
Abstract
Background:
Anastomotic complications remain the principal source of morbidity in metabolic and bariatric surgery. Bleeding, leakage, and stricture are most often related to the anastomosis itself and to the permanent hardware left behind by staplers and sutures. Magnetic compression anastomosis has been proposed as an incisionless, sutureless alternative that avoids retained foreign material.
Objective:
To describe the surgical technique for the creation of a side-to-side duodeno-ileal anastomosis using the Magnet Anastomosis System (MagDI) and to summarize early clinical outcomes.
Technique:
Two linear neodymium magnets are positioned on opposite intestinal walls—one in the proximal duodenum and one in the ileum, 250 cm from the ileocecal valve. The magnets self-align and apply sustained compression to the interposed tissue. Over the following weeks the entrapped tissue undergoes controlled necrosis, a patent anastomosis is formed, and the magnets detach and are eliminated through the gastrointestinal tract, leaving no retained material.
Results:
In early clinical experience, magnet placement and anastomotic patency were achieved in all cases, with no device-related leaks, obstructions, or deaths. When combined with sleeve gastrectomy, the procedure produced substantial weight loss and improvement of type 2 diabetes.
Conclusion:
Magnetic side-to-side duodeno-ileostomy is a feasible and reproducible technique that may reduce anastomotic morbidity in bariatric and metabolic surgery. Longer-term, larger studies are warranted to confirm durability.
Keywords
Introduction
For nearly two centuries, surgeons have searched for safer methods to reconnect the divided segments of the gastrointestinal tract. From the seromuscular sutures introduced by Lembert in the early nineteenth century to the absorbable metallic buttons devised by Murphy at its close, each successive technique aimed to restore continuity while minimizing harm. Progress, however, was rarely free of cost: bleeding, leakage, retained foreign material, and chronic complications such as inflammation and stricture continued to affect patients well after operation. Metabolic and bariatric surgery (MBS) is currently the most effective treatment for severe obesity and type 2 diabetes (T2D). Procedures such as Roux-en-Y gastric bypass and sleeve gastrectomy achieve durable weight loss and metabolic improvement, yet their most vulnerable point remains the anastomosis. Bleeding, infection, and leakage can convert a therapeutic operation into a life-threatening emergency. Even with contemporary stapling devices, permanently retained hardware may contribute to chronic inflammation, stricture formation, and non-uniform collagen deposition at the anastomotic line. 1 Magnetic compression anastomosis was conceived as a way to eliminate these drawbacks. Rather than approximating tissue with staples or sutures, two linear neodymium magnets are placed on opposite intestinal walls. The magnets draw together across the bowel, applying continuous, controlled compression until a channel forms between the two lumens. Within several weeks the magnets detach and are eliminated through the gastrointestinal tract, leaving a clean, durable anastomosis composed only of healed tissue, with no retained foreign body.2,3 After early validation in animal models, the concept advanced to clinical use only in recent years. 2 This technical note describes the operative technique for the creation of a side-to-side duodeno-ileal anastomosis with the Magnet Anastomosis System (MagDI) and summarizes the early clinical outcomes reported to date.
Surgical Technique
Objective
The aim of the procedure is to create a side-to-side duodeno-ileal anastomosis between the first portion of the duodenum and the ileum, 250 cm proximal to the ileocecal valve (Fig. 1).
Objective of the procedure: creation of a side-to-side duodeno-ileal anastomosis.
Device
The MagDI consists of a pair of linear neodymium-iron-boron (Nd2Fe14B) magnets enclosed in a titanium housing. In its first-generation design, each magnet carries a stainless steel/nitinol/polyester suture loop at one end to facilitate intraluminal placement or retrieval of the secondary magnet (Fig. 2).

Magnet anastomosis system components.
The Magnet Anastomosis Delivery System (MADS) is a flexible orogastric delivery catheter constructed of stainless steel, nitinol, and polymer. It is used to engage and advance the magnets within the lumen of the small intestine. The laparoscopic positioning device incorporates a non-magnetic titanium tube and a hinge pin with a magnetically attracted, articulating stainless steel tip, which allows controlled advancement of the magnet through the jejunum and ileum.
Clinical case
This is a 62-year-old female patient who underwent a laparoscopic sleeve gastrectomy 13 years ago as her primary bariatric procedure. She has no history of T2DM and no other significant comorbidities, including no documented hypertension, dyslipidemia, or obstructive sleep apnea. Her past surgical history is otherwise notable for a gynecological procedure: she underwent a hysterectomy in 2024.
Over the years following her initial bariatric surgery, the patient experienced significant weight regain. At the time of the current evaluation, she weighed 90 kilograms, with a body mass index (BMI) of 38, placing her in the category of class II obesity. Weight regain after sleeve gastrectomy is a well-recognized phenomenon and may result from a combination of factors, including gastric pouch or sleeve dilation, hormonal adaptation, and changes in dietary and lifestyle patterns over time.
As part of the preoperative workup, a comprehensive assessment was carried out. Laboratory studies were within normal limits, with no evidence of nutritional deficiencies, metabolic abnormalities, or anemia. Abdominal ultrasound was unremarkable, and spirometry demonstrated normal pulmonary function, supporting the patient’s suitability for further surgical intervention.
An upper gastrointestinal contrast series was performed to evaluate the anatomy of the previous sleeve gastrectomy. The study showed a normal sleeve configuration, with no significant dilation, stricture, hiatal hernia, or gastroesophageal reflux on imaging.
Based on the clinical and the imaging findings, the decision was made to proceed with a side-to-side duodeno-ileal anastomosis with the MagDI as a revisional bariatric surgery to address the patient’s weight regain.
Operative procedure
The patient first swallows the distal magnet (a second-generation magnet of 40 or 50 mm with a biodegradable contour) with water. Approximately 2 hours later, an abdominal radiograph is obtained to confirm its position. (Fig. 3).

Control abdominal radiograph after swallowing the distal magnet to verify device position.
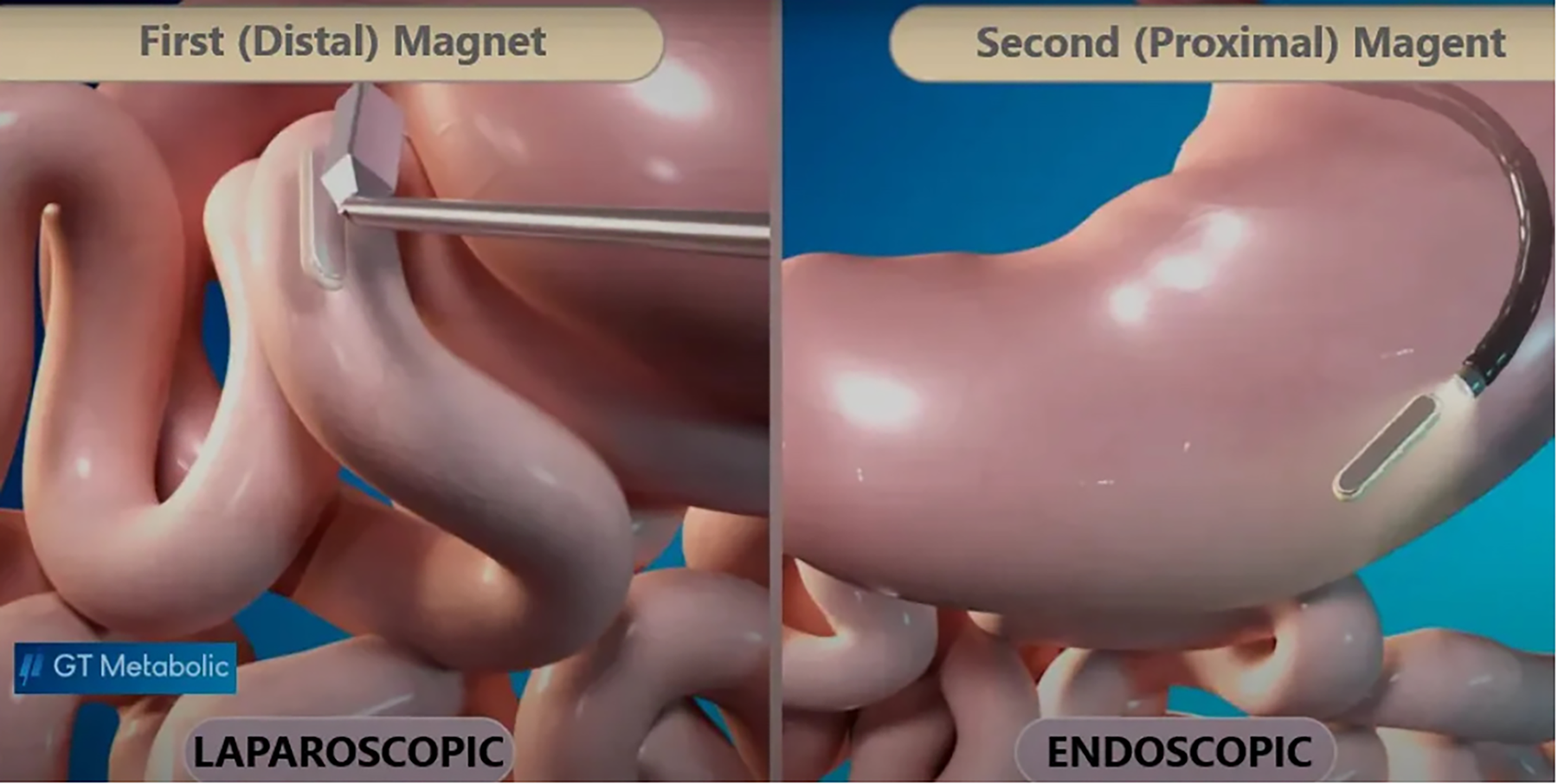
Under general anesthesia, a laparoscopic marker is placed in the ileal mesentery 250 cm from the cecum using titanium clips. With the laparoscopic magnetic positioning device, the distal magnet is located within the bowel and advanced intraluminally to the level of the clip marker. The proximal magnet is then introduced into the first portion of the duodenum by intraoperative endoscopy and released, allowing it to self-align with the distal magnet across the intestinal walls. (Fig. 4). The endoscope and the positioning device are subsequently withdrawn. (Fig. 5). The mesenteric defect is closed on its left side with a 2-0 silk suture. Correct placement of the system is confirmed by abdominal radiography at the end of the procedure. The patient recovered in a standard ward, started on oral feeding, and was discharged at 24 hours.
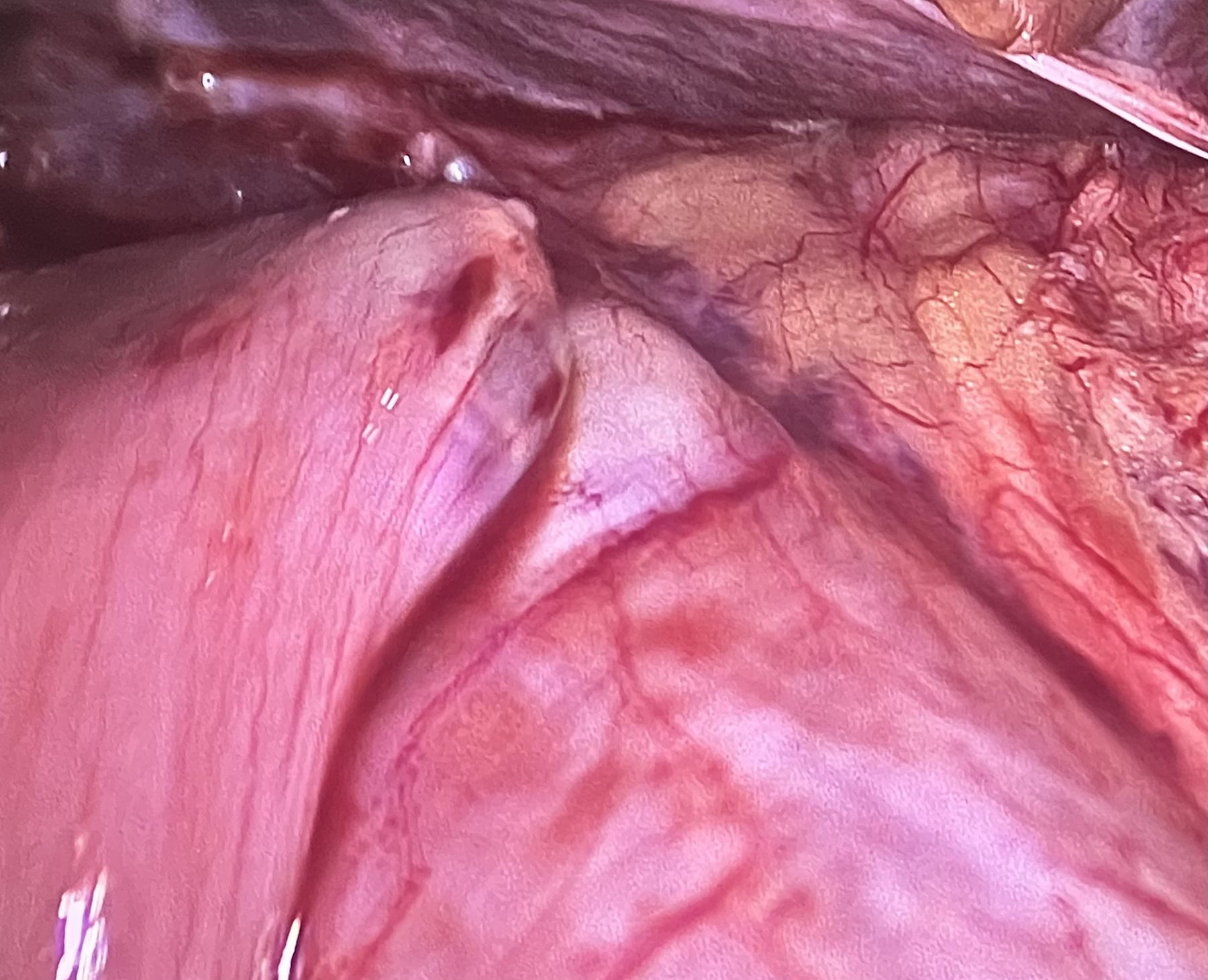
Laparoscopic view of the final position of the magnetic anastomosis.
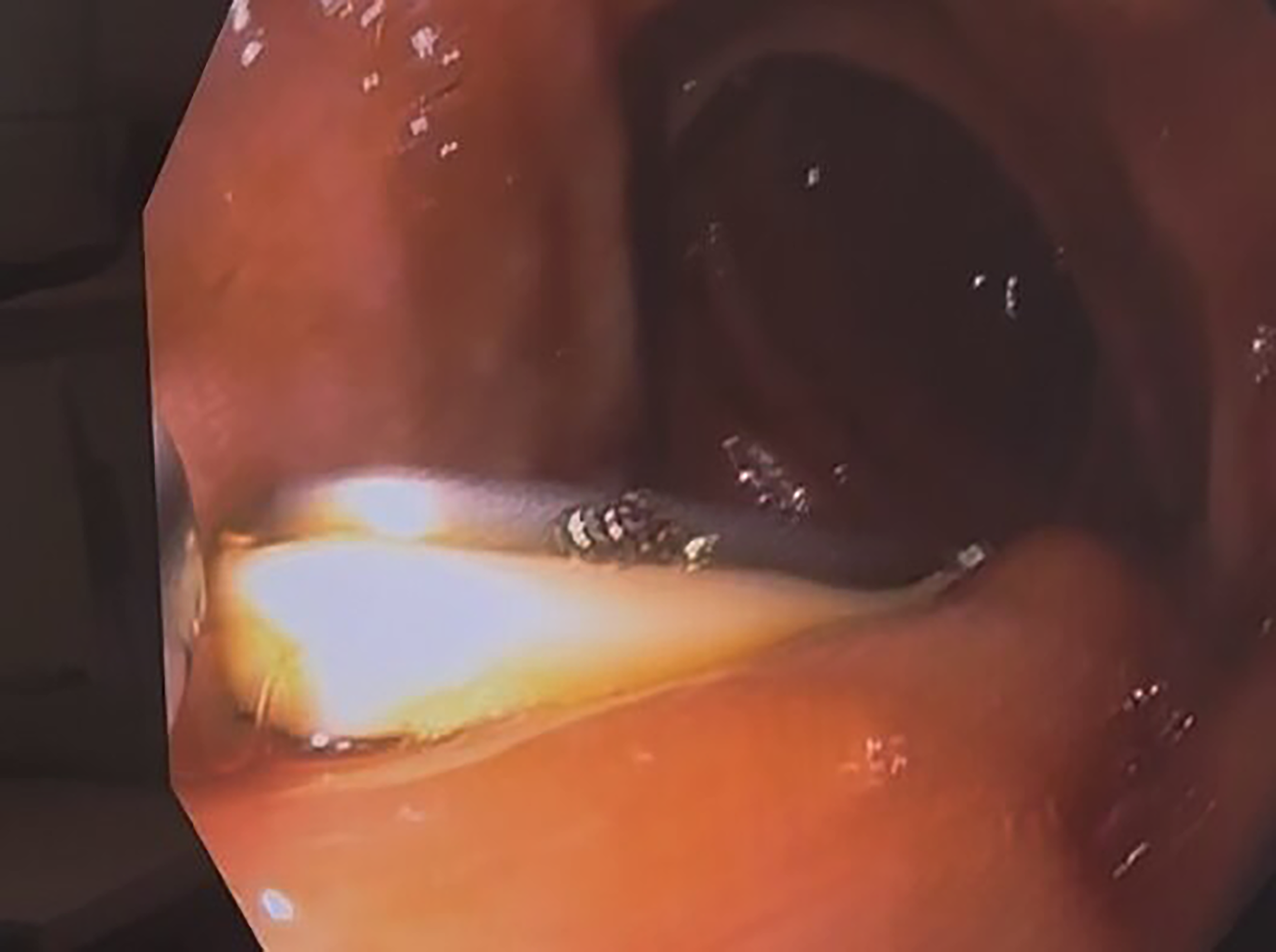
Intraoperative endoscopic introduction of the proximal magnet into the duodenum and alignment with the distal magnet.
Approximately 1 month postoperatively, the magnets are expected to have completed compression, necrosis, and sloughing of the interposed tissue, resulting in a fused, patent anastomosis; this is verified fluoroscopically. The paired magnets then detach from the duodeno-ileal site and are eliminated naturally through the gastrointestinal tract. Thereafter, food passes both through the native duodenal lumen and through the patent anastomotic diversion into the ileum.
Results
Indications and contraindications
Indications
Patients with a BMI of 30.0–50.0 kg/m2 and type 2 diabetes (HbA1c ≤ 6.5%). Patients with weight regain or residual type 2 diabetes more than 12 months after a previous sleeve gastrectomy. Patients with a BMI ≥ 40 kg/m2 who are candidates for laparoscopic single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S).
Contraindications
Previous intestinal, colonic, or duodenal surgery. Previous gastrointestinal trauma. Other digestive implants. Severe uncontrolled systemic illness. Severe intra-abdominal adhesions. Inflammatory bowel disease. Peritonitis. Any narrowing of the digestive tract. Abnormal anatomy that would impede progression of the implant.
Early clinical outcomes
First-in-Human Experience: In late 2021, 5 women in the Republic of Georgia became the first patients worldwide to undergo a side-to-side duodeno-ileostomy created by magnetic compression. All had severe obesity, and most also had type 2 diabetes. The intervention combined two steps: a standard sleeve gastrectomy and the magnetic anastomosis. Under combined endoscopic and laparoscopic guidance, the distal magnet was advanced to the ileum 250 cm from the cecum, while the proximal magnet was released in the duodenum. The two components self-aligned and initiated a gradual, bloodless union. 2
At 1 year, patients had lost an average of 34% of total body weight, corresponding to approximately 40 kg; mean excess weight loss reached 80%, and mean BMI fell by 15 points. Glycemic control improved markedly: mean HbA1c decreased from 6.8% to 4.8%, with normalization of glucose levels. No leaks, infections, or device-related complications were observed. 2
Multicenter experience: Following the first-in-human series, the investigation was extended. Between 2021 and 2023, 43 patients were treated at centers in Georgia, Belgium, Spain, and Canada. Some had undergone a previous sleeve gastrectomy and returned for a revisional procedure (MagDI after sleeve gastrectomy), while others received the magnetic anastomosis concurrently with a primary sleeve gastrectomy (MagDI with sleeve gastrectomy).
The feasibility endpoint was met in 100% of cases: every magnet was successfully placed, every pair was expelled, and every anastomosis was patent. No device-related adverse events—leaks, obstructions, or deaths—were recorded. Outcomes varied with the timing of the procedure. Patients who underwent concurrent sleeve gastrectomy achieved the greatest weight loss, exceeding 34 kg at 6 months with excess weight loss above 66%. Patients treated after a previous sleeve gastrectomy lost weight more modestly, averaging approximately 8 kg at 6 months. In both groups, patients with type 2 diabetes showed clear metabolic improvement, and many discontinued antidiabetic medication entirely.4,5
Safety and learning curve: Adverse events reported in the multicenter experience were largely related to the accompanying surgical manipulation rather than to the magnetic device. Mild serosal tears occurred during laparoscopic handling, and some patients developed gallstones, constipation, or vitamin deficiencies requiring supplementation. None of these complications were attributed to the device itself.
A learning curve was reflected in operative time, which exceeded 2 hours initially and shortened progressively as the surgical teams refined their technique. Although the underlying concept—two magnets drawing bowel loops together—is simple, safe delivery and accurate alignment of the components require careful operative choreography.
Discussion
Magnetic duodeno-ileostomy represents not only a new instrument but a different operative principle. By using sustained magnetic compression, the technique converts the creation of an anastomosis from a mechanical act into a controlled biological process: tissue union is achieved through gradual compression and necrosis rather than through the placement of permanent hardware. The absence of retained foreign material may reduce the risk of chronic inflammation and stricture associated with conventional staple lines.
The early clinical data are encouraging. Across the first-in-human and multicenter experiences, the system demonstrated complete technical feasibility and an absence of device-related complications, while producing clinically meaningful weight loss and metabolic improvement, particularly when combined with sleeve gastrectomy. These results should nonetheless be interpreted with caution, given the small number of patients and the limited duration of follow-up. Larger studies with longer follow-up will be required to confirm anastomotic durability, define the most appropriate indications, and characterize the learning curve more precisely. If these early findings are confirmed, magnetic compression anastomosis may become a standard option in bariatric and metabolic surgery, with potential application to other forms of gastrointestinal reconstruction.
Conclusion
Magnetic side-to-side duodeno-ileostomy with the MagDI system is a feasible, reproducible, and well-tolerated technique. In early clinical experience it has been performed without device-related leaks, obstructions, or deaths while achieving substantial weight loss and improvement of type 2 diabetes when combined with sleeve gastrectomy. By replacing staples and sutures with controlled magnetic compression, the technique offers a sutureless, incisionless approach to gastrointestinal anastomosis. Confirmation of these results in larger series with longer follow-up will determine its definitive role in MBS.