
Abstract
We have identified 9 pregnant patients who were diagnosed with malignancy and initiated chemotherapy during their second trimester (cervical cancer [n = 3], leukemia [n = 3], breast cancer [n = 2], and Hodgkin’s lymphoma [n = 1]). Five of the patients’ placentas were small for gestational age (SGA). Pathologic examination revealed inflammatory changes in 4 of the placentas: 2 from the SGA placentas and 2 from non-SGA placentas. Examination revealed 3 placentas with villitis of unknown etiology (VUE) and 1 with intervillositis; all were negative for bacterial and viral cultures and by immunohistochemical (IHC) stains. In the VUE cases, IHC stains showed positivity of CD25+/FOXP3+ with focal positivity and CD3 and CD4 IHC were focally to strongly positive. Literature suggests that the use of chemotherapy during pregnancy can be detrimental to both the mother and the fetus; however, there has been limited focus on the effects of chemotherapy on the placenta. We suggest that the inflammatory process noted in the placentas is due to chemotherapy-induced toxic effects.
Keywords
Introduction
Chemotherapy during pregnancy can lead to various maternal complications including increased risk of infection, spontaneous abortions, maternal immunosuppression, anemia, and neutropenia. 1 Neonatal complications include anemia and neutropenia secondary to in utero myelosuppression. 1 When considering the use of chemotherapy during pregnancy, the survival of the mother is weighed against the potential harm to the fetus. 2 Chemotherapeutic agents are typically classified as U.S. Food and Drug Administration (FDA) pregnancy category C, potentially harmful to the fetus, or FDA pregnancy category D, harmful to the fetus.3,4 Low-molecular weight and highly diffusible drugs, such as lipid soluble drugs, should be avoided due to the risk of these agents crossing the placental barrier.2,5
The effects of chemotherapy use during pregnancy to the fetus have been studied; however, its effects on the placenta are not well documented. While analyzing placentas from 9 mothers who underwent chemotherapy during pregnancy, we noted some interesting changes in the histopathology. Previous observational studies in humans and experimental animal studies investigating the effects of cancer on the placenta have reported that the placenta is relatively resistant to cancer cells because the trophoblasts act as a protective barrier. 6
In our study, we report 3 placentas with villitis of unknown etiology (VUE) and 1 with intervillositis with negative results for bacterial and viral cultures and immunohistochemical (IHC) stains. In the VUE cases, IHC stains showed increased numbers of CD25+/FOXP3+ with focal positivity and CD3 and CD4 IHC were focally to strongly positive (Figure 1) compared to our normal controls. To our knowledge, no previous studies have specifically discussed placental inflammation in women undergoing chemotherapy during pregnancy. We hypothesize that the reported changes in placental pathology in our cases can be attributed to the use of chemotherapy during pregnancy. Chemotoxicity from the treatment may lead to the interruption of maternal–fetal tolerance leading to inflammation of the placenta.
IHC 400×. A, CD25 shows strong positivity. B, FOXP3 shows positivity in the stromal cells. C and D, CD3 shows focal and strong positivity, respectively. E and F, CD4 shows focal and strong positivity, respectively.
Methods
After obtaining institutional review board approval, we searched our files to identify any cases of chemotherapy use during pregnancy. Nine identified cases were reviewed by 2 pathologists for the maternal history, infant information, and placental examination including available bacterial and viral cultures at the time of the study. The placental sections were examined using hematoxylin and eosin (H&E) stains and IHC panels including fusobacterium, mycobacterium, tuberculosis, syphilis, and toxoplasma that included positive and negative controls. Polymerase chain reaction (PCR) that included cytomegalovirus, herpes simplex virus, human papillomavirus, and varicella-zoster virus to identify potential viral etiology was performed on the 4 cases with inflammatory changes only at the time of the study. In addition, IHC was performed on VUE cases for specific immune cell subsets CD3, CD4, CD25, and FoxP3, and a normal placenta was used as a control.
All placentas are examined using the institutions protocol. This protocol includes a minimum of 5 sections; from cassette A, 3 sections of the cord (proximal, middle, and distal); cassette B, 3 sections with ruled membrane with margins; cassette C, 3 full-thickness central sections; cassette D, 3 full-thickness para-central sections; and cassette E, 3 full-thickness para marginal sections. Then any observed gross abnormalities are to be submitted in cassettes F, G, H, and so on. With this meticulous protocol, it was ensured that adequate sampling of the placentas was performed. The criteria used for the placental SGA was referenced according to tables by Dr Perrin and Fetal Placental ratios by Gestational age by Dr Benirchke.
Results
Patient Prior Pregnancy History.
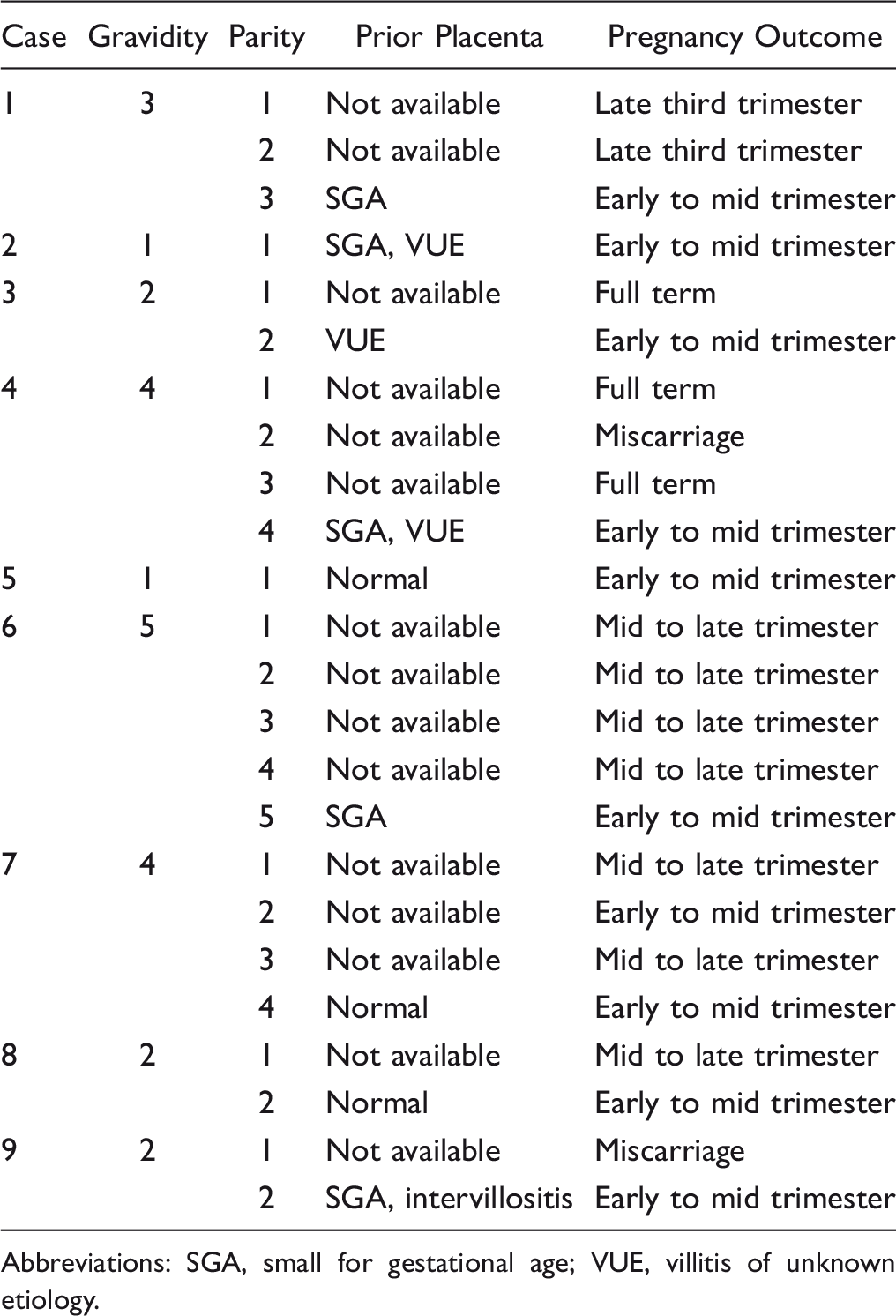
Abbreviations: SGA, small for gestational age; VUE, villitis of unknown etiology.
Patient Information and Placental Pathology.
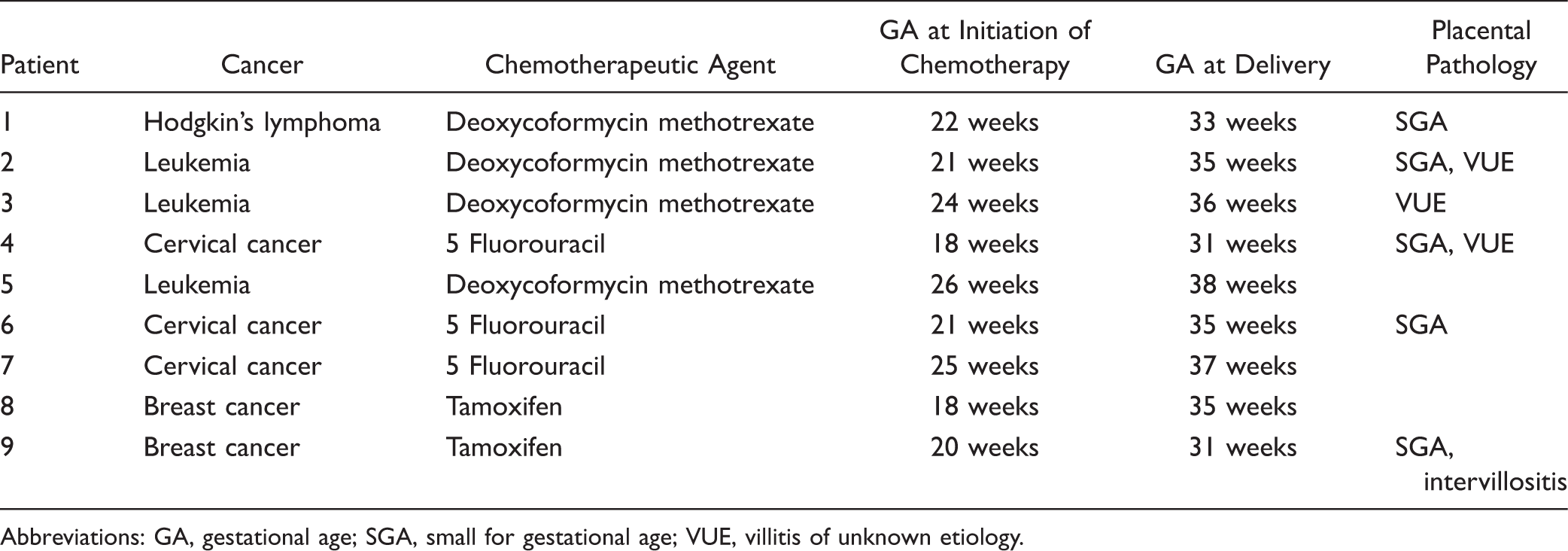
Abbreviations: GA, gestational age; SGA, small for gestational age; VUE, villitis of unknown etiology.
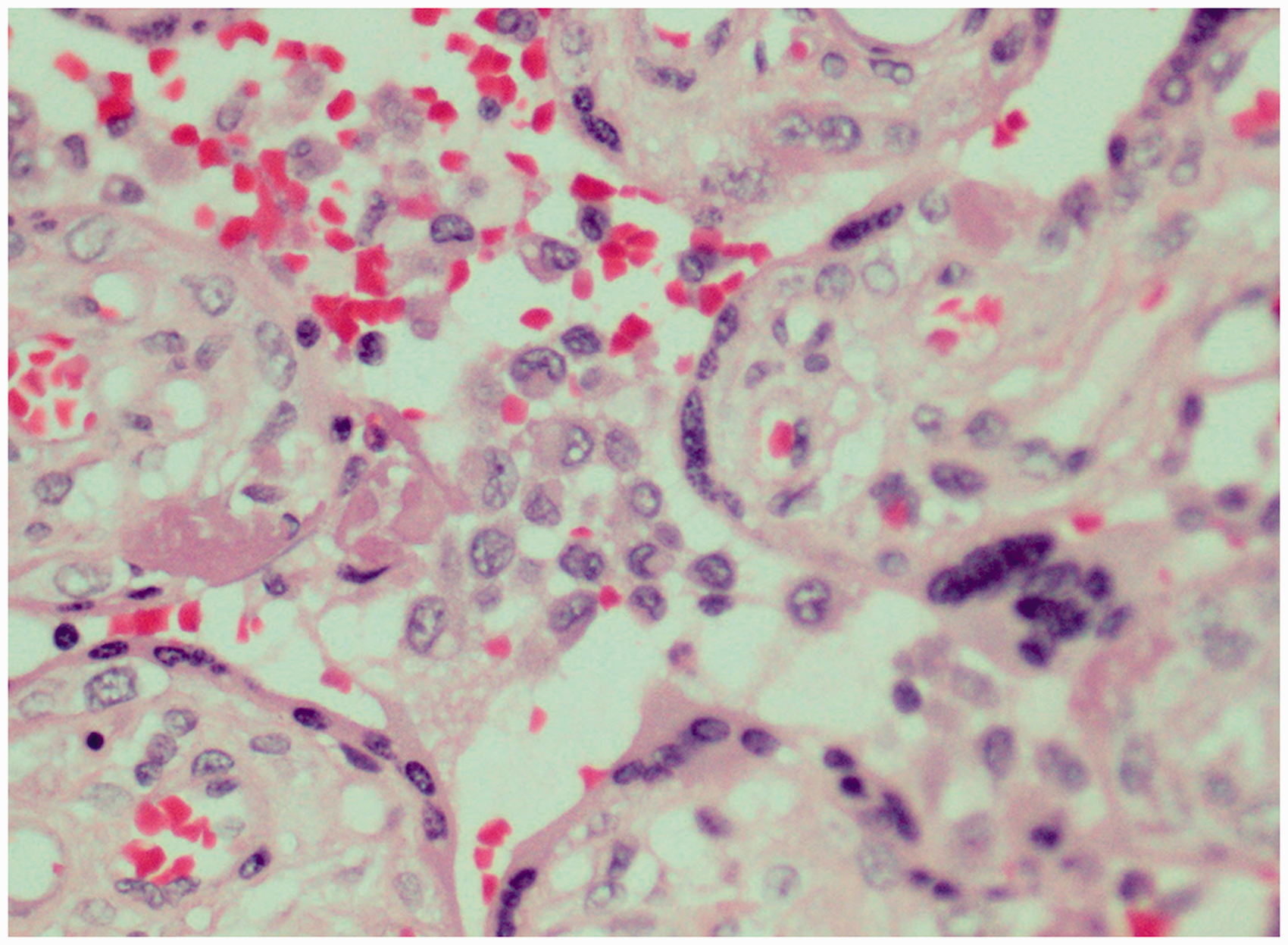
All patients were diagnosed and initiated chemotherapy in their second trimester. The stage of the cancer in the mothers was hard to assess due to the old retrospective chart review. Five infants presented with intrauterine growth restriction (IUGR) and their placentas were SGA. The other 4 infants were below the mean size for gestational age (30–40th percentile). There was no significant evidence of distal villous hypoplasia, accelerated maturation, decidual atherosis, thrombosis, calcification, villous stromal-vascular karyorrhexis, stem villous vascular obliteration, infarction or failure of physiologic conversion, and so on compared to placentas from patients without IUGR. Results of the viral and bacterial cultures and IHC stains were negative. Additional PCR were negative for any bacterial or viral etiology. In all cases of VUE, IHC showed positivity of CD25+/FOXP3+. In addition, CD3 and CD4 IHC were focally to strongly positive (see Figure 1). Pathologic examination revealed 3 cases of VUE (Figure 2), 2 from SGA placentas, and 1 case of severe intervillositis (Figure 3). In the 3 cases of VUE according to the Amsterdam criteria, the inflammatory lesions were high grade. The lesions were diffuse in cases 2 and 3 and patchy in case 4. Case 9 displayed massive intervillositis seen in over 50% of the placental sections examined.
H&E, 200×: section of the placenta showing a prominent villitis with diffuse villous necrosis. The lesions were high grade. H&E, 400×: section shows intervillositis with aggregates of macrophages in the intervillous spaces.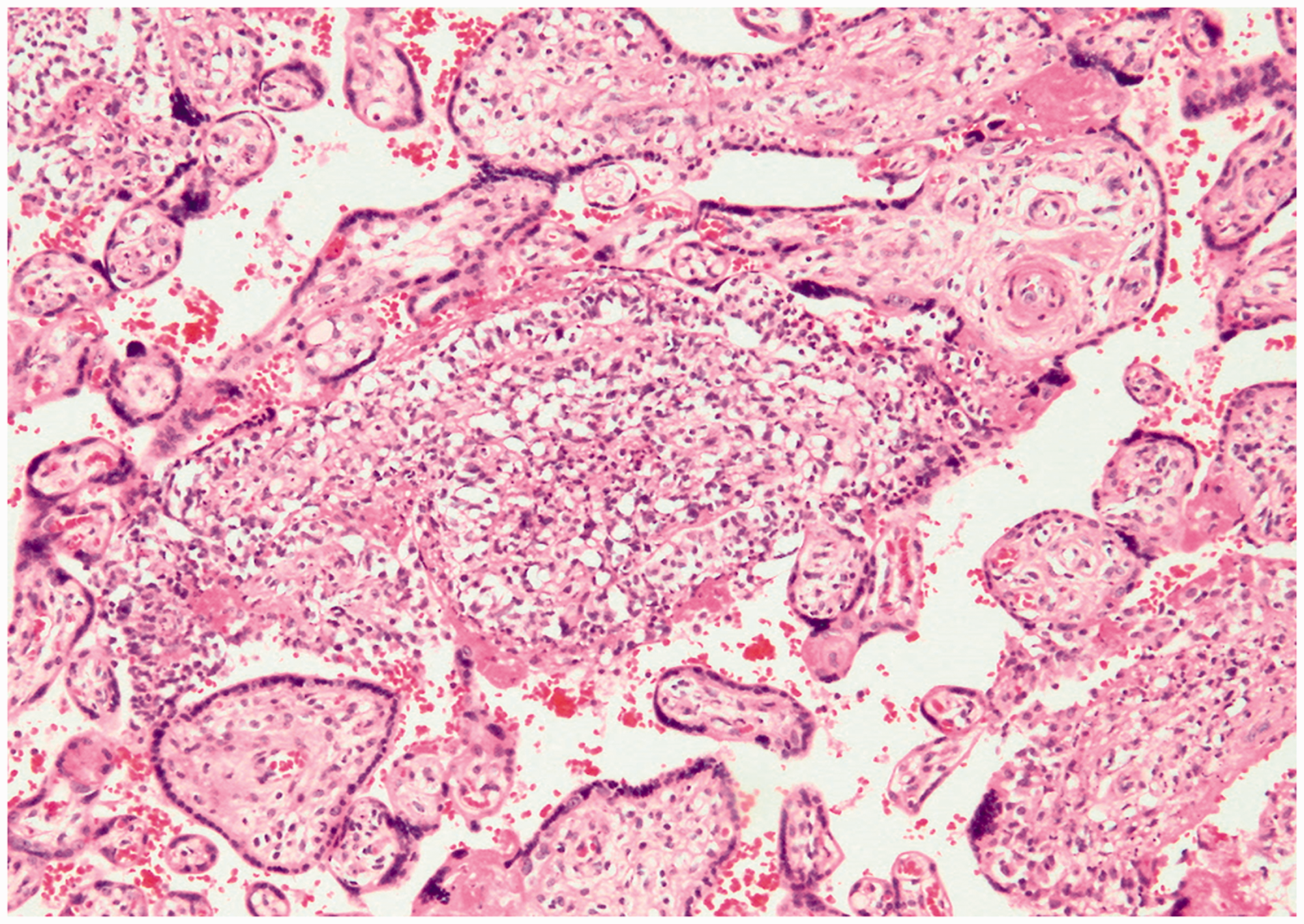
According to our institutions protocol, there is a minimum 10-year follow-up of the infants if the mother received chemotherapy during pregnancy. The infants’ charts showed no increased incidence of infection compared to children whose mothers did not have immunosuppressive therapy during pregnancy. Their growth was within normal limits, and they demonstrated no neurocognitive disorders. No evidence of malignancy was seen in these children.
Discussion
The past several decades have seen a shift in beliefs and theories about the maternal immune system during pregnancy. More than 50 years ago, the prevailing theories described the fetus as a semiallograft that escaped maternal rejection. 7 However, numerous recent studies characterize the maternal immune system during pregnancy as one that is modified by the developing immune system of the fetus and one that responds differentially to threats depending on the stage of pregnancy. 7 The Danger Model, introduced by Matzinger and adapted to pregnancy by Bonney, is the major alternative to the classic models of maternal tolerance of the fetus.8,9 The model proposes that T cell activation is not reliant wholly upon recognition of nonself, but it is truly reliant upon recognition of “danger” expressed in fetal tissues and the decidua through necrosis and dysregulation of critical metabolic processes. 8 Therefore, the Danger Model proposes that maternal T cell recognition of fetal antigens in the absence of continued danger signals will lead to the death of maternal T cell populations rather than these cells causing fetal harm. 8
Just as beliefs about the maternal immune system during pregnancy have shifted to a more complex model, what is known about the placenta and its role in immune regulation has also shifted. Recent observations indicate that the placenta functions to regulate traffic between the mother and a fetus rather than bar it. 10 Furthermore, the fetal/placental unit is now thought to act as an immunologic organ of its own eliciting various immunological responses and contributing to pregnancy outcomes. For instance, the presence of placental infection may stimulate the production of inflammatory cytokines such as tumor necrosis factor-α, interferon-γ, interleukin-12, and interleukin-6 and activate the maternal immune system leading to placental damage. However, viral infection in the placenta may trigger a milder inflammatory response that would involve an immune response from both the mother and the fetus. 10 Considering these studies, it is unsurprising that the placenta may play an important role in regulating the immune response to chemotherapeutic agents during pregnancy. These responses may potentially lead to the compromise of both the structural and immunologic integrity of the placenta.
Chemotherapy during pregnancy has been linked to major fetal malformations including hydrocephalus, cardiac anomalies, syndactyly, and periventricular leukomalacia.2,11 Pregnant women diagnosed with malignancy are recommended to wait until the second or third trimester, if possible, to allow fetal maturity and minimize risk of spontaneous abortions, fetal death, and fetal malformation.5,2 However, exposure to chemotherapeutic agents during the second and third trimesters can increase risk of IUGR and low birth weight. 2
Long-term effects of chemotherapy during pregnancy on children have been previously investigated. Amant et al. assessed the neurocognitive and cardiac outcomes of 70 children whose mothers underwent chemotherapy during pregnancy and found that the children’s outcomes were no different than the general population’s at the time of their follow-up. 12 Aviles et al. also conducted long-term follow-up studies on children whose mothers underwent chemotherapy during their first trimesters of pregnancy that demonstrated normal child development and no physical or psychological abnormalities even after 22 years of follow-up. 13 In addition, the children displayed no increase in childhood infections compared to children whose mothers did not undergo chemotherapy during pregnancy.13,14
Abellar et al. examined 13 placentas from mothers who underwent chemotherapy during pregnancy. Results from their study demonstrated that women who received DNA-active cytotoxic chemotherapy during the second and/or third trimester had placentas that were small for gestational age. In addition, the histopathological findings included villous hypermaturity, excessive septal extravillous trophoblast (EVT), and chorioamnionitis; however, no mention of VUE or intervillositis was made. 1 It has been suggested that chemotherapeutic agents such as 5-fluorouracil, vincristine, and 6-mercaptopurine have growth-inhibiting effects on human placental trophoblast.15,16 Placental findings from a mother who received chemotherapy during all 3 trimesters demonstrated cytoplasm vacuolization, nuclear enlargement, and nuclear pleomorphism of the EVT of the chorion leave of the placental membrane. 1 The authors hypothesize that the nuclear pleomorphism of the EVT in the area where maternal and fetal tissue are in contact could be an adaptive response to toxins present in the amniotic fluid during trophoblast development that serves a protective role between the allogenic tissues. 1 Without further investigation, it is difficult to identify whether this placental pathology is the direct result of the effect of chemotherapy toxins or affected by indirect factors such as immune suppression or stress. 1
Our investigation of placentas from mothers who underwent chemotherapy during pregnancy revealed 4 placentas with inflammatory changes. Three placentas showed VUE and the fourth showed intervillositis. It is important to note that due to the complex endocrine effects of Tamoxifen, we are unable to determine whether the intervillositis observed in case 9 was due to the chemotherapy used or other factors. In further prospective studies, maternal and infant blood will be collected and additional parameters will be reviewed in order to better explain our observations in cases like this.
Villitis of unknown etiology has not been previously identified in placentas exposed to chemotherapy. It has been characterized by inflammatory lesions that contain Hoffbauer cells and T-cell lymphocytes infiltrating the placental villi.17,18 Growing evidence suggests that VUE has underlying immunopathology. IHC analyses of areas of VUE have shown increased numbers of CD25+/FOXP3+ without evidence of microbial infection. 19 Furthermore, complex analysis of VUE by Redline and Patterson demonstrated conclusively that maternal CD3+ T cells are a major component of the inflammatory infiltrate in VUE, suggesting that VUE represents multiple independent foci of maternal cell infiltration involving multiple contiguous groups of villi not belonging to the same villous tree. 17 Both studies support a working theory that VUE has an underlying immunopathology that results from dysregulation of maternal T lymphocytes leading to failed maternal–fetal tolerance that possibly causes placental inflammation. Thus, our findings of increased numbers of CD25+/FOXP3 as well as focally to strongly positive CD3 and CD4 support the underlying immunopathology compared to our normal control.
We suggest a possible phenomenon of medication-induced villitis to describe our observations from these placentas. We postulate that chemotoxins cause disruption of crucial metabolic processes at the maternal–fetal interface, leading to maternal T lymphocyte dysregulation and causing inflammation of the placenta. In addition, an unknown immune system suppression mechanism in those patients could be a contributing factor. To our knowledge, no previous studies have reported villitis in pregnancies that can possibly be attributed to the use of chemotherapy. Our study was limited due to its small retrospective nature. However, our IHC analysis for CD4+, CD25+, FOXP3+, and CD3+ T lymphocytes has shed light on this phenomenon. In future studies, we will collect data using prospective patients so that we are able to include more cases, parameters, and information such as prior pregnancy placental findings, stages of cancer, chemotherapy choice used, and the possible effects on the placenta.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.