
Abstract
Introduction:
The optimal level of inferior mesenteric artery (IMA) ligation during colorectal cancer (CRC) surgery remains controversial. Low ligation with preservation of the left colic artery (LCA) may maintain bowel perfusion, but concerns persist regarding adequacy of central lymph node dissection.
Aim:
To evaluate the technical feasibility and short-term safety of central lymphadenectomy at the IMA root during low ligation with preservation of the LCA in laparoscopic CRC surgery.
Methods:
This prospective observational study included 30 patients with nonmetastatic sigmoid colon or rectal adenocarcinoma who underwent laparoscopic resection between October 2025 and April 2026 at the National Cancer Institute, Cairo University. Low ligation of the IMA with LCA preservation and central lymphadenectomy at the IMA root was performed in all cases. Feasibility, lymph node retrieval, operative outcomes, and short-term postoperative outcomes were assessed.
Results:
All procedures were completed laparoscopically without conversion to open surgery. Preservation of the LCA and successful central lymphadenectomy were achieved in all patients. Mean total lymph node harvest was 24 ± 4, while mean central node retrieval was 5 ± 1. R0 resection was achieved in all cases. Mean operative time was 180 ± 19 minutes. Postoperative complications occurred in 10% of patients, including one case of anastomotic leakage (3.3%). Median hospital stay was 4 days.
Conclusions:
Central lymphadenectomy during low ligation of the IMA is feasible and safe in laparoscopic CRC surgery, providing adequate nodal harvest while preserving colonic vascular supply.
Keywords
Introduction
Colorectal cancer (CRC) continues to represent a major global health burden, ranking among the most frequently diagnosed malignancies and a leading cause of cancer-related mortality worldwide. 1 Despite advances in multimodal treatment, surgical resection remains the cornerstone of curative therapy, necessitating continuous refinement of operative strategies to optimize both oncologic efficacy and perioperative safety.
Minimally invasive approaches have transformed the surgical management of CRC. Laparoscopic resection is now widely accepted as an oncologically sound alternative to open surgery, providing comparable long-term outcomes while conferring well-established short-term benefits, including reduced postoperative pain, faster recovery, and decreased morbidity.2,3
Adequate lymphadenectomy is a critical determinant of oncologic quality in colorectal surgery, ensuring accurate staging and contributing to prognostic stratification. Traditionally, high ligation of the inferior mesenteric artery (IMA) at its aortic origin has been advocated to facilitate complete clearance of apical lymph nodes. However, this approach may compromise perfusion to the distal colon, potentially increasing the risk of ischemia-related complications, particularly anastomotic leakage. 4
Conversely, low ligation of the IMA with preservation of the left colic artery (LCA) has been proposed as a strategy to maintain vascular supply to the anastomosis. While this technique offers physiological advantages, concerns persist regarding its oncologic adequacy, specifically the potential for incomplete dissection of central lymph nodes located at the IMA root.5,6
Recent surgical concepts have sought to reconcile these competing priorities by combining vascular preservation with radical oncologic resection. Central lymphadenectomy at the IMA origin performed in conjunction with low ligation represents a technically demanding approach aimed at achieving adequate nodal clearance without compromising colonic perfusion. However, evidence regarding its technical feasibility, safety, and reproducibility in laparoscopic colorectal surgery remains limited.7,8
The present study was designed to evaluate the feasibility of central lymphadenectomy at the IMA root during low ligation in laparoscopic CRC surgery. The primary objectives were to assess the adequacy of lymph node retrieval at the IMA root, operative performance, and short-term perioperative outcomes.
Methods
Study design and setting
This prospective observational study was conducted at the National Cancer Institute, Cairo University, from October 2025 to April 2026. The study aimed to assess the feasibility and safety of performing central lymphadenectomy at the root of the IMA during low ligation in laparoscopic CRC surgery.
Patient selection
As this was an exploratory feasibility study, a sample of 30 consecutive eligible patients with histologically confirmed colorectal adenocarcinoma was prospectively enrolled to assess technical feasibility, safety, and preliminary oncologic outcomes.
Inclusion criteria included age ≥18 years, tumors located in the sigmoid colon or rectum, clinical staging consistent with nonmetastatic disease (cT1–T3, N0–N2, M0), and eligibility for elective laparoscopic resection.
Exclusion criteria included distant metastases, locally advanced unresectable tumors (cT4b), emergency presentation (e.g., obstruction or perforation), prior major abdominal surgery limiting laparoscopic access, and severe comorbidities precluding general anesthesia or minimally invasive surgery.
Preoperative evaluation
All patients underwent standardized preoperative assessment, including detailed clinical evaluation; colonoscopy with histopathological confirmation; contrast-enhanced computed tomography of the chest, abdomen, and pelvis; and routine laboratory investigations. Patients with rectal cancer received neoadjuvant chemoradiotherapy when indicated, in accordance with our institution’s protocol.
Surgical technique
All procedures were performed laparoscopically by experienced colorectal surgeons following a standardized technique. After medial-to-lateral mobilization of the left colon, the IMA was identified at its origin from the abdominal aorta (Fig. 1).
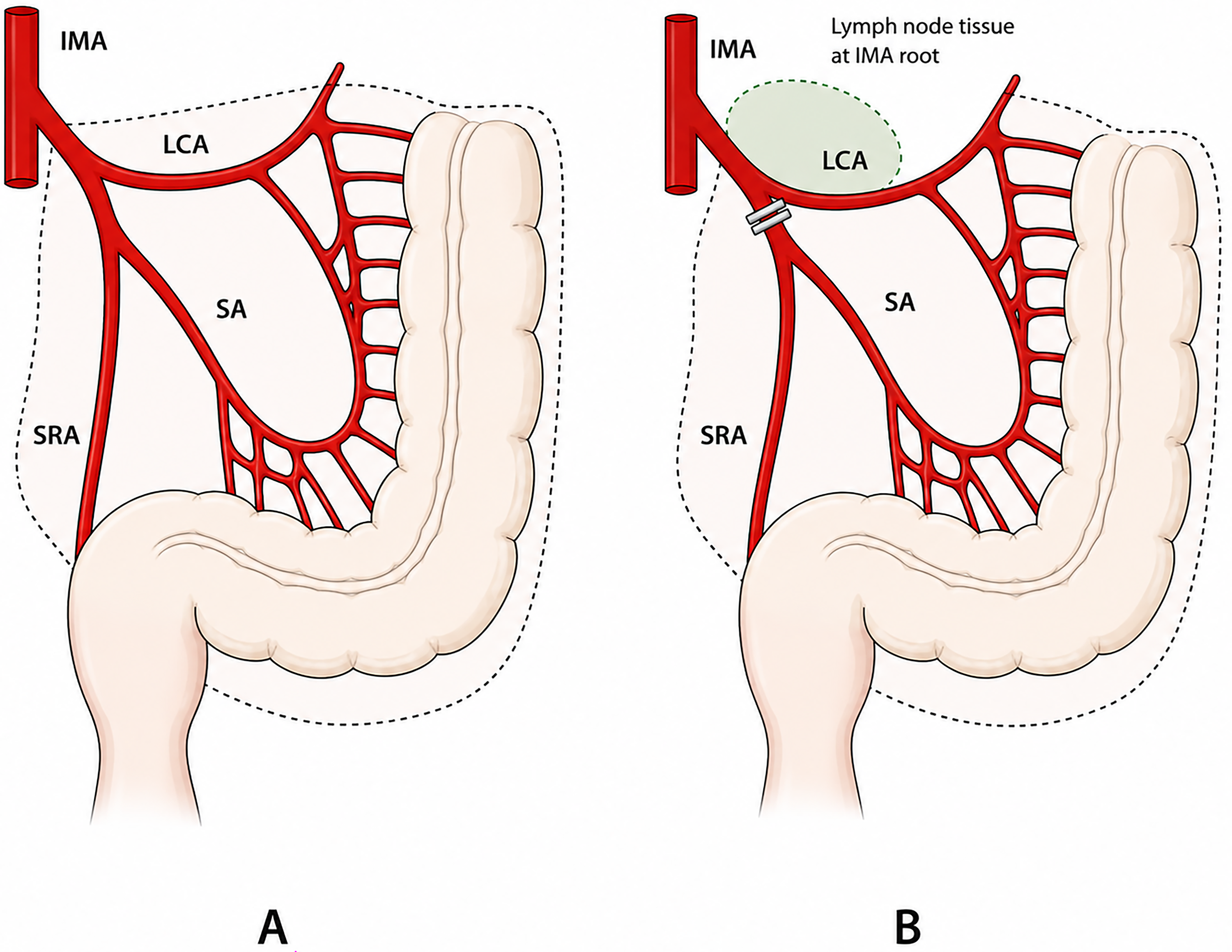
(
Low ligation of the IMA was performed distal to the origin of the LCA, with preservation of the LCA to maintain adequate colonic perfusion. Central lymphadenectomy was subsequently carried out through meticulous dissection of lymphatic tissue at the IMA root, including apical lymph nodes, while preserving the arterial supply (Fig. 2).
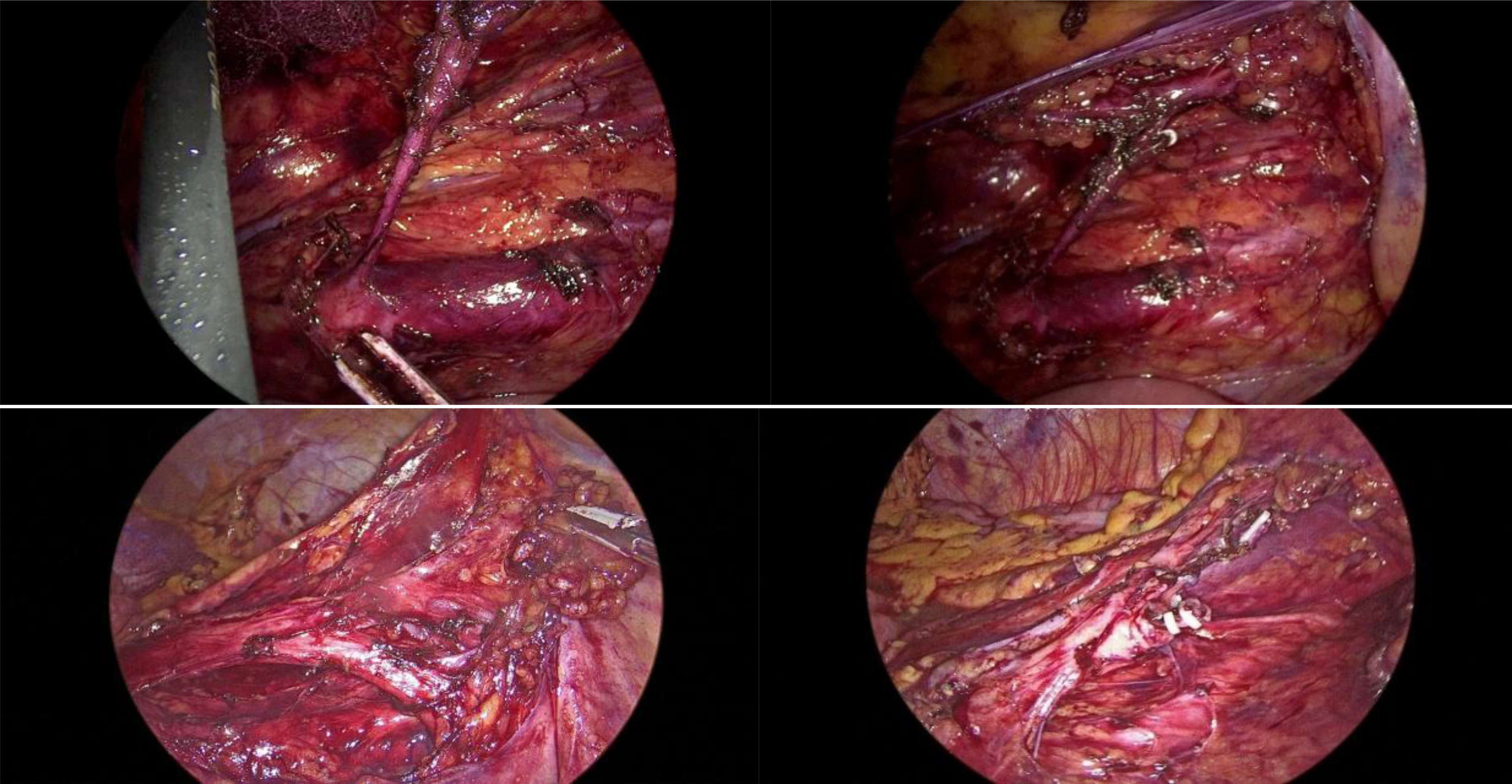
Intraoperative laparoscopic views from two cases illustrating central lymphadenectomy at the inferior mesenteric artery root followed by low ligation with preservation of the left colic artery.
The inferior mesenteric vein was divided when indicated. Resection of the affected bowel segment adhered to oncologic principles, ensuring adequate proximal and distal margins. Reconstruction was performed using stapled anastomosis after adequate mobilization of the remaining colonic segment.
Outcome measures
The primary endpoint was procedural feasibility, defined as successful laparoscopic preservation of the LCA with complete central lymphadenectomy at the IMA root without conversion to open surgery.
Secondary endpoints included total lymph node yield, operative time, intraoperative blood loss, conversion to open surgery, postoperative complications, and length of hospital stay.
Postoperative management and follow-up
Postoperative care followed standardized perioperative protocols, including early mobilization and progressive reintroduction of oral intake. Complications were recorded and graded according to the Clavien-Dindo classification. All patients were followed for a minimum of 30 days to evaluate short-term surgical outcomes and safety.
Ethical considerations
The study protocol was approved by the institutional review board (IRB Review Number: 2510-510-140-203).
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics software. Data were checked for completeness and accuracy prior to analysis. Continuous variables were presented as mean ± standard deviation or median and interquartile range, depending on data distribution, which were assessed using the Shapiro–Wilk test. Categorical variables were expressed as counts and percentages. All statistical tests were two sided. P values of <.05 were considered significant.
Results
This exploratory study comprised 30 patients with CRCs involving the sigmoid colon and rectum, all of whom underwent laparoscopic surgery to assess the feasibility of performing central lymphadenectomy at the root of the IMA. Each patient completed a 30-day follow-up period. The mean age was 49.7 ± 8.2 years. The most common tumor location was the lower rectum (36.7%), followed by the sigmoid colon (30%). Baseline characteristics of the cohort are presented in Table 1.
Baseline Characteristics of the Studied Group (n = 30)
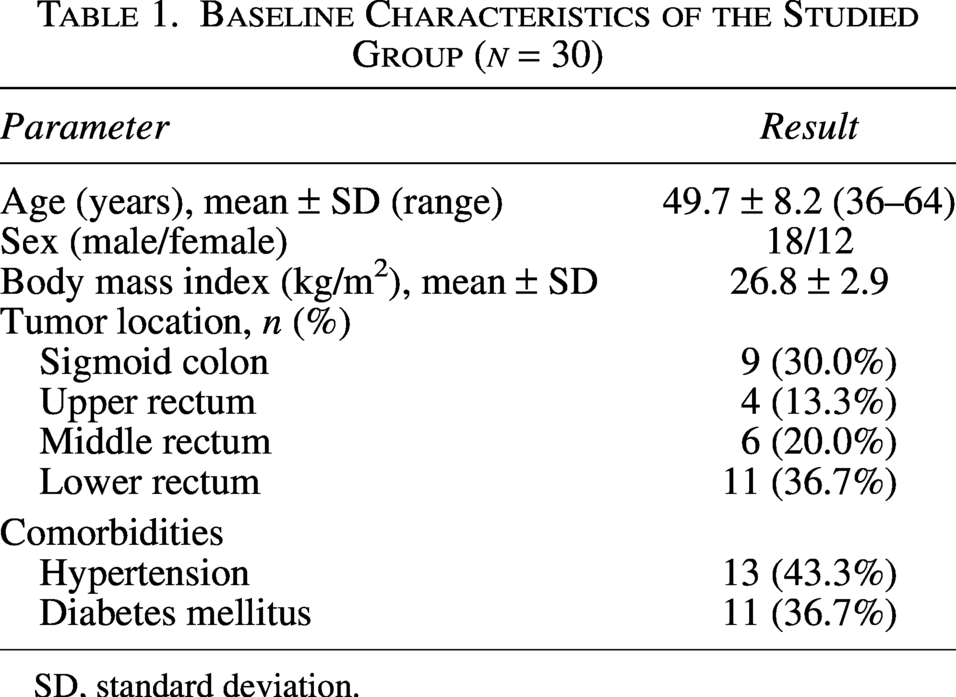
SD, standard deviation.
Low or ultralow anterior resection was the predominant surgical procedure in this study. Neoadjuvant chemoradiotherapy was administered to 43.3% of patients with locally advanced rectal cancer. No procedures required conversion to open surgery. Preservation of the LCA was achieved with a technical success rate of 100%. The IMA was identified up to the origin of the LCA, with structural integrity maintained after removal of adjacent central lymph nodes. Operative details are presented in Table 2.
Treatment Details of the Studied Group
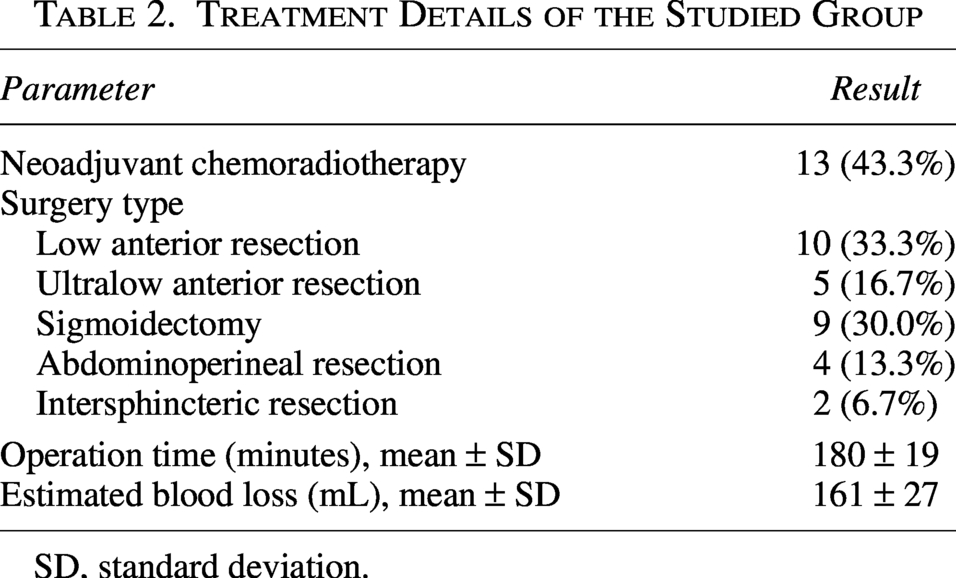
SD, standard deviation.
Pathological TNM staging demonstrated that the majority of tumors were classified as T3 lesions (76.7%), while the remaining cases were T2 tumors (23.3%). Regarding nodal involvement, N1 disease represented the most frequent nodal stage, observed in 53.4% of patients, followed by N2 disease in 33.3%, whereas only 13.3% of cases were node negative (N0). All patients were free from distant metastasis at the time of surgery (M0).
The total number of lymph nodes retrieved met adequacy criteria (≥12) for all patients, with counts ranging from 17 to 30. Central node harvest varied between 4 and 7 per case. Oncologic radicality was preserved, as evidenced by a 100% rate of R0 resection. The number of harvested central lymph nodes was not affected by the type of surgery, comparing low or ultralow anterior resection versus other types. Similarly, there was no difference between sigmoid and rectal cancer cases in the number of central lymph nodes yielded. There was no correlation between the number of harvested central nodes and the total number of harvested nodes. Detailed oncologic outcomes are shown in Table 3.
Oncologic Outcomes of the Studied Group
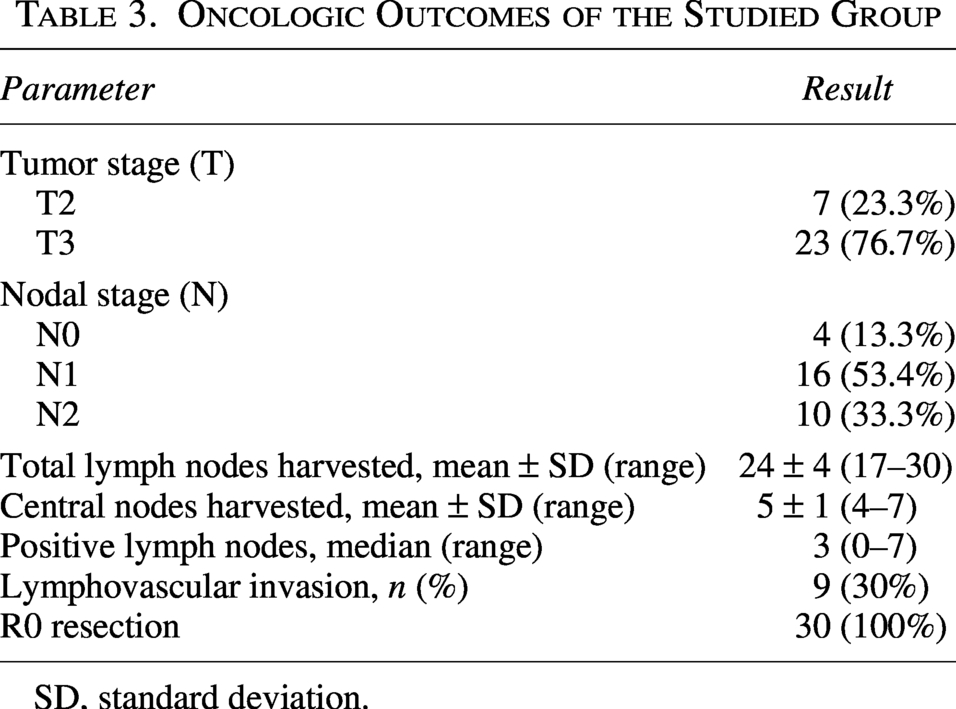
SD, standard deviation.
The median time to restoration of bowel function was 2 days, highlighting the technique’s potential for facilitating prompt gastrointestinal recovery following surgery. A single patient underwent reoperation for ileostomy diversion. Postoperative morbidity was evaluated using the Clavien-Dindo classification system. In total, postoperative complications were observed in three patients (10.0%). One patient experienced both wound infection and anastomotic leakage (3.3%), while two others developed postoperative ileus. The low rate of anastomotic leakage suggests that low ligation of the IMA may provide adequate bowel perfusion. No patients required hospital readmission during the 30-day follow-up period. Detailed postoperative outcomes are shown in Table 4.
Postoperative Outcomes of the Studied Group
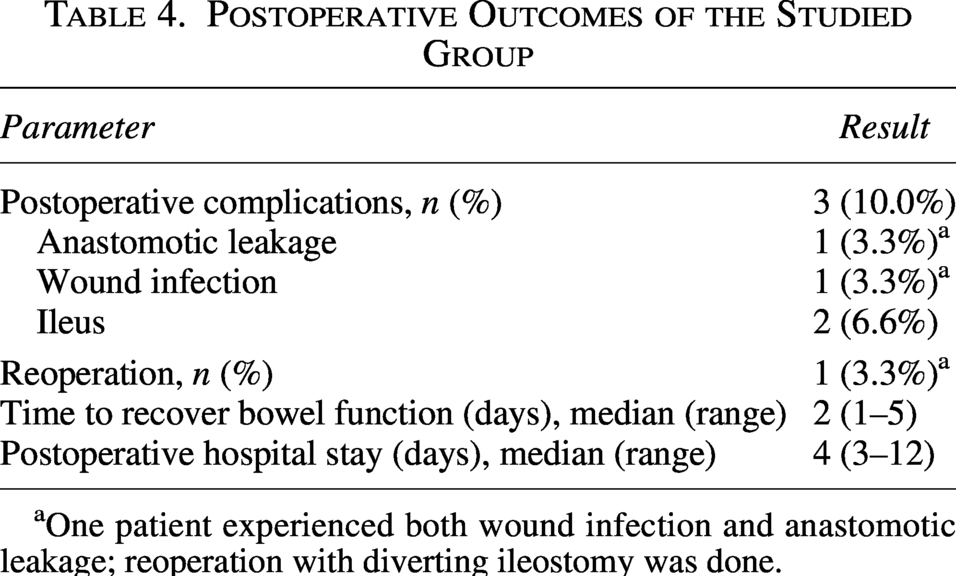
One patient experienced both wound infection and anastomotic leakage; reoperation with diverting ileostomy was done.
Discussion
The optimal level of IMA ligation during CRC surgery remains controversial. While high ligation has traditionally been advocated to facilitate radical lymphadenectomy and complete apical nodal clearance, concerns regarding impaired colonic perfusion and postoperative morbidity have encouraged increasing interest in low ligation with preservation of the LCA. The present study evaluated the feasibility of combining low ligation with central lymphadenectomy during laparoscopic CRC surgery and demonstrated that this approach is technically achievable, oncologically adequate, and associated with acceptable short-term outcomes. The present approach resembles D3 lymphadenectomy as described by the Japanese Society for Cancer of the Colon and Rectum while preserving the LCA through low vascular ligation.
In the current series, preservation of the LCA was successfully achieved in all patients without conversion to open surgery. In addition, central lymph node dissection at the IMA root was completed laparoscopically in every case, supporting the technical reproducibility of this approach when performed by experienced colorectal surgeons. These findings are consistent with recent studies suggesting that low ligation combined with apical lymphadenectomy can provide oncologic radicality comparable to high ligation while maintaining vascular integrity of the proximal bowel segment.9,10
Adequate lymph node retrieval remains a major quality indicator in CRC surgery. In the present study, the mean total lymph node harvest was 24 ± 4 nodes, with a mean of 5 ± 1 central nodes retrieved at the IMA root. Importantly, all patients exceeded the recommended minimum harvest threshold of 12 lymph nodes. This supports the oncologic adequacy of the procedure and suggests that preservation of the LCA does not compromise nodal clearance when meticulous central lymphadenectomy is performed. Similar observations were reported by Yin et al., who demonstrated equivalent apical node retrieval between low ligation with high dissection and conventional high ligation techniques. 9
Anastomotic integrity remains strongly influenced by tissue perfusion, particularly in rectal surgery where distal blood flow may already be compromised following mesorectal excision. The low incidence of anastomotic leakage observed in this cohort may be attributable to preservation of colonic perfusion through maintenance of the LCA. Several meta-analyses have demonstrated lower rates of anastomotic leakage and postoperative morbidity with low ligation when compared with high ligation techniques.9,11 Our findings further support the concept that vascular preservation can be achieved without sacrificing oncologic radicality.
Another notable finding in this study was the absence of any significant relationship between the number of harvested central nodes and either tumor location or surgical procedure type. This suggests that central lymphadenectomy at the IMA root can be consistently performed across different left-sided colorectal resections. Moreover, the lack of correlation between total harvested nodes and central node yield indicates that targeted central dissection represents a distinct oncologic component rather than merely a reflection of overall nodal retrieval.
The operative outcomes reported in the current study were also acceptable. Mean operative time and blood loss were comparable to previously published laparoscopic colorectal series utilizing advanced vascular-preserving techniques. 12 Furthermore, postoperative recovery was favorable, with early return of bowel function and a relatively short hospital stay. These findings support the feasibility of incorporating central lymphadenectomy into minimally invasive colorectal surgery without substantial perioperative burden.
From an oncologic perspective, the rationale for high ligation has historically centered on the possibility of apical lymph node metastasis and more radical D3 lymphadenectomy. However, multiple contemporary studies have questioned whether routine sacrifice of the LCA translates into superior survival outcomes. Increasing evidence suggests that low ligation combined with apical node dissection may achieve equivalent oncologic clearance while reducing ischemic complications and autonomic nerve injury.10,13 Preservation of autonomic nerve fibers surrounding the IMA origin may additionally contribute to improved postoperative urinary and sexual function, although these parameters were not specifically assessed in the present study because of the relatively short follow-up period, warranting further long-term functional evaluation.
Patient selection and intraoperative assessment of colonic perfusion are important when adopting low IMA ligation with central lymphadenectomy. Although LCA preservation is generally advantageous, collateral circulation may be insufficient in patients with vascular disease or poor mesenteric flow. Intraoperative indocyanine green (ICG) fluorescence imaging has been shown in recent meta-analyses to improve assessment of anastomotic perfusion and reduce leakage rates, supporting its use as an adjunct in vascular-preserving strategies. 14 Future studies incorporating perfusion-guided decision-making and stratified patient cohorts may help refine indications for this technique and optimize oncologic and functional outcomes.
This feasibility study benefits from its prospective design, standardized laparoscopic technique, and focused evaluation of central lymphadenectomy during LCA preserving low ligation. However, it has several limitations. First, the relatively small sample size and single-center design may limit generalizability. Second, the follow-up period was restricted to short-term outcomes, preventing assessment of genitourinary function and long-term oncologic outcomes such as disease-free survival, overall survival, and recurrence patterns. In addition, the absence of a direct comparison group undergoing conventional high ligation limits definitive conclusions regarding superiority between techniques. Last, the absence of routine perfusion assessment using IGC fluorescence imaging represents another limitation because objective evaluation of anastomotic blood supply was not performed.
Nevertheless, the prospective design and standardized operative approach strengthen the validity of the presented findings. Overall, the present study demonstrates that central lymphadenectomy during low ligation of the IMA is feasible and safe in laparoscopic CRC surgery. The technique allows adequate central nodal retrieval while preserving the LCA and maintaining favorable perioperative outcomes. Larger comparative studies with long-term oncologic follow-up are warranted to further define the role of this vascular-preserving strategy in modern CRC surgery.
Conclusions
Central lymphadenectomy at the root of the IMA during low ligation is a feasible and safe technique in laparoscopic CRC surgery. Preservation of the LCA can be achieved without compromising the adequacy of lymph node harvest or oncologic radicality. The technique was associated with favorable short-term perioperative outcomes, low conversion and complication rates, and acceptable postoperative recovery. These findings support further evaluation of vascular-preserving low ligation combined with central lymphadenectomy in larger comparative studies. This approach appears to be a promising vascular-preserving strategy that maintains oncologic adequacy while potentially avoiding the disadvantages associated with conventional high ligation. Further large-scale studies with long-term oncologic follow-up are required to validate these findings.
Authors’ Contributions
A.E.F.M.O. developed the main concept of the study and drafted the article. F.A.F. contributed to the review of the literature. I.A.S. was responsible for data collection and performed the statistical analysis. W.A.S. contributed to the critical revision and editing of the article. All authors reviewed the final version of the article and approved it for submission.
Ethics Approval and Consent to Participate
This research was performed at the Department of Surgical Oncology, National Cancer Institute, Cairo University, Egypt. All data were collected and analyzed after approval of the Institutional Review Board and Ethical Research Committee (IRB Review Number: 2510-510-140-203).
Footnotes
Acknowledgment
The authors are grateful to all individuals who actively participated in and contributed to this study.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author upon request.
Author Disclosure Statement
The authors report no conflicts of interest in the materials or methods used in this study.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.