
Abstract
The autopsy is an integral part of the service of a large academic pathology department. Timely reporting is central to providing good service and is beneficial for many stakeholders, including the families, the clinical team, the hospital, and the wider community. The current study aimed to improve hospital-consented autopsy reporting times (turnaround time, TAT) by using lean principles modified for a healthcare setting, with an aim of signing out 90% of autopsies in 90 days. An audit of current and historical TATs was performed, and a working group incorporating administrative, technical, and professional staff constructed a value stream map documenting the steps involved in constructing an autopsy report. Two areas of delay were noted: examination of the microscopy and time taken to sign-out the report after the weekly autopsy conference. Several measures were implemented to address these delays, including visual tracking using a whiteboard and individualized tracking sheets, weekly whiteboard huddles, and timelier scheduling of clinicopathologic conference rounds. All measures resulted in an improvement of TATs. In the 30 months prior to the institution of lean, 37% of autopsies (53/144) were signed out in 90 days, with a wide variation in reporting times. In the 30 months following the institution of lean, this improved to 74% (136/185) (P < .0001, Fisher exact test), with a marked reduction in variability. Further, the time from autopsy to presentation at weekly clinicopathological rounds was also reduced (median: 73 days prior to lean; 63 days post-lean). The application of lean principles to autopsy sign-out workflow can significantly improve TATs and reduce variability, without changing staffing levels or significantly altering scheduling structure.
Introduction
Autopsies are one of the service cornerstones provided by a pathology department in large academic hospitals. They serve many functions, including determination of cause of death, documentation of the extent of disease, discovery of new clinicopathological entities, epidemiological monitoring of emerging disease patterns and trends, teaching and clinical audit purposes.1–6 However, prioritization of more time-sensitive matters often results in prolonged turnaround times (TATs) for autopsy reports. 7 Delays in autopsy report TATs results in frustration for families, physicians, peripheral hospitals, and the wider community. Thus, it is important to provide timely and accurate autopsy reports to maintain good service for all stakeholders.
The Hospital for Sick Children in Toronto, Canada, is a large academic pediatric hospital and serves a population of approximately 12 million throughout Ontario, as well as receiving national and international referrals. The Division of Pathology performs approximately 120 autopsies per year, with 70% being next-of-kin consented and 30% being performed under a Coroner’s warrant. Given autopsies performed under a warrant already had a Coroner’s-based workflow and quality assurance (QA) process, the current project focused on hospital-consented cases. Historically, there was no specific expectation for hospital-consented autopsy report TATs within our division, and many were delayed past the 90-day period. Lean management principles have been used to eliminate waste and improve efficiency in many areas of healthcare, including laboratory medicine8–10 and autopsies. 7 The objectives of this study were to improve the hospital-consented autopsy report TAT to 90% signed out within 90 days using lean management principles optimized for the healthcare setting.
Methods
As part of one author’s greenbelt lean training at the Hospital for Sick Children, the process of hospital-consented autopsy reporting and TATs was studied. Our division has 11 pathologists; the number of pathologists performing autopsies varied over the study period, but was between 4 and 6, with 2 pathologists doing the bulk of the autopsies. After meetings and discussions with relevant stakeholders (autopsy pathologists, physicians using the autopsy service, and hospital executive), the departmental aim was to improve the autopsy TATs so that 90% of reports would be signed out within 90 days or less, with a reduction in variability.
Terms and Definitions.
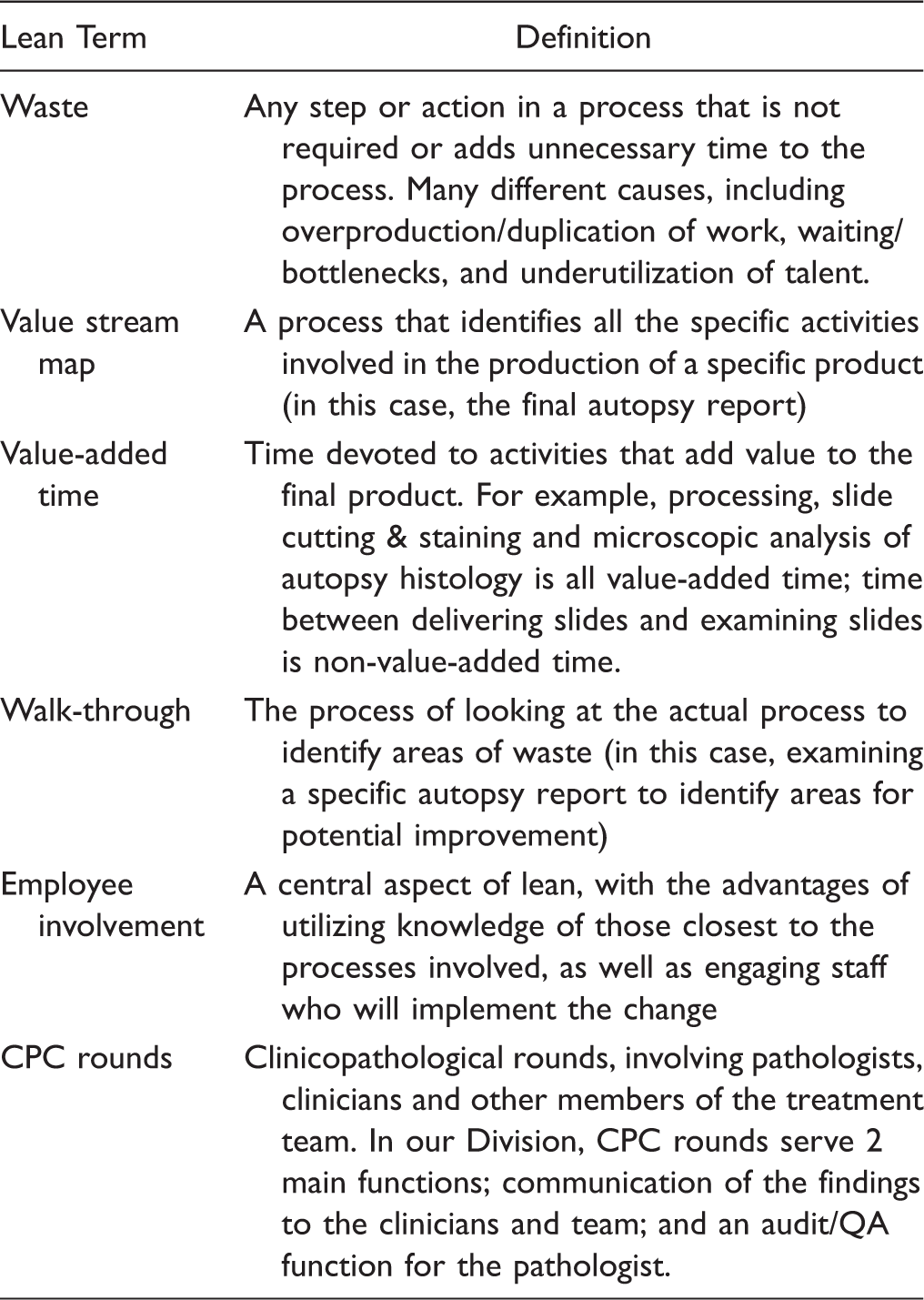
Note: CPC, clinicopathologic conference; QA, quality assurance.
Baseline metrics of autopsy TATs were obtained from 2011 to 2015, with the exception of time from clinicopathologic conference to sign-out (2012–2015); lean measures were implemented in July 2013. The total autopsy TAT was calculated from performance of the postmortem examination to final sign-out. Additionally, times from performance of the autopsy to the Pathology Division’s autopsy QA rounds, as well as the times from QA rounds to autopsy sign-out, were collected. Statistical analyses of the data were performed using Microsoft Excel 2007.
Results
Autopsy Numbers
Hospital consented autopsy numbers remained relatively stable over the study period, with an average number of 66 consented autopsies performed per year (range, 54–73).
Case Example and Value Stream Mapping
Areas of Waste/Delay in the Autopsy Sign Out Process, With Potential Causes.

Note: CPC, clinicopathologic conference.
Implementation of Lean Principles
By examining the main reasons for the delayed TATs (vide supra), potential avenues for improved TATs were examined via the application of lean strategies. After discussion with the pathologists performing the autopsies, the delay in examining the microscopic slides was thought to be due to 2 issues: competing priorities, such as other clinical priorities, specifically surgical biopsies and clinical rounds; and lack of a visible incentive to complete pending autopsy cases, such as reminder boards and tracking sheets. The delay in sign-out after presenting at CPC rounds was thought to be due to the time taken for incorporation of discussion and additional ancillary tests emanating from the CPC, delaying the sign-out by several more weeks (see Table 2 for summary).
Improvement Initiatives and Results.
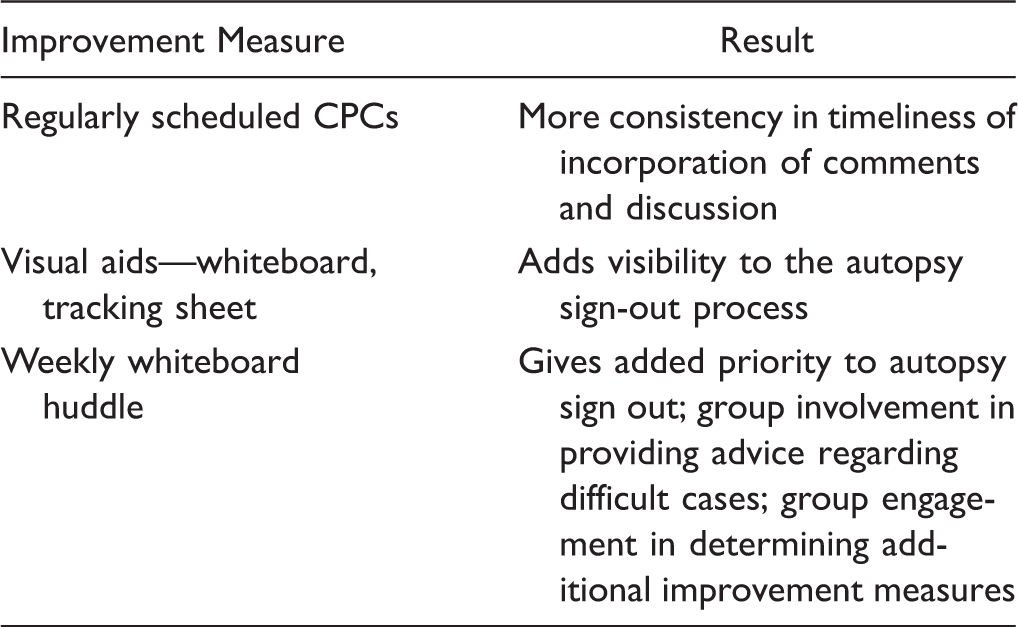
Note: CPC, clinicopathologic conference.

Example of an individualized tracking sheet was used for all hospital-consented autopsies. All key tasks are assigned responsible individuals and deadlines.
Measurable Improvements
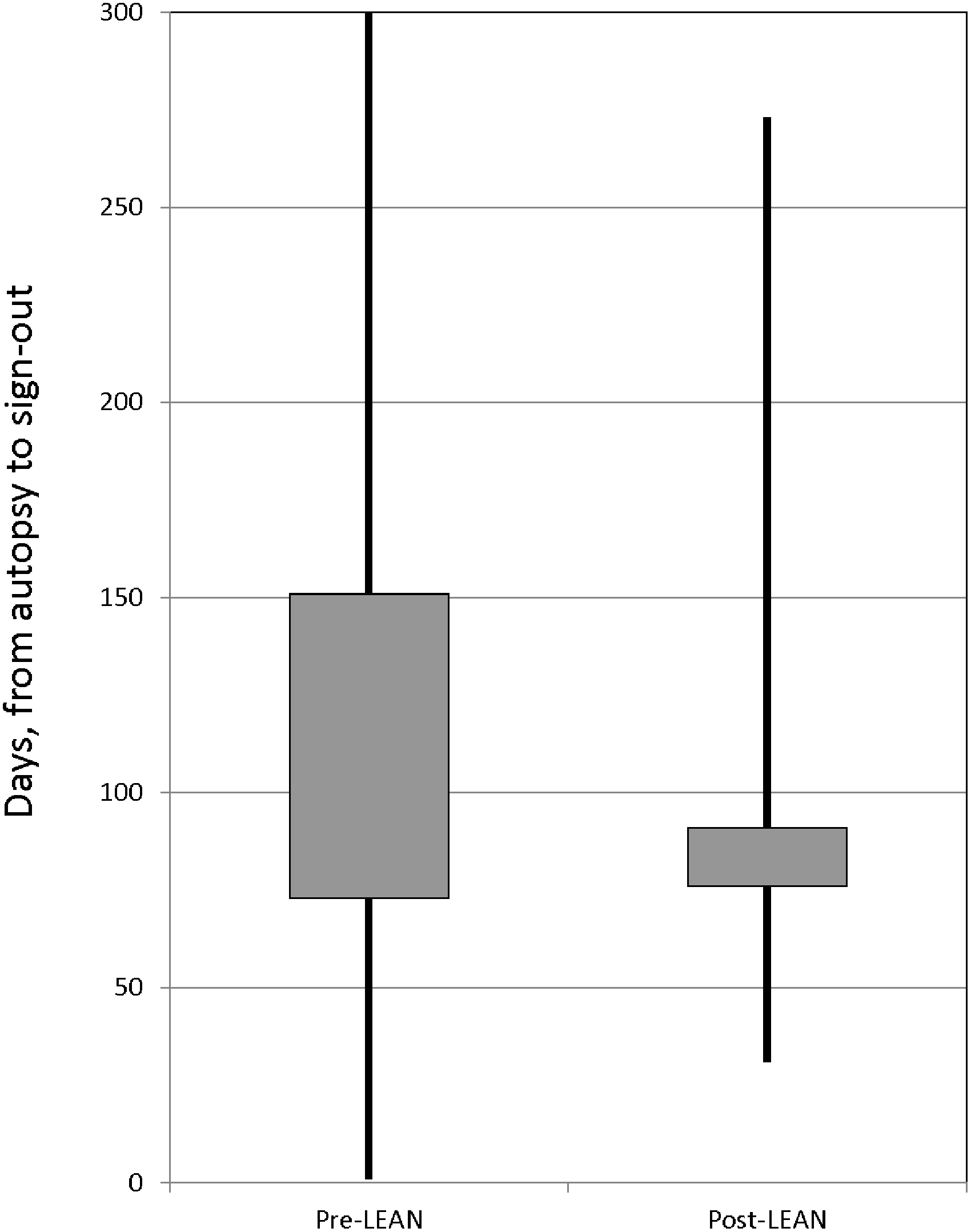
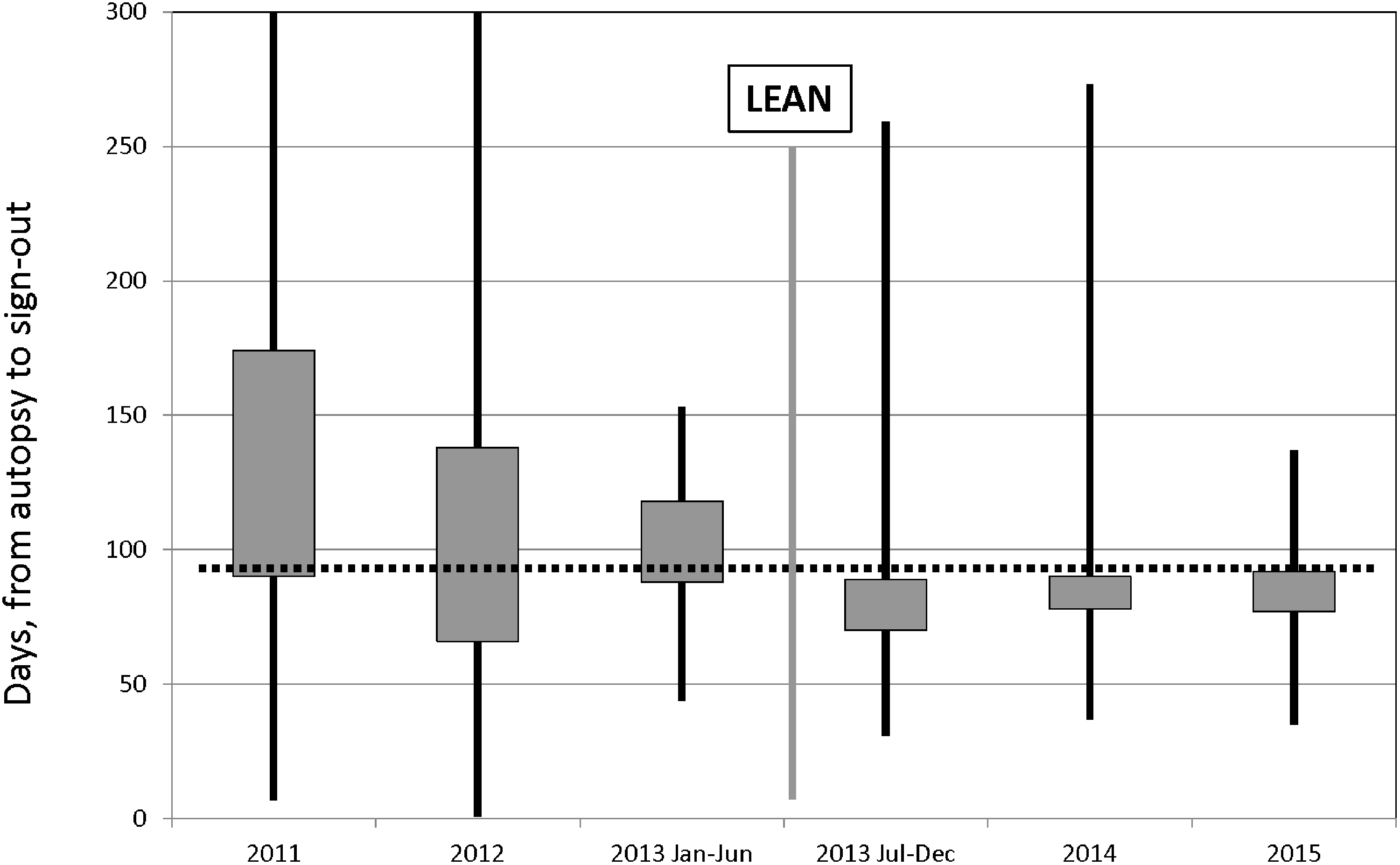
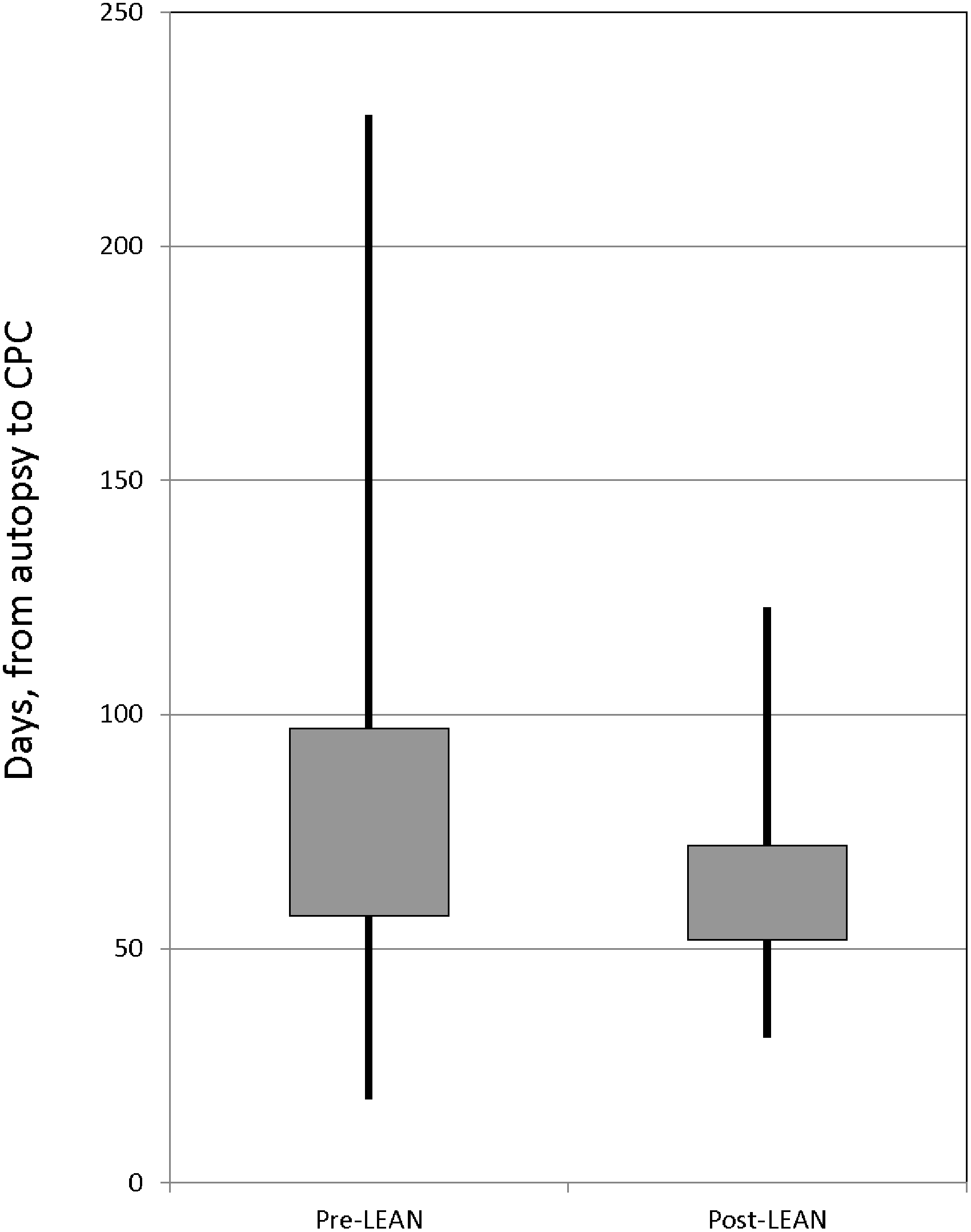
In the 30 months prior to the implementation of lean, 37% of hospital-consented autopsies were signed out within 90 days (median: 102 days). In the 30 months after the implementation, the rate has increased to 74% (median: 85 days) (Figure 2). Furthermore, the variability in the time to sign-out decreased considerably; the interquartile range (the value between the 25th and 75th percentiles) reduced (78 prior to lean; 15 post-lean) (Figures 3 and 4); time to CPC also improved (prior to lean: median 73 days, interquartile range 40 days; post-lean: median 63 days, interquartile range 20 days) (Figure 5). Time from CPC to sign-out (for 2012 – 2015) did not show a marked improvement; however, the variability markedly decreased (prior to lean: median 25 days, interquartile range 45 days; post-lean: median 21 days, interquartile range 20 days).
Percentage of autopsies signed out within 90 days pre- and post-lean implementation. The difference is significant (P < .0001, Fisher exact test). Box and whisker plot of autopsy sign out times pre- and post-lean. The boxes represent the 25th (lower edge) and 75th (upper edge) percentiles, giving an indication of variability. The straight bars represent the maximum (upper) and minimum (lower) sign-out times. The upper limit pre-lean was actually 870 days. The plots display the marked improvement in autopsy times and the marked reduction in variability. Box and whisker plots of autopsy sign-out times per year, with the vertical dashed line representing the implementation of lean. The improvement in sign-out times and consistency is apparent. Box and whisker plots showing the improvement in the timeliness and consistency in the scheduling of clinicopathological rounds for the autopsies.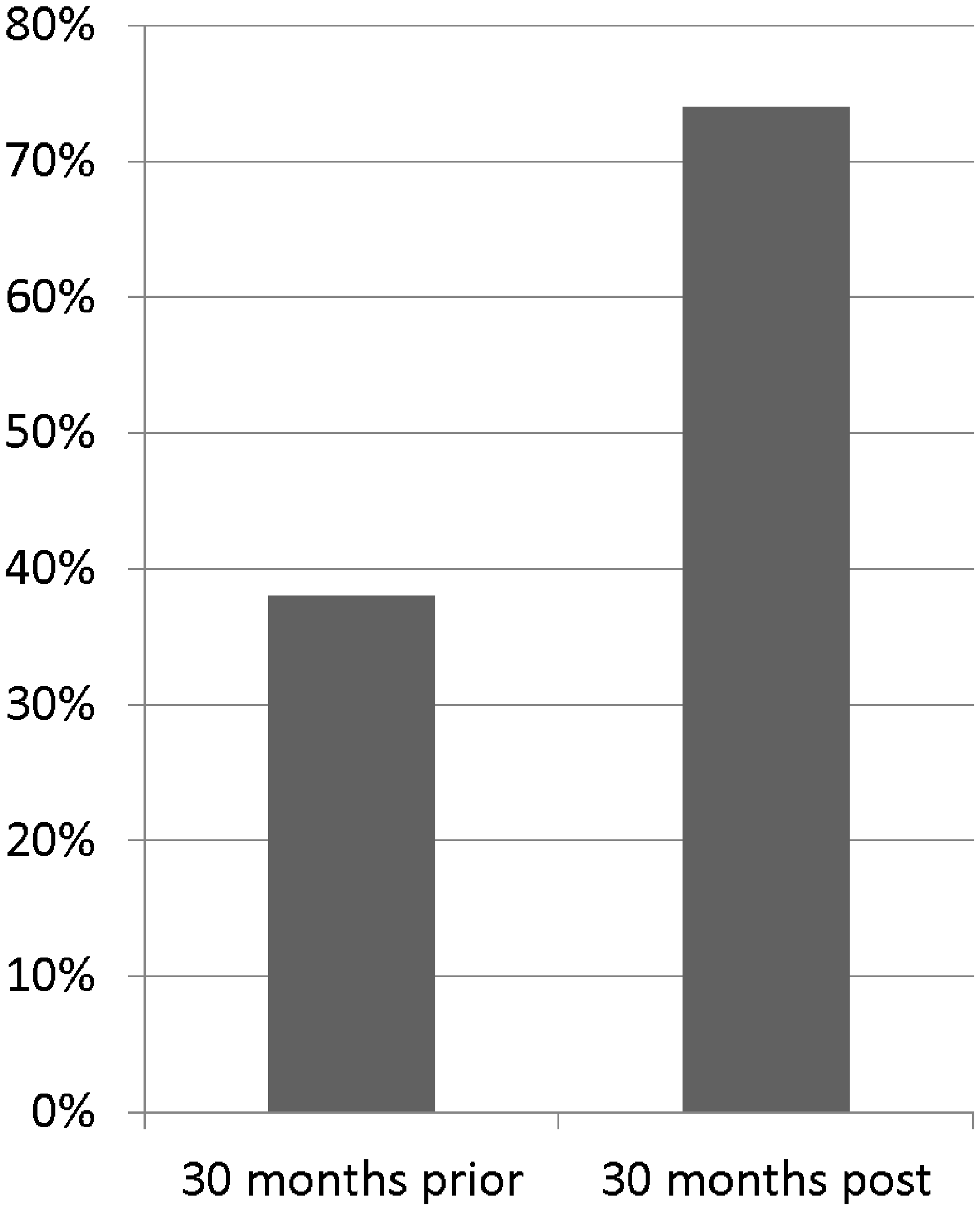
Certain aspects of the lean implementation resulted in “unquantifiable” aspects of improvement, including a reduction in overwork/duplication, improved relationships with clinical staff using the autopsy service, and an increased engagement of pathologists in improving autopsy TATs.
Discussion
Lean has been used in many aspects of healthcare, 11 including radiology,12,13 pediatric surgery, 14 outpatient clinics, 15 mental health, 16 primary care settings, 17 and laboratory medicine.7–10 Lean management principles are based on the Toyota Production System and have the central principles of elimination of waste and respect for the worker.18–20 Thoughtful application of such principles results in a more consistent and systematic approach to complex problems, resulting in a more efficient delivery of care. In the current study, our application of the lean management system allowed us to minimize waste in our autopsy reporting process, resulting in significantly reduced and more consistent TATs for the autopsy report.
The first step in our improvement project was to engage all stakeholders. Clinicians were made aware of our attempts to decrease autopsy reporting TATs and provided to us the key metric of aiming for 90% of cases signed out within 90 days. Other members of the team were also engaged in the process, and contributed by building a consensus for targeting certain areas of waste. Further, all pathologists were able to see the steps involved in the reporting process and potential areas for improvement in real time. One of the benefits of the value stream map was to reduce duplication. For example, due to delays in reporting, tasks such as summarizing the clinical history and reviewing the microscopy were often repeated; however, by utilizing the tracking sheet, pathologists were able to perform each task once and within certain timeframes. Furthermore, widespread engagement ensured the change process was a transformative one, with each member invested in the outcome.
Two major areas of waste were identified: time to review the autopsy microscopy and time to sign-out after presenting at our weekly CPC/audit rounds. Three measures were implemented to address both major areas of delay, specifically increasing the visibility of outstanding autopsies, regular discussions around outstanding autopsies, and timelier scheduling of weekly CPC/audit rounds. After the implementation of all 3 measures, the autopsy TATs improved significantly, with the percentage of reports signed out within 90 days improving from 37% to 74%. Consistency also increased, with a marked reduction in the interquartile range (78 days to 15 days).
However, we are still short of our ultimate goal of 90% of reports completed within 90 days. Surveying our staff, continuing issues include staff absences and vacations, staff scheduling issues, and CPC scheduling difficulties, some of which were identified as issues in a previous study. 7 Given the additional challenges, we are currently undergoing an additional cycle of improvement measures (“second cycle PDSA”) and are implementing increased use of pathologists’ assistants in creating report templates, increased use of residents in planning and presenting CPCs, and automated reminders to pathologists of outstanding autopsy reports.
The current healthcare climate demands increased efficiency, while maintaining fiscal responsibility and stable staffing resources. Lean management principles, when thoughtfully applied to our autopsy sign-out process, have helped to identify areas of waste and provided insight into sources for improvement.
Footnotes
Acknowledgments
The authors wish to thank the Continuous Improvement Team at the Hospital for Sick Children, specifically Michael Hartman, Shiraz Bajwa, Travis Beamish, David During and Daniele Ingleton, for major support and assistance during the initiation and implementation of the project. The authors extend gratitude to the staff of the Division of Pathology for supporting this initiative.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.