
Abstract
Introduction:
Objective data quantifying the trend of the robotic-assisted learning process remains limited. The aim of this study is to evaluate the efficiency and progression of surgical skill acquisition during robotic-assisted pyeloplasty by comparing performance parameters between expert and non-expert surgeons using a dual-console system over a 3-year period.
Methods:
A total of 25 robotic-assisted pyeloplasties were retrospectively analyzed; all were performed by a Da Vinci Xi robotic platform equipped with dual operative consoles, operated simultaneously by a robotic expert (C1) and a non-expert surgeon (C2). The procedures were divided into five standardized phases. Surgical performance was assessed using Tracker® motion analysis software, which measured operative times, console utilization, instrument collisions, and motion efficiency. Trends across years were assessed using one-way analysis of variance (P < .05).
Results:
A total of 25 cases were analyzed. The total operative time decreased significantly from 210 minutes in year 1 to 185 minutes in year 3 (P = .008). The expert surgeon’s console time ratio decreased from 90.0% in year 1 to 14.5% in year 3 (P < .001), with a corresponding increase in non-expert surgeon’s console time. A significant reduction in the number of instrument collisions (from 1457 in year 1 to 97 in year 3, P < .001) and a marked increase in motion efficiency (from 14% to 88%, P < .001) were observed for the non-expert surgeon. Phase-specific analysis revealed a steady improvement in the non-expert surgeon’s performance across all phases.
Conclusions:
Robotic-assisted pyeloplasty significantly accelerates skill acquisition for non-expert surgeons, as evidenced by improvements in operative time, instrument collisions, and motion efficiency. The dual-console approach provides a valuable educational framework, facilitating real-time supervision and progressive task delegation. These findings support integrating dual-console systems and objective motion analysis into structured robotic training programs to enhance surgical proficiency and safety in pediatric surgery.
Introduction
Since its introduction to pediatric surgery in 2001, robotic-assisted surgery (RAS) has grown over the years, with an ever-expanding range of procedures now possible, including operations on younger children, infants, and neonates. 1
Compared to traditional laparoscopic surgery, the robotic platform offers some advantages: magnified high-definition visualization, wristed instruments providing 7 degrees of freedom, 90° of articulation and 540° of rotation, motion scaling, tremor filtering, and improved ergonomics, resulting in reduced operative fatigue. 2
These features improve dexterity and visualization in confined spaces. 3
In pediatric urology, for instance, robotic surgery has swiftly become the gold standard, 4 with complex procedures such as pyeloplasty becoming increasingly prevalent, particularly among children weighing over 15 kg.5,6 To date, pyeloplasty remains one of the most common indications for robotic surgery in the pediatric population. 7
One of the most relevant advantages of RAS is its relatively short learning curve compared with other surgical procedures8–10. However, most of the published studies addressing the learning curve are retrospective and include small numbers of surgeons with heterogeneous experience. These studies also assess a variety of outcome measures. 11
In this context, recent studies have emphasized the need to define objective measures of surgical expertise and patient-related factors and to develop standardized robotic training programs based on well-characterized learning curves. 12
This study aimed to objectively assess the learning curve in dual-console robotic-assisted pyeloplasty by quantitatively analyzing surgical performance parameters, such as motion efficiency, instrument collisions, and console utilization, using motion-tracking software over a 3-year period.
Methods
Study design and data collection
This was a retrospective observational study conducted at a single high-volume pediatric robotic surgery center over a 3-year period. A total of 25 recorded videos of robotic-assisted pyeloplasty procedures performed over 3 years were included. All surgeries were carried out using the Da Vinci Xi robotic platform equipped with dual operative consoles.
Each operation was performed simultaneously by the same expert robotic surgeon (console 1) and the same non-expert surgeon (console 2). We considered as “expert robotic surgeon” a consultant with robotic surgery certification (master's degree or Da Vinci certificate) with at least 5 years of practice. Only standard dismembered pyeloplasty procedures according to the Anderson-Hynes technique were included. Cases involving anomalous crossing vessels were excluded.
Procedures were segmented into five standardized phases, and performance was compared between an expert and a non-expert surgeon using a dual-console platform.
Surgical performance metrics were assessed using Tracker®, a validated motion analysis software developed specifically for robotic surgery assessment.
For each phase of all procedures, the following quantitative parameters were extracted: mean total operative time (T) and total phase-specific durations, mean console time (C1 and C2), and the ratio of expert console utilization (C1/T).
The software automatically identified and calculated the total number of instrument collisions per console and the efficiency of instrument motion, expressed as the percentage of effective movement within the total instrument path.
All data were independently verified by 2 investigators to ensure measurement consistency.
Statistical analysis
All data were analyzed using IBM SPSS Statistics (IBM Corp. Armonk, NY, USA). Continuous variables, including total operative time, phase-specific durations (A–E), console utilization times, number of instrument collisions, and instrument motion efficiency, were summarized as mean ± standard deviation when normally distributed, or as median and interquartile range when nonnormally distributed.
Data normality was assessed using the Shapiro–Wilk test for each continuous variable.
Comparisons across the three observation periods (year 1, year 2, and year 3) were performed using one-way analysis of variance for normally distributed variables or the Kruskal–Wallis test for non-parametric data.
Comparisons between the expert and non-expert surgeons (console 1 vs. console 2) within each year and for each procedural phase were performed using independent samples t-tests or Mann–Whitney U tests, according to data distribution.
The level of statistical significance was set at P < .05. All statistical tests were two-tailed.
Results
A total of 25 robotic-assisted pyeloplasty procedures were analyzed: 6 in year 1, 8 in year 2, and 11 in year 3.
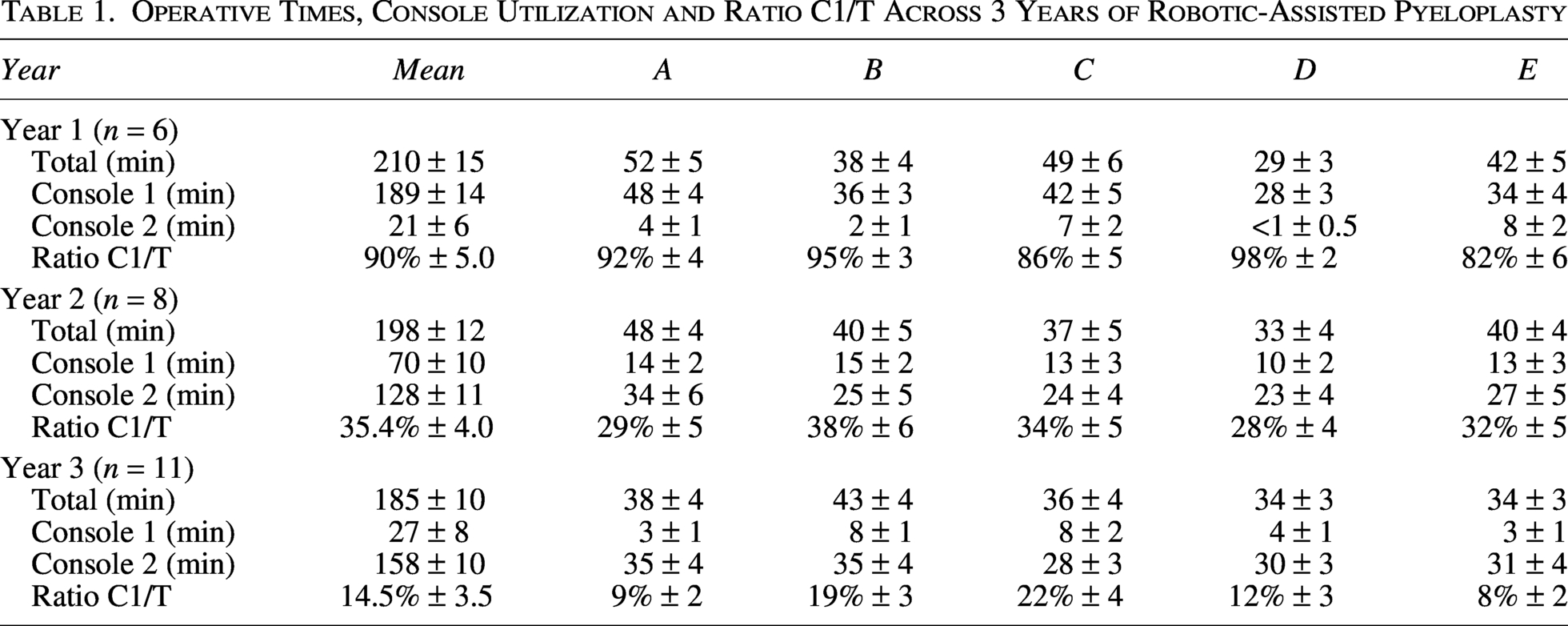
The mean total operative time (T) progressively decreased from 210 minutes in year 1 to 198 minutes in year 2 and 185 minutes in Year 3 (P = .008).
An overall reduction was observed across all five procedural phases (A–E), indicating improved procedural efficiency and workflow standardization.
The expert surgeon’s mean console time (C1) decreased over the 3 years (from 189 minutes the first year to 70 minutes the second year and 27 minutes the third, P < .001), while the non-expert surgeon’s mean console time (C2) increased correspondingly (21 minutes the first year, 128 minutes the second year, and 158 minutes the third year) (P < .001).
The expert console time ratio (C1/T) declined from 90.0% in Year 1 to 35.4% in Year 2 and 14.5% in Year 3 (P < .001), demonstrating a progressive transfer of operative responsibility and autonomy to the non-expert surgeon.
All this data are presented in Table 1.
Operative Times, Console Utilization and Ratio C1/T Across 3 Years of Robotic-Assisted Pyeloplasty
When analyzed by phase, the ratio of expert console time per phase (A–E) decreased proportionally across all components of the procedure, with the steepest reduction observed during phases B (dismemberment) and D (anastomosis) (Fig. 1).
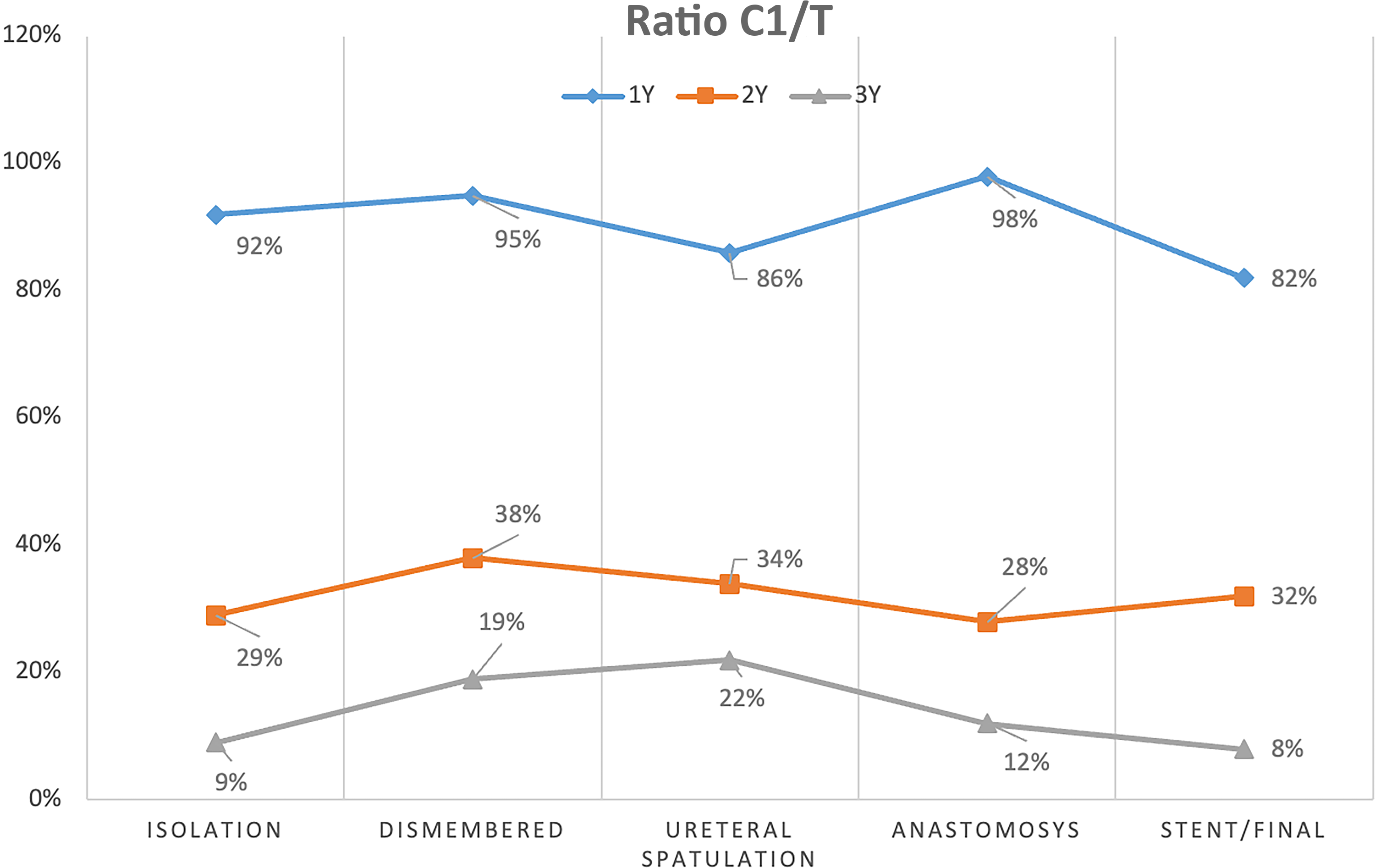
Trend of Expert Console Time Ratio (C1/T) by Surgical Phase Over the Three-Year Training Period.
The total number of instrument collisions recorded for console 2 (non-expert) showed a dramatic reduction, from 1457 in year 1 to 652 in year 2 and 97 in year 3 (P < .001).
Conversely, collision counts for the expert surgeon (console 1) remained low overall, with no statistically significant temporal trend (P = n.s.), despite a slight increase in absolute numbers in Year 3.
This reflects a substantial improvement in hand–eye coordination and spatial awareness for the non-expert operator, consistent with a steep learning curve in robotic-assisted pyeloplasty.
Motion efficiency, as analyzed by the Tracker® software, increased significantly for the non-expert surgeon, from 14% in year 1 to 86% in year 2 and 88% in year 3 (P < .001). Motion efficiency for the expert surgeon remained relatively stable over the 3-year period, without a clear temporal trend (P = n.s.).
Instrument collisions and motion efficiency metrics for both surgeons are summarized in Table 2.
Instrument Collisions and Motion Efficiency Metrics for Expert and Non-Expert Surgeons Over 3 Years

Discussion
Although numerous studies in the literature confirm that robotic surgery has a reduced learning curve,1–3,13 few studies have provided a detailed objective quantification of this process.
Our study aims to provide an objective and quantitative evaluation of the learning curve in robotic-assisted pediatric pyeloplasty, comparing the performance of an expert and a non-expert surgeon using a dual-console system over 3 years.
To achieve this, we analyzed videos of dismembered pyeloplasty procedures performed using the Anderson-Hynes technique, a highly complex laparoscopic procedure. 14
Our results demonstrate a progressive and measurable improvement in the non-expert surgeon’s technical proficiency, as evidenced by reduced operative times, fewer instrument collisions and significantly greater motion efficiency.
These findings support the idea that robotic technology enables a steeper and safer learning curve than conventional minimally invasive surgery.
A recent study (2023) by Planchamp et al., based on an evaluation of surgical times, determined that 30 cases are necessary to acquire a learning curve for a robotic pyeloplasty. 13 This aligns with our case series, which shows that, over approximately 25 consecutive operations, the expert surgeon’s console time ratio decreases significantly from 90% to 14.5%. These results suggest a gradual and structured transfer of operative autonomy, with optimal robotic skills being acquired within 1 year of practice.
A recent randomized controlled trial by Kelly et al. found that a virtual reality warm-up before robot-assisted surgery did not significantly improve early intraoperative performance, suggesting that minimal preparation is sufficient to maintain technical skill in robotic surgery. 15
However, we believe that the use of dual-console assessments is essential to enable an inexperienced surgeon to operate independently. These provide a controlled, real-time mentoring environment, allowing the expert surgeon to supervise and operate if necessary and to progressively delegate more complex procedural steps.
This dynamic appears to accelerate skill acquisition while maintaining patient safety, which is a significant advantage in pediatric surgery, where case volume is often limited. Furthermore, it indirectly affects the cost of training a young surgeon.
For these reasons, integrating a dual-console system should be standard practice in robotic training programs.16,17 These data also suggest that, in RAS, objective performance metrics may eventually serve as credentialing benchmarks, replacing or complementing requirements based on procedure count.
In terms of surgical stages, it appears that expert surgeons have primarily focused on the central stages (dismemberment and ureteral spatulation) over the years. The suturing stage is considered the most critical for this type of surgery and requires expert intervention only in the first year, with a marked reduction in subsequent years. 18 This is probably due to the need for experience-based guidance from the expert rather than manual intervention during the operation itself.
To address this, a tele-mentoring system could be adopted to provide less experienced practitioners with advice. Future research on artificial intelligence applied to robotics will probably address this issue.19,20
Finally, the demonstrated correlation between motion-tracking metrics and established observational assessments suggests that objective, automated systems could be used not only to monitor technical progression and skill retention but also to provide standardized, curriculum-level evaluations of surgical trainees. This makes it good practice to consider adopting such systems across all robotic surgery centers.
This study has several limitations. Firstly, it was a retrospective study conducted in a single center with a fixed expert-trainee pair, which may limit its generalizability. While the relatively small sample size reflects the rarity of pediatric robotic pyeloplasty, it also highlights the value of using objective motion analysis to detect significant trends despite limited case numbers. Future prospective multicenter studies with larger cohorts and standardized performance metrics are needed to validate these findings.
Additionally, while Tracker provides a robust quantitative assessment, it does not consider the qualitative aspects of surgical decision-making or teamwork, which also evolve with experience.
Moreover, the software is not specifically designed for surgery, and we believe that specific RAS software will be created in the future to assist with training.
Conclusions
This study objectively demonstrated progressive and significant improvements in the performance of non-expert surgeons over a 3-year period.
The stable metrics of the expert surgeon, combined with the gradual transfer of operative time, highlight the dual-console approach as an optimal educational model that ensures patient safety and continuous skill development.
Quantitative motion analysis proved to be a valuable, objective tool for monitoring technical progression, offering measurable benchmarks for competency-based robotic training.
We believe that integrating objective performance metrics and dual-console systems into standardized robotic training curricula will accelerate learning while maintaining surgical precision and safety in pediatric patients.
Authors’ Contributions
V.C. and C.E. conceived and designed the study. V.C., C.D.M., F.C., M.S.C., F.T., F.D.C., and M.E. contributed to data collection and analysis. G.E. provided critical revision of the article for important intellectual content. V.C. drafted the article, and all authors reviewed and approved the final version of the article.
All authors agree to be accountable for all aspects of the work.
Ethical Approval
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments. Ethical approval was obtained from the Ethics Committee of the University of Naples Federico II (approval date: June 21, 2008).
Informed Consent
Written informed consent was obtained from all individual participants included in the study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.