situations—particularly when the hydrocele is located too distally for safe laparoscopic access or when dissection poses a substantial risk of injury to the vas deferens or spermatic cord vessels. It is important to acknowledge that the aspiration group was subject to selection bias, as this technique was reserved for cases where distal dissection posed a high risk of injury to the vas deferens or spermatic vessels. However, the recurrence in this group was driven by the persistence of the secretory tunica vaginalis, rather than the anatomical complexity itself. This suggests that simple aspiration is mechanistically inadequate for long-term cure. Therefore, in difficult cases where laparoscopic excision is not feasible, converting to a scrotal incision to ensure complete sac removal is a more reliable strategy than relying on aspiration. These exceptional circumstances should be carefully individualized, and complete distal sac removal should remain the standard whenever feasible.
The overall recurrence rate in this series was exceptionally low, which aligns with contemporary reports supporting laparoscopic repair for pediatric hydrocele.10,11,20 The ability to visualize the internal ring clearly, manage contralateral PV patency during the same operation, and remove the hydrocele sac under magnified view provides substantial advantages over open techniques. Additionally, avoiding scrotal incisions minimizes postoperative discomfort and cosmetic concerns, particularly in older children.
Despite the strengths of a large cohort and standardized surgical protocol, this study has limitations. Its retrospective nature introduces potential selection bias, especially regarding the small proportion of patients treated with aspiration. In addition, the aspiration group consisted predominantly of SHs, which are typically located more distally from the internal inguinal ring, indicating that aspiration was preferentially applied to anatomically distal cases. This shows that the two groups were inherently different in their baseline surgical characteristics; therefore, a direct comparison between hydrocelectomy and aspiration may not be possible. Although intraoperative criteria guided the decision to avoid distal dissection, surgeon judgment may still have influenced case selection. In addition, the relatively small number of recurrence cases precluded statistically meaningful subgroup analyses, including evaluation of potential age-related effects. Furthermore, all operations were performed by a single experienced laparoscopic surgeon, which improves technical consistency but may limit generalizability to centers with varying levels of expertise. Future prospective studies incorporating standardized indications for aspiration and multicenter validation would further strengthen these findings.
Conclusion
In this large cohort of children with NCH, laparoscopic hydrocelectomy combined with high ligation demonstrated excellent safety and the lowest recurrence rate across SH and ESCH. Aspiration, despite its technical simplicity, was associated with a substantially higher risk of recurrence and should therefore be considered only in highly selective circumstances where sac excision is not feasible or carries meaningful operative risk. Overall, these findings support laparoscopic hydrocelectomy as a reliable and effective operative strategy for pediatric NCH and reinforce the value of complete distal sac removal during minimally invasive repair.
Footnotes
Acknowledgments
The authors thank Hyejin Park for conducting the primary English grammar correction of this article and Beom Seok Oh from the Research Center of Damsoyu Hospital and Young Hyun Lee from the Ewha Womans University Graduate School of Engineering for their assistance with statistical analysis and data organization.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Authors’ Contributions
S.R.L. and Y.C. jointly conceived and supervised the study. They contributed to the interpretation of the data, critical revision of the manuscript, and provided overall guidance throughout the research process. Both authors served as co-corresponding authors and approved the final version of the manuscript.
Author Disclosure Statement
S.R.L. and Y.C. have no conflicts of interest or financial ties to disclose.
Funding Information
The authors have no financial ties to disclose.