
Abstract
Background
The reliability of intraoperative evaluation of ganglion cells in the appendix as a guide to a diagnosis of total colonic aganglionosis is unclear.
Objective
To evaluate the diagnostic utility of appendicular innervation in colonic Hirschsprung disease (HD) and TCA.
Methods
Prospective, systematic study of ganglion cells and the neural plexii in appendices from cases (HD and TCA) and age matched controls with frozen and paraffin sections, rapid acetylcholinesterase (AChE) and immunohistochemistry.
Results
A total of 48 appendices (28 controls, 20 cases; 19 frozen) were evaluated. Of these 48, 30 were neonates. Ganglion cell clusters were smaller in controls (28) and HD (6) than those in the rectum, distorted at places and mimicked lymphocytes and endothelial cells, especially in neonates. Complete study of 13 appendices in TCA showed absence of ganglion cells, hypertrophic nerves, AChE activity, and calretinin staining. In 2/13 TCA, an erroneous frozen section identification of ganglia was later corrected based on AChE histochemistry and a panel of IHC stains. Ileal biopsies guided the placement of a ganglionic ileostomy in all. One case each of skip segment aganglionosis in a TCA and variable hypoganglionosis in long segment colonic HD is reported.
Conclusion
Intraoperative characterization of appendicular innervation as a guide to the diagnosis of TCA is unreliable, in part because of the possibility of skip segment disease/variable hypoganglionosis. We propose terminal ileal biopsies for diagnosis and leveling of aganglionosis. AChE on frozen/calretinin on paraffin tissue is the best approach to avoid diagnostic errors.
Introduction
Neonatal distal small bowel obstruction is commonly due to meconium ileus—cystic fibrosis complex, distal ileal atresia, or total colonic aganglionosis (TCA). If the preoperative contrast enema and intraoperative findings do not suggest meconium ileus or ileal atresia, the differential diagnosis of a microcolon and small bowel dilatation is narrowed to TCA. Though it was traditionally held that an aganglionic appendix implied an aganglionic colon and the surgeon biopsied the appendix for an intraoperative frozen evaluation at the outset of laparotomy to confirm/rule out a TCA, 1 this practice has been recently questioned because of possibility of an erroneous diagnosis with such an approach.2,3
The appendix is a small, thin-walled tubular structure with proportionately small neural plexii, especially in a neonate. Intraoperative evaluation of ganglion cells in the appendix as a guide to a diagnosis of TCA is controversial. 4 However, the quantum of literature on the normal and abnormal innervation of the appendix and their therapeutic implications in TCA is still sparse. This study, a systematic histological, histochemical, and immunohistochemical evaluation of the appendicular innervation in the normal and those with varying extents of colonic and distal small bowel aganglionosis, seeks to clarify these clinicopathological issues.
Materials and Methods
Materials
This prospective study was conducted at the Department of Pathology of a tertiary teaching and referral institute for the diagnostic work up for Hirschsprung disease (HD) and allied disorders. Clinical cases included those referred from the Departments of Paediatric and Neonatal Surgery of this institute and other locoregional centers over 36 months. This was performed after review of literature concerning the safety of appendectomy in various circumstances
5
and requisite institutional ethical review board approval. Each case was systematically evaluated clinicoradiologically, and the diagnosis histologically confirmed (Figure 1) prior to surgical management. The study material included appendices from HD (rectosigmoid HD [RSHD], long segment colonic HD [LScHD]), TCA, and normal age matched controls. The nomenclature reflects the extent of contiguous aganglionosis extending cranially from the anal canal up to the sigmoid (RSHD), up to any point between the descending colon and the ascending colon (LScHD), or further up to 50 cm proximal to the ileocecal junction (TCA). The following were the inclusion and exclusion criteria.
Algorithm of study design on appendices from normal controls, suspect HD, and TCA.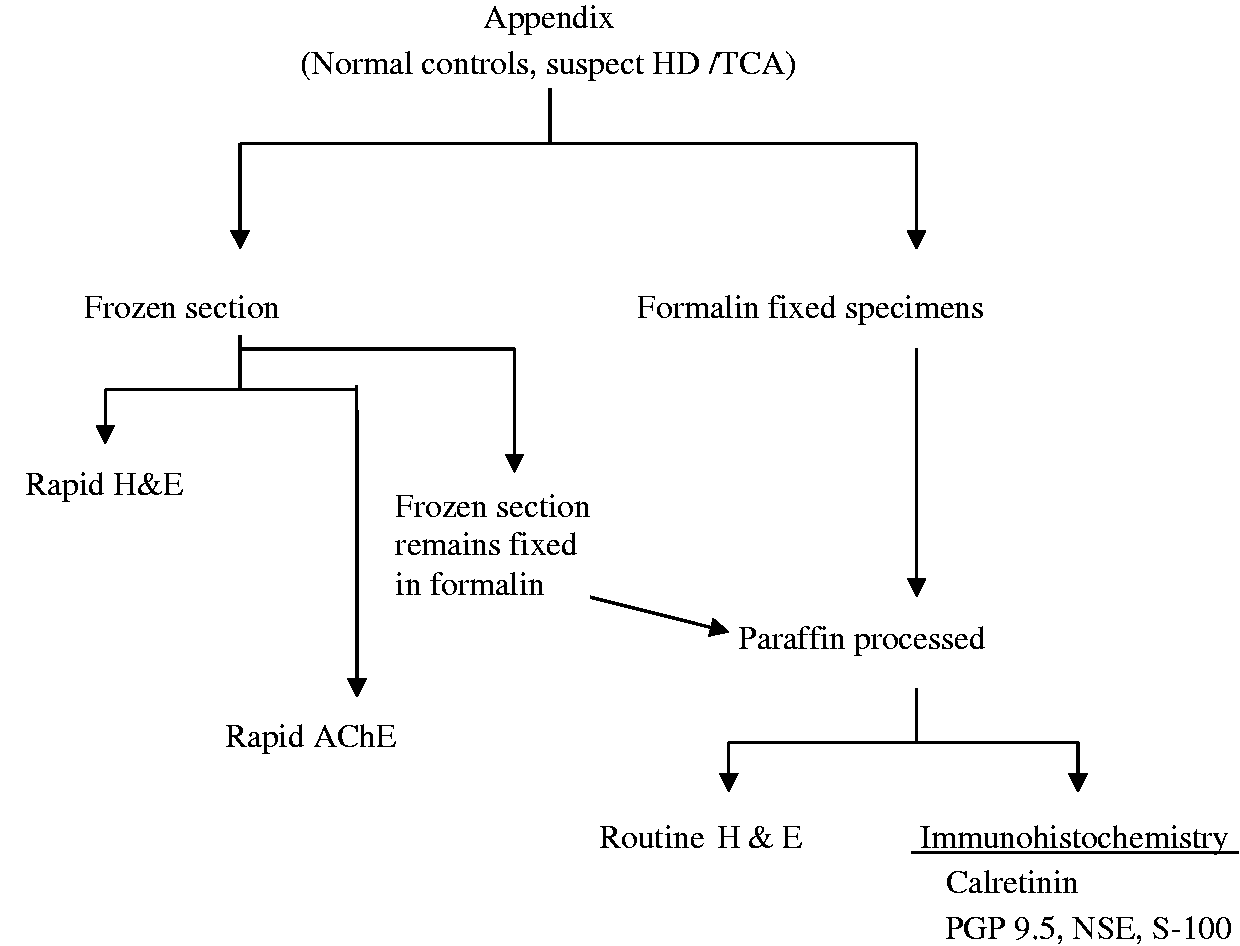
Inclusion criteria
(a) Controls: Appendectomy specimens were obtained from unrelated conditions such as malrotation of the midgut where appendectomy is a routine therapeutic procedure or ileocecal resection for conditions without a primary appendicular pathology, eg, trauma. (b) Cases:
(i) Colonic HD (RSHD, LScHD): Appendectomy specimens from confirmed cases of colonic HD during creation of a stoma/staged pull through procedure. (ii) TCA: Appendectomy specimens from cases of TCA confirmed by histological examination of the colon and small bowel.
Exclusion criteria
All situations where the appendix looked macroscopically pathological, eg, acute inflammation/edema/neoplasia etc were excluded from the study.
Methods
Appendicular specimens were collected onto a 0.9% saline soaked gauze piece. Three cross sectional samples were taken from the base, middle, and tip of the appendix and directly frozen together in a single block in the Leitz cryostat. Ten microns cryostat sections were cut from the frozen tissues with each slide having an average of three sections. Two such slides were stained for rapid hematoxylin and eosin (H&E) for routine morphology, and one stained for rapid acetylcholinesterase enzyme histochemistry (AChE) by the modified method6,7 with a positive control (rectal biopsy of a known case of HD). The rapid AChE method takes approximately 45 min for intraoperative assessment. After frozen section, the tissue remains were processed for paraffin section. Two slides with an average of three paraffin sections each were stained with H&E and further examined. The remaining portion of the appendix was also processed for paraffin sections if there was any suspicion of aganglionosis. All the frozen and paraffin sections were evaluated by three consultant pathologists separately. A consensus opinion was finalized by the three after the initial individual assessment. In our practice, the above combination of frozen (H&E, AChE) and paraffin section evaluation (H&E) affords a reliable means of diagnosis.
All the sections were studied for ganglion cells in the submucosal and myenteric plexuses and nerve fibers in the submucosa. Frozen sections from appendices of the control groups showed distinct ganglion cells in myenteric plexuses, and they were confirmed by the AChE and paraffin sections.
Further, paraffin sections were immunohistochemically stained for calretinin, 8 PGP 9.5, NSE, and S-100 to highlight ganglion cells and neural fibers in the mucosa and muscularis mucosa. The data obtained from frozen sections including AChE were compared with that obtained from paraffin sections including immunohistochemistry. Where frozen section evaluation was not feasible as the sample was received in formalin, only H&E staining and immunohistochemistry were employed.
Results
A total of 48 appendices were studied, and all were processed for paraffin sections.
A total of 19 were available for frozen evaluation; 10 controls and 9 cases (5 TCA, 4 RSHD). After frozen section evaluation, all 19 were fixed in formalin and processed for paraffin section and stained for calretinin, PGP 9.5, NSE, and S-100 immunohistochemistry.
A total of 29 appendices were received in formalin for routine evaluation; 18 controls and 11 cases (8 TCA including 1 with a skip segment, 1 RSHD, 2 LScHD including 1 with variable hypoganglionosis).
Details of appendices received in saline for diagnostic evaluation.
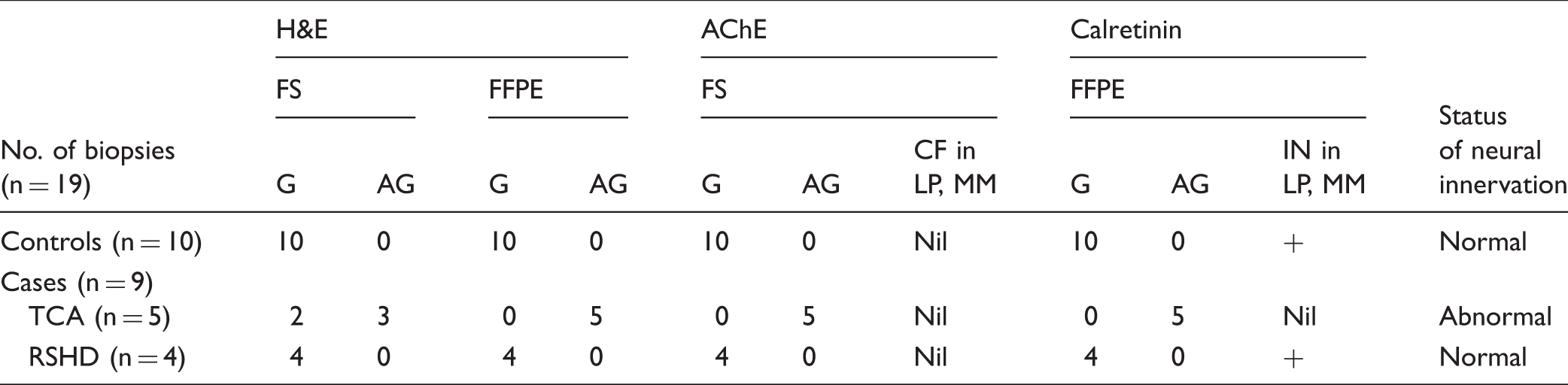
AChE, acetylcholinesterase; AG, aganglionic; CF, cholinergic nerve fibers; FFPE, formalin fixed paraffin embedding; FS, frozen section; G, ganglionic; H&E, hematoxylin & eosin; IN, intrinsic nerve fibers; LP, lamina propria; MM, muscularis mucosa; RSHD, rectosigmoid Hirschsprung disease; TCA, total colonic aganglionosis; +present.
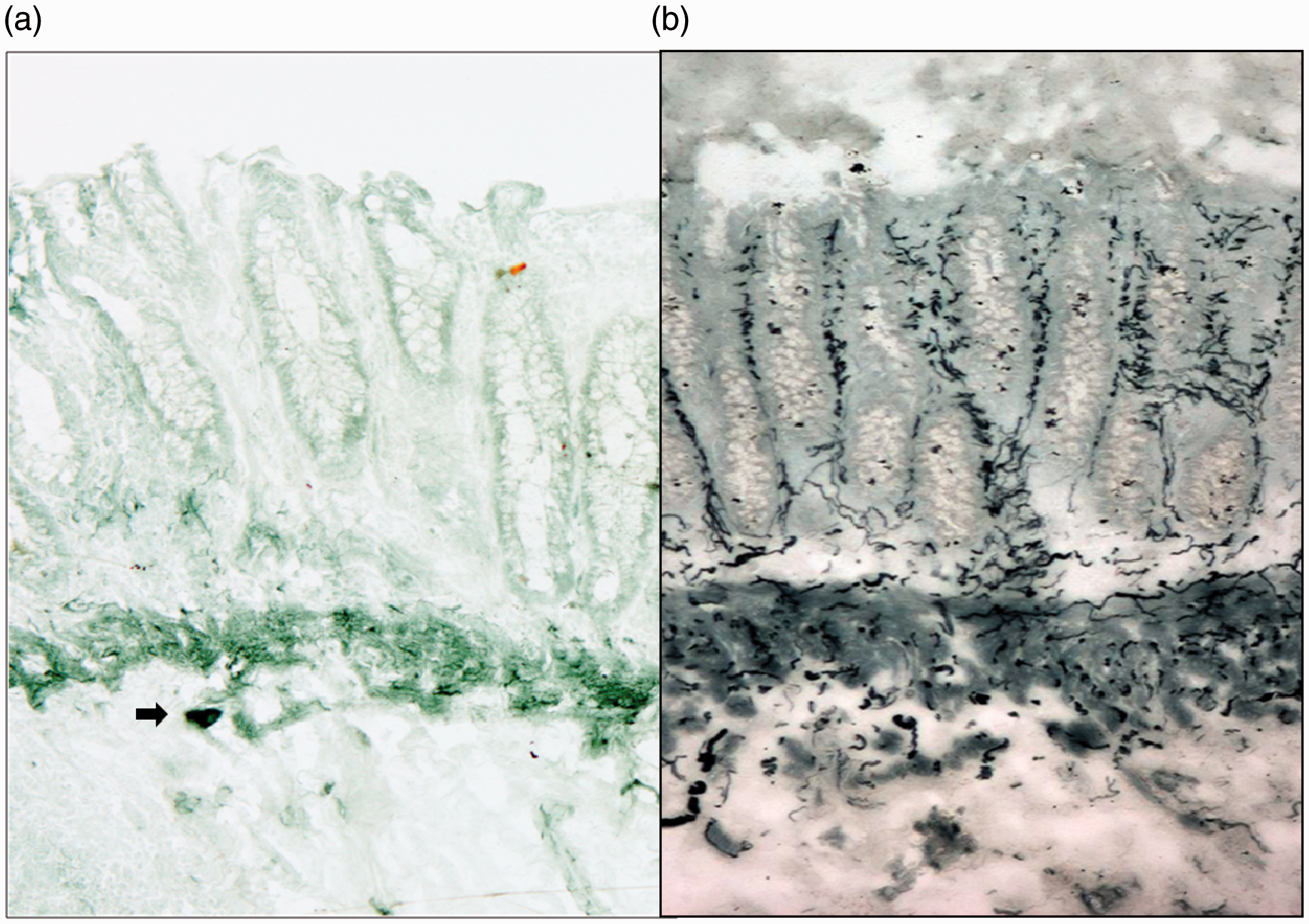
Rapid AChE staining (×100) of (A) normal ganglionic rectal mucosa showing equivocal staining pattern and no increase in AChE activity. The arrow indicates a cluster of ganglion cells in the submucosa and (B) aganglionic rectal mucosa in a case of Hirschsprung disease showing increased AChE activity evidenced by the arborising greenish black fibers in the muscularis mucosa and lamina propria akin to a tree branching pattern.
Details of appendices received in formalin for routine evaluation.
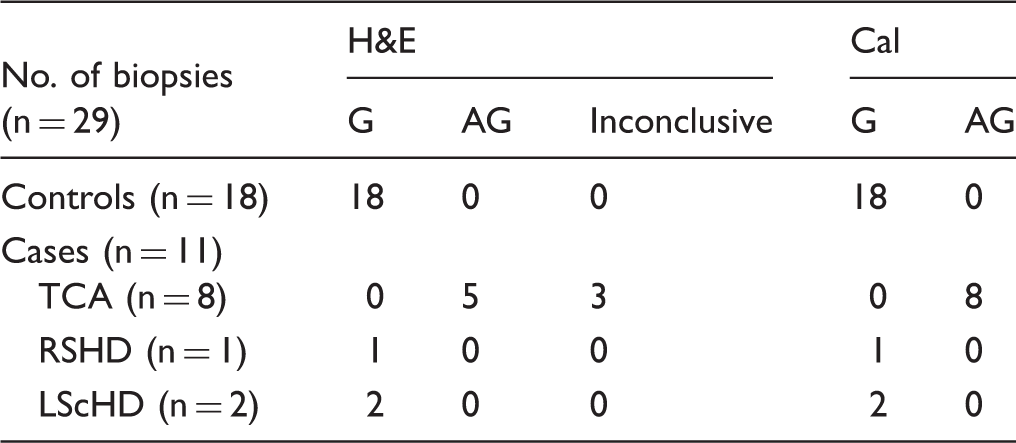
Note. One each of TCA and LScHD with skip segments are detailed in the text.
AG, aganglionic; Cal, calretinin; FS, frozen section; G, ganglionic; H&E, hematoxylin & eosin; LScHD, long segment colonic Hirschsprung disease; RSHD, rectosigmoid Hirschsprung disease; TCA, total colonic aganglionosis.
Appendices (fresh and formalin fixed) from normal controls and colonic HD—RSHD, LScHD
The H&E stained sections of the 28 controls (10 fresh frozen, 18 formalin fixed paraffin processed) were uniformly ganglionated in the myenteric plexuses (Figure 3(A)). Compared to their normal appearance in the rectum, these ganglion cell (immature) clusters appeared smaller and mimicked lymphocytes and plump endothelial cells. The ganglion cells were detected with difficulty at 10× magnification and needed confirmation at 40× in almost all cases, especially in the submucosal plexus. The AChE stain highlighted the ganglion cell clusters and an occasional nerve fiber (Figure 4(A)). Calretinin immunostaining demonstrated the intrinsic nerve fibers in the lamina propria and muscularis mucosa as well as the ganglia by staining both nucleus and cytoplasm (Figure 5(A)). The PGP 9.5 and NSE stained the nerve fibers and ganglion cells in the mucosa and submucosa. S-100 stained nerve fibers only. Compared to the ganglion cells in the rectum of the same cases or the appendices of older children, the ganglia in the neonatal appendices were smaller with proportionately smaller darker nuclei and lower nucleocytoplasmic ratio (Figure 6).
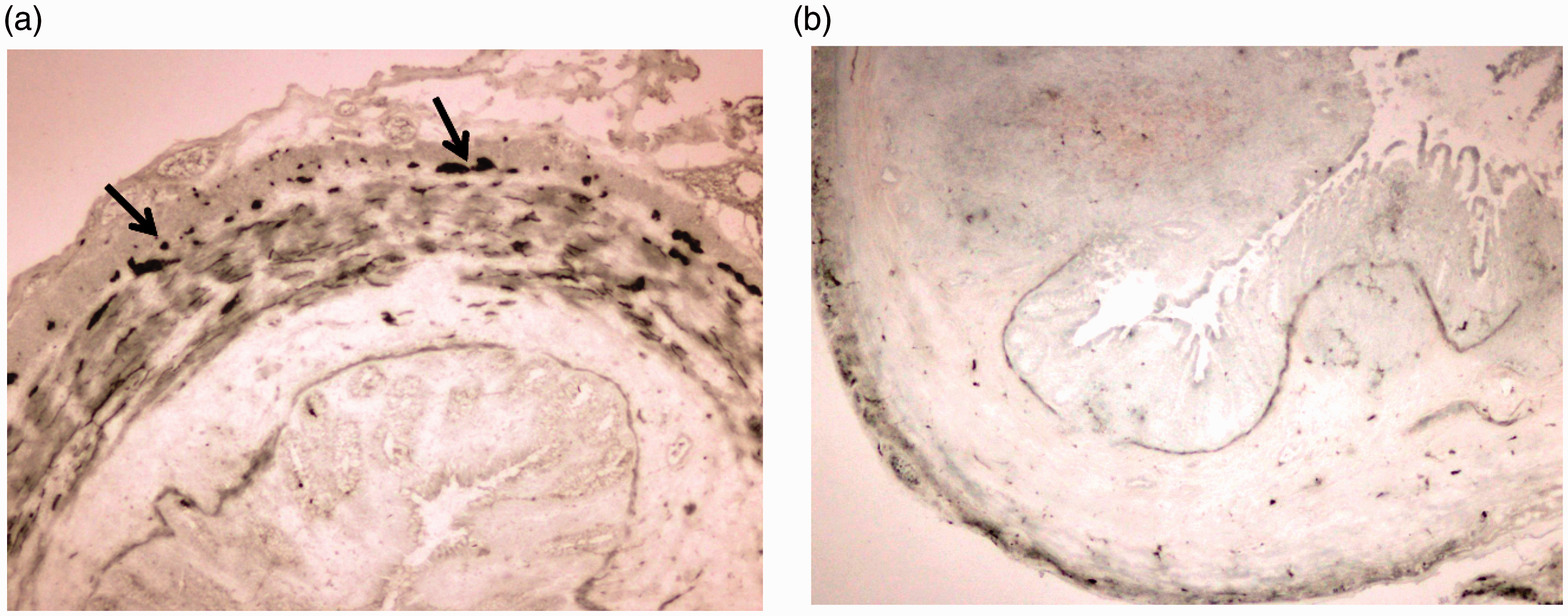
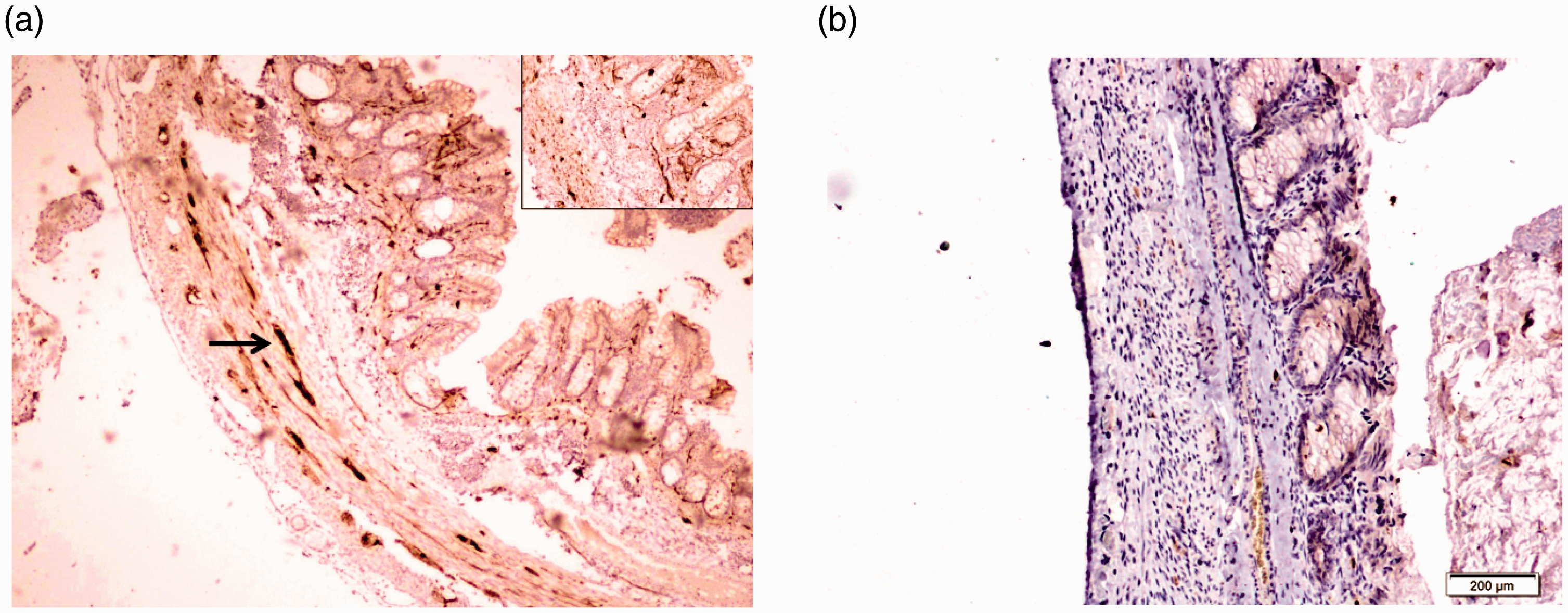
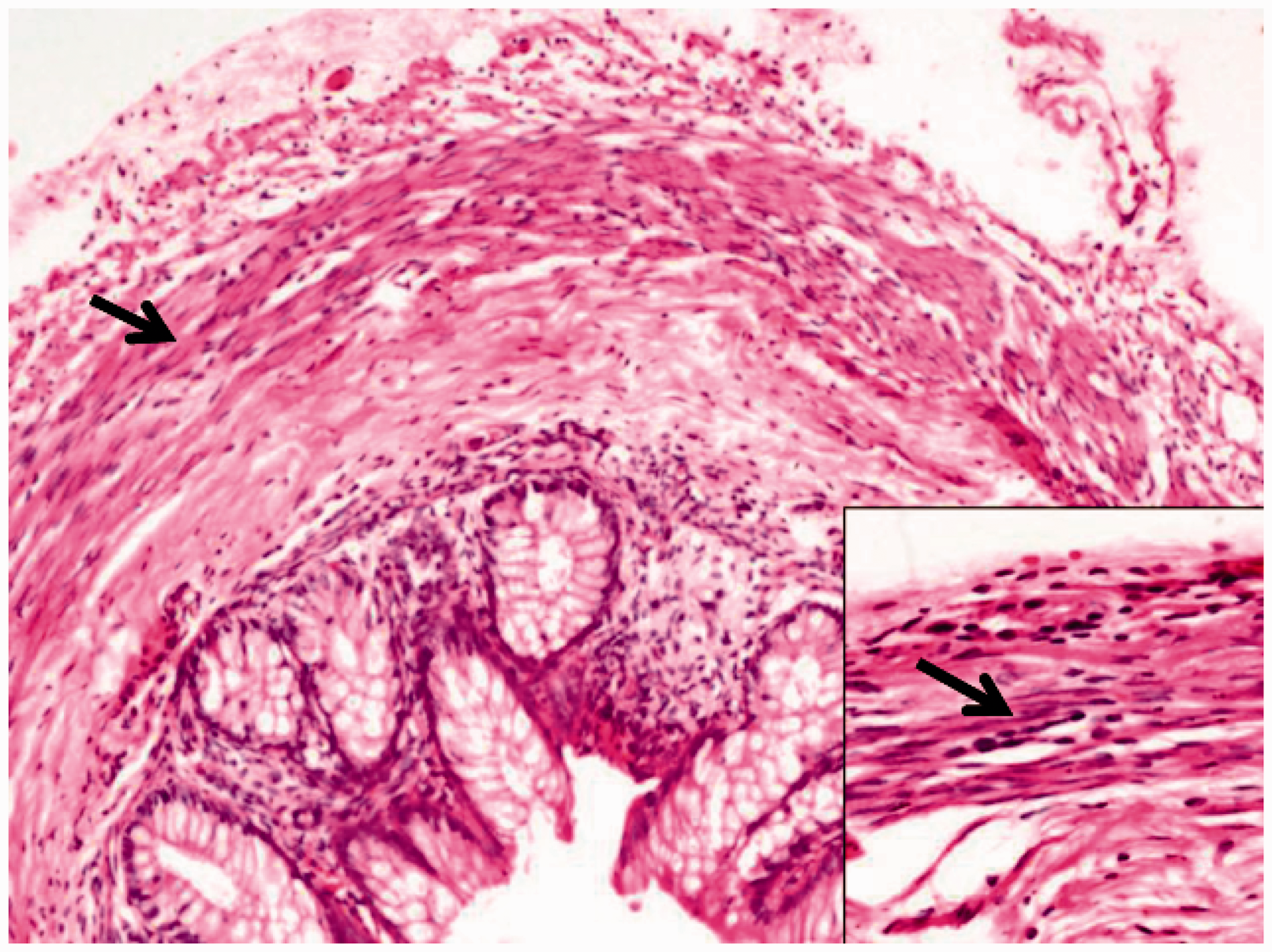
A, Normal appendix showing ganglion cell clusters (arrow) in the myenteric plexus (Frozen section, H&E stain ×400). Inset shows scanner view of wall of appendix (H&E stain ×40). B, TCA: Note the absence of myenteric plexus (arrow) in the appendicular wall (Frozen section, H&E stain ×400). Inset shows scanner view of wall of appendix (H&E stain ×40). A, Normal appendix: AChE stain on frozen section highlighting ganglion cell clusters in the myenteric plexus (arrow) and no fibers in the mucosa (×200). B, TCA with a “non reactive” myenteric plexus or a “bland” appearance without any enzyme activity (AChE stain ×200). A, Normal appendix: Calretinin stain highlighting ganglion cells (arrow) and fibers in the muscularis mucosa (×40). Inset shows the fibers in the muscularis mucosa (Paraffin section, ×200). B, TCA: Calretinin stain showing negative staining with neither fibers in the mucosa nor ganglion cells in the muscularis (Paraffin section, ×200). Appendix in a neonate showing immature ganglia (arrow) in the myenteric plexus (Frozen section, H&E stain ×40). Inset showing the immature ganglia (arrow) at higher magnification (×200).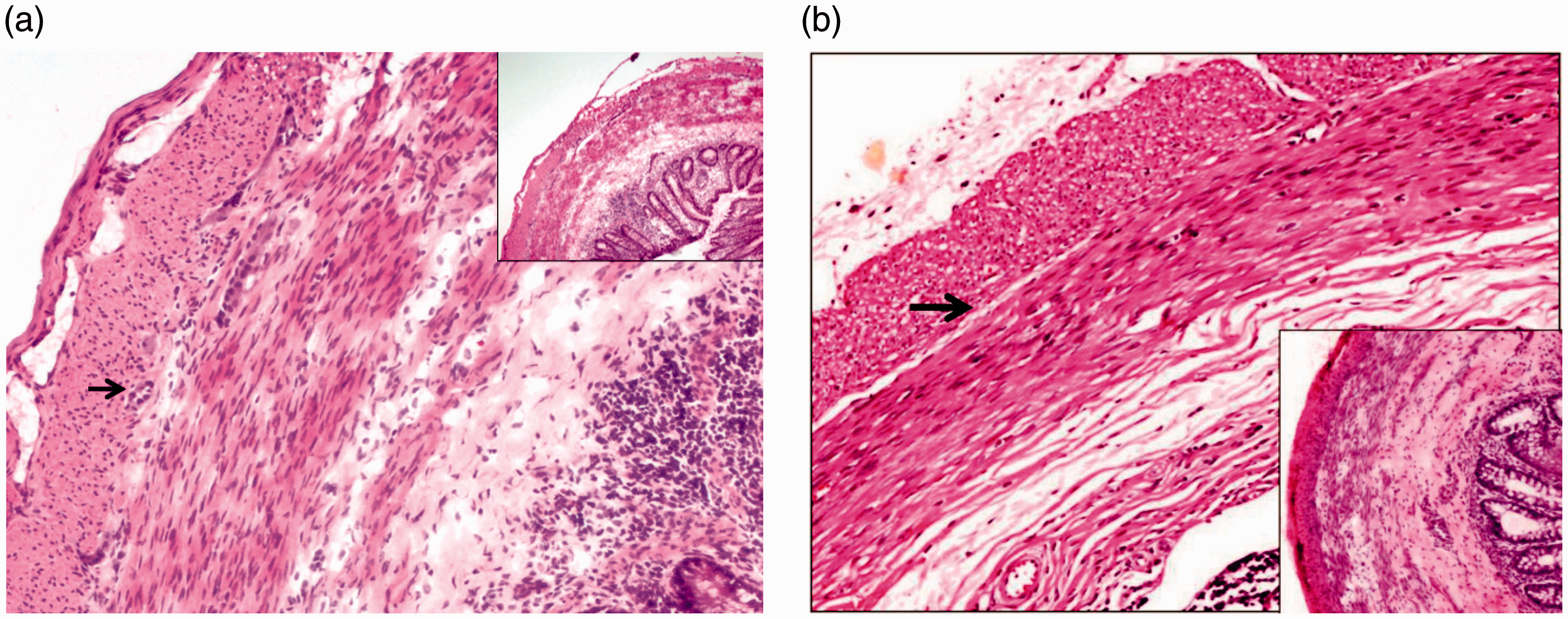
In one case of LScHD, there was a 2-cm skip segment disease distal to a functioning, transition zone colostomy (Figure 7(B)). Though seromuscular frozen section biopsies from the ascending colon and terminal ileum were normal, the appendix and 2 cm transverse colon just proximal to the stoma showed features of a transition zone on the paraffin sections with an occasional ganglion cell and a few hypertrophic nerve bundles
Schematic representation of the ganglionic–aganglionic areas in (A) skip segment aganglioosis in a TCA and (B) variable hypoganglionosis in a long segment colonic Hirschsprung disease. (red – aganglionic, green – ganglionic, stippled red and green – transition zone).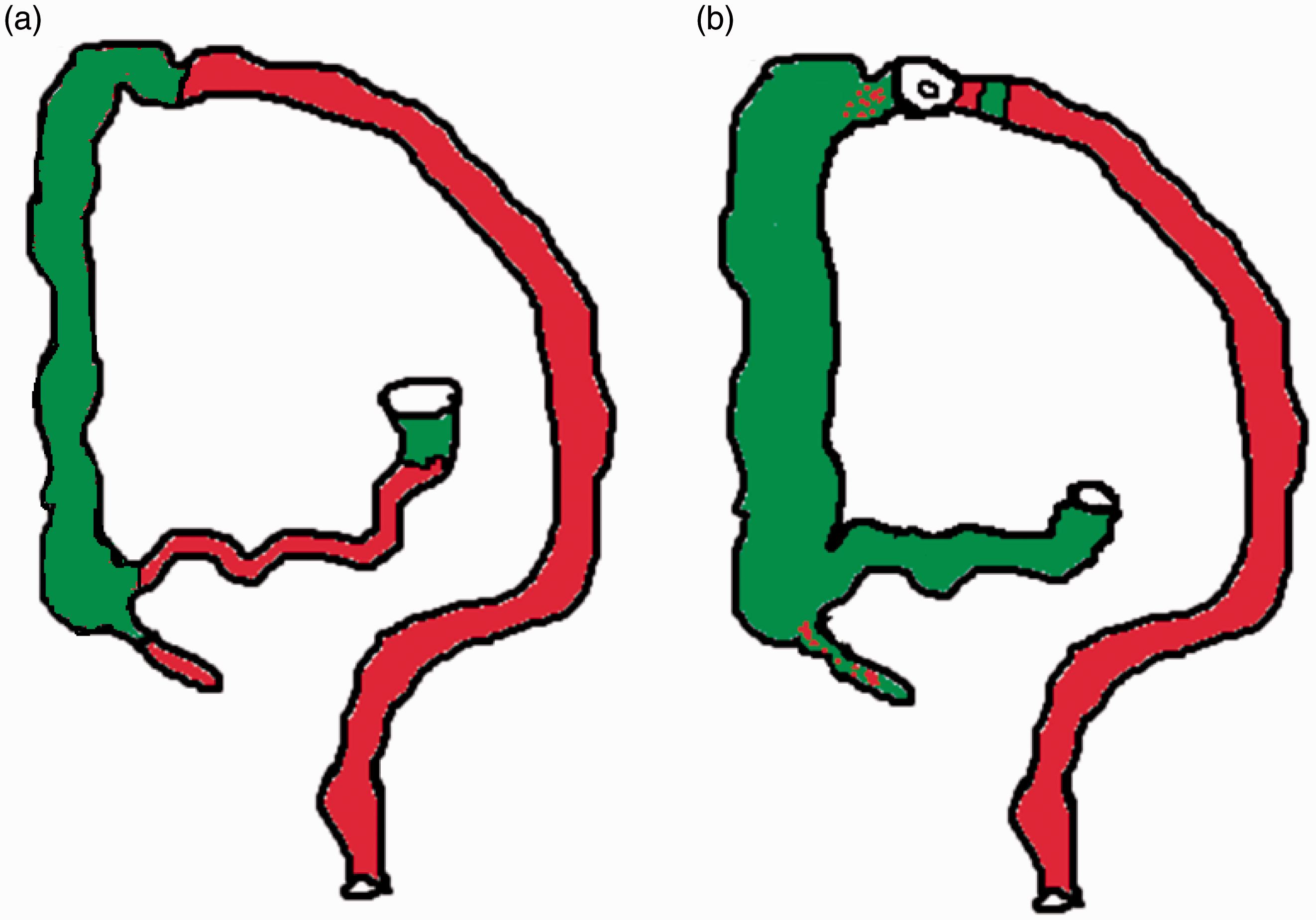
Appendices in TCA
In TCA, the appendices were small sized with inconspicuous lumen. The myenteric plexuses were indistinct with neither ganglion cells nor nerve bundles.
Frozen sections: Out of 5, 3 TCA showed no ganglion cells (Figure 3(B)) which was corroborated on paraffin sections and with immunohistochemical stains. In TCA, AChE stain showed a nonreactive appendicular wall with no cholinergic activity in its entire thickness (Figure 4(B)) unlike the other typical patterns (Pattern A/B/equivocal) seen in the corresponding rectal biopsy. 6
Paraffin sections
Of 8 cases of suspect TCA, the appendices were aganglionic in 5 and inconclusive in 3 with H&E. They were subsequently proved to be aganglionic with calretinin immunohistochemistry which showed neither ganglion cells nor any positive fibers in the muscularis mucosa and lamina propria (Figure 5(B)). The PGP 9.5 and NSE showed a few delicate nerve fibers and no ganglion cells.
In two cases of suspect TCA, the presence of “ganglion cells” on H&E stained frozen sections were proved to be erroneous by AChE, H&E stained paraffin sections, and immunohistochemistry. The biopsy showed dense inflammation and serositis due to perforation. The lymphocytes, macrophages, and plump endothelial cells lining the blood vessels (Figure 8) were mistaken for ganglion cells. An additional terminal ileal biopsy showed aganglionosis with no hypertrophic nerve bundles, confirming a diagnosis of TCA. A leveling stoma was performed after confirming normal circumferential innervation in a more proximal full thickness ileal ring biopsy.
Sections from appendices in different cases of TCA showing macrophage cluster (arrow) resembling immature ganglia (A), a group of endothelial cells (arrow) in muscularis (B) and a group of lymphocytes (arrow) in muscularis (C), all of which were mistaken for ganglion cells. (Frozen section, H&E stains ×200).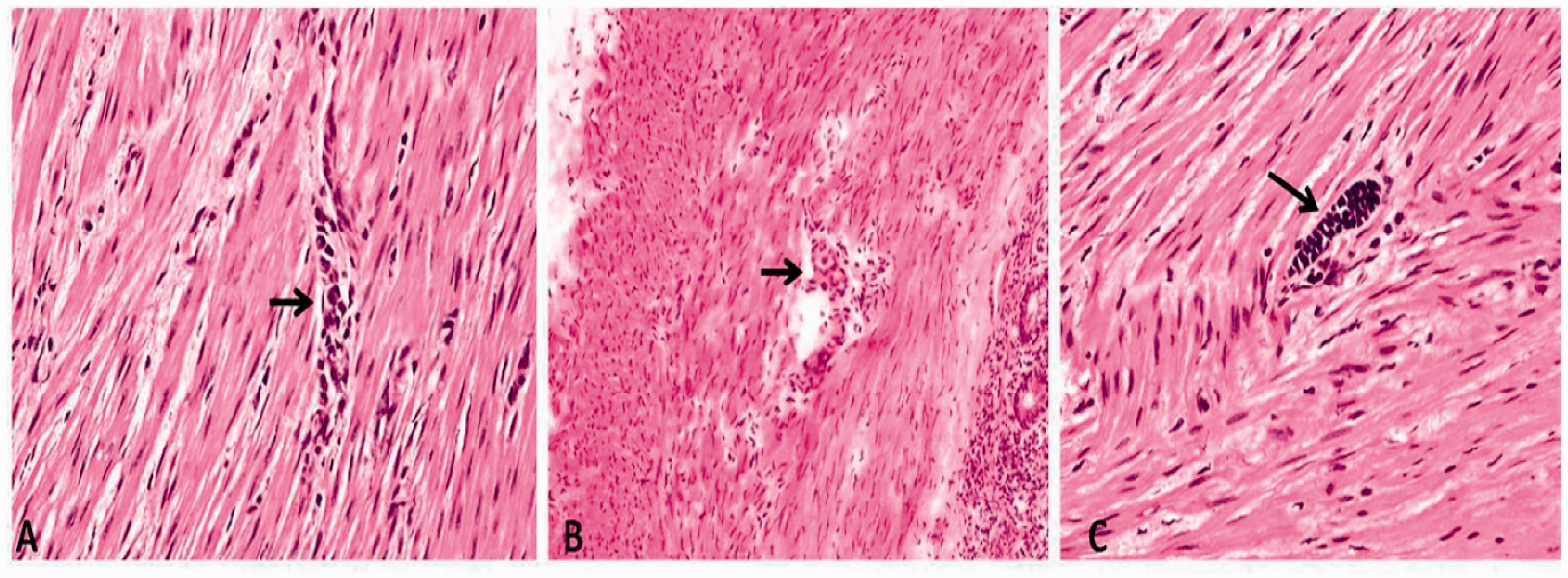
The solitary case of skip segment aganglionosis was in an 8-month infant with TCA (Figure 7). A section from the base of appendix showed an isolated ganglion cell (Figure 9); the ascending colon and hepatic flexure was contiguously ganglionic while sections from the distal colon (transverse colon to rectum), rest of the appendix and 15 cm of terminal ileum were aganglionic. The biopsy from the ileostomy site showed normal innervation (Figure 7(A)). Interestingly, calretinin immunohistochemistry on the base of the appendix showed no stainable nerve fibers in the lamina propria or in the muscularis mucosa and failed to identify the ganglion cells noted in the H&E.
An isolated ganglion cell (arrow) at the base of appendix of skip segment Hirschsprung's disease in TCA represented in Figure 7(A) (Paraffin section, H&E stain ×400).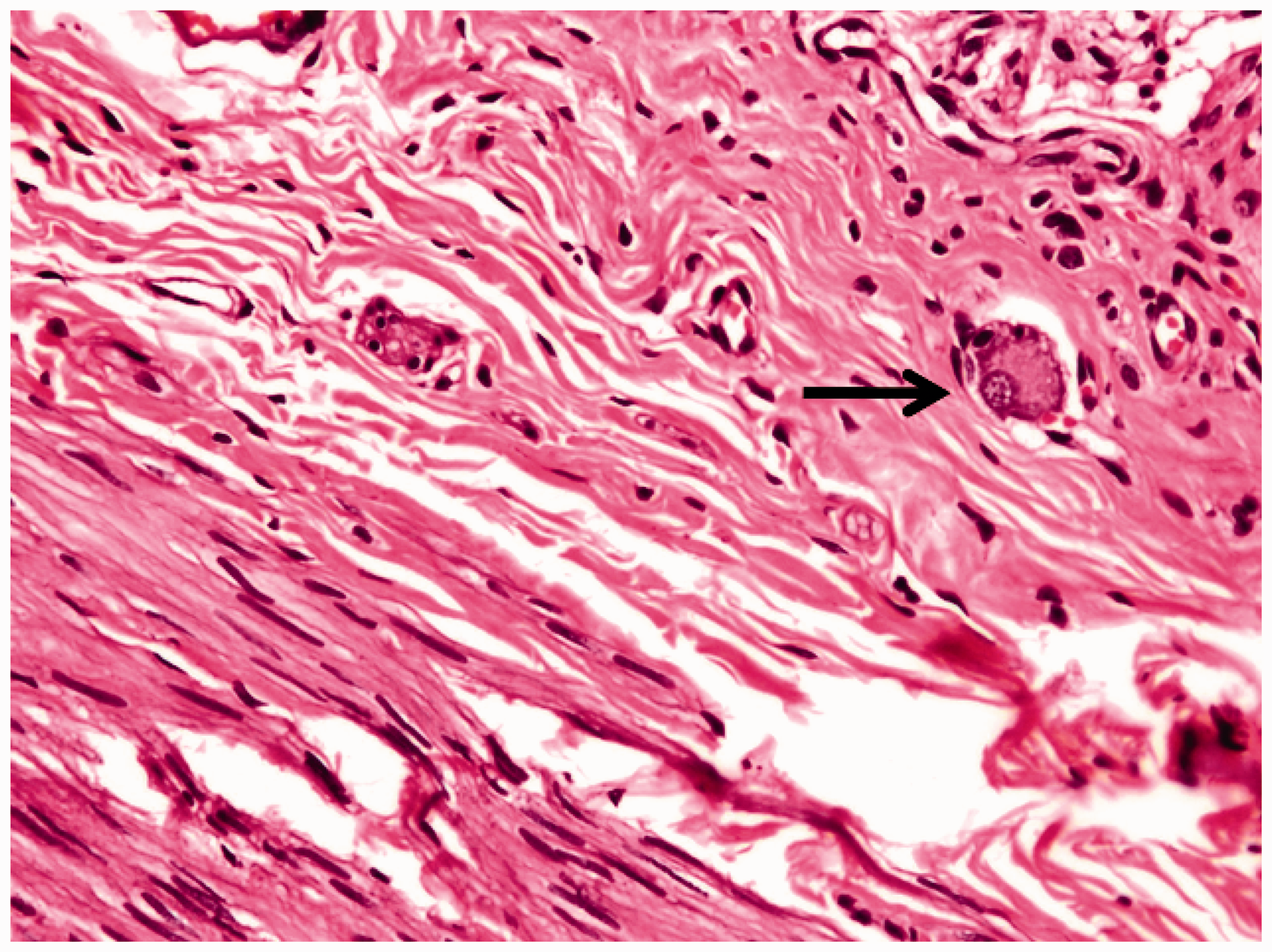
Discussion
It is a veritable challenge for a neonatal/pediatric surgeon to make a definite diagnosis of TCA based on radiological findings and surgical anatomy alone, and the diagnosis is clinched on the presence/absence of ganglion cells in the rectal and proximal leveling biopsies intraoperatively. Based on traditional embryologic craniocaudal migration of ganglion cells, an aganglionic appendix implied an aganglionic colon. Conventionally, in the clinical setting of a microcolon, an aganglionic appendix had been proposed to confirm a diagnosis of TCA,1,9 following which more proximal biopsies determined a level with normal ganglia. Though appendicectomy is a safe and technically easy procedure, not all observers concur on the diagnostic value of appendicular histology in TCA. Also, abnormal neural innervation of the appendix with a ganglionic distal colon has been reported by several authors.10,11 These observations about the possibility of skip segment disease involving the appendix question the reliability of appendicular morphology in mapping the extent of aganglionosis in HD, and the surgeon is wary about a false positive diagnosis of TCA.2,3 Similarly, many believe that evaluation of the appendix alone is unreliable for identification of ganglion cells in Hirschsprung disease.12–15 Even in the normal appendix, the ganglion cells are displaced irregularly into the circular and longitudinal muscle layers. 16 Recent insights into embryology in experimental avian and murine models postulate several additional pathways for ganglionic cell migration from the neural crest to the rectum 17 that do not involve the appendix. Thus, appendicular biopsy is not recommended for leveling of aganglionosis in TCA. At the outset, the authors concede the following limitations of the study: (a) the study cohort of cases (13 TCA) is modest as the entity is relatively uncommon, and recruitment was limited to the duration of the study period and (b) the final diagnosis was a consensus opinion after individual evaluation by three blinded pathologists. The following sections discuss the relevance of our results in the light of earlier observations.
Appendix in Normal Controls
Irwin 12 showed that the lowest number of neurons occurred in the cecum between the taenia. Kamoshita and Landing 13 stressed that the ganglion cell population was directly proportional to the amount of innervated muscle mass. Indeed, in comparison to the rectum, we have found it difficult to identify ganglion cells in the myenteric plexuses of normal appendices. The task was more tedious in neonates, often requiring confirmation at high magnification. Furthermore, the distribution of the ganglion cell/cluster in the appendicular tissue was highly variable. Submucosal ganglia in the appendix were particularly difficult to identify because of paucity and uneven distribution.
We have employed PGP 9.5, NSE, S-100, and calretinin 8 immunohistochemistry to confirm/disprove our preliminary observation on H&E. Of these, calretinin staining of the normally innervated appendix was consistent. This calcium-binding protein stained the ganglion cells and showed a fibrillar network in the lamina propria and muscularis mucosa in appendices of normal controls and rectosigmoid and long segment HD. In contrast, the other neural markers showed non-specific positive fibers and a few ganglion cells but were inconsistent.
We agree with the published literature that neonatal ganglion cells often appear small and immature with small dense nuclei and indistinct nucleoli. They are few and located far apart, unlike the clusters in older children. They appear smudged with indistinct cytoplasm mimicking lymphocytes.18–20 Indeed, these features multiply the difficulty in recognizing ganglion cells in appendix based exclusively on the morphology for a diagnosis of TCA in a neonate 21 with contiguous aganglionosis.
Appendix in Skip Segment Aganglionosis/Variable Hypoganglionosis
Our observation on appendicular histomorphology was similar in both normal controls and colonic Hirschsprung disease of rectosigmoid/long segment forms. In both the cases of a rare skip segment aganglionosis in a TCA and a variable hypoganglionosis in a LScHD, reliance on introperative evaluation of either appendix would have been misleading. The diagnosis was established by serial mapping of the ganglion cells in the terminal ileum, appendix, and colon on intraoperative frozen section and subsequent paraffin section evaluation. Such perplexing situations on frozen are overcome by a detailed examination of multiple cross sections of the entire appendix—the base examined separately from the rest. The skip segment aganglionosis involving the appendix (Figure 7(A)) in a TCA has been detailed elsewhere, 22 and earlier reports have involved different parts of the colon especially transverse colon (like the other case detailed here, Figure 7(B)), ascending colon, and cecum. 19
Appendix in TCA
The characteristic AChE positive extrinsic autonomic nerve hypertrophy associated with aganglionosis is seen in the rectal biopsy of RSHD, and to a comparatively lesser extent in TCA. It does not extend proximal to the splenic flexure and invariably the appendix and ileum is typically “non reactive” or “bland.” Like Shaw, 14 we found that the appendices in TCA had a uniformly “bland” morphology of the entire wall with neither ganglion cells nor nerve bundles in the submucosal or myenteric plexuses in H&E and AChE. In the presence of this typical “bland” picture, the diagnosis of TCA is relatively easy. Unfortunately, coexistent dense serosal inflammation, proliferating endothelial cells, lymphocytes, and macrophages can mimic ganglion cells 20 and cloud the decision-making. In the two false positive cases of TCA, lymphoid aggregates/plump endothelial cells were mistaken for ganglion cells on frozen H&E which led to an erroneous diagnosis .In retrospect, we realized that the endothelial cells lining blood vessels can be differentiated from ganglion cells in that the endothelial cells lie along the long axis of blood vessels which are disposed at right angles to the muscle fibers where as ganglia lie parallel to them; also the lumina of the vessels can be identified with a few red blood cells. Lane et al. 23 have cautioned against reliance on the histology of the appendix in the diagnosis of TCA.
As the “non reactive” or “bland” morphology described above is essentially a negative one that involves a clear anatomic visualization of the layers and plexii of the thin walled appendix, intraoperative diagnosis is unreliable and inadvisable. Here, a terminal ileal biopsy depicting a similar morphology clinches the intraoperative diagnosis of TCA conclusively and dictates proximal leveling and operative management. Moore 24 has also concurred on this issue.
Calretinin immunostaining to study the innervation of the appendix has not been hitherto reported in literature. In appendices that were received in formalin, the benefit of AChE staining was lost; complete absence of the nerve fibers on calretinin immunostaining was confirmatory of aganglionosis. Though the other neural markers stained a few random nerve fibers, they were similar to those seen in normal controls and non-specific.
Conclusion
The conclusive identification and characterization of ganglion cells in the appendix, a thin walled, narrow part of the gastrointestinal tract, is a practically difficult task especially in neonates. This focused study discusses problems encountered by the pathologist in the intraoperative interpretation of appendicular biopsies in different forms of aganglionosis.
We conclude that the frozen section evaluation of the appendix alone for a conclusive diagnosis of TCA is fraught with uncertainty. Though a “non reactive” or “bland” appendix on AChE/calretinin staining is compatible with a diagnosis of TCA, and the presence of ganglion cells in the appendix does not exclude TCA nor does its absence confirm a TCA because—(a) primarily, the identification and characterization of appendicular ganglion cells are difficult and (b) there is a rare possibility of a skip segment aganglionosis involving the appendix. Therefore, we propose that in all suspect cases of TCA with a microcolon, the following intraoperative frozen section evaluation is advisable: (a). evaluation of rectal mucosal biopsy for a preliminary diagnosis of aganglionosis, (b) evaluation of the terminal ileal biopsy sent simultaneously for confirmation of TCA, and (c) biopsy from the most distal dilated ileum after confirmation of TCA for “leveling.” Though rare, a skip segment aganglionosis in a suspect case of TCA must be identified for optimal surgical management. This stepwise diagnostic algorithm demands patience but is decidedly superior to a misplaced reliance on sole evaluation of appendicular morphology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research Society, St. John’s Medical College, Bangalore, India.