
Abstract
Background:
The advantages of robotic surgery have expanded its use, including in liver transplantation, where donor safety is paramount. Improved short- and long-term outcomes, such as reduced hernia and wound pain, are beneficial for liver transplantation. Here, we provide a narrative review and didactic video illustrating the key steps, technical tips, and insights of robot-assisted donor hepatectomy.
Methods:
A literature search was performed until June 2025, focusing on the outcomes of minimally invasive donor hepatectomy. Relevant studies were identified using predefined keywords. In addition, a representative case of robot-assisted left lateral sectionectomy has been performed and documented.
Results:
Current evidence demonstrates increasing interest in robot-assisted approaches for donor hepatectomy, with reported outcomes primarily addressing surgical safety, perioperative parameters, and donor recovery.
Conclusion:
Robot-assisted surgery may be a useful tool in the surgical armamentarium for liver transplantation.
Introduction
Robotic surgery offers several advantages over conventional laparoscopic techniques, including enhanced dexterity, three-dimensional views, and improved ergonomics. 1 These features facilitate more precise dissection and manipulation of the liver parenchyma, contributing to several intraoperative and early postoperative advantages such as less blood loss, lower pain scores, and shorter hospital stay.2,3 Recent studies also suggest that robotic techniques may reduce the long-term complications commonly associated with open surgery. 4 These include incisional hernia, bowel obstruction, and chronic wound pain commonly observed after open surgery. 5 The reduction in postoperative complications underscores the potential of robotic techniques to improve the long-term outcomes and quality of life of donors. 6 This is an essential consideration during donor hepatectomy, in which the health and recovery of living donors are critical for the overall success of the transplantation process. Despite these advances, the application of robotic techniques in living donor liver transplantation (LDLT) is still in its early stages, with ongoing debates regarding their superiority over traditional laparoscopic or open methods, and more evidence is needed, as stated in the guidelines. 7
This narrative review summarizes existing evidence on robotic donor hepatectomies. In addition, we present a didactic video highlighting the tips and tricks from our experience with robot-assisted donor hepatectomy developed through our practice in robotic hepatopancreatobiliary surgery.
Methods
Literature search strategy and study selection
The literature for this narrative review was retrieved from Medline, PubMed, Cochrane Library, and Embase databases covering all records up to June 2025. The following search terms were used: “Liver,” “Liver transplantation,” “Living donor,” “Surgery,” “Donor operation,” “Robotic Surgery,” “Minimally invasive surgery,” “Parenchymal transection,” “Learning curve,” “Operative time,” “Liver specific complications,” “Donation related complication,” “Conversion,” and “Length of hospital stay.”
In the literature, we focused on the most commonly reported outcomes associated with the adoption of minimally invasive approaches in donor hepatectomy, and priority was given to studies that evaluated these endpoints. The reference lists of articles were screened to identify additional relevant studies.
Video demonstration
A 32-years-old male, with no significant medical or family history. Candidate for LDLT for his daughter. On preoperative evaluation, the patient had normal vascular and biliary hepatic anatomy without any variation. Incdocyanin green (ICG) was administered intravenously at a dose of 3.125 mg, 1 hour before anesthesia induction. The operating room setup is illustrated in detail in Figure 1. The patient was placed in a 15-degree reverse Trendelenburg position on the operating table with the legs abducted (Fig. 2).
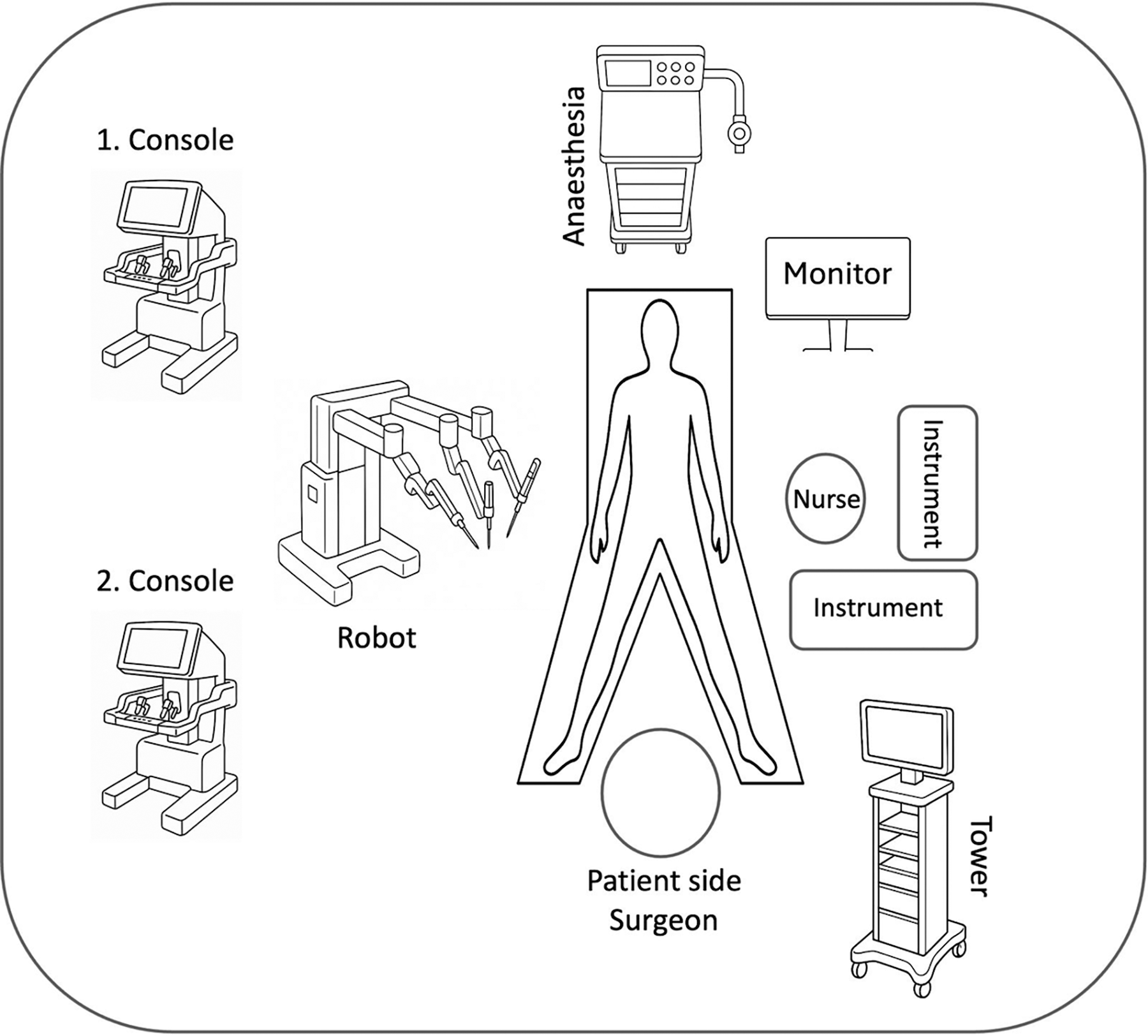
Operating room setup.
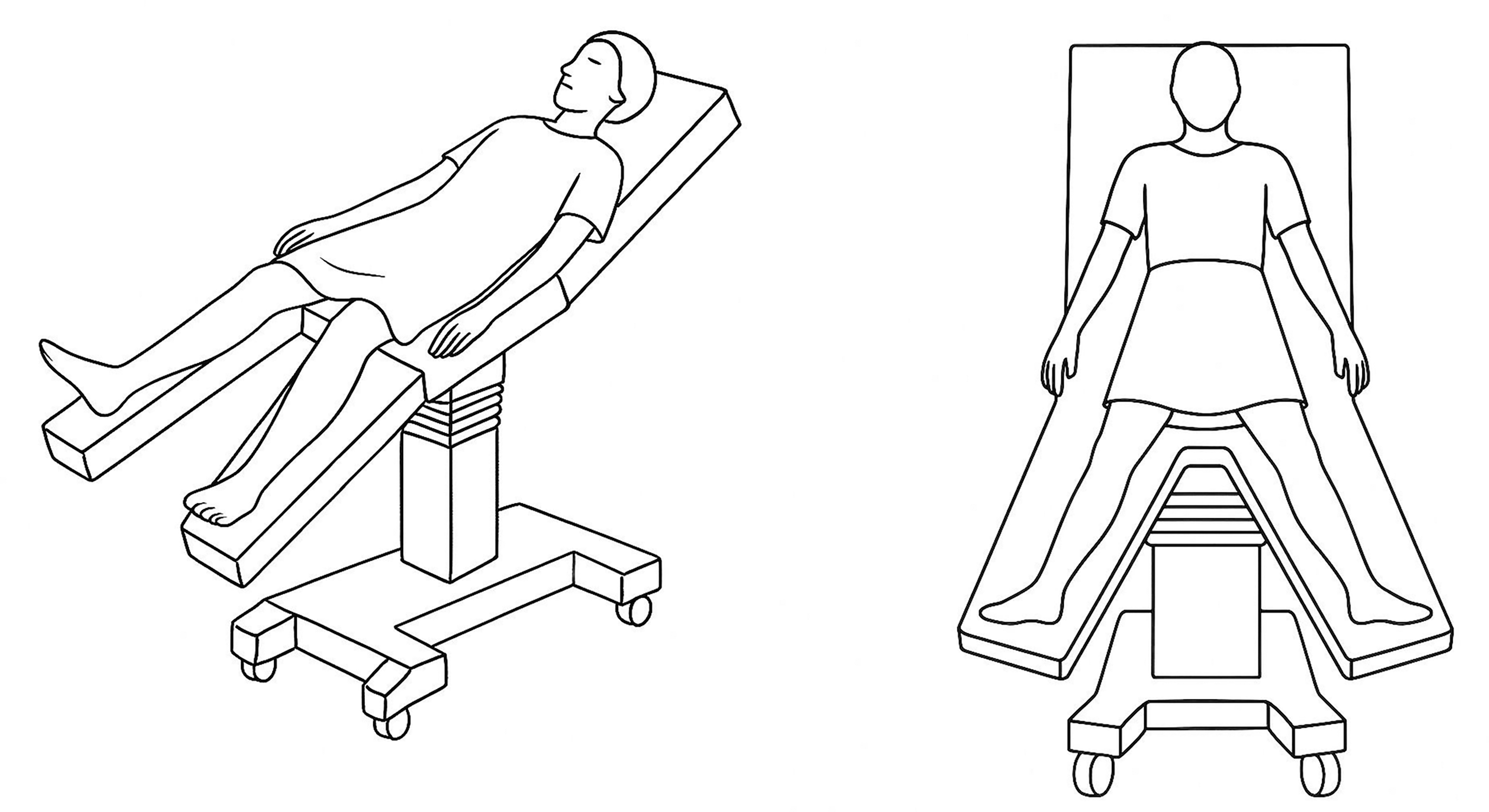
Patient positioning.
Surgical procedure (video attached)
The planned operation was a robot-assisted left lateral sectionectomy. It was performed using a 12 mm assistant trocar placed at the umbilicus to evaluate the abdomen for any undetected pathology, along with four 8 mm robotic trocars and one additional 5 mm assistant trocar (Fig. 3). To avoid time loss during specimen extraction, a Pfannenstiel incision was made, and the Alexis® wound retractor system with its laparoscopic cap was placed at the beginning of the operation. The left lateral lobe of the liver was mobilized by dissecting the falciform ligament, coronary ligament, omentum minus, and Arantius ligament using the double-bipolar technique. After complete mobilization of the left lateral lobe, the hepatoduodenal ligament was dissected, the hilar plate was exposed, the bile ducts were visualized using ICG fluorescence mode, and a landmark clip was applied along the anticipated transection line. The left hepatic artery and portal vein were then slinged. The parenchymal transection line was identified, and transection was initiated using the robotic double bipolar technique assisted by a patient-side surgeon with laparoscopic Cavitron Ultrasonic Surgical Aspirator (CUSA) and clip appliers. Before dividing the vascular structure, the left lateral lobe specimen was placed in an organ-retrieval bag. The left hepatic artery was clipped and divided, the left portal vein was clipped, and the left hepatic vein was divided using a vascular stapler. The previously clipped left portal vein was then divided, and the left lateral lobe was extracted through a Pfannenstiel incision for back-table preparation (Supplementary Video S1).
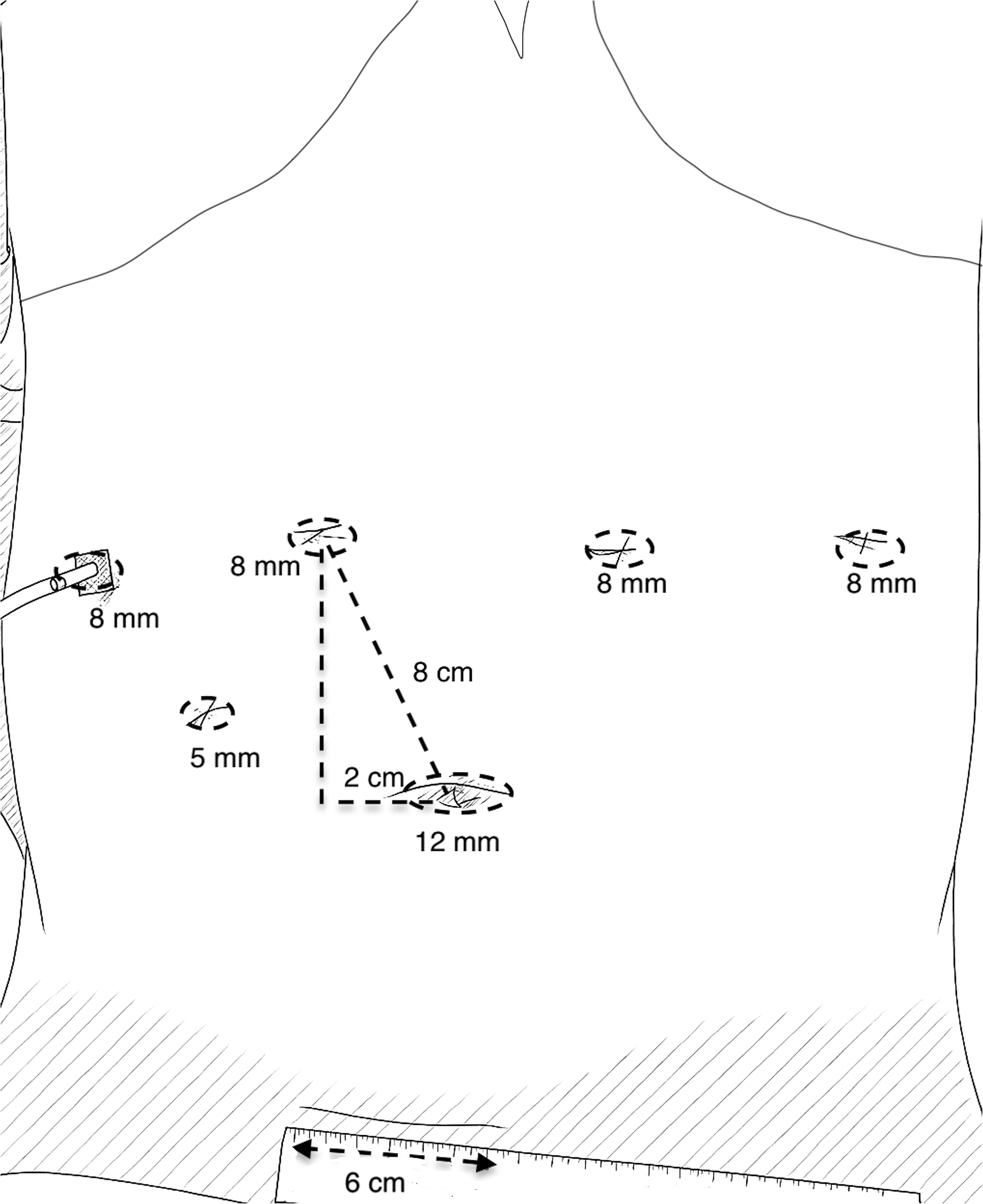
Trocar placement and port sites.
Results
Literature search
Recent studies have highlighted the growing interest in robot-assisted techniques for donor hepatectomies. This approach is increasingly being considered as an alternative to the traditional open or laparoscopic methods. The literature has primarily focused on evaluating the surgical safety of these procedures. Perioperative outcomes such as operative time, blood loss, and complications were closely examined. Donor recovery, including hospital stay and return to normal activities, is another key assessment area.
Case
The total operative time was 310 minutes, with graft retrieval achieved at 260 minutes. The Pringle maneuver was not performed. The estimated intraoperative blood loss was 100 mL. The graft weighed 265 g. The postoperative course was uneventful. The abdominal drain was removed on postoperative day 3, and the patient was discharged on postoperative day 4.
Discussion
Although its application was previously limited owing to commonly cited disadvantages such as high costs, technical challenges, and a lack of robust evidence, robotic surgery has now been adopted for complex procedures such as liver transplantation, following several successful cases and the demonstration of its benefits in surgeries involving other organs. 8
Among hepatobiliary applications, the feasibility of robotic donor hepatectomy was first demonstrated by Chen et al. in a series of 13 patients, who showed outcomes comparable to those of open surgery in terms of blood loss, complication rates, and donor recovery. 9 In a comparative study of robotic and laparoscopic approaches, Troisi et al. reported that the robotic technique offers advantages in terms of reduced blood loss, lower conversion rates to open surgery without statistical significance, and shorter hospital stay, while maintaining comparable postoperative outcomes. 6 Although a longer operative time is frequently cited as a disadvantage compared with open surgery, recent literature suggests that operative time improves significantly after a certain number of cases.10,11 In our case, the operative time was 310 minutes, with graft retrieval at 260 minutes, which aligns with data reported in the literature (290 ± 45 minutes). 6
As presented here, we adapted our CUSA-based parenchymal transection technique, originally developed for laparoscopic liver surgery, for use in robot-assisted donor hepatectomy. By transferring this established technique to a robotic platform, we facilitated the smooth transition from conventional approaches to robotic techniques. This modification was essential to overcome one of the main limitations of robotic liver surgery, namely the absence of a dedicated instrument for parenchymal transection. Careful donor selection, step-up approach starting from the left lateral sectionectomy donor operation, and reproducibility of the technique are key steps in success, especially during the learning curve, and allow surgeons to acquire technical proficiency easily. The literature also supports its reproducibility, indicating that approximately 15–20 cases are sufficient to reach the mastery phase in robotic donor hepatectomy, which is notably lower than the 60 cases typically required to achieve mastery using the laparoscopic approach.2,12,13
Given that the health and recovery of living donors are critical to the overall success of the transplantation process, assessing post-donation quality of life is essential. Approximately 48% of donors report donation-related issues, more than half of which are attributed to the surgical technique and procedure rather than the liver resection itself. 14 These include hernias, scar-related problems, intra-abdominal adhesions, and physical activity restrictions. Minimally invasive techniques, particularly robotic approaches, have been associated with fewer scar-related complications than the conventional methods. 14 Furthermore, robotic donor hepatectomy has not been linked to an increased risk of major liver-specific complications or issues involving the graft or remnant liver. 15 Although conversion to open surgery is an important metric of procedural success, Schulze et al. reported a conversion rate as low as 0.4%, which is lower than that reported for the laparoscopic approach and supports the acceptability of the robotic technique even in this complex setting. 16
As the body of evidence continues to grow and access to robotic technology becomes more widespread, it is likely that robotic surgery will become increasingly part of the standard clinical practice for liver transplantation and will serve as a valuable tool in the surgical armamentarium of liver transplant teams.
Authors’ Contributions
Conceptualization, E.B., A.A., and T.K.; Literature search, E.B., F.H., S.Y., A.Y., and B.D.; Data curation, E.B., A.Y., and B.D.; Original draft preparation, E.B., F.H., S.Y., A.A., and B.D.; Review and editing, E.B., T.K., and A.A.; Visualization, E.B., S.Y., F.H., A.Y. and B.D.; Supervision, E.B., T.K., and A.A. All the authors contributed to this work and approved the final version of the article.
Supplementary Video S1
Footnotes
Disclosure Statement
Drs. Emre Bozkurt, Ferid Hamad, Samet Yigman, Baris Demir, Aydin Alper, and Turan Kanmaz declare no conflict of interest or financial ties. RN Ali Yalcin has no conflict of interest or financial ties to disclose.
Funding Information
This study did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sector.