
Abstract
Background:
Enhanced recovery after surgery (ERAS) protocols aim to improve perioperative outcomes through evidence-based, multimodal care pathways. While ERAS is well established in radical cystectomy, its role in robotic-assisted radical prostatectomy (RARP) remains less clearly defined. This systematic review and meta-analysis evaluates the safety and efficacy of ERAS protocols in patients undergoing RARP.
Methods:
A systematic search of PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies comparing ERAS or modified ERAS protocols with standard care in patients undergoing RARP were included. Outcomes assessed included length of stay (LOS), return of bowel function, operative time, estimated blood loss, and postoperative complications. A random-effects meta-analysis was performed using Stata 18, with results reported as Hedges’ g standardized mean differences and 95% confidence intervals (CI).
Results:
Seven studies comprising 1314 patients (615 ERAS, 699 standard care) met inclusion criteria. ERAS protocols were associated with a statistically significant reduction in LOS (mean 5.98 versus 7.45 days, Hedges’ g –0.68; 95% CI: –1.21 to –0.15). ERAS also showed an earlier return of gastrointestinal function: time to flatus (mean 1.66 versus 2.03 days, Hedges’ g –0.60; 95% CI: –0.91 to –0.30) and time to defecation (mean 2.68 versus 3.13 days, Hedges’ g –0.43; 95% CI: –0.61 to –0.24). No significant differences were observed in complication rates, operative time, or blood loss.
Conclusions:
ERAS protocols in RARP are associated with improved short-term postoperative recovery, particularly gastrointestinal function. However, the clinical impact on LOS may be modest in contemporary practice, where early discharge is increasingly routine, particularly with the adoption of single-port surgery. Future studies should focus on identifying high-yield ERAS components and evaluating their role in higher-risk patient populations who may derive greater benefit from structured perioperative optimization.
Keywords
Introduction
Prostate cancer remains one of the most prevalent malignancies among men worldwide, with radical prostatectomy representing a cornerstone of curative treatment for localized disease. 1 In recent decades, the adoption of minimally invasive surgical techniques such as robotic-assisted radical prostatectomy (RARP) has become widespread due to improved perioperative outcomes such as reduced blood loss, shorter hospital stay, and faster recovery compared with open and laparoscopic approaches.2,3
Enhanced recovery after surgery (ERAS) programs, originally developed in colorectal surgery, are now being increasingly applied across a range of surgical specialties. 4 These multimodal pre-, peri-, and postoperative care pathways aim to prehabilitate, attenuate the surgical stress response, promote early mobilization and nutrition, reduce postoperative complications, and ultimately shorten the length of hospital stay while improving patient satisfaction. 5 In urology, the implementation of ERAS protocols has been most extensively studied in radical cystectomy, where clinical guidelines have been established by the ERAS Society. 6 However, despite the growing uptake of ERAS in RARP, it’s effectiveness in this setting remains less well defined, and no specialty-specific ERAS guidelines currently exist for prostatectomy.
A previous systematic review and meta-analysis by Zhao et al. (2020) evaluated the impact of ERAS protocols in patients undergoing minimally invasive radical prostatectomy, including both laparoscopic and robotic approaches. That review demonstrated improvements in postoperative recovery parameters, such as reduced length of stay (LOS) and earlier return of bowel function, but the inclusion of heterogeneous surgical techniques limits the generalizability of its findings to contemporary robotic practice. 7
Given the widespread adoption of robotic surgery in prostate cancer management and the increasing interest in ERAS implementation, there is a clear need for an updated synthesis of the evidence focused specifically on RARP. The present systematic review and meta-analysis aims to evaluate the clinical efficacy and safety of ERAS protocols in patients undergoing RARP, using data from contemporary studies that exclusively examined robotic cases. By isolating this population, we aim to provide a more accurate and relevant assessment of the benefits and limitations of ERAS in modern prostate cancer surgery.
Methods
Registration and search strategy
The literature search was conducted in accordance with the latest Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8 The review was prospectively registered on 02/06/2025 in PROSPERO under the registration ID CRD420251065585. A comprehensive literature search was conducted in PubMed, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL) up to 03/06/2025. Search strategies combined free-text keywords related to ERAS and prostatectomy, using Boolean operators, truncation, and field tags as appropriate for each database. No language or publication status restrictions were applied.
In addition, grey literature sources were searched, including Google Scholar, ProQuest Dissertations & Theses Global, and conference proceedings from the American Urological Association, European Association of Urology, and Society of International Urology. Clinical trial registries were searched via ClinicalTrials.gov, the World Health Organization International Clinical Trials Registry Platform, and the EU Clinical Trials Register.
The reference lists of all included studies and a previous systematic review on this topic were screened to identify additional eligible articles. A complete breakdown of included studies is presented in the PRISMA flow diagram (Fig. 1).
PRISMA flow diagram illustrating the study selection process for the systematic review of enhanced recovery after surgery (ERAS) protocols in patients undergoing robotic-assisted radical prostatectomy.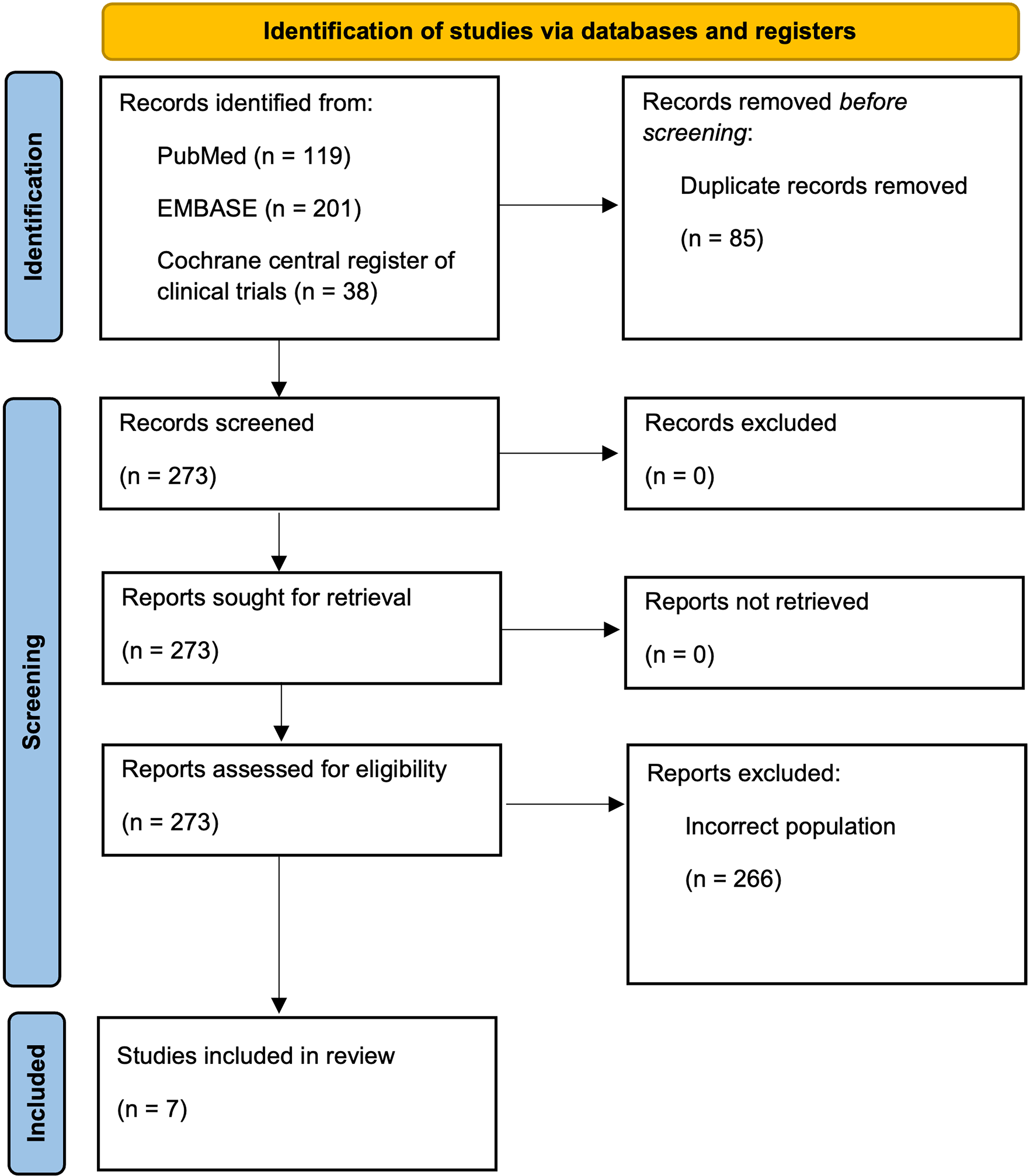
Inclusion criteria:
Patients aged 18 years and older. Studies published after 2000 Studies incorporating ERAS or modified ERAS protocols in the setting of RARP. Randomized controlled trials, as well as prospective or retrospective cohort studies. Studies that clearly detail the ERAS elements implemented. Studies reporting on patient outcomes.
Exclusion criteria:
Case reports, case series, and conference abstracts. Studies that do not include a comparison between ERAS (or modified ERAS) and a standard care control group. Non robotic surgery.
Identification of studies and outcomes of interest
All studies that met the inclusion criteria were incorporated into this review. Study selection was guided by the following PICO framework: 9
Population: Patients undergoing RARP.
Intervention: Implementation of the ERAS program.
Comparison: Standard non-ERAS care.
Outcome: Safety and efficacy-related patient outcomes.
All studies were independently screened by 2 reviewers (J.B. and R.N.) using Rayyan. 10 In cases of disagreement, a third reviewer (W.Q.) facilitated discussion to reach consensus on study eligibility. Duplicate studies were identified and excluded manually without the use of automated tools.
The primary outcomes of interest are LOS, time to first flatus, time to first defecation, time to regular diet, time to ambulation, time to catheter removal and time to drain removal.
Secondary outcomes of interest include operative time, estimated blood loss, postoperative complication rate, oncological outcomes and elements of ERAS utilized.
Data extraction
Patient demographics and relevant variables were extracted from each study and documented using Google Sheets (Mountain View, CA, USA). Data extraction was performed independently by 2 reviewers (J.B. and W.Q.).
Study selection
This systematic review and meta-analysis included all eligible retrospective and prospective studies that satisfied the predefined inclusion and exclusion criteria.
Risk of bias assessment
The risk of bias in non-randomized studies was assessed using a modified version of the Newcastle-Ottawa Scale. 11 This tool evaluates studies across multiple domains, classifying each as either ‘satisfactory’ or ‘unsatisfactory’ and applies a star-based scoring system to reflect methodological quality. Studies were awarded a total score ranging from 0 to 9, with scores of 0 to 2 considered low quality, 3 to 5 moderate quality, and 6 to 9 high quality. Two reviewers (H.T. and W.Q.) independently conducted the assessments, and any discrepancies were resolved through discussion with a third reviewer (J.B.).
Statistical analysis
Statistical analyses were performed using Stata version 18 (StataCorp. 2021. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC). Hedges g standardized mean difference results were reported with 95% confidence intervals, and a P value ≤.05 was considered statistically significant. 12 Heterogeneity among studies was assessed using the I2 statistic, with thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively.13,14 An I2 value greater than 50% was interpreted as evidence of substantial heterogeneity; however, this was not used as the primary reason for choosing random effects. Due to expected variability in study design and populations, a random-effects model was employed. 15
Results
Literature search
After a review of the literature and application of the selection process outlined in Figure 1, seven articles were included in this systematic review.16–22
Study characteristics
Included studies were published between 2017 and 2023 and comprised 699 patients in the standard postoperative cohort and 615 patients in the ERAS cohort. The largest study had 176 standard patients, and the smallest had 20 standard patients.
Patient characteristics
The mean age of the patients included in the standard cohort was 67.75 years, and the ERAS cohort was 66.74 years. The range of mean ages in the standard cohort was 63.50–74.54 years, and in the ERAS cohort was 62.10–73.64 years. The mean ASA scores were similar between both groups when mentioned. The mean PSA was slightly higher in the standard group at 14.25 ug/L compared with 13.55 ug/L in the ERAS cohort. Prostate volume and Gleason score were similar within each cohort. All patients underwent RARP for prostate cancer (Table 1).
Patient Demographics
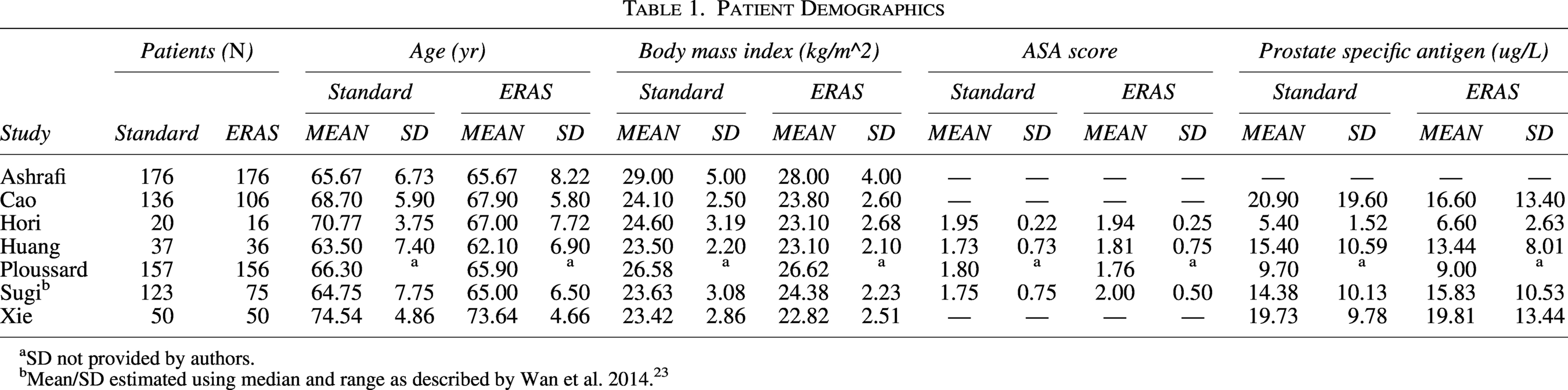
aSD not provided by authors.
bMean/SD estimated using median and range as described by Wan et al. 2014. 23
Postoperative Details
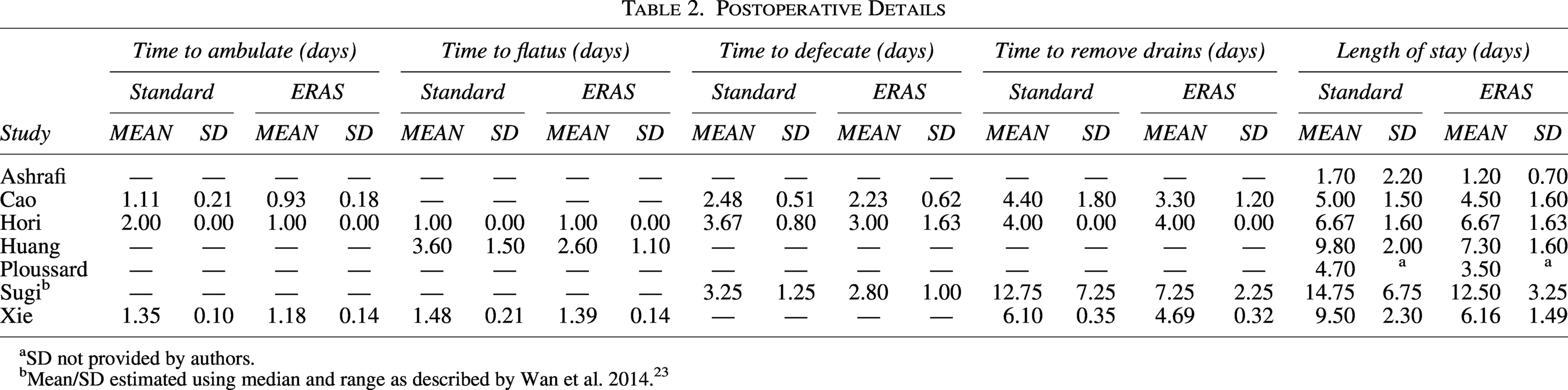
aSD not provided by authors.
bMean/SD estimated using median and range as described by Wan et al. 2014. 23
Primary outcomes
Time to ambulation, flatus, defecation, and drain removal were all significantly shorter in the ERAS group compared with the standard care cohort. Specifically, time to ambulation (mean 1.04 versus 1.49 days) showed a large effect size favoring ERAS, with a pooled Hedges’ g of –1.12 (95% CI: –1.58 to –0.65). Time to flatus (mean 1.66 versus 2.03 days) demonstrated a moderate effect (Hedges’ g –0.60; 95% CI: –0.91 to –0.30) (Fig. 2), while time to defecation (mean 2.68 versus 3.13 days) showed a mild to moderate effect (Hedges’ g –0.43; 95% CI: –0.61 to –0.24). Time to drain removal (mean 4.81 versus 6.81 days) showed the greatest numerical difference; however, the pooled mean difference of –2.55 days (95% CI: –5.21 to 0.10) was not statistically significant. Length of inpatient stay was shorter in the ERAS group (mean 5.98 days versus 7.45 days with standard care), with a pooled Hedges’ g of –0.68 (95% CI: –1.21 to –0.15), displaying a statistically significant effect on reduction in hospital stay favoring ERAS protocols (Table 2 and Fig. 3) (Supplementary Figures S1, S2, and S3).
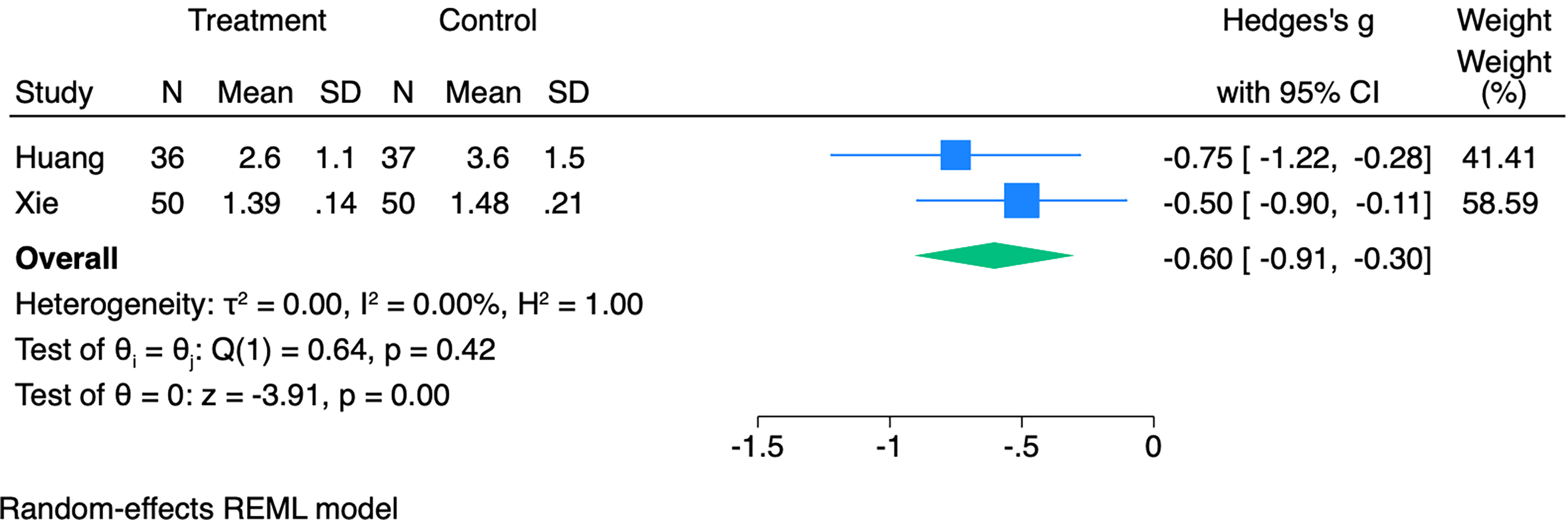
Forest plot of standardized mean differences (Hedges’ g) comparing time to flatus between (treatment) ERAS and (control) standard care following RARP. CI, confidence interval.
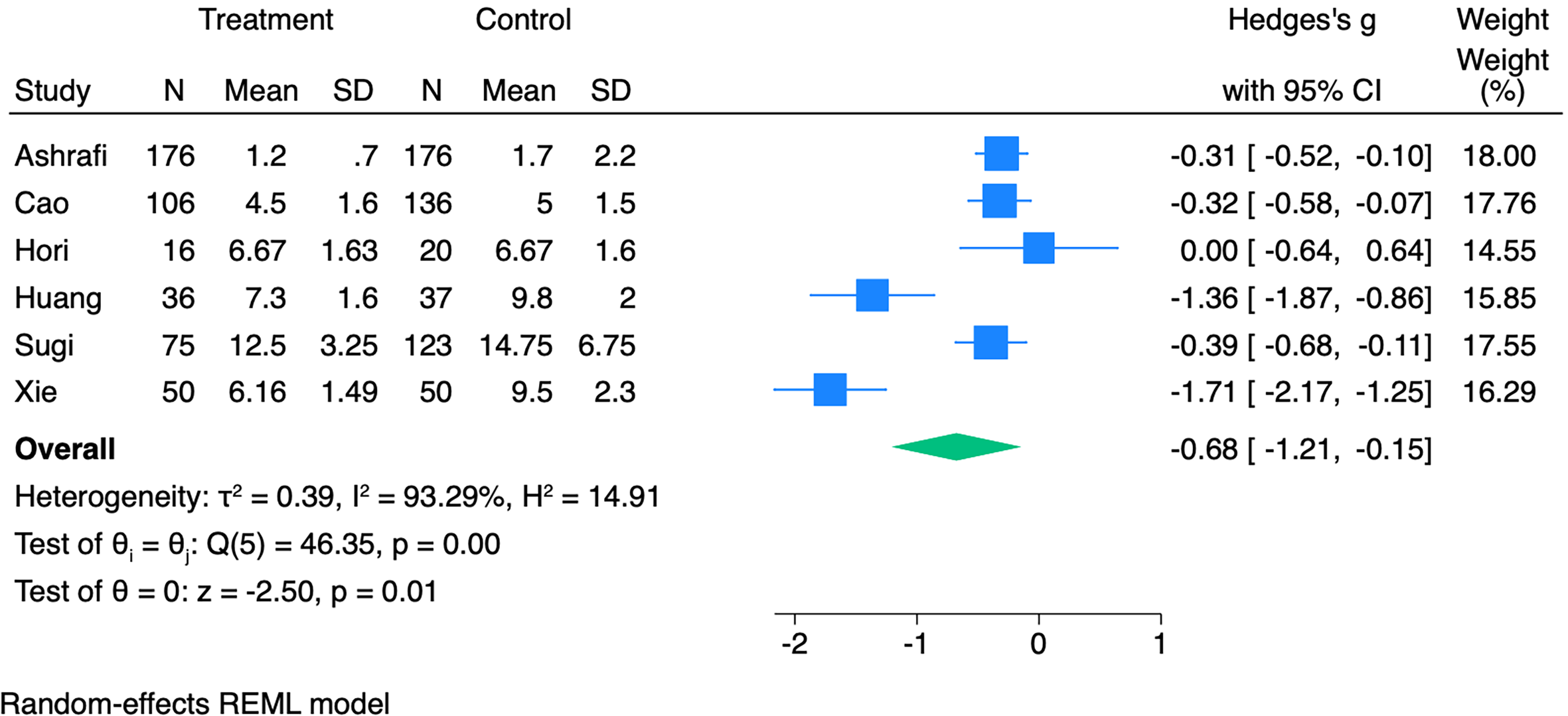
Forest plot of standardized mean differences (Hedges’ g) comparing length of stay between (treatment) ERAS and (control) standard care following RARP. CI, confidence interval.
Operative Info
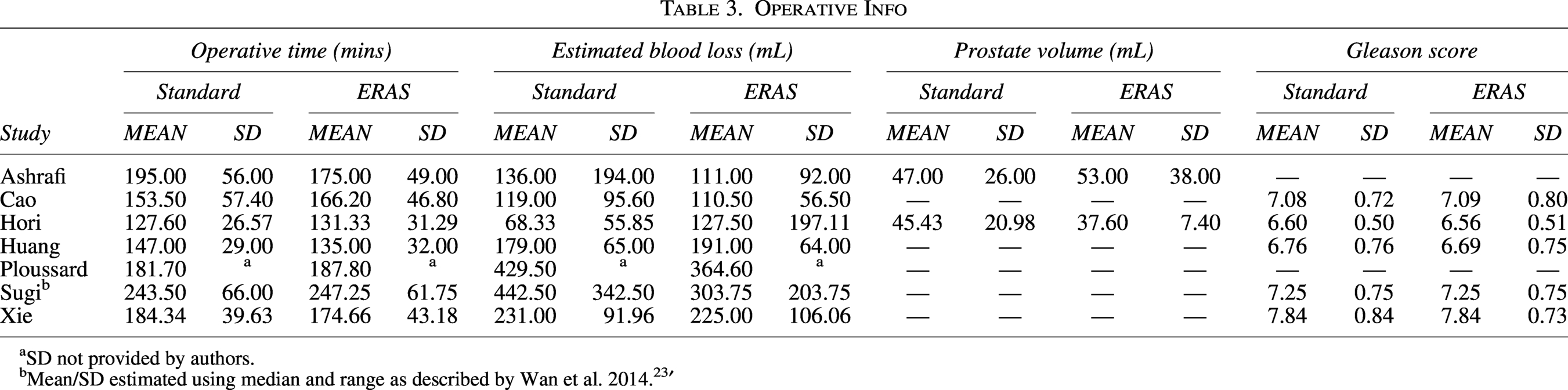
aSD not provided by authors.
bMean/SD estimated using median and range as described by Wan et al. 2014. 23 ′
Secondary outcomes
The mean operative time and intraoperative blood loss of patients in the standard cohort were slightly higher than in the ERAS group; however, this was not statistically significant (176.09 minutes versus 173.89 minutes and 229.33 mL versus 204.76 mL) (Table 3) (Supplementary Fig. S4 and 4). Postoperative complications occurring within 30 days of the procedure date were recorded using the Clavien–Dindo Classification 24 with no statistically significant difference detected between groups (Supplementary Table S1 and Supplementary Figures S6, S7, and S8).
The number of ERAS elements implemented was assessed. The study with the highest compliance was Cao et al. with 13/15 elements. 18 For all studies mentioned, the median ERAS elements implemented was 10 (range: 8–13) (Supplementary Table S2). Across the included studies, there was high concordance in the implementation of core ERAS elements, with preoperative education, omission of mechanical bowel preparation, limited preoperative fasting, multimodal pain control, early mobilization, and early oral intake implemented in 7/7 studies (100%). Avoidance of nasogastric tubes was reported in 6/7 studies (86%), while goal-directed fluid therapy was incorporated in 5/7 studies (71%). In contrast, preoperative carbohydrate loading and formal preoperative nutritional optimization were each utilized in 4/7 studies (57%), and prevention of intraoperative hypothermia was reported in 3/7 studies (43%). Specific measures aimed at preventing postoperative ileus were infrequently described (1/7 studies, 14%), and epidural analgesia was not utilized in any study (0/7). Pharmacological venous thromboembolic prophylaxis was not explicitly reported as an ERAS component in any included study (0/7).
One study reported oncological outcomes and found there was no statistically significant difference in post-operative histopathology between groups. 22
Risk of bias
Two studies were “very good,” four studies were “good,” one study was “satisfactory,” and zero studies were “unsatisfactory.” Supplementary Table S3 summarizes the results of our risk of bias assessment.
Discussion
This is the first systematic review and meta-analysis to exclusively evaluate the impact of ERAS protocols in patients undergoing RARP, thereby eliminating confounding from mixed surgical modalities and providing a more accurate assessment of outcomes in contemporary robotic practice.
A key finding of this review was a significantly earlier return of bowel function in patients managed with ERAS protocols. Time to flatus and defecation were both reduced in the ERAS group, with pooled effect sizes indicating small to moderate clinical benefit. These improvements are likely attributable to several ERAS components, including early oral intake and minimization of perioperative opioids, which is shown to enhance gastrointestinal motility.4,5,25 The consistency of these results across multiple studies suggests that gastrointestinal recovery is a reliable and reproducible benefit of ERAS in the context of RARP.
While gastrointestinal recovery appears to be a consistent benefit of ERAS in RARP, comprehensive interpretation of individual ERAS components is limited by the lack of standardized definitions and heterogeneous reporting across studies. Although several elements were commonly included, the specific content, timing, and intensity of these interventions were variably described, precluding meaningful pooling of individual ERAS components or component-specific meta-analysis. Consequently, assessment of ERAS implementation was restricted to qualitative synthesis, highlighting patterns of utilization rather than quantifying the independent contribution of individual elements.
Notwithstanding these limitations, several key ERAS components emerged as central to enhanced recovery following RARP. In addition to early feeding and opioid minimization, which likely underpin improved bowel function, early mobilization was universally prioritized and is particularly relevant in this population, given its role in reducing thromboembolic risk and facilitating functional recovery after minimally invasive pelvic surgery. 26 Preoperative education, including counselling regarding postoperative expectations and indwelling catheter care, was also consistently incorporated and may contribute to improved patient engagement, adherence to early mobilization and feeding targets, and readiness for early discharge. Together, these findings suggest that ERAS pathways for RARP preferentially emphasize interventions that support rapid functional recovery and patient self-management, while variation in protocol composition underscores the need for standardized reporting of ERAS elements in future studies.
Beyond physiological benefits, earlier return of gastrointestinal function has meaningful implications for patient well-being. Zhou et al. showed that faster bowel recovery following intestinal surgery achieved via enhanced recovery protocols is associated with reduced stress, improved nutrition, and higher patient satisfaction. 27 Patients in the rapid recovery group had shorter times to flatus and defecation, fewer adverse events, and lower stress markers such as insulin resistance and cortisol. These findings suggest that early GI recovery supports both physical and psychological health, reinforcing ERAS as a valuable tool for enhancing postoperative outcomes and patient experience following RARP. 27
While this meta-analysis demonstrated a statistically significant reduction in LOS favoring ERAS protocols, the clinical significance may be more nuanced. In many Western countries such as the USA, Australia, and the UK, routine discharge on postoperative day one following RARP is already standard practice.28,29 Consequently, reductions in LOS may offer limited incremental benefit in high-volume centers with established early discharge pathways and robust outpatient support. In contrast, the observed LOS reductions may be more clinically meaningful in health care settings where baseline hospitalization remains prolonged or where structured perioperative pathways are less established, suggesting that the impact of ERAS on LOS is highly system-dependent.
While the widespread adoption of next-day discharge has limited the overall impact of ERAS protocols in routine RARP, there may be a potential role for ERAS in selected patient subgroups at higher risk of delayed recovery. Patients with a history of extensive opioid use, prior abdominal surgery requiring adhesiolysis, or other factors predisposing to postoperative ileus may particularly benefit from a structured ERAS pathway. 23 In these individuals, targeted interventions such as opioid-sparing analgesia, early mobilization, and early reintroduction of oral intake may help mitigate delays in gastrointestinal recovery and reduce overall LOS. Tailoring ERAS components to address these specific risk factors could enhance recovery trajectories and improve patient outcomes in otherwise complex cases. An area of increasing relevance within ERAS protocols for single-port RARP where same-day discharge is common is the postoperative home recovery phase. There is a need for high-quality evidence evaluating the impact of structured home-based recovery and exercise programs on key outcomes such as hospital readmission rates, early return of urinary continence, and preservation of erectile function. The development of formal, evidence-based recommendations in this domain is essential to optimize long-term functional outcomes for men undergoing single-port RARP.
Importantly, the implementation of ERAS protocols did not increase the risk of postoperative complications. Rates of Clavien–Dindo grade I–III complications were comparable between ERAS and standard care groups, reinforcing the safety of accelerated recovery pathways in the setting of RARP. Additionally, ERAS implementation had no significant impact on operative metrics such as duration of surgery or estimated blood loss.
There are several limitations of this systematic review and meta-analysis. The overall number of included studies was small, with only seven meeting the eligibility criteria, limiting the statistical power and generalizability of the findings. Most studies were retrospective in design, which introduces potential bias and limits causal inference. There was also substantial heterogeneity in ERAS protocol composition across studies, with the number of implemented elements ranging from 8 to 13. This variation complicates efforts to identify which specific interventions are most responsible for the observed benefits. Furthermore, only one included study reported oncological outcomes, and none meaningfully evaluated key functional recovery metrics such as urinary continence or erectile function. As such, the findings of this review are limited to short-term perioperative and gastrointestinal recovery outcomes and do not inform the oncologic or functional efficacy of ERAS protocols in RARP.
The definition of “time to ambulation” was not uniform across included studies; one study explicitly defined this as the first postoperative time out of bed, while the remaining studies reported it more generally as “time to ambulation” without further specification, which may contribute to inter-study variability in this outcome.
Future research should focus on delineating which individual components of ERAS protocols contribute most significantly to improved outcomes in the pre, peri and post operative domain, particularly in the context of RARP, where routine early discharge is already standard. Additionally, further studies are warranted to assess the role of ERAS in select high-risk patients who may still benefit from a more structured perioperative approach to enhance recovery and reduce complications, while also incorporating standardized reporting of functional and oncologic endpoints to better define the broader clinical impact of ERAS pathways.
Conclusion
ERAS protocols in RARP improve gastrointestinal recovery and modestly reduce hospital stay without compromising safety. However, with early discharge already common, routine ERAS may offer limited benefit. Future focus should be on identifying the most effective components and targeting high-risk patients, such as those with prior abdominal surgery or chronic opioid use.
Authors’ Contributions
J.B., B.M.C. and N.A.C. contributed to drafting the main article text. J.B., R.N., and W.Q. were involved in data collection and assisted with the screening and review of publications during the literature search. B.M.C. conducted the statistical analysis whilst H.C.T. and W.Q. facilitated the risk of bias assessment. B.M.C. provided overall supervision and strategic direction for the project. All authors critically reviewed and approved the final version of the article.
Supplemental Material
sj-docx-1-lat-10.1177_10926429261468581 — Supplemental material for Effectiveness of Enhanced Recovery After Surgery Protocols for Robot Assisted Radical Prostatectomy Radical Prostatectomy: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-lat-10.1177_10926429261468581 for Effectiveness of Enhanced Recovery After Surgery Protocols for Robot Assisted Radical Prostatectomy Radical Prostatectomy: A Systematic Review and Meta-Analysis by Joshua Bruinsma, Nicholas A. Clausen, Rostyslav Nikolenko, Hugo C. Temperley, Wanyang Qian, and Benjamin M. Mac Curtain
Footnotes
Declaration of Use of Generative AI
During the preparation of this article, the authors used ChatGPT (OpenAI) to assist with language refinement and proof reading. After using this tool, the authors carefully reviewed, edited, and verified all content to ensure accuracy and originality, and the authors take full responsibility for the final article.
Availability of Data and Materials
All data generated or analyzed during this study are included in the published article and the supplementary information.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was provided or sought for this systematic review.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.