
Abstract
Background:
A miniaturized, self-powered Brain NeuroModulator (BNM) device, endoscopically implanted under neuroleptanalgesia in the submucosal layer of the proximal lesser gastric curvature, has the potential to consistently increase parasympathetic tone as measured by heart rate variability (HRV).
Objective:
Since type-2 diabetes mellitus is associated with autonomic nervous system dysfunction, we assessed whether BNM induced autonomic rebalancing translates into measurable improvement of glycemic control through a change of HRV.
Methods:
The BNM device was implanted on a 69-year-old male with a 25-year history of insulin-dependent type-2 diabetes mellitus under treatment with 22 IU/night of insulin plus semaglutide and metformin. HRV was assessed before and after the procedure. After the implant, continuous glucose monitoring (CGM) with an Abbott FreeStyle Libre sensor (15-minute sampling interval) was performed.
Results:
The endoscopic procedure was uneventful and lasted 15 minutes. The BNM device remained in a stable position throughout the observation period. HRV analysis confirmed increased variability. Post-implant morning HRV showed progressive parasympathetic recovery compared with baseline. Within 2 months of implantation, therapy with semaglutide and metformin was discontinued, and insulin was progressively reduced from 22 to 0 IU.
Conclusions:
The BNM implant was feasible and safe, with clinically meaningful improvement in glycemic control associated with autonomic rebalancing within approximately 10 weeks of implantation. These data provide compelling preliminary evidence that correcting sympathetic dominance through vagal afferent stimulation may alter the clinical course of insulin-dependent type 2 diabetes.
Keywords
Introduction
Metabolic syndrome is one of the major medical problems in Western countries, affecting more than 40% of adults and representing a modifiable risk factor for cardiovascular disease, type-2 diabetes mellitus (T2DM), and other critical health outcomes.1–3 The underlying pathogenetic mechanisms of metabolic syndrome include insulin resistance, satiety default in central obesity, and low-grade systemic inflammation. 4 Autonomic nervous system (ANS) imbalance—specifically the prevalence of sympathetic over parasympathetic tone—represents a transversal and underappreciated feature, shared across the entire spectrum of metabolic disorders.5,6
The history of autonomic nerve system physiology is deeply rooted in neuroscience. In 1849, Claude Bernard demonstrated the induction of diabetes by puncturing the base of the fourth ventricle of the brain, establishing the nervous origin of glycemic dysregulation. Although the induced hyperglycemia was transient, it clearly resulted from stimulation of the sympathetic nervous system—a finding whose mechanistic implications took over a century to be elucidated. 7 It is now established that the ANS exerts a critical role in regulating metabolic homeostasis, insulin secretion, and immune function, 8 with the vagus nerve and central cholinergic signaling identified as pivotal modulators of the inflammatory reflex and of peripheral insulin sensitivity.9,10
In 2006 Gene-Jack Wang et al. assessed the neurobiological responses to an implantable gastric stimulator acting on the vagal plexus of the stomach, which elicited the brain circuits located in the right hippocampus, right anterior cerebellum, orbitofrontal cortex, and striatum. 11 Furthermore, measurement of heart rate variability (HRV) has provided a well-validated, non-invasive method to test the functional state of the central ANS and the balance between the sympathetic and parasympathetic branches. 12 A reduced HRV, reflecting sympathetic dominance, is consistently associated with insulin resistance, poor glycemic control, and increased cardiovascular risk in T2DM patients.12,13
Previous experience with gastric electrical stimulation in morbidly obese patients demonstrated that electrical gastric pacing modulates the ANS by increasing HRV and decreasing the LF/HF ratio (sympathetic-to-parasympathetic balance), with potential clinical benefits on metabolic syndrome independently from weight loss.9,15 Based on these observations, a novel approach was developed consisting of an endoscopically implantable electronic device, the Brain NeuroModulator (BNM), which is catheter-free, self-powered, and designed to be placed into the submucosal layer of the proximal lesser gastric curvature—an area called the “gastric node” (GN), where the anterior and posterior branches of both vagal trunks merge to supply the stomach.
The first BNM human implant was performed on a healthy 30-year-old male volunteer in July 2018. At 96 months of follow-up, the device still remains in the thickness of the gastric wall, with no adverse events or tissue damage, confirming long-term biocompatibility and safety. Post-procedural HRV analysis in this subject demonstrated a consistent increase in the parasympathetic tone, validating the proposed mechanism of action. 17 Further animal testing has confirmed the feasibility of this minimally invasive endoscopic approach. 1
The present study describes the first BNM human implant on an insulin-dependent T2DM patient. The primary study aim was to assess whether ANS rebalancing induced by BNM stimulation of the afferent vagal pathway is associated with measurable improvement of glycemic control and/or reduction of pharmacological burden. A secondary study aim was to characterize the dynamic properties of the glycemic signal before and after implantation using high-resolution continuous glucose monitoring (CGM).
Methods
Patient
A 69-year-old Caucasian male (BMI 20.4 kg/m2, blood pressure 110/70 mmHg), with a 25-year history of T2DM and no personal history of smoking, alcohol abuse, or cardiovascular disease, was implanted with BNM on February 14, 2026. He had been under CGM with an Abbott FreeStyle Libre sensor since December 2025. The pre-implant pharmacological regimen included semaglutide 7 mg once daily in the morning, metformin extended-release 1000 mg twice daily, canagliflozin/metformin 50/850 mg twice daily, and insulin glargine 300 U/mL 22 IU subcutaneously before sleep. Detailed informed consent was obtained for the procedure. Ethics committee approval was obtained (protocol no. 000347-119, Jan. 14, 2000, ULSS 12).
Device
The BNM is a miniaturized (51 × 6 × 3.5 mm) self-powered electronic device consisting of two integrated components. The tail of the device comprises a piezoelectric power strip that captures mechanical energy from pulsations of the left gastric artery, gastric peristaltic motility, and overall body movement, thereby eliminating the need for a battery or external power source. The head contains two platinum electrodes on its surface and circuitry with embedded software to generate and modulate a bipolar depolarizing output voltage directed at the gastric wall in the GN area. All device components, including the endoscopic delivery system, represent proprietary know-how of MedAutonomic.
Endoscopic implantation procedure
The procedure was performed under short neuroleptanalgesia (fentanyl 100 mcg + midazolam 3 mg). The patient was positioned in a right-lateral semiprone position to facilitate direct access to the lesser gastric curvature and to exploit the effect of gravity. A standard 9,2 mm sterilized endoscope was equipped with a custom-designed tool assembly comprising: (i) a sterile silicon shuttle pre-loaded with the BNM; (ii) a needle dissector for submucosal pocket creation; (iii) an introducer for device positioning. No antibiotic prophylaxis was needed.
After passing the upper esophageal sphincter and reaching the gastric cavity, the implant site was precisely identified on the proximal lesser gastric curvature (GN). Saline was injected in the gastric wall to create a submucosal pocket, and the BNM was smoothly introduced (Fig. 1). The overall endoscopic procedure lasted 15 minutes, of which just 4 minutes were required for device implantation. No mucosal bleeding occurred.
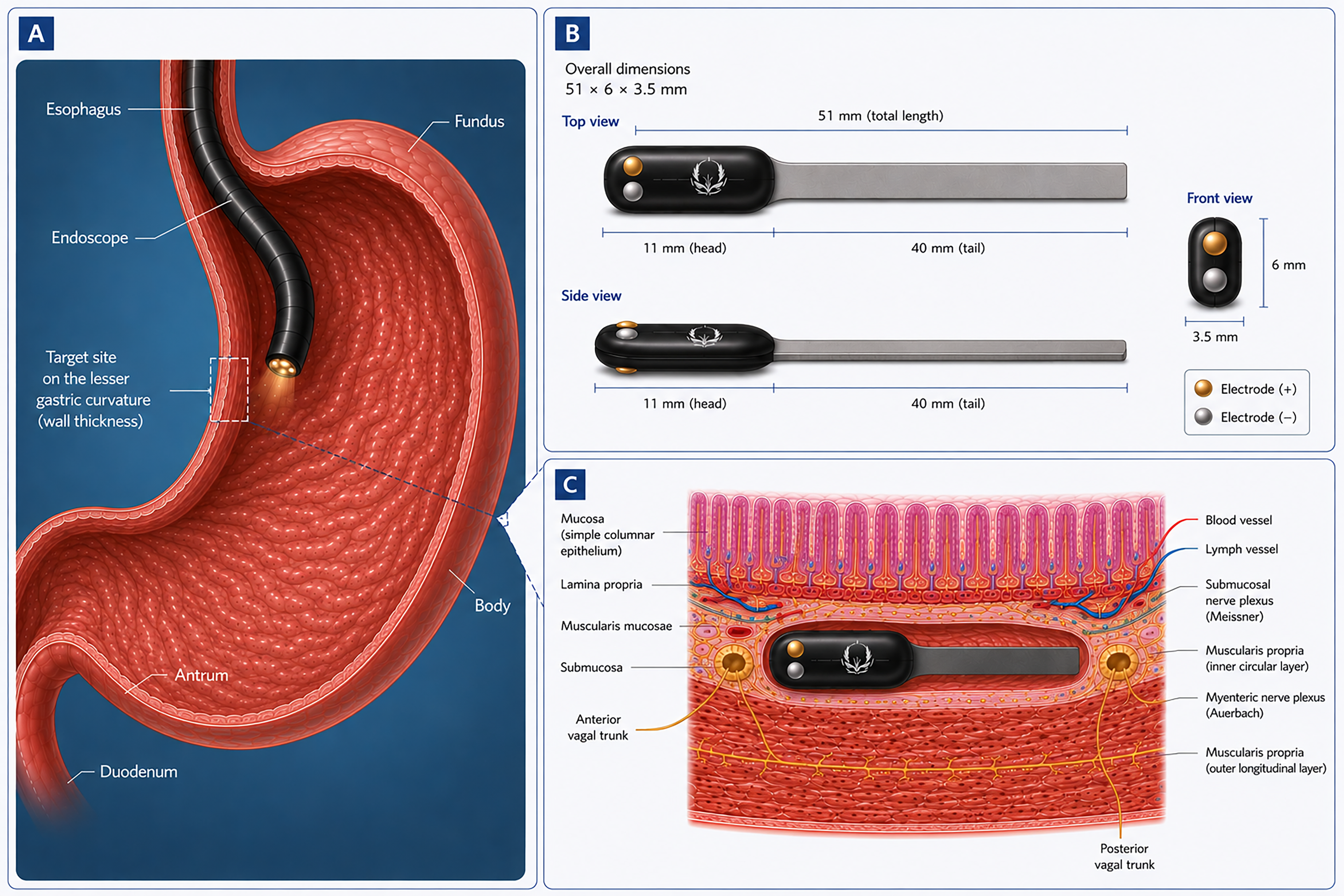
The BNM device and its anatomical placement. Schematic representation of the lesser gastric curvature (gastric node area) showing the bipolar electrode placement relative to the anterior and posterior vagal trunks.
HRV assessment and metrics
A 5-minute ECG recording was performed twice daily (morning measurement, pre-breakfast, and night measurement after-dinner in standardized conditions) after the endoscopic implantation. Data were analyzed using a dedicated algorithm to extract time-domain and frequency-domain HRV parameters, including RMSSD, LF/HF ratio, and total power, as indices of sympathetic-parasympathetic balance, and were compared with baseline values.
Continuous glucose monitoring assessment and metrics
Glycemic data were collected continuously using the Abbott FreeStyle Libre CGM system at 15-minute intervals (96 data points per day) from January 23, 2026, to April 30, 2026, yielding a dataset of approximately 5800 data points over 66 days. The analysis was carried out over 56 days and 7 consecutive observation periods (Table 1).
Data Points in the Observation Periods
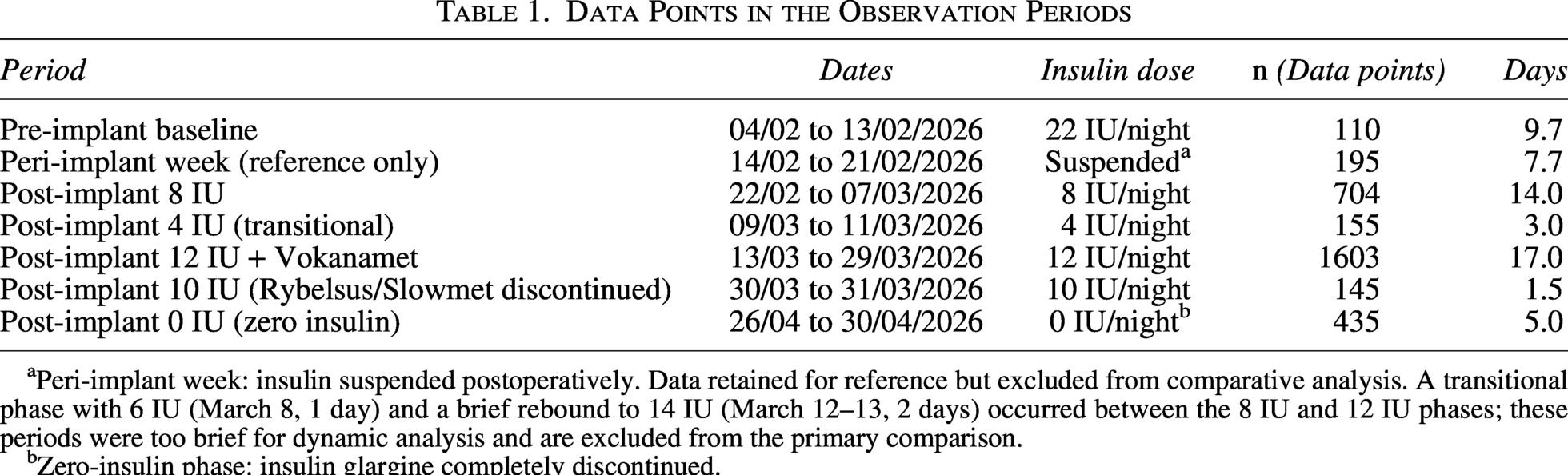
Peri-implant week: insulin suspended postoperatively. Data retained for reference but excluded from comparative analysis. A transitional phase with 6 IU (March 8, 1 day) and a brief rebound to 14 IU (March 12–13, 2 days) occurred between the 8 IU and 12 IU phases; these periods were too brief for dynamic analysis and are excluded from the primary comparison.
Zero-insulin phase: insulin glargine completely discontinued.
Standard CGM metrics were computed per international consensus18 (Table 2).
Standard CGM Metrics
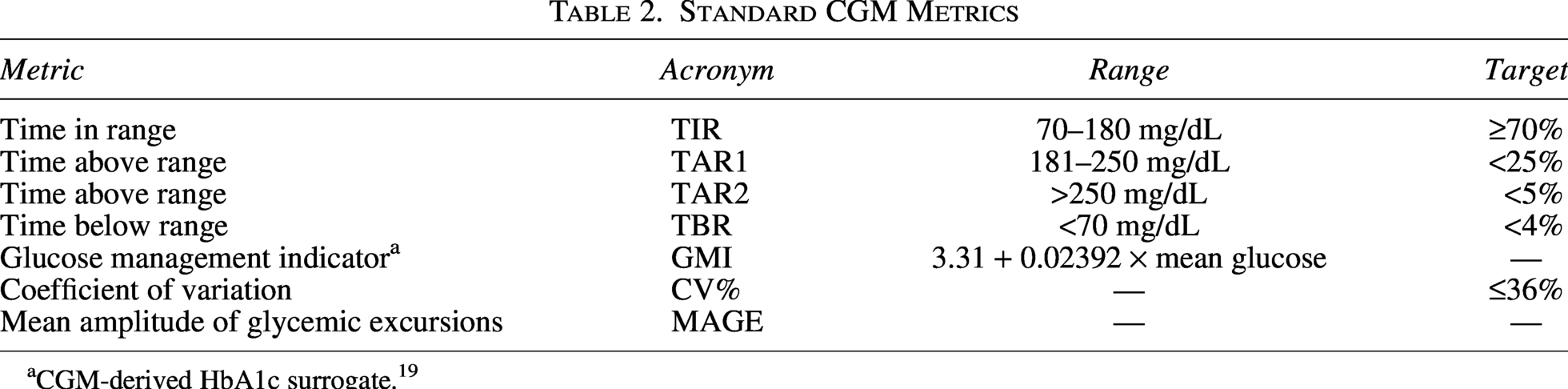
CGM-derived HbA1c surrogate. 19
Dynamic analysis of glycemic oscillations
To quantify the glycemic hunting phenomenon—that is, the persistent oscillatory behavior of the glycemic signal around its set point, characteristic of systems with excessive feedback gain or phase delay—we applied dynamic signal analysis methods to the 15-minute CGM time series.
Poincaré plot analysis. SD1, the standard deviation of successive glycemic differences normalized by √2, quantifies short-term (high-frequency) glycemic variability and was used as the primary proxy for the hunting phenomenon. SD2, reflecting long-term variability (circadian excursions), was computed simultaneously. The SD1/SD2 ratio indicates the relative contribution of rapid oscillations to total variability.
19
Autocorrelation function (ACF). The ACF of the glycemic time series was computed at lags from 0 to 12 hours. In a system with active hunting, the ACF decays slowly (the signal retains memory of its past states); in a well-damped system, the ACF decays rapidly toward zero. Key values reported: ACF at 2h, 4h, 6h, and 8h lags. The first zero-crossing and the first negative ACF minimum (proxy for the half-period of the dominant oscillation) were identified. FFT spectral analysis was performed on resampled (uniform 15-minute grid), mean-subtracted time series. Dominant periods and the fraction of spectral power at the dominant frequency were computed for periods in the 2–24 hour range, corresponding to physiologically relevant glycemic oscillation timescales.
Results
Procedural safety and device stability
The BNM implantation was performed without complications. The total endoscopic procedure lasted 15 minutes, with the actual device implantation taking approximately 4 minutes. No mucosal bleeding occurred. The patient was discharged the same day, reported no post-procedural discomfort, and had a light dinner at home in the evening. The device detector confirmed a stable BNM position in the gastric wall.
Post-implant reduction of pharmacological load
Within 10 weeks after the BNM implant, the following sequential modifications of medical therapy were made based on CGM-guided monitoring (Table 3).
Pre-Implant and Post-Implant Medical Therapy
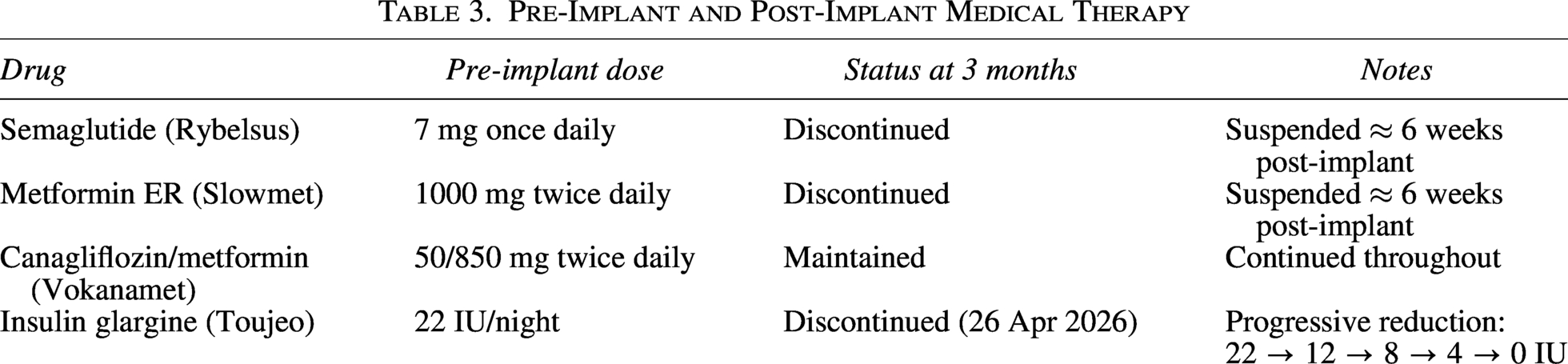
The reduction in insulin dose from 22 IU to 12–4 IU/night represents a decrease of 45%–100% from baseline, with complete discontinuation of exogenous insulin achieved by 26 April 2026—approximately 10 weeks post-implant. This was accompanied by preserved and indeed improved glycemic control (see section: Standard CGM Metrics), with TIR reaching 92.4% and mean glucose 152.3 mg/dL during the first 5-day insulin-free period. The discontinuation of semaglutide and metformin further underscores the magnitude of metabolic change.
Standard CGM metrics
Table 4 summarizes the standard CGM metrics across the primary observation periods. The pre-implant baseline (22 IU/night, n = 110 data points over 9.7 days) was compared with the most robust post-implant period: 12 IU/night (n = 1603 data points over 17 days), which provides the strongest statistical basis for comparison.
Standard CGM Metrics Across the Primary Observation Periods
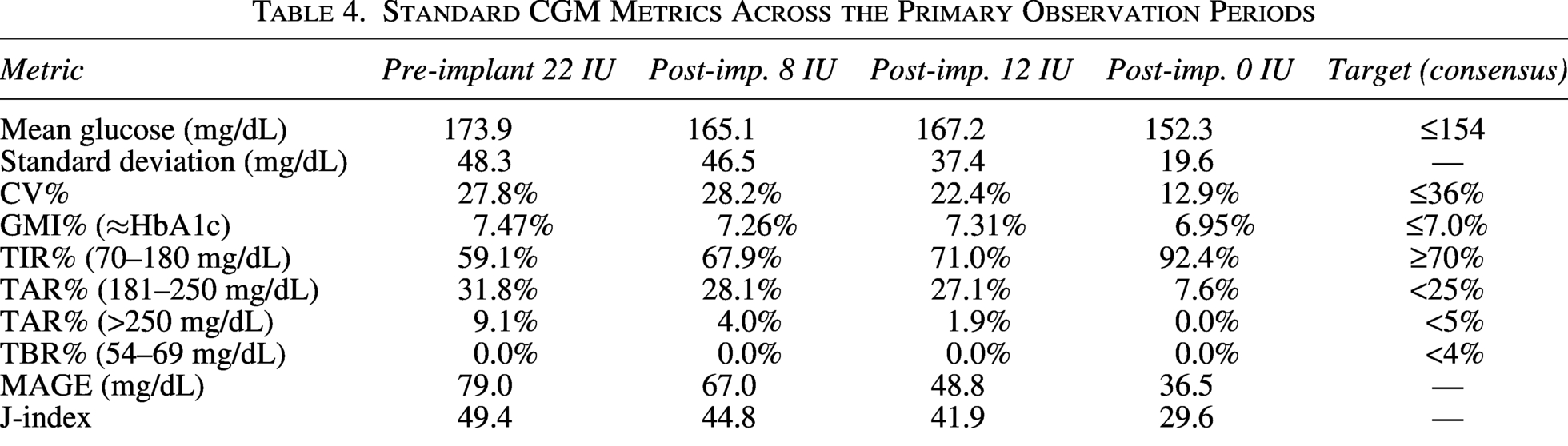
Of note, TIR reached 71.0% in the 12 IU post-implant phase, meeting the international consensus target of ≥70% for T2DM patients. 17 The proportion of readings exceeding 250 mg/dL decreased from 9.1% to 1.9%, while hypoglycemic events (TBR < 70 mg/dL) remained at 0% throughout. CV% decreased from 27.8% to 22.4%, remaining well below the 36% safety threshold.18 In the subsequent zero-insulin phase (26–30 April 2026, n = 435 data points), all metrics improved further: TIR 92.4%, mean glucose 152.3 mg/dL, SD 19.6 mg/dL, CV% 12.9%, GMI 6.95%, TAR > 250 mg/dL 0.0%, MAGE 36.5 mg/dL, J-index 29.6—representing the best glycemic profile across the entire observation period, achieved in the complete absence of exogenous insulin.
Dynamic analysis of glycemic hunting and system damping
The analysis of dynamic properties of the CGM signal revealed a marked and progressive reduction in the glycemic hunting phenomenon following BNM implantation. Results are presented for the four periods with sufficient data for dynamic analysis: pre-implant baseline (22 IU), post-implant 8 IU, 12 IU, and 0 IU phase (Table 5).
Dynamic Analysis of Glycemic Hunting and System Damping
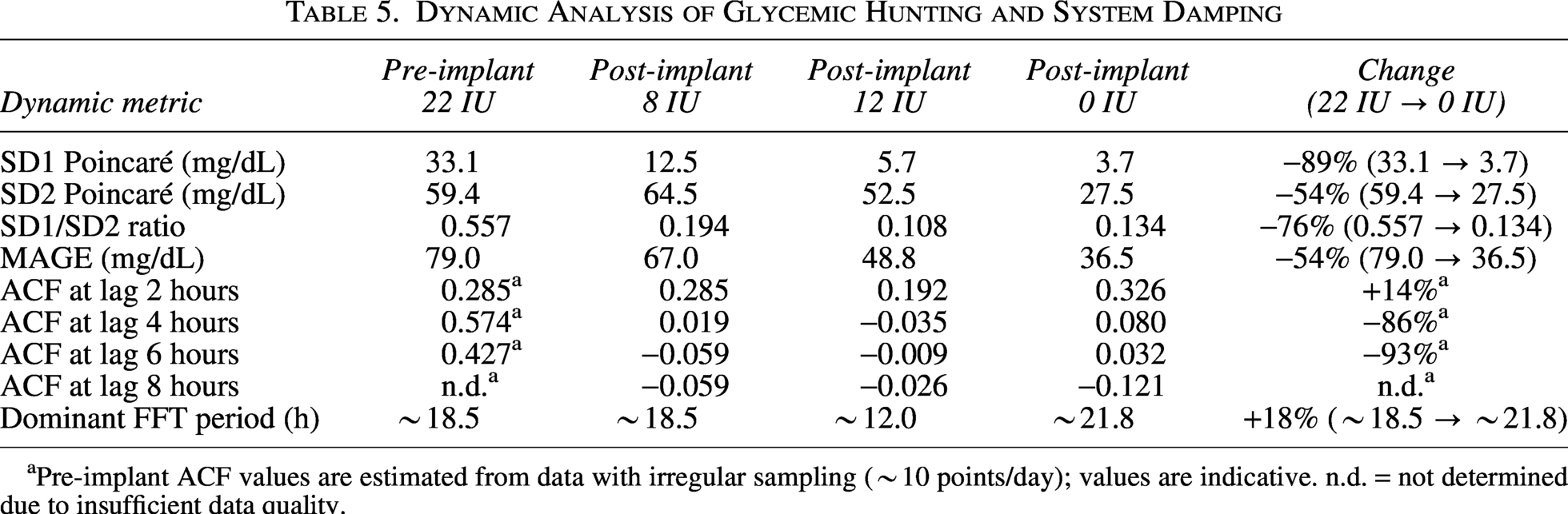
Pre-implant ACF values are estimated from data with irregular sampling (∼10 points/day); values are indicative. n.d. = not determined due to insufficient data quality.
SD1 Poincaré, the most direct index of high-frequency glycemic oscillations, decreased by 83% from pre-implant baseline (33.1 mg/dL) to the 12 IU post-implant phase (5.7 mg/dL), with an intermediate value of 12.5 mg/dL during the 8 IU phase. This monotonic reduction across all post-implant periods indicates progressive and sustained attenuation of rapid glycemic oscillations, independent of the specific insulin dose used. In the subsequent zero-insulin period (26–30 April 2026), SD1 decreased further to 3.7 mg/dL—an 89% reduction versus baseline and the lowest value recorded across the entire observation—confirming that glycemic hunting attenuation persists and indeed deepens in the complete absence of exogenous insulin (Fig. 2).
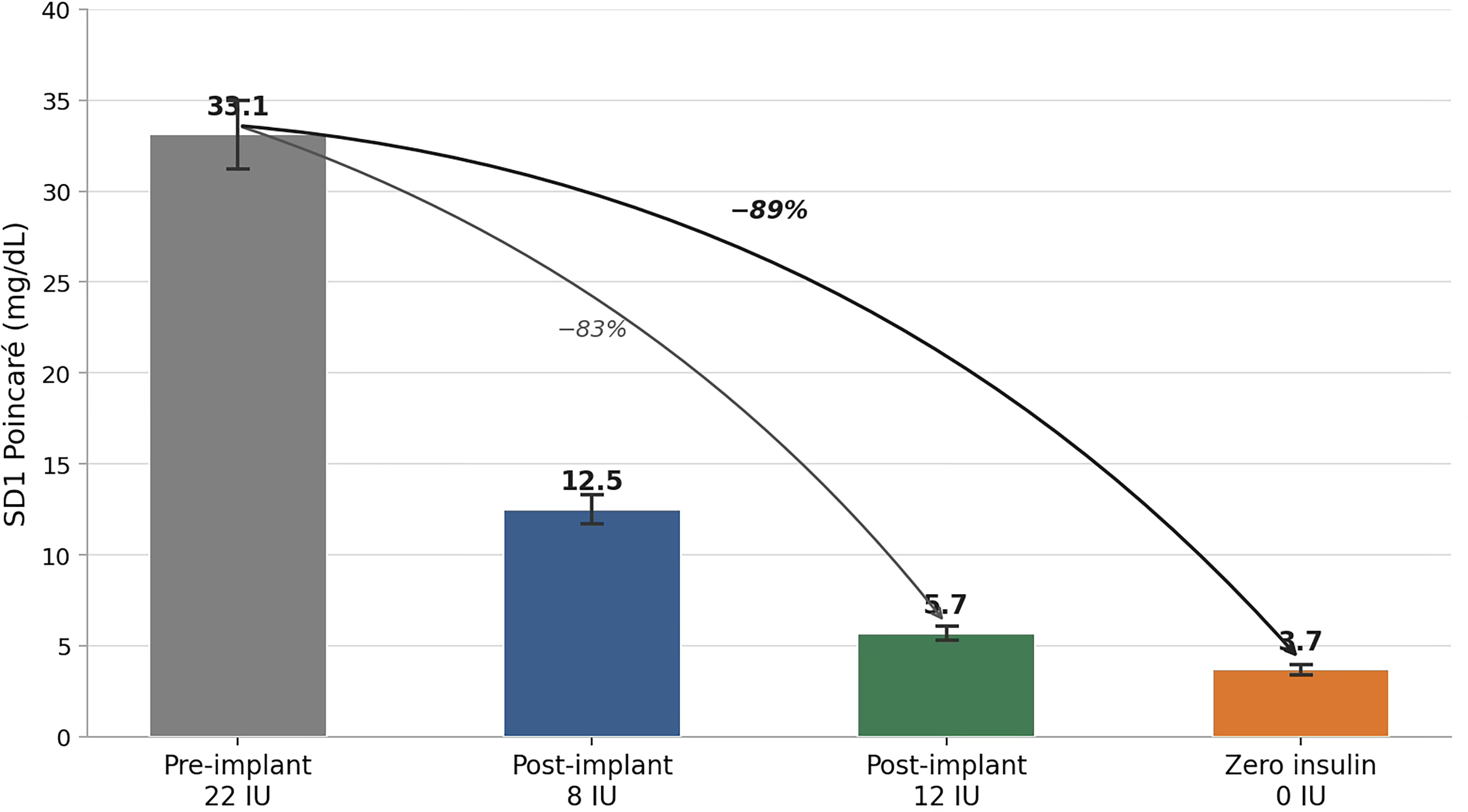
Poincaré SD1 across observation periods. Bar chart showing the progressive reduction in SD1 Poincaré (high-frequency glycemic variability, mg/dL) from pre-implant baseline. Error bars represent 95% confidence intervals. The 89% reduction from baseline (33.1 mg/dL) to the zero-insulin phase (3.7 mg/dL) documents progressive attenuation of the glycemic hunting phenomenon culminating in near-complete suppression in the absence of exogenous insulin.
The ACF analysis confirms that the glycemic signal in the post-implant 12 IU phase loses its autocorrelation substantially faster than in the 8 IU phase. At the 2-hour lag, r = 0.285 (8 IU) versus r = 0.192 (12 IU). The most discriminating comparison is at the 3-hour lag: r = 0.107 (8 IU) versus r = 0.021 (12 IU), an 80% reduction. By the 4-hour lag the 12 IU ACF has already crossed zero (r = −0.035), while the 8 IU phase crosses at ∼4.4 hours (r = −0.035), indicating the system is already well-damped (Fig. 3). This indicates that the post-implant glycemic system loses memory of its prior state 4–6 times more rapidly, consistent with a well-damped feedback system. Notably, the ACF structure of the zero-insulin phase differs from the insulin-treated phases: rather than showing faster early decay, it reveals a shift toward longer-period oscillations (first zero crossing ∼6.5 hours versus ∼3–4 hours for the 8 IU and 12 IU phases), consistent with the removal of the rapid insulin feedback loop and the emergence of slower, meal-driven and circadian glycemic rhythms. The critical finding is nonetheless confirmed by SD1: high-frequency hunting is near-absent in the zero-insulin phase, decoupling the damping effect from insulin dose and strongly implicating ANS rebalancing as the primary driver.
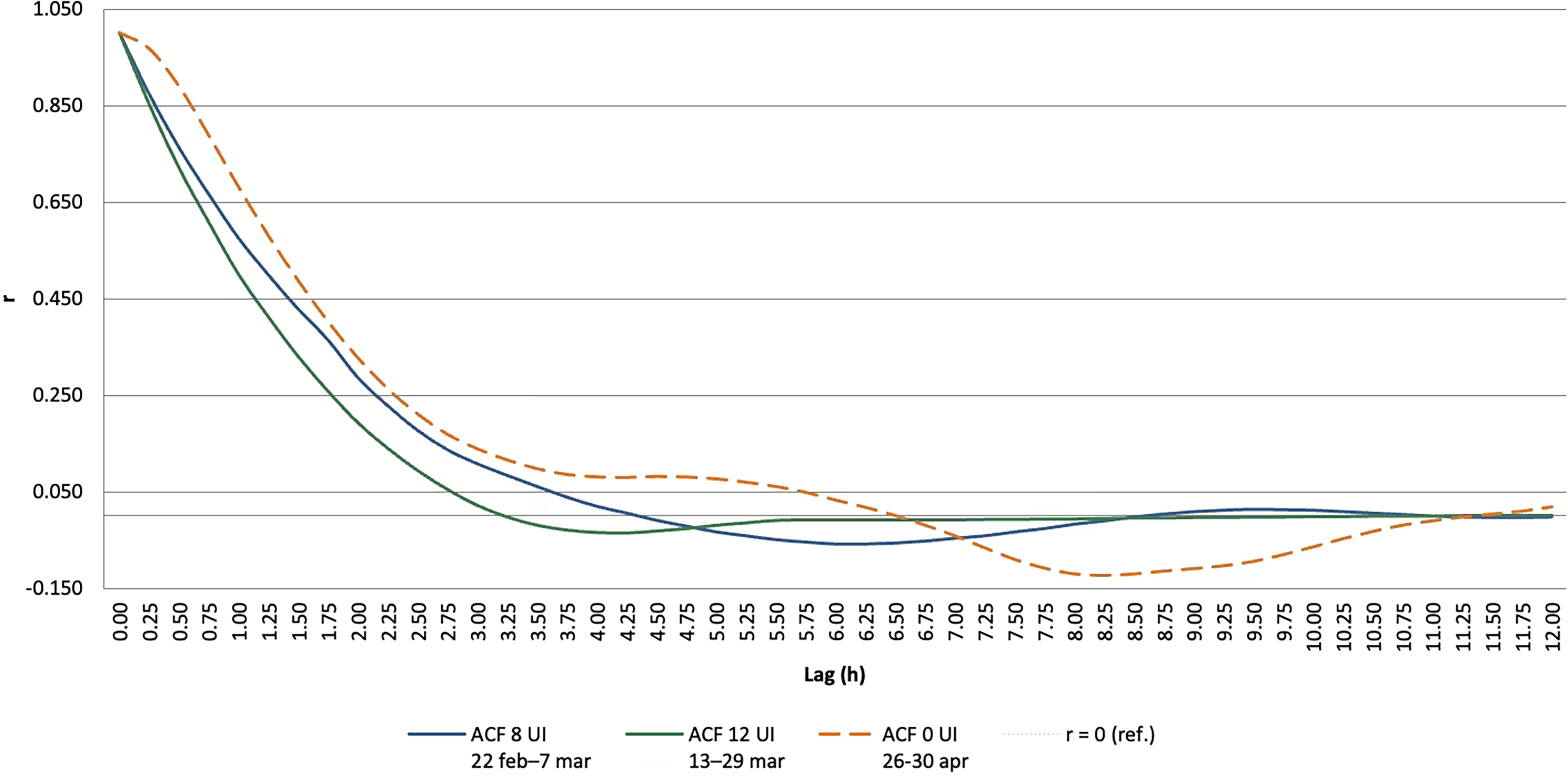
Autocorrelation function (ACF) of the glycemic time series. Comparison of ACF decay curves across three post-implant observation periods: 8 IU (solid blue line, 22 Feb–7 Mar), 12 UI (solid green line, 13–29 Mar), and no insulin (dashed orange line, 26–30 Apr 2026). Grey dotted horizontal line: r = 0 reference. The 8 IU and 12 IU phases show similar decay patterns, reaching its first zero-crossing at lag ∼3.1 hours and lag ∼4.4 hours, consistent with rapid attenuation of short-term glycemic oscillations in both post-implant phases. The zero-insulin phase shows a slower overall decay with first zero-crossing around lag 6.5 hours, reflecting a shift in the dominant oscillation frequency from short-term (insulin feedback-driven) to longer-period rhythms, consistent with meal-driven and circadian glycemic patterns in the absence of exogenous insulin. The near-zero negative excursion in the 0 UI phase is substantially smaller in magnitude, confirming attenuation of high-frequency hunting despite the absence of insulin therapy.
HRV and ANS assessment
Pre-implant baseline HRV assessment showed a sympathetic dominant ANS profile with markedly reduced system elasticity—defined as the capacity to rapidly transition between sympathetic and parasympathetic states in response to physiological stimuli. Pre-implant ECG-based recordings (Shimmer3/Kubios HRV, March 2025, August 2025, and December 2025) confirmed severe sympathetic dominance: RMSSD 6.5–7.0 ms, SNS index 3.8–5.5, stress index 25–35, PNS index −2.1 to −2.2, resting HR 85–90 bpm. These values are abnormal for a subject of this age and BMI, indicating a resting autonomic state comparable to moderate physical exertion or acute psychological stress. The DFA α1 (1.17–1.33 in winter sessions) indicated a signal with Brownian-noise characteristics, consistent with impaired autonomic complexity and reduced regulatory flexibility. Post-implant smartphone-based HRV monitoring (morning measurements, pre-breakfast, standardized conditions; March–April 2026) demonstrated a consistent and progressive shift toward parasympathetic dominance. Best post-implant morning values reached RMSSD 21 ms, SNS index 0.53, stress index 14, HR 61 bpm—values that had no precedent in the pre-implant dataset and exceeded even the optimal baseline (August 2025: RMSSD 15–18 ms, SNS 0.97–1.50, HR 70–71 bpm). The peak RMSSD of 21 ms recorded on 12 April 2026 represents a 3-fold improvement over the pre-implant baseline. The monitoring revealed substantial day-to-day variability in HRV, with nocturnal sympathetic activation episodes strongly correlated with postprandial glycemic excursions (SNS index spikes above 3.5 reliably followed glucose excursions above 200 mg/dL), while at least one episode of extreme nocturnal sympathetic activation (SNS index 4.64) was definitively attributed to acute psychological stress in the presence of optimal glycemia—underscoring the importance of concurrent CGM monitoring for correct HRV interpretation.
The overall pattern, however—a structural upward shift in morning parasympathetic indices, with the best post-implant values exceeding any pre-implant reference—is consistent with the proposed mechanism of BNM action, that is, chronic subthreshold stimulation of gastric vagal afferents resetting the central autonomic “set point” toward parasympathetic dominance.25–27 The ANS rigidity observed pre-implant—with a predominantly elevated sympathetic tone and blunted HRV—is statistically consistent with the established association between sympathetic dominance and impaired insulin sensitivity, reduced glucose uptake, and impaired first-phase insulin secretion in T2DM.12,21 The post-implant shift toward greater parasympathetic activity provides a plausible neurophysiological substrate for the observed metabolic improvements.
Discussion
This report describes the feasibility and safety of endoscopic BNM implant in an insulin-dependent T2DM patient. A clinically meaningful reduction in glycemic variability and a dramatic reduction in pharmacological burden were achieved within 3 months of implantation. Most notably, complete discontinuation of exogenous insulin was achieved 10 weeks post-implant, with optimal glycemic control in the zero-insulin phase. The putative mechanism of the BNM—rebalancing the ANS by increasing parasympathetic tone through stimulation of the gastric node area—was confirmed by post-operative HRV analysis. The improvement of glycemic control, including the ability to maintain euglycemia without insulin, is interpreted as a downstream metabolic consequence of ANS rebalancing.14–17,18–21
Autonomic rebalancing as a therapeutic target in T2DM
The mechanistic link between sympathetic dominance and T2DM pathophysiology is well established. Chronic SNS hyperactivation promotes hepatic glucose output through catecholamine-driven glycogenolysis and gluconeogenesis, inhibits pancreatic insulin secretion via α-adrenergic receptors, and reduces peripheral glucose uptake by inducing skeletal muscle vasoconstriction and insulin resistance. 21 Conversely, vagal (parasympathetic) activation stimulates insulin secretion through a well-characterized cholinergic reflex arc involving the dorsal vagal nucleus and pancreatic β-cells.10,22
The pre-implant ANS profile was characterized by sympathetic dominance and markedly reduced system elasticity—defined as the capacity to transition smoothly between sympathetic and parasympathetic activation in response to physiological demands. This “rigid” ANS phenotype, quantified by HRV analysis, is consistent with the severe insulin resistance and high exogenous insulin requirement observed. The post-implant shift toward parasympathetic dominance, confirmed by HRV parameters, provides a coherent mechanistic framework for the reduction in insulin requirements and improvement in glycemic metrics. The magnitude of baseline sympathetic dominance deserves particular emphasis: pre-implant RMSSD of 6.5–7.0 ms and SNS index of 3.8–5.5 represent values at the lower parasympathetic range. 13 The concurrent DFA α1 of 1.17–1.33 indicates a regulatory phenotype with near-complete loss of short-term autonomic complexity—a pattern associated with cardiovascular risk and impaired metabolic regulation. This profile is fully consistent with the hypothesis that chronic sympathetic dominance is not merely a consequence of metabolic dysregulation but a primary upstream driver of insulin resistance.21,25 The post-implant HRV trajectory, while subject to the previously discussed methodological, showed a structural shift. The best post-implant morning RMSSD (21 ms, 12 April 2026) exceeded the optimal 2025 pre-implant reference values, and the resting HR reduction (from 85 to 90 bpm pre-implant to 61 bpm post-implant) is the typical signature of increased vagal tone. If confirmed by prospective ECG-based HRV studies, this trajectory would represent direct physiological evidence of the BNM’s proposed mechanism of action—vagal upload leading to central upregulation of parasympathetic outflow.26,27 A further finding of this study was the strong correlation between nocturnal index spikes and postprandial glycemic excursions concurrently measured by CGM. This combined HRV-CGM monitoring approach allowed to associate nocturnal autonomic events to glycemic rather than psychological stressors, a distinction with important clinical implications. Specifically, one episode of extreme nocturnal sympathetic activation occurred despite optimal glycemia, attributable to acute psychosocial stress—a finding that would have been incorrectly attributed to glycemic dysregulation without concurrent CGM data. This highlights the complementary nature of HRV and CGM monitoring in characterizing the ANS-metabolic interface. 24
Glycemic hunting phenomenon
A notable and novel finding of this study is the quantification of the glycemic hunting phenomenon—persistent oscillatory behavior of the glycemic signal around its set point—and its progressive attenuation following BNM implant. This phenomenon, analogous to the “hunting” observed in closed-loop feedback systems with excessive gain or phase delay, has received so far limited attention in the clinical literature. In the context of exogenous insulin administration, the feedback loop comprising meal-induced hyperglycemia → insulin injection → glucose lowering → counterregulatory response is inherently prone to oscillatory instability, particularly when the gain of the loop (insulin dose) is high relative to the system’s intrinsic damping capacity. The high pre-implant insulin dose (22 IU), combined with sympathetically driven counter-regulatory responses (epinephrine-mediated glycogenolysis and glucagon secretion), may have amplified this instability. The 83% reduction in SD1 Poincaré and 64%–80% reduction in ACF at 4–6 hour lags observed from the 8 IU to the 12 IU post-implant phase indicate that the glycemic system became substantially more damped. Importantly, this improvement appears to be driven primarily by ANS rebalancing rather than the specific insulin dose, as evidenced by the monotonic improvement in SD1 across all post-implant periods, regardless of dose variations. The zero-insulin phase (26–30 April 2026) provides the most compelling evidence for this interpretation: with no exogenous insulin whatsoever, SD1 reached its nadir (3.7 mg/dL, −89% versus baseline), TIR peaked at 92.4%, and CV% fell to 12.9%—values within the range observed in non-diabetic individuals. It should be noted that the ACF profile of the zero-insulin phase shows a different oscillatory structure from the insulin-treated phases—with a slower overall decay and later zero-crossing (∼6.5 hours versus ∼3 to 4 hours for the 8 IU and 12 IU phases)—reflecting the removal of short-period insulin feedback dynamics and the emergence of longer-period circadian rhythms. The SD1 Poincaré metric, which captures high-frequency oscillations independently of this spectral shift, remains the most valid comparator across phases and confirms the attenuation of glycemic hunting. The dissociation between zero insulin dose and glycemic stability constitutes strong evidence that the BNM restores central autonomic regulation of pancreatic function and hepatic glucose metabolism independently of exogenous insulin.
Stress-induced glycemic excursions and the CGM–HRV interface
Another clinically relevant observation in this study concerns the dynamic relationship between acute stress, sympathetic activation, and glycemic excursions. High-resolution CGM revealed that glycemic peaks not attributable to meals—occurring in fasting conditions, at night, or in temporal association with identifiable stressors—were consistently accompanied by increases in sympathetic tone as reflected in HRV measurements. This is consistent with the phenomenon of stress-induced hyperglycemia, which encompasses the full spectrum of physiological stressors: physical pain, sleep disruption, and psychological stressors such as situational anxiety.23,24 The mechanism is uniform across stressor types: activation of the hypothalamic-pituitary-adrenal axis and releases of cortisol, epinephrine, norepinephrine, and glucagon, all of which promote hepatic glucose output and reduce peripheral insulin sensitivity. 23 In a patient with pre-existing impaired insulin secretion and insulin resistance, these counter-regulatory responses produce disproportionate and prolonged hyperglycemia.
The high-resolution CGM (15-minute sampling) provides sufficient temporal resolution to capture these stress-induced glycemic spikes that would be invisible to conventional fingerstick glucose monitoring. Typically, a glycemic excursion occurring with simultaneously elevated SNS tone (reduced HRV, elevated LF/HF ratio) is consistent with a stress-driven origin, whereas a post-prandial excursion typically occurs in a setting of relative parasympathetic activation (the “rest and digest” response mediated by cephalic and gastric vagal reflexes). 24 This CGM-HRV integration approach represents, to our knowledge, a novel analytical framework to clarify the etiology of glycemic excursions in real-world ambulatory monitoring and warrants systematic investigation in future studies.
The progressive ANS rebalancing induced by BNM may attenuate stress-induced glycemic excursions through two complementary mechanisms: first, by reducing the baseline sympathetic tone available in response to stressors; and second, by enhancing the parasympathetic buffering capacity (ANS elasticity) that normally moderates counter-regulatory responses.
Limitations and future directions
Limitations of the present report must be acknowledged. First, this is a single-patient case study, and generalizability is inherently limited. The observed improvements, while compelling, require confirmation in larger, controlled studies with appropriate comparator arms. Second, the observation period remains limited (10 weeks of high-quality 15-minute CGM data including a zero-insulin phase). Therefore, further follow-up is required to assess the durability of the metabolic improvements.
Future studies should include: (i) a standardized pre-implant pharmacological run-in period to ensure a stable baseline; (ii) blinded HRV analysis with pre-specified endpoints; (iii) extended long-term CGM follow-up beyond the initial 10-week observation; (iv) inclusion of patients across a broader spectrum of T2DM severity; and (v) systematic assessment of the CGM–HRV correlation as a diagnostic tool for stress-induced hyperglycemia.
Conclusions
This feasibility study demonstrates that implant of BNM in the lesser curve of the gastric wall is feasible, safe, and well tolerated. It is associated with an increase in parasympathetic tone and reduction in high-frequency glycemic variability consistent with marked attenuation of the glycemic hunting phenomenon, ultimately leading to discontinuation of exogenous insulin.
Correcting ANS imbalance through targeted vagal afferent stimulation via the gastric node may represent a novel therapeutic approach to T2DM and metabolic syndrome. The long-term safety profile of the BNM procedure established over 8 years of follow-up and the metabolic efficacy data reported here indicate the need of a prospective multicenter trial. The BNM may represent a paradigm shift from pure pharmacological management to a targeted neurophysiological approach in T2DM.
Footnotes
Acknowledgments
All tools and devices developed to support and enable the implantation procedure are part of MedAutonomic proprietary know-how. The authors thank Arfeo Canaglia, Ugo Scalabrin MVet Med, Simone Cigaina, Andrea Arduini MEng, Betty Grassi PharmD, and Domenico Moro for their contributions to device development and clinical support. The authors thank the patient for his informed consent and dedicated participation in the monitoring protocol.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.