
Abstract
Background:
The clinical significance of residual gallstones (RGSs) in the gallbladder neck–cystic duct after cholecystectomy for acute cholecystitis (AC) remains unclear. This study aimed to evaluate the association between RGSs and postoperative outcomes, including the development of common bile duct stones (CBDSs) in AC.
Materials and Methods:
We retrospectively analyzed 272 consecutive patients who underwent cholecystectomy for AC at our institution between April 2016 and December 2025. RGSs in the gallbladder neck–cystic duct were identified based on imaging findings and surgical records. The postoperative outcomes and their associated risk factors were evaluated.
Results:
RGSs after surgery were identified in 24 (8.8%) of 272 patients. Postoperative complications, length of hospital stay, and the incidence of remnant cholecystitis did not differ significantly between the RGS-positive and -negative groups. Postoperative CBDSs occurred significantly more frequently in the RGS-positive group than the RGS-negative group (37.5% versus 3.2%, P < .001). Multivariate analysis identified RGS positivity as the only independent risk factor for CBDS after cholecystectomy (P < .001). All symptomatic CBDSs occurred within 6 months after surgery. Among patients with RGSs, stone location and volume showed limited predictive performance for CBDS. All postoperative CBDSs were successfully treated endoscopically, and no patient required reoperation.
Conclusions:
RGSs in the gallbladder neck–cystic duct are associated with an increased risk of postoperative CBDS in patients with AC. When feasible, intraoperative stone removal should be considered; however, postoperative endoscopic management represents an effective alternative when stone removal is technically challenging.
Introduction
Acute cholecystitis (AC) is one of the most common abdominal emergencies worldwide, developing in approximately 200,000 people in the United States each year.1–3 The Tokyo Guideline 2018 (TG18) has established evidence-based treatment strategies for AC and provides systematic guideposts for physicians and patients worldwide. 4 However, in actual clinical practice for AC, patient backgrounds and local inflammatory findings in the gallbladder vary considerably, resulting in treatment decisions that can often be challenging even when these informative guidelines are followed. Although laparoscopic cholecystectomy (LC) has become the standard treatment for AC, the surgical approach encompasses a remarkably broad spectrum of technical difficulties.3–6 In difficult surgical cases, particularly those with severe fibrosis and scarring in the Calot’s triangle, avoidance of bile duct injury (BDI) is undoubtedly one of the highest priorities. 6 TG18 has recommended the selection of a bailout procedure and subtotal cholecystectomy if, when the Calot’s triangle is appropriately retracted and used as a landmark, a critical view of safety (CVS) cannot be achieved. 6 However, particularly when bailout procedures, such as subtotal cholecystectomy, are selected, it is sometimes difficult to avoid residual gallstones (RGSs) in the gallbladder neck–cystic duct. Previous systematic reviews of long-term outcomes after subtotal cholecystectomy have reported an incidence of common bile duct stones (CBDSs) of approximately 13% and remnant cholecystitis of 3%–11%.7–9 However, no detailed investigations have examined differences in clinical outcomes based on the presence or absence of RGSs. Furthermore, in surgically difficult cases with cystic duct stones adjacent to the common bile duct, the necessity and appropriateness of the risky surgical removal of the stones remain a common real-world clinical question. These ambiguities indicate that the specific clinical significance and long-term outcomes of RGSs in the gallbladder neck–cystic duct—particularly the frequency of clinical events requiring intervention—remain insufficiently characterized.
Based on these surgical dilemmas concerning difficult gallstones, the present study aimed to evaluate the clinical significance of RGSs in the gallbladder neck–cystic duct after cholecystectomy for AC and to investigate their association with postoperative outcomes.
Materials and Methods
Study design and patient selection
We retrospectively reviewed the records of consecutive patients with AC who underwent cholecystectomy at Minami-Nara General Medical Center between April 2016 and December 2025. In this study, stones located in the gallbladder neck and/or cystic duct remnant after surgery were collectively defined as RGS. For all patients, two or more surgeons and radiologists classified RGS status based on a combination of pre- and postoperative imaging studies, including computed tomography (CT), magnetic resonance imaging, and surgical reports.
Clinical data and patient management
The diagnosis, definition, and severity of AC were defined using TG18.4,10 Patient clinical data, including the age-adjusted Charlson comorbidity index (aCCI) and American Society of Anesthesiologists physical status (ASA-PS), were retrospectively reviewed and collected from our database.6,10–13 Previous endoscopic papillary procedures included endoscopic retrograde biliary drainage and sphincterotomy. All patients with AC received intravenous antibiotics, general supportive care, general organ support, and appropriate intravenous fluid administration as initial treatment. Surgeons, gastroenterologists, emergency physicians, and interventional radiologists discussed and determined treatment strategies, including emergency surgery and percutaneous cholecystostomy. Urgent surgery was defined as surgery performed within 48 hours of diagnosis. The CVS was evaluated according to TG18. 6 Postoperative CBDSs were defined as CBDSs detected after cholecystectomy during follow-up imaging or endoscopic evaluation. This study was approved by the Local Ethics Committee on Clinical Investigation of Minami-Nara General Medical Center (approval number: 26) and was conducted in accordance with the Declaration of Helsinki.
Surgical procedures
Open cholecystectomy was selected in patients with a history of multiple prior upper abdominal surgeries and significant adhesions, whereas LC was performed in all remaining patients. LC for AC was performed using a four-port technique as the standard surgical approach, with an additional port placed in difficult cases when necessary. At least one experienced laparoscopic surgeon participated in all the operations. At our institution, intraoperative cholangiography (IOC) and ultrasound are not performed routinely. When the CVS could not be achieved due to severe fibrosis and scarring in the Calot’s triangle, a bailout procedure was selected based on TG18. 6 In cases with cystic duct stones, we attempt stone removal by dividing the cystic duct as distally as possible, guided by the location of the stones on preoperative imaging, provided that procedural safety can be ensured. Before dividing the cystic duct, the presence of stones is assessed by palpation using grasping forceps. When the attending surgeons judged the case to be high-risk of BDI due to fibrosis and scarring around the cystic duct, the stones were left in situ. The criteria for conversion to open cholecystectomy were as follows: (1) uncontrolled persistent bleeding; (2) disorientation of anatomical landmarks; and (3) inability to secure a safe surgical view due to unresolvable adhesions of the colon, duodenum, and stomach.
Statistical analysis
Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate, depending on the expected cell counts. For continuous variables, the Mann–Whitney U test was performed to compare differences between the two groups, given the non-normal distribution of the data. Univariate and multivariate logistic regression analyses were performed to identify the risk factors for postoperative CBDSs in AC using clinicopathological variables, including age, sex, aCCI, ASA-PS, previous endoscopic papillary procedures, marked local inflammation, severity grade, white blood cell count, platelet count, serum C-reactive protein, total bilirubin, albumin, creatinine, percutaneous cholecystostomy, urgent surgery, operation time, estimated blood loss, surgical procedure, CVS, subtotal cholecystectomy, and RGS status. The volume (V) of RGS was estimated from (a) short diameter, (b) long diameter in the axial CT slice, and (c) long diameter in the coronal CT slice using the following formula: V = (4/3)π(abc/8). The resulting RGS volumes were used to determine the area under the curve (AUC) values for each of the receiver operating characteristic plots that were evaluated using MedCalc statistical software V.19.8 (MedCalc Software bvba, Ostend, Belgium).14–17 We estimated the cumulative risk of the clinical events caused by RGSs using the Kaplan–Meier method and analyzed the primary endpoint using a stratified log-rank test. 18 Hazard ratios and their corresponding confidence intervals (CIs) were estimated using a Cox proportional hazards model. Median follow-up times were calculated using the reverse Kaplan–Meier method. 19 A P value <0.05 was considered statistically significant. Statistical analyses were performed using MedCalc statistical software V.19.8, and GraphPad Prism V8.0 (GraphPad Software, San Diego, CA, USA).14,15,17
Results
Patient characteristics and RGS status
The entire patient cohort evaluated in this study is shown in Figure 1. We retrospectively reviewed data from 290 patients who underwent surgical treatment for AC at Minami-Nara General Medical Center between April 2016 and December 2025. Of the 290 patients, we excluded 18 patients with common bile duct obstruction due to 16 stones or 2 pancreatic cancers. Consequently, 272 eligible patients with AC were enrolled and analyzed in this study (Table 1 and Fig. 1). The median follow-up time after surgery in all patients was 30 months. Based on the imaging tests and surgical reports, postoperative RGSs in the gallbladder neck–cystic duct were identified in 24 (8.8%) of the 272 patients (Table 1 and Fig. 2a). Patients in the RGS-positive group had significantly longer operative times and higher rates of conversion to open surgery and subtotal cholecystectomy, suggesting greater surgical difficulty in this group (Table 1). Among the patients who underwent subtotal cholecystectomy, two required postoperative interventional radiological drainage for bile leakage from the gallbladder stump; however, no BDI occurred in all patients. There is no significant difference between the RGS-positive and -negative groups in postoperative length of hospital stay (Table 1).
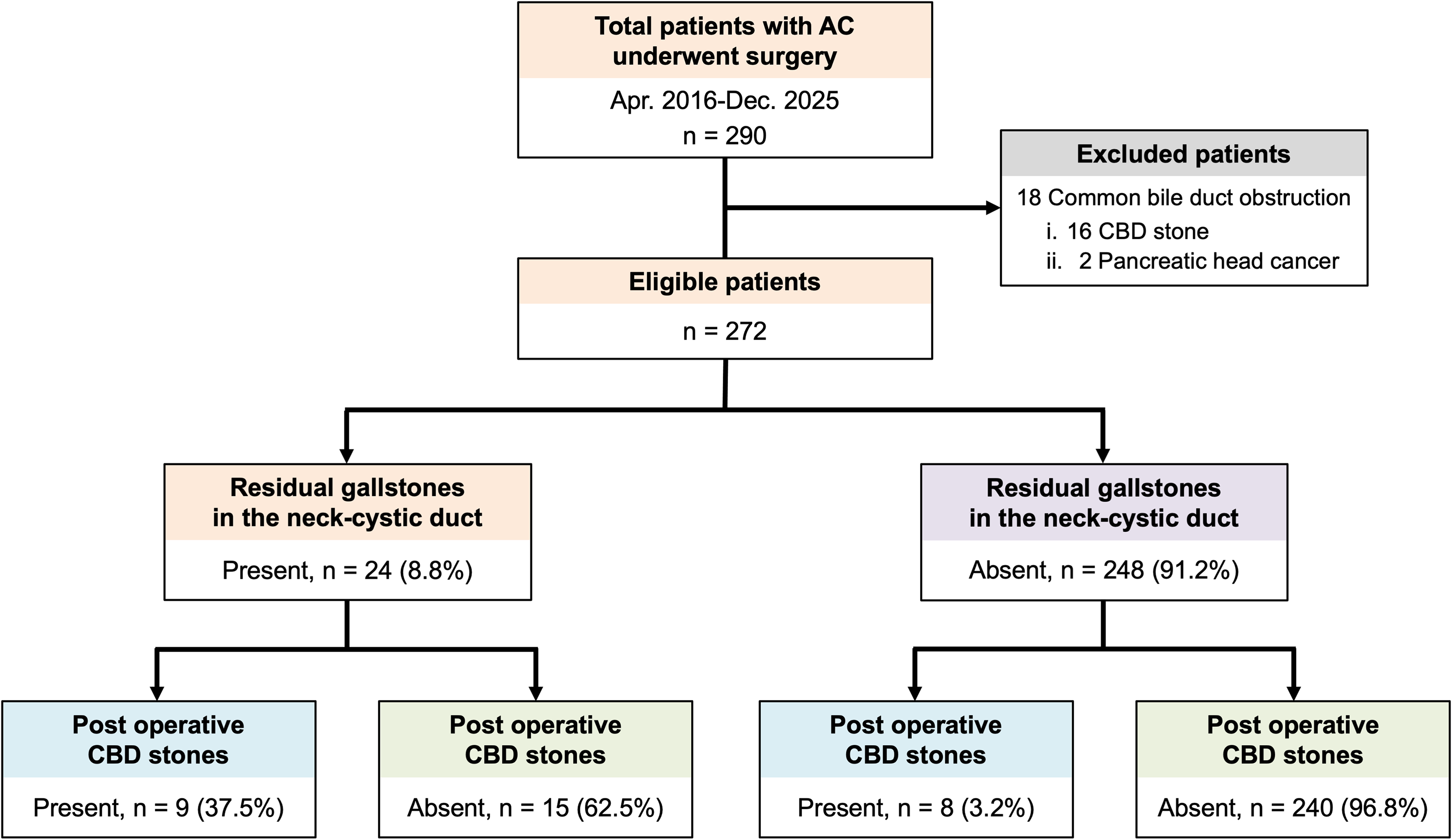
Overview of the patient cohort.
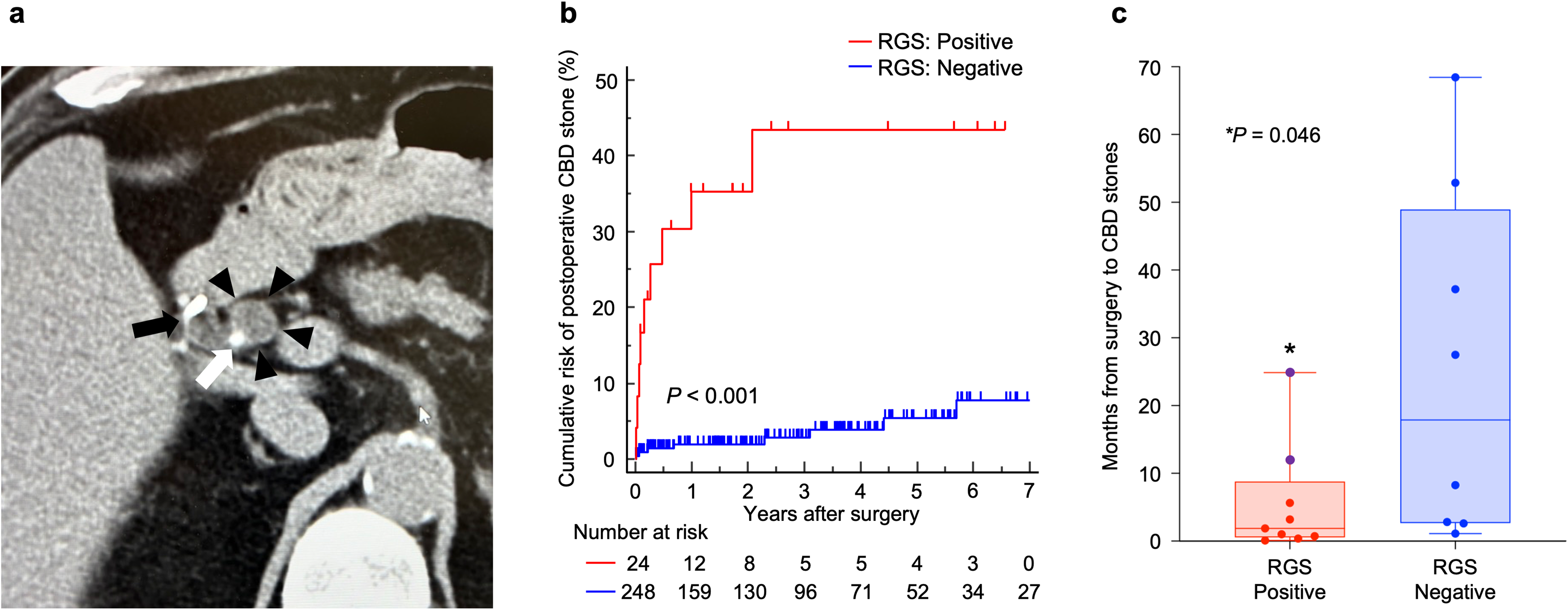
Association between residual gallstones (RGSs) after cholecystectomy and postoperative common bile duct stones (CBDSs).
Patient Characteristics
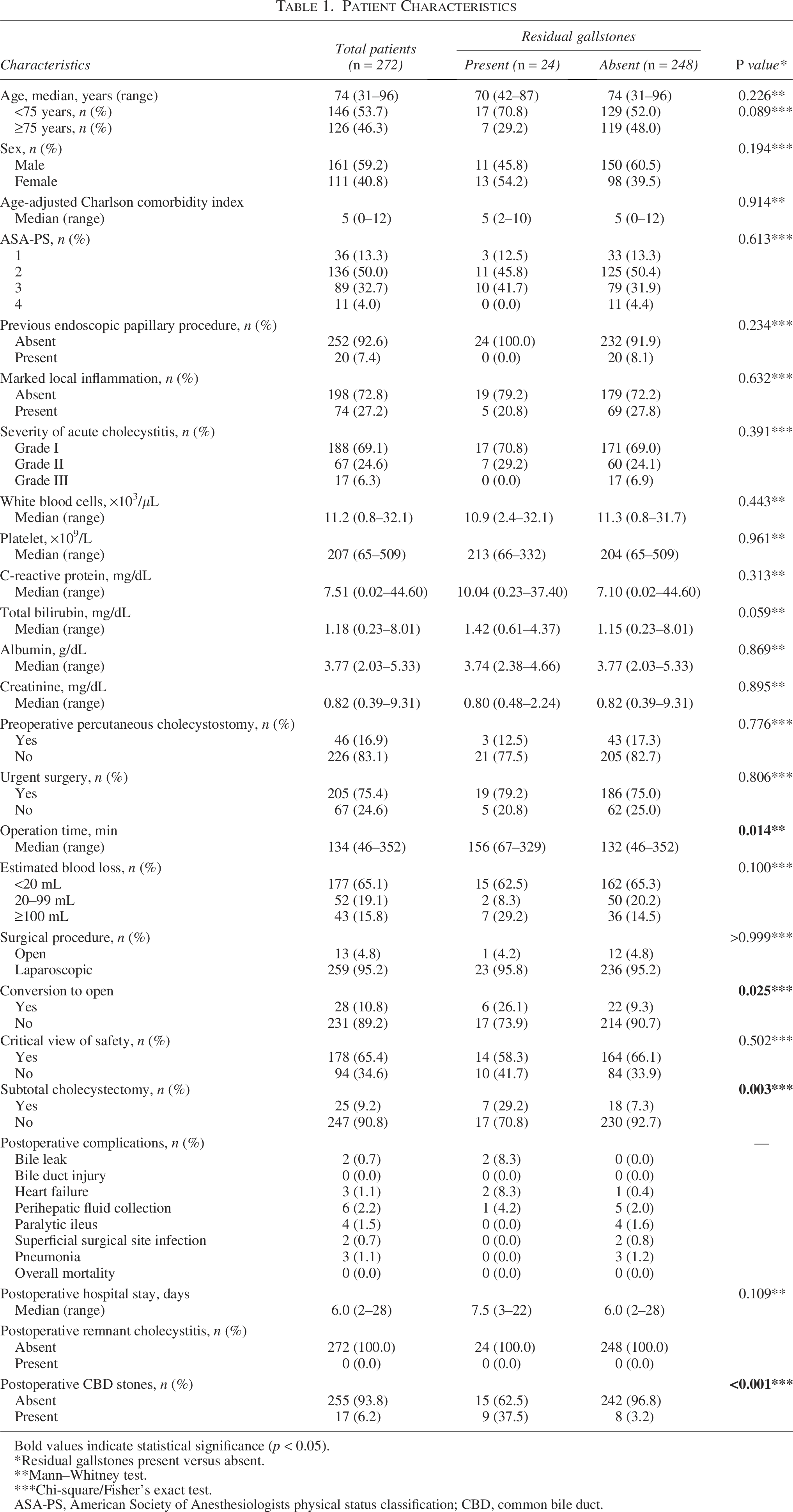
Bold values indicate statistical significance (p < 0.05).
*Residual gallstones present versus absent.
**Mann–Whitney test.
***Chi-square/Fisher’s exact test.
ASA-PS, American Society of Anesthesiologists physical status classification; CBD, common bile duct.
Regarding long-term outcomes after cholecystectomy, no cases of remnant cholecystitis were observed during follow-up in both groups. Importantly, the incidence of postoperative CBDSs was significantly higher in the RGS-positive group than in the negative group (37.5% versus 3.2%, P < .001; Table 1). Based on imaging findings at the time of CBDS onset, migration of RGSs into the CBD was confirmed in all patients in the RGS-positive group. RGS-positive patients exhibited a significantly higher cumulative risk of postoperative CBDSs than RGS-negative patients (P < .001; Fig. 2b). In addition, CBDSs developed significantly earlier after surgery in the RGS-positive group (RGS-positive/negative, median: 1.9 months [range: 0.2–24.9]/17.9 [range: 0.8–68.4], P = .046; Fig. 2c). Interestingly, except for two incidentally detected asymptomatic CBDS cases, all CBDSs developed within 6 months after surgery in the RGS-positive group (Fig. 2c).
Multivariate analysis for postoperative CBDSs after cholecystectomy in patients with AC
Next, we conducted univariate and multivariate logistic regression analyses to identify predictors of postoperative CBDS, including preoperative clinicopathological variables and RGS status (Supplementary Table S1). Univariate analysis revealed that long operation time, failure to achieve CVS, subtotal cholecystectomy, and RGS-positive were significantly correlated with postoperative CBDS (Table 2). In multivariate analysis, RGS-positive patients emerged as the only independent risk factor for postoperative CBDS in patients with AC (odds ratio = 17.577; 95% CI = 5.201–59.401; P < .001; Table 2). These results highlight the clinical impact of RGS in the gallbladder neck–cystic duct on postoperative outcomes in patients with AC.
Logistic Regression Analysis for Postoperative Common Bile Duct Stones in Acute Cholecystitis

Bold values indicate statistical significance (p < 0.05).
aCCI, age-adjusted Charlson comorbidity index; ASA-PS, American Society of Anesthesiologists physical status classification; CI, confidence interval; OR, odds ratio.
Subgroup analysis of RGSs
Subsequently, to stratify the risk of postoperative CBDS in the RGS-positive group, we conducted a subgroup analysis of patients with RGS after surgery (Table 3). No significant differences were observed between the two groups in any clinical factors when classified based on the presence or absence of postoperative CBDS. No clinical factors were significantly associated with the development of CBDSs in patients with RGS (Table 3). Next, we hypothesized that the frequency of stone migration into the CBD may vary according to the location and size of RGSs and conducted an exploratory analysis. The size of the RGSs was measured using multidirectional CT images, and their association with the development of CBDS was analyzed. RGSs were located in the gallbladder neck in four cases (16.7%) and in the cystic duct in 20 cases (83.3%). Postoperative CBDSs developed in one case (25.0%) and eight cases (40.0%), respectively, with no statistically significant difference between the two locations (Table 3 and Fig. 3a). Larger stones tended to migrate into the CBD less frequently (cutoff value: 53.3 mm3, sensitivity: 88.89%); however, stone size did not demonstrate significant predictive value for the development of postoperative CBDS (AUC = 0.59; Fig. 3b and c). Taken together, these findings suggest that stone migration is difficult to predict in patients with RGS. Management of CBDSs consisted of endoscopic stone removal in seven patients. Of the remaining two patients, one experienced spontaneous stone passage into the duodenum during treatment planning, while the other was not considered a candidate for endoscopic intervention due to poor general condition. Endoscopic treatment was successful in all seven patients, with no cases requiring reoperation.
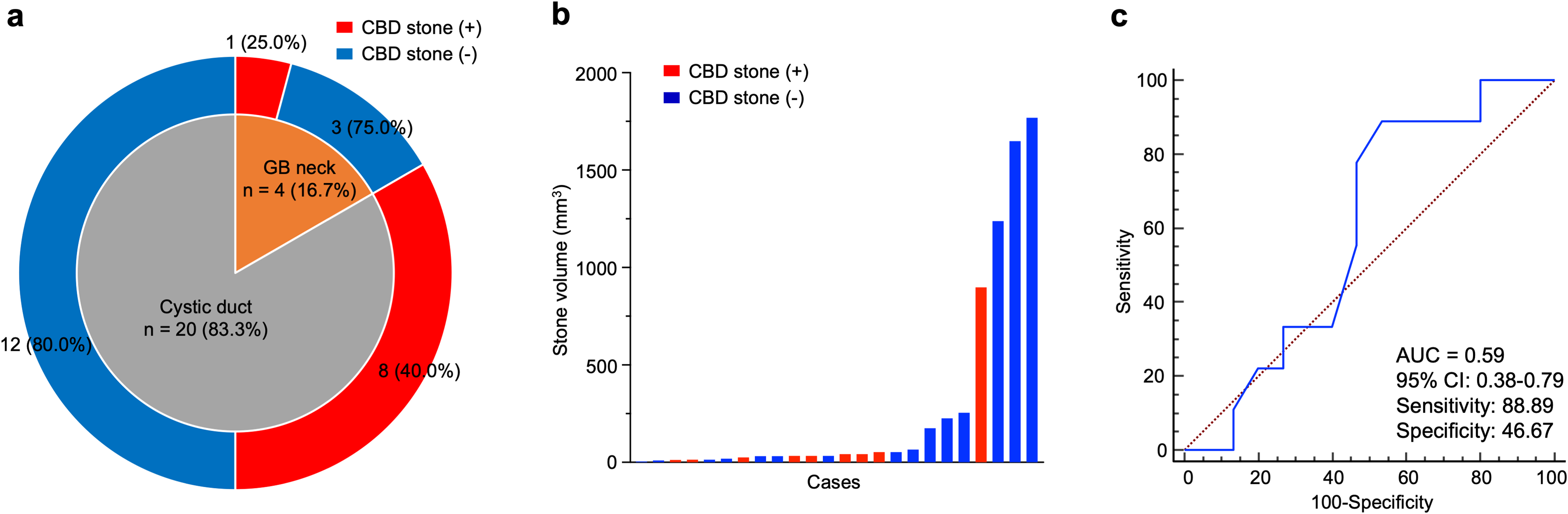
Exploratory subgroup analysis of residual gallstones (RGSs).
The Characteristics of Patients with Residual Gallstones
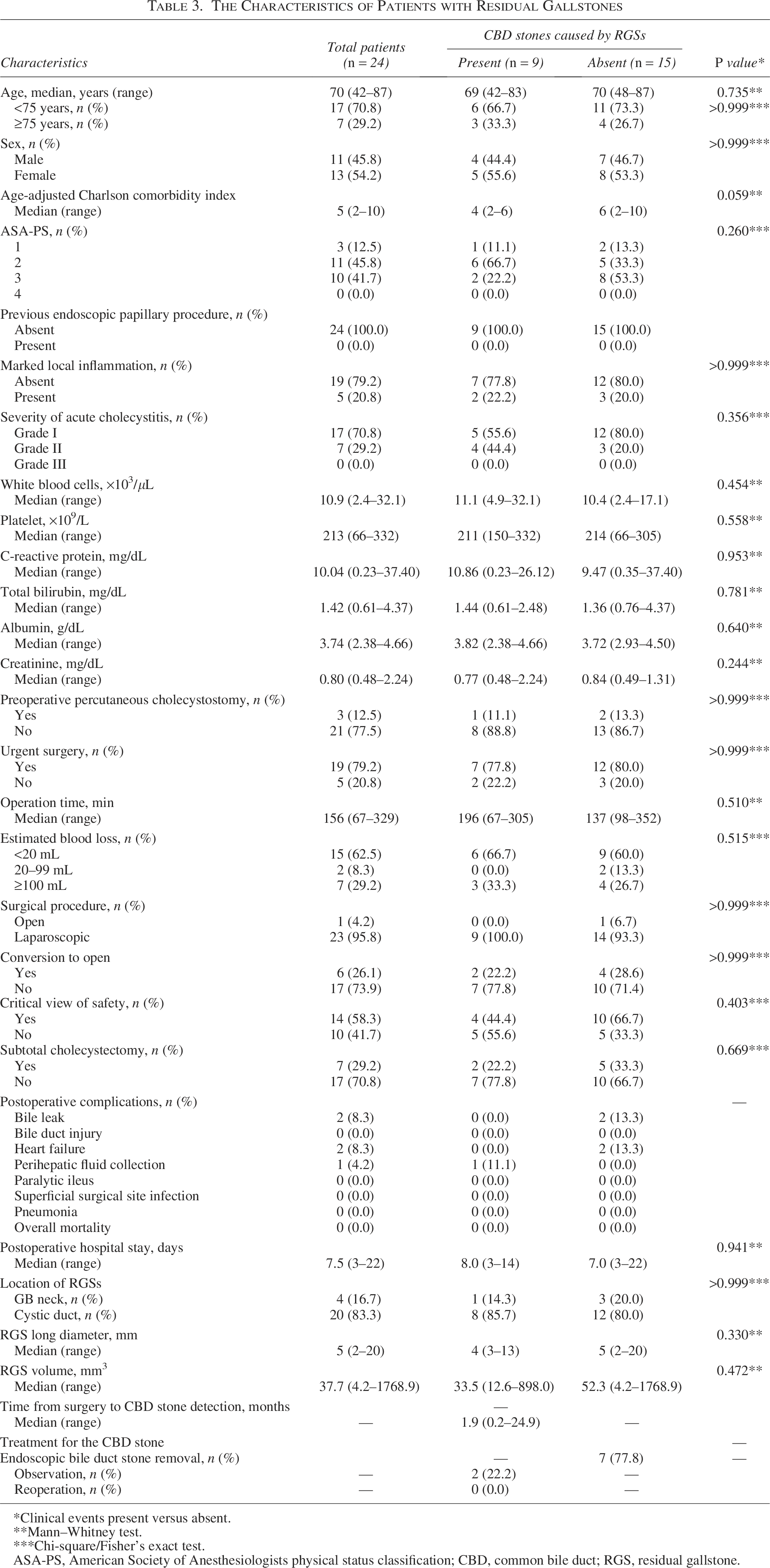
*Clinical events present versus absent.
**Mann–Whitney test.
***Chi-square/Fisher’s exact test.
ASA-PS, American Society of Anesthesiologists physical status classification; CBD, common bile duct; RGS, residual gallstone.
Discussion
AC is a common disease encountered in daily clinical practice and is characterized by substantial heterogeneity in patient background, disease severity, and stone characteristics. Clinical presentations range from mild inflammation to severe cases requiring urgent intervention, often necessitating individualized treatment strategies. The TG18 provides widely accepted recommendations for the diagnosis and management of AC.4,6,10,20 However, complex or “special” situations are frequently encountered in real-world clinical practice, and flexible decision-making is often required. This study focused on RGS in the gallbladder neck–cystic duct, which are relatively common in clinical practice; however, their clinical significance remains controversial. 21 In this cohort, RGSs were identified in 8.8% of patients, and postoperative CBDSs caused by migration of these residual stones developed in 37.5% of these cases. These findings suggest that RGSs in the gallbladder neck–cystic duct may have clinically important implications and should not be overlooked during surgical management of AC.
Previous studies have reported that the presence of cystic duct stones on preoperative imaging is associated with an increased risk of postoperative CBDSs.22–24 However, these studies did not clarify whether the cystic duct stones were successfully removed during surgery or remained as residual stones, which limits the applicability of this evidence to actual clinical practice. In contrast, the strength of our study lies in the direct evaluation of RGSs after surgery and the assessment of their subsequent clinical outcomes, yielding findings more closely aligned with real-world clinical questions. Notably, none of the patients in whom cystic duct stones were successfully removed intraoperatively developed postoperative CBDSs in our cohort (Supplementary Table S1). These findings suggest that residual stones, rather than the mere presence of preoperative cystic duct stones, may play a key role in the development of postoperative CBDSs.
Although RGSs may have clinical significance, all cases of CBDSs resulting from RGSs in this study were successfully managed with endoscopic intervention, and no patients required reoperation. Moreover, no severe postoperative complications, including BDI, were observed. These findings suggest that intraoperative stone removal should be attempted whenever it can be performed safely. However, when stone removal is technically difficult or potentially hazardous, treatment strategies may be planned with consideration of possible postoperative endoscopic management. This approach can be interpreted as an acceptable trade-off to prioritize surgical safety and avoid BDI and may facilitate surgeons in balancing intraoperative safety with postoperative management in patients with AC. However, severe cholangitis due to CBDSs can lead to a systemic, life-threatening infection in patients with high-risk comorbidities. With recent advances in endoscopic techniques, endoscopic stone removal has increasingly been performed even in challenging cases such as cystic duct stones. However, since endoscopic stone removal is an invasive procedure, the indication for prophylactic stone removal in asymptomatic RGSs remains controversial. At our institution, patients are carefully informed after surgery about the potential risk of subsequent CBDS development, and prophylactic stone extraction is not routinely performed. Further investigation is warranted to clarify the role and validity of prophylactic endoscopic treatment for RGSs.
On the other hand, this study was unable to stratify the risk of postoperative stone migration among RGS-positive patients. In this study, we hypothesized that the physical size of the residual stone might be associated with the risk of migration into the CBD. In the present analysis, only one migration event occurred among patients with a stone volume greater than 52.3 mm3 (sensitivity: 88.9%), suggesting that larger stones may be less likely to migrate into the CBD. However, the specificity and AUC value were low (specificity: 46.7%; AUC: 0.59), indicating that RGS volume had limited predictive performance for postoperative CBDS development. Given the relatively small number of RGS-positive cases in this study, further investigations using large multicenter datasets are warranted to identify reliable risk factors for postoperative CBDSs and to re-evaluate the clinical significance of stone size. Since predicting stone migration remains clinically challenging, careful postoperative surveillance may be warranted in patients with RGSs. In this study, all symptomatic CBDSs in the RGS-positive group occurred within 6 months after surgery. This finding may provide useful information for establishing appropriate postoperative surveillance strategies.
Although our results provide useful insights into the actual clinical practice for AC, we acknowledge a few potential limitations to our present study. First, this was a retrospective single-institution study, which may introduce potential selection bias related to surgical strategies and region-specific patient demographics. Second, in this study, only cases in which RGSs were clearly identified on imaging studies were defined as RGS-positive; therefore, small stones may have been overlooked. Consequently, the incidence of residual stones may have been underestimated. In addition, preexisting CBDSs may have been overlooked before surgery. In the RGS-negative group, three of eight patients (37.5%) developed CBDSs early after surgery, suggesting that stones may have already been present in the bile duct or cystic duct in these cases. Although it is difficult to eliminate this potential statistical bias completely, routine IOC—which were not routinely performed at our institution—might facilitate the reduction of this limitation. Although IOC can be technically challenging, particularly in difficult cholecystectomy cases, it is useful for identifying cystic duct stones. Therefore, it may be considered a standard procedure, especially in patients with suspected cystic duct stones. To minimize these biases associated with the limitations of imaging studies, preoperative imaging was retrospectively reviewed by a multidisciplinary team, including radiologists, surgeons, and gastroenterologists, in our study. Importantly, the overall incidence of postoperative CBDSs in our cohort was 17 (6.3%) of 272, which is not higher than that reported in previous studies, 7 suggesting that our preoperative imaging assessment was within an acceptable standard, despite its limitations. Finally, given the relatively small sample size and number of events, the statistical models—including multivariable analyses—may be unstable and prone to overfitting. Accordingly, these analyses should be considered exploratory, and the magnitude of the estimated effect sizes should be interpreted with caution. Prospective multicenter studies with larger cohorts are warranted to validate our findings. Nonetheless, our present study provides additional insight into the clinical significance of RGS in predicting postoperative CBDSs in patients with AC, which is one of the most common diseases worldwide.
Conclusion
RGS in the gallbladder neck–cystic duct was associated with an increased risk of postoperative CBDSs in patients undergoing cholecystectomy for AC. When feasible, intraoperative stone removal should be considered; however, postoperative endoscopic management represents an effective and reasonable alternative when stone removal is technically challenging.
Authors’ Contributions
S.N.: Conceptualization, methodology, data curation, visualization, analysis, writing—original draft and editing, and surgical procedure. Tetsuya.T.: Conceptualization, methodology, data curation, analysis, writing—review and editing, supervision, validation, and surgical procedure. T.H.: Conceptualization, methodology, supervision, writing—review and editing, and radiological procedure. Y.K.: Data curation and surgical procedure. Takeshi.T.: Data curation and surgical procedure. T.S.: Data curation and surgical procedure. H.N.: Data curation and surgical procedure. M.K.: Data curation and radiological procedure. K.H.: Data curation and gastroenterological procedure. Y.T.: Data curation and gastroenterological procedure. K.M.: Data curation and gastroenterological procedure. J.S.: Data curation and gastroenterological procedure. H.H.: Data curation and gastroenterological procedure. Y.O.: Data curation and gastroenterological procedure. M.S.: Conceptualization, methodology, supervision, writing—review and editing, and gastroenterological procedure. A.Y.: Conceptualization, methodology, writing—review and editing, supervision, and surgical procedure. T.N.: Conceptualization, methodology, writing—review and editing, supervision, validation, and surgical procedure. All authors have read and approved the final article.
Supplemental Material
sj-docx-1-lat-10.1177_10926429261468977 — Supplemental material for Clinical Impact of Residual Gallbladder Neck–Cystic Duct Stones on Postoperative Outcomes in Acute Cholecystitis: A Retrospective Study
Supplemental material, sj-docx-1-lat-10.1177_10926429261468977 for Clinical Impact of Residual Gallbladder Neck–Cystic Duct Stones on Postoperative Outcomes in Acute Cholecystitis: A Retrospective Study by Satoshi Nishiwada, Tetsuya Tanaka, Teruyuki Hidaka, Yuki Kirihataya, Takeshi Takei, Tomomi Sadamitsu, Hiroki Nakahara, Masataka Kakiuchi, Kanako Hosota, Yoshiki Tamada, Kazusuke Matsumoto, Junya Suzuki, Hazuki Horiuchi, Yasushi Okura, Masayoshi Sawai, Atsushi Yoshimura, and Tadashi Nakagawa
Footnotes
Acknowledgments
The authors would like to thank the Department of Emergency at the Minami-Nara General Medical Center for their support throughout the study. They also express their gratitude to the nursing, radiography, and operating room staff for their assistance in patient care.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.