
Abstract
Background:
Severe obesity is a growing global health issue and a significant risk factor for cardiovascular diseases. Bariatric and metabolic surgeries, such as sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB), are effective interventions for managing cardiometabolic comorbidities associated with obesity. This study investigates early changes in leptin and perilipin-1 levels following SG and RYGB and their impact on cardiometabolic comorbidities.
Methods:
A total of 60 individuals with severe obesity (body mass index [BMI] >35 kg/m2 with cardiometabolic comorbidities or BMI >40 kg/m2) underwent bariatric and metabolic surgery at a single center. Demographic data, preoperative and postoperative (1st-month) laboratory values (leptin, perilipin-1, hemoglobin A1c [HbA1c], low-density lipoprotein [LDL] cholesterol, triglycerides), and weight loss were recorded. Statistical analyses compared changes between the groups.
Results:
Forty individuals underwent SG, and 20 underwent RYGB. Both SG and RYGB resulted in significant weight loss and improvements in metabolic parameters within the first 30 postoperative days. Perilipin-1, a lipid droplet-coating protein that regulates lipolysis and is implicated in atherosclerotic plaque formation, showed significantly different postoperative trajectories between the two groups. RYGB demonstrated greater reductions in leptin and perilipin-1 levels compared with SG (P = .007 for perilipin-1). LDL cholesterol and HbA1c levels also decreased more significantly in the RYGB group. While SG showed no significant changes in perilipin-1 levels postoperatively, RYGB significantly reduced this marker, suggesting superior efficacy in addressing obesity-related cardiometabolic comorbidities.
Conclusion:
Within the first 30 postoperative days, RYGB produces earlier and more pronounced reductions in key metabolic markers, including leptin, perilipin-1, LDL cholesterol, and HbA1c, compared with SG. These early hormonal differences may help explain the long-term cardiometabolic advantages of RYGB reported in the literature and support prioritizing RYGB in patients with severe obesity with associated metabolic comorbidity components. Further prospective studies with long-term follow-up are warranted.
Introduction
Severe obesity is a complex metabolic condition with an increasing prevalence worldwide and is recognized as a significant risk factor for cardiovascular diseases (CVDs). Excess adipose tissue leads to chronic inflammation, dyslipidemia, and insulin resistance, accelerating the development of atherosclerosis and other obesity complications.1,2 Furthermore, metabolic disorders associated with severe obesity cause alterations in biochemical markers, opening new avenues for research aimed at better assessing cardiovascular risk. In this context, molecules, such as leptin and perilipin 1, hold significant potential in understanding the mechanisms of both severe obesity and cardiovascular complications.2,3
Leptin, an adipokine, plays a central role in regulating energy balance, appetite, and body weight. Under normal physiological conditions, leptin regulates fat stores by increasing energy expenditure and suppressing appetite. 4 However, in individuals with severe obesity, leptin resistance develops, and elevated levels of this hormone may contribute to increased cardiovascular risk through pro-inflammatory effects. Studies have demonstrated that leptin is associated with endothelial dysfunction and oxidative stress, key factors in the development of atherosclerosis. 5
Perilipin 1, on the other hand, is a protein located on the surface of lipid droplets, playing a critical role in regulating lipolytic processes and the metabolic activity of adipose tissue. This protein controls the access of lipolytic enzymes to lipid droplets, thereby influencing energy storage and expenditure. 6 Changes in perilipin 1 levels following bariatric and metabolic surgery have been associated with improvements in lipid metabolism; however, its direct impact on cardiovascular risk factors remains inadequately elucidated. 7
Sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) are the two most commonly performed bariatric and metabolic surgery procedures for the treatment of severe obesity. These procedures not only facilitate weight loss but also trigger metabolic improvements.8,9 The postsurgical changes in leptin and perilipin 1 levels are thought to be linked to hormonal and metabolic effects in addition to weight loss. 15 However, studies comparing the effects of these two surgical methods on leptin and perilipin 1 are limited.10,11
This study aims to investigate the early changes in leptin and perilipin 1 in individuals with severe obesity undergoing two different bariatric and metabolic surgical procedures, SG and RYGB, which may provide valuable insights into their long-term effects on cardiometabolic comorbidities.
Materials and Methods
This study was conducted between February and August 2024 at the General Surgery and Gastroenterology Surgery Clinics of Antalya Training and Research Hospital, involving a total of 60 individuals with severe obesity who underwent bariatric and metabolic surgery. Individuals aged over 18 years with a body mass index (BMI) >35 kg/m2 and associated obesity complications, or a BMI >40 kg/m2, were evaluated for surgery by bariatric and metabolic surgeons with relevant subspecialty training and endocrinologists. At our institution, all patients considered for bariatric surgery undergo a mandatory multidisciplinary assessment that includes an endocrinology consultation, as well as evaluations by a dietitian, psychiatrist or psychologist, and cardiologist when clinically indicated. This evaluation aims to exclude secondary causes of obesity—such as hypothyroidism, Cushing’s syndrome, or polycystic ovarian syndrome—and to optimize glycemic and hormonal management prior to bariatric surgery. The choice of surgical procedure for each individual was determined based on their specific cardiometabolic comorbidity profile, preoperative endoscopic findings, and personal preferences.
Contraindications to SG at our institution included Barrett’s esophagus with dysplasia or severe gastroesophageal reflux disease unresponsive to medical therapy. Contraindications to RYGB included prior complex abdominal surgery that precluded safe bowel anastomosis and patient refusal after informed consent. The final selection between procedures incorporated individual patient anatomy, comorbidity burden, preoperative endoscopic findings, and shared decision-making between the surgical team and the patient. In terms of cardiometabolic comorbidity profile, patients with poorly controlled type 2 diabetes (HbA1c >8% despite two or more antidiabetic medications), severe dyslipidemia refractory to medical therapy, or established CVD were preferentially directed toward RYGB given its superior metabolic efficacy. SG was generally offered to patients without these high-risk metabolic features or when the patient expressed a preference for a less complex procedure after thorough informed discussion. No absolute HbA1c or medication-number threshold was applied rigidly; rather, each case was evaluated holistically within the multidisciplinary team.
Forty individuals who underwent SG were operated on by the General Surgery Department, while 20 individuals planned for RYGB were operated on by the Gastroenterology Surgery Department. The individuals’ demographic data, preoperative laboratory values (hemogram, blood urea nitrogen [BUN], creatinine, glomerular filtration rate [GFR], fasting glucose, HbA1c, total protein, albumin, triglycerides, LDL cholesterol, leptin, and perilipin 1 levels), postoperative 1st-month laboratory values, and weight loss were recorded.
Individuals with a history of previous surgery for severe obesity who were scheduled for revision or modification were excluded. Patients whose laboratory values were unsuitable for evaluation due to inadequate sample quality (e.g., hemolyzed specimens), as repeat sampling was not systematically available within the study protocol window, were also excluded. In addition, patients with significant postoperative complications—including anastomotic leak, prolonged intensive care unit stay (>1 day), or deep vein thrombosis impairing postoperative mobilization—were excluded. These patients were excluded because systemic inflammation, immobility, altered nutritional intake, and medications, such as corticosteroids or anticoagulants, in such cases could independently confound leptin and perilipin-1 measurements, as well as LDL cholesterol and HbA1c levels, which are key secondary outcomes in this study.
The SG procedure was performed under general anesthesia using 5 trocars, with a 36 Fr bougie, starting 4 cm proximal to the pylorus. The RYGB procedure was also performed under general anesthesia using 5 trocars, with a 40 Fr bougie, creating a 5 cm long (approximately 30 mL) pouch. The procedure included a 50 cm biliopancreatic limb and a 150 cm alimentary limb, completed with a 25–30 mm linear gastrojejunostomy anastomosis.
Blood samples for all laboratory analyses, including leptin and perilipin-1, were collected under standardized conditions. Preoperative samples were obtained on the morning of surgery following a minimum 8-hour overnight fast. Postoperative samples were collected at the 1-month follow-up visit (between postoperative days 28 and 35), also under fasting conditions in the morning.
Serum human perilipin-1 (Cat No: E3223Hu) and leptin (Cat No: E1559Hu) levels were measured using a commercially available ELISA kit (Bioassay Technology Laboratory, Zhejiang, China). Five milliliters of venous blood were collected in tubes containing spray-dried clot activator and gel separator and centrifuged at 4000 rpm for 10 minutes. The serum samples were stored at −80°C until analysis. Perilipin-1 and leptin assays had a repeatability %CV <10, with an analytical range of 0.1–40 ng/mL for perilipin-1 and 0.05–10 ng/mL for leptin. Cholesterol tests were measured spectrophotometrically using the AU5800 Beckman Coulter autoanalyzer.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 22 (IBM SPSS, Turkey). The Shapiro–Wilk test was used to assess the normal distribution of parameters. Descriptive statistical methods (mean, standard deviation, frequency) were employed. A one-way ANOVA test was applied to compare normally distributed parameters between groups, and the Tukey HSD test was used for post hoc analysis. The Kruskal–Wallis test was used for non-normally distributed parameters, with Dunn’s test for pairwise comparisons. The Student’s t-test was used for normally distributed two-group comparisons, while the Mann–Whitney U test was used for non-normally distributed parameters. For qualitative data, chi-square, Fisher’s exact, and Fisher–Freeman–Halton tests were applied. The paired t-test was used to evaluate preoperative versus postoperative 1st-month changes. A P value of <0.05 was considered statistically significant.
Results
A total of 60 individuals, with a median age of 38.1 years (range: 18–63 years) and a BMI of 45.7 kg/m2 (range: 37.9–57.4 kg/m2), were included in the study. Among them, 40 individuals who underwent SG were classified as Group 1, and 20 individuals who underwent RYGB were classified as Group 2. The two groups were similar in terms of age and BMI. Gender distribution included 45 females and 15 males, with no statistically significant difference between the groups.
Demographic and preoperative laboratory values for the two groups are summarized in Table 1. Group 1 had a significantly higher preoperative albumin level compared with Group 2 (37.8 versus 36.1, P = .04). Preoperative leptin levels were 3.2 in the SG group and 2.6 in the RYGB group, with no statistically significant difference. Similarly, preoperative perilipin-1 levels were 10.2 and 7.6, respectively, with no statistical difference observed. Other preoperative values were comparable between the two groups.
Demographic Data and Preoperative/Postoperative 1st-Month Laboratory Values
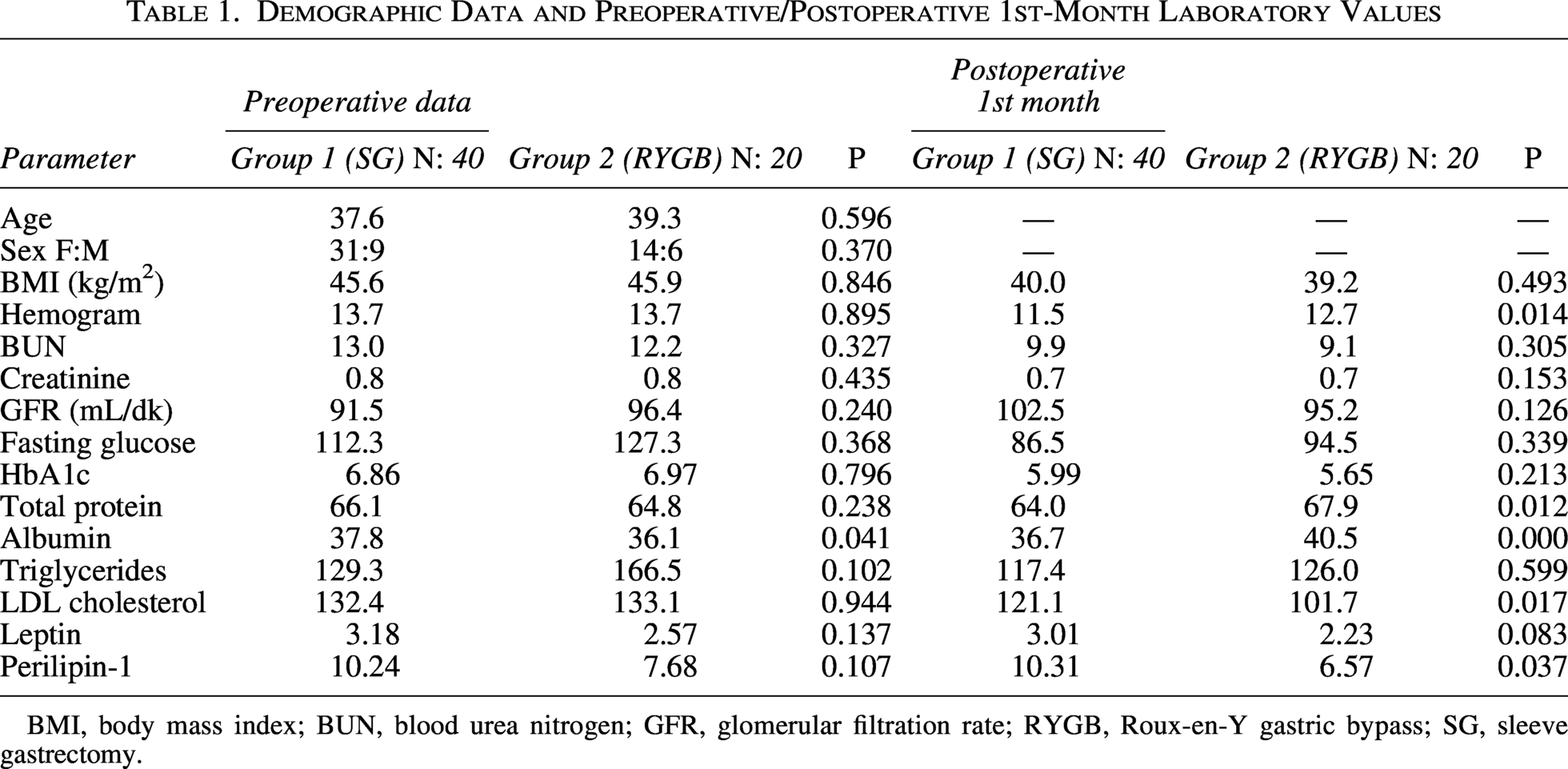
BMI, body mass index; BUN, blood urea nitrogen; GFR, glomerular filtration rate; RYGB, Roux-en-Y gastric bypass; SG, sleeve gastrectomy.
In terms of postoperative 1st-month laboratory values, the RYGB group demonstrated higher hemogram, total protein, and albumin levels compared with the SG group, while the LDL cholesterol level was lower (Table 1). Postoperative 1st-month leptin levels were 3.01 in the SG group and 2.23 in the RYGB group, with no statistically significant difference. However, postoperative 1st-month perilipin-1 levels were 10.3 and 6.6, respectively, with the difference being statistically significant (P = .037).
When comparing preoperative and postoperative 1st-month values for all individuals, a decrease was observed in BUN, creatinine, hemogram, triglycerides, LDL cholesterol, perilipin-1, and leptin levels, while increases were noted in albumin, total protein, and GFR. The BMI decreased from 45.7 to 39.8 kg/m2 overall; from 45.6 to 40.0 kg/m2 in the SG group, and from 45.9 to 39.2 kg/m2 in the RYGB group.
In the SG group, the decrease in leptin levels (3.18 versus 3.01; P = .242) and the change in perilipin-1 levels (10.2 versus 10.3; P = .878) were not statistically significant. In the RYGB group, both the decrease in leptin levels (2.57 versus 2.23; P = .00) and the decrease in perilipin-1 levels (7.69 versus 6.57; P = .007) were statistically significant. The differences between preoperative and postoperative laboratory values are presented in Table 2.
Evaluation of the Differences Between Preoperative and Postoperative 1st-Month Values
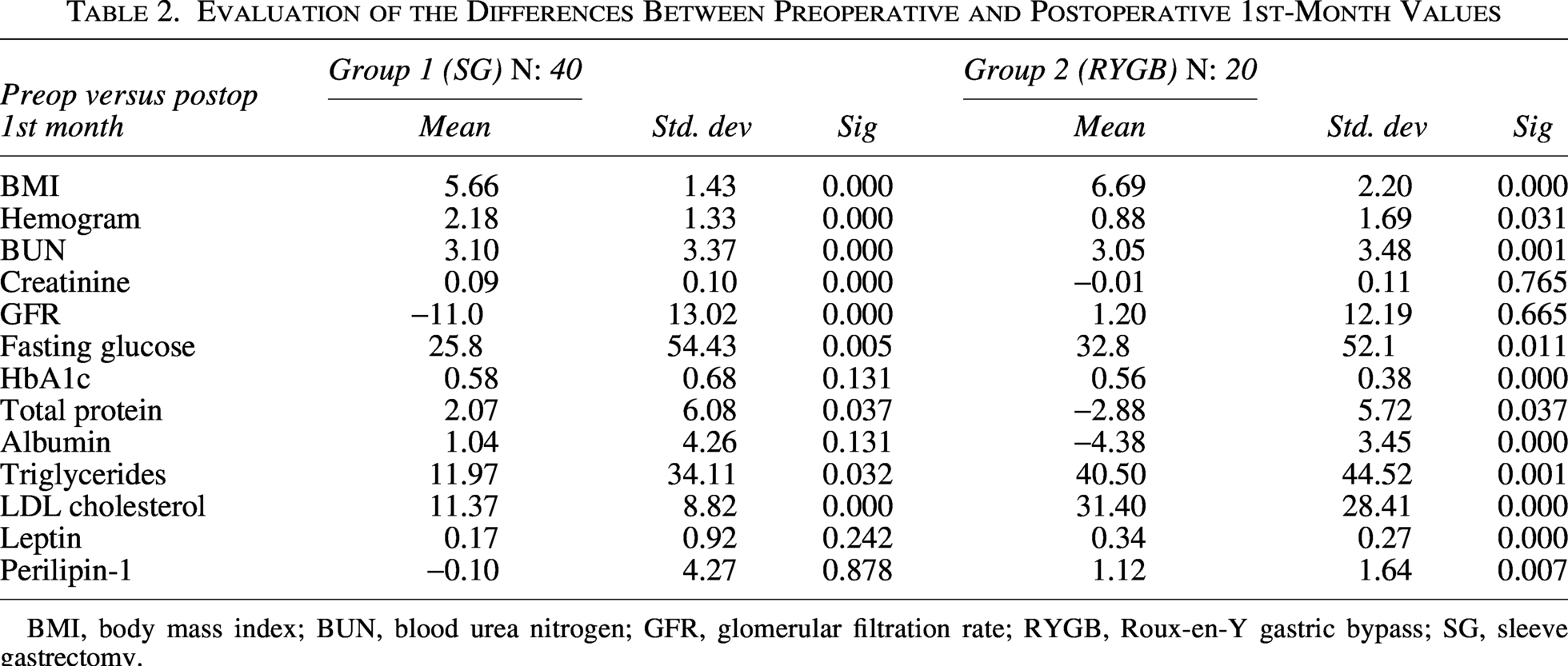
BMI, body mass index; BUN, blood urea nitrogen; GFR, glomerular filtration rate; RYGB, Roux-en-Y gastric bypass; SG, sleeve gastrectomy.
Discussion
While one of the primary goals of bariatric and metabolic surgery is to improve the social lives of individuals, its metabolic effects should not be overlooked. 12 In individuals with severe obesity, the cardiac complications associated with metabolic syndrome significantly reduce life expectancy.12–14 Both SG and RYGB are well-established, effective bariatric procedures that improve cardiometabolic comorbidities associated with obesity. The present study examines whether differences in adipokine levels—specifically leptin and perilipin-1—emerge as early as the first postoperative month and whether these early hormonal differences may provide a mechanistic basis for the divergent long-term metabolic trajectories reported in the literature, potentially persisting and amplifying over time to explain the more durable cardiometabolic benefits associated with RYGB. SG is an effective restrictive surgical procedure that leads to rapid weight loss and is the most commonly performed bariatric and metabolic surgery worldwide.16,17 However, RYGB is less frequently chosen due to its technical complexity and associated risks. 18 Nevertheless, RYGB not only results in significant weight loss but also improves metabolic outcomes, contributing to an increase in healthy life expectancy.
These observations are based on data collected within the first 30 days following surgery. When comparing preoperative and postoperative levels of leptin and perilipin-1 in individuals undergoing RYGB and SG procedures, we observed that RYGB had a more pronounced effect on reducing leptin, perilipin-1, HbA1c, and LDL cholesterol levels than SG. Both SG and RYGB procedures were effective in reducing body weight and triglyceride levels, particularly in individuals with diabetes. However, RYGB demonstrated a more significant reduction in metabolic syndrome parameters such as LDL cholesterol and HbA1c levels. Consistently, RYGB led to a statistically significant reduction in leptin and perilipin-1 levels, aligning with improvements in parameters associated with cardiometabolic comorbidities. These findings suggest that RYGB may be the preferred procedure for individuals with cardiometabolic comorbidities such as prediabetes, diabetes, or hypertension, as it offers superior early metabolic benefits compared with SG.
There is a well-established correlation between leptin and CVD risk. Leptin influences blood pressure, platelet aggregation, and inflammatory vascular responses, contributing to cardiovascular complications.19,20 The primary mechanism of RYGB, which involves augmentation of glucagon-like peptide-1 levels and early improvement in insulin resistance, addresses this complex physiology.21–23 Although statistically significant leptin reduction was observed only in the RYGB group at 30 days (P = .00 versus P = .242 for SG), these early differences align with long-term findings from larger studies demonstrating greater and more durable comorbidity resolution with RYGB compared with SG over 1–5 years.25,26 The early hormonal differences we document may therefore reflect mechanistic distinctions that underlie the divergent long-term metabolic trajectories reported in the literature. Moreover, independent of severe obesity, some studies have identified leptin as a predictor of myocardial infarction, coronary events, and stroke.3,24,27,28
Perilipin-1 warrants particular attention given its central role in adipose tissue biology. As a lipid droplet surface protein, perilipin-1 acts as a gatekeeper regulating lipolytic enzyme access, thereby controlling both energy storage and expenditure. 6 Beyond its metabolic function, perilipin-1 has been implicated in atherosclerotic plaque formation and instability through its role in foam cell development within the arterial wall. 29 Studies have associated PLIN1 gene variants and circulating perilipin-1 levels with early coronary syndrome risk.30,31
In the present study, RYGB led to a statistically significant reduction in postoperative perilipin-1 levels at one month (7.69 versus 6.57; P = .007), whereas SG showed no significant change (10.2 versus 10.3; P = .878). This differential response is clinically meaningful: the simultaneous reduction in perilipin-1 and LDL cholesterol with RYGB (P = .017 between groups) suggests a coordinated improvement in lipid metabolism and adipose tissue remodeling that may confer early protection against atherosclerotic progression. These perilipin-1 reductions, alongside improved HbA1c, further support RYGB’s broader impact on cardiometabolic risk beyond weight loss alone.
BMI is a recognized contributor to insulin resistance, which can lead to type 2 DM.32,33 In our preoperative evaluation, there was no statistically significant difference in HbA1c levels between the two groups (P = .796). However, at the 1-month follow-up, RYGB resulted in a statistically significant reduction in HbA1c levels compared with preoperative values (P = .000), while the SG group showed no such reduction (P = .131). Similarly, while there was no preoperative difference in perilipin-1 levels between the groups (P = .107), postoperative perilipin-1 levels decreased significantly in the RYGB group (P = .037). When comparing preoperative and postoperative values, SG showed no significant change in perilipin-1 levels (P = .878), whereas RYGB demonstrated a statistically significant reduction (P = .007). These differences highlight the superior efficacy of RYGB in addressing insulin resistance and metabolic complications compared with SG within the first postoperative month. Regarding lipid metabolism, RYGB showed a statistically significant advantage in lowering LDL cholesterol compared with SG (P = .017). Lowering LDL cholesterol is critical for reducing the cardiovascular complications of atherosclerosis, as highlighted in studies by Guijarro et al. 34 Consistent with our findings, Wu et al. also demonstrated a correlation between LDL cholesterol and type 2 DM, suggesting that lowering LDL cholesterol reduces DM risk. 35
Limitations and future directions
Several limitations of this study should be acknowledged. First, the sample size is relatively small, particularly in the RYGB group (n = 20), which may limit statistical power and generalizability. Second, the single-center design and nonrandomized allocation of surgical procedure introduce potential selection bias. Third, the follow-up period of 30 days is short; hormonal changes observed at this time point may not reflect longer term trends. Fourth, patients who experienced significant postoperative complications were excluded to minimize confounding, which may have introduced survivor bias. Fifth, data on postoperative dietary intake and physical activity were not collected, both of which can independently influence leptin and perilipin-1 levels. Sixth, repeat blood sampling was not systematically available for patients with inadequate preoperative specimens.
Future studies should include prospective, randomized designs with larger cohorts and extended follow-up intervals (6, 12, and 24 months) to track the evolution of these biomarkers and their relationship to clinical outcomes such as type 2 diabetes remission, hypertension resolution, and major adverse cardiovascular events. Expanding the biomarker panel to include additional adipokines (e.g., adiponectin, resistin) and inflammatory markers (e.g., CRP, IL-6) would further elucidate the metabolic mechanisms differentiating SG and RYGB.
Conclusion
Within the first 30 postoperative days, RYGB produces earlier and statistically greater reductions in leptin, perilipin-1, LDL cholesterol, and HbA1c compared with SG. These early hormonal differences may reflect distinct mechanistic pathways activated by each procedure and may help explain the more durable cardiometabolic comorbidity resolution associated with RYGB in long-term literature. Clinicians managing patients with severe obesity and significant cardiometabolic comorbidities such as type 2 diabetes, hypertension, or dyslipidemia should consider these early biomarker differences when selecting between bariatric procedures. Further prospective randomized trials with extended follow-up are warranted to confirm these findings and to determine the long-term clinical significance of early perilipin-1 and leptin changes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.