
Abstract
Chronic intervillositis of unknown etiology (CIUE) is a rare placental inflammatory process associated with pregnancy loss and recurrence. We conducted a quality assurance study to assess the diagnostic accuracy and reproducibility of CIUE grading at our institution. Hematoxylin and eosin-stained slides from 20 CIUE cases (31 slides) were reviewed by 7 perinatal pathologists in 2 sequential rounds. Reviewers were instructed to use the diagnostic criteria they were presently following for CIUE and to grade each slide according to the Rota scheme. In the first round, 20 slides were assessed. The diagnostic accuracy was 94%, the average percent agreement of Rota grade was 79%, and the Fleiss’ kappa value for interobserver variability was 0.54. The results were reviewed by all pathologists with diagnostic and grading criteria agreed upon prior to the second round. In round 2, the remaining 11 slides were assessed. Diagnostic accuracy was 83%, the average percent agreement on Rota grade was 70%, and the Fleiss’ kappa value for interobserver variability was 0.36. Overall, diagnostic accuracy was high and agreement on Rota grade was moderate. Group review did not appear to improve accuracy. Simplifying CIUE grading to a low-grade/high-grade scheme (<50% or ≥50%) might improve grading reproducibility.
Keywords
Introduction
Chronic intervillositis of unknown etiology (CIUE) is a rare placental inflammatory process associated with pregnancy loss, intrauterine growth restriction, and significant recurrence risk.1–6 CIUE is characterized by intervillous collections of histiocytes with variable associated fibrin and can be graded according to the proportion of involved intervillous space. Higher grade CIUE has been associated with poorer outcomes.2,4
Aspirin, steroids, and heparin have been used in attempts to treat CIUE, but whether these therapies have any beneficial effect is unclear.1–3,7–10 This ambiguity may be due to variability in the definition and grading of CIUE. 11 An accurate and reproducible grading scheme is thus an important component to meaningful investigation of this disorder and assessing the efficacy of potential therapies. To facilitate future investigation and treatment of CIUE, we conducted a quality assurance study to assess the diagnostic accuracy and reproducibility of CIUE grading at our institution.
Materials and Methods
Research ethics board approval was obtained for reporting of study results. The pathology archives of BC Children’s Hospital were searched for embryofetal losses and placentas with a diagnosis of CIUE using search terms CIUE, chronic intervillositis of unknown etiology, chronic intervillositis, chronic histiocytic intervillositis, and chronic intervillitis between 2011 and 2017. To exclude cases with infectious etiologies, cases with concurrent acute chorioamnionitis and/or acute villitis were excluded from the study. Other placental lesions, including chronic villitis, were not used as exclusionary criteria. A total of 20 cases were identified including 15 first trimester and 5 second trimester pregnancy losses.
Deidentified hematoxylin and eosin-stained slides from all submitted placental tissue from each case were reviewed by 7 perinatal pathologists in 2 sequential rounds. In the first round, 20 slides (15 cases) were assessed. Reviewers were instructed to use the diagnostic criteria they were presently following for CIUE and to grade each slide according to the Rota scheme: 0 = negative, 1 = <10%, 2 = 10% to <50%, and 3 = ≥50% of intervillous space occupied by histiocytes with or without associated fibrin. 12 The majority Rota grade for each slide was considered correct for measuring accuracy and percent agreement. Interobserver variability was assessed by Fleiss’ kappa to account for the effect of chance agreement. Cohen’s kappa was calculated for each pathologist to illustrate individual variability compared to the consensus score.
After collection of the first-round data, each slide was reviewed as a group with discussion of criteria used for diagnosis and Rota grading and potential areas for improvement in diagnostic accuracy and reproducibility. The process was then repeated for the remaining 11 slides (5 cases) to assess whether there was an improvement in interobserver variability.
Results
Round 1 Individual Pathologist Scores and Consensus Scores.
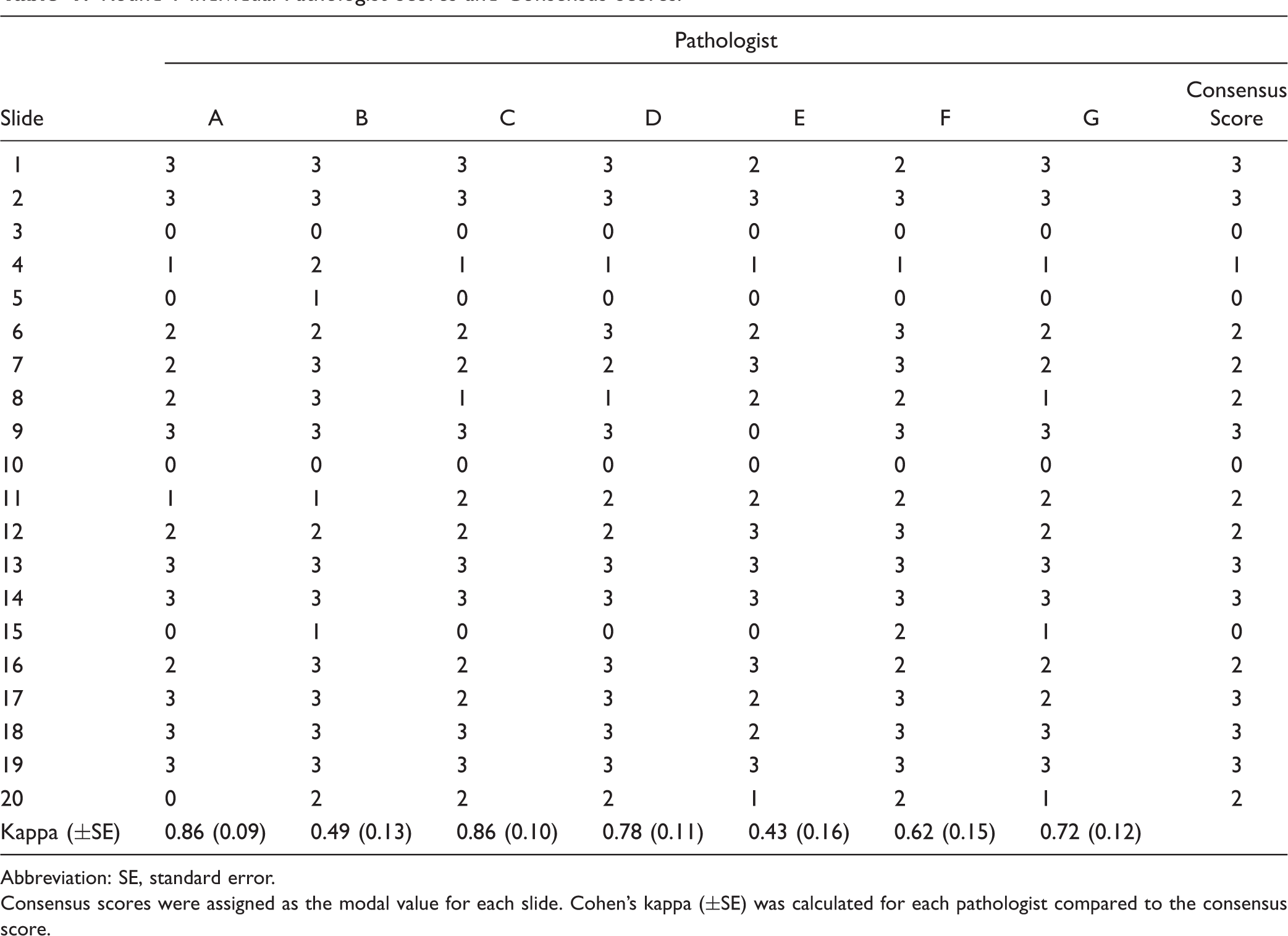
Abbreviation: SE, standard error.
Consensus scores were assigned as the modal value for each slide. Cohen’s kappa (±SE) was calculated for each pathologist compared to the consensus score.
Inclusion criteria for CIUE universally included intervillous histiocytes (Table 2). All pathologists indicated that a minimum threshold of intervillous involvement was required but this threshold subjective; one used the criterion of any abnormal clustering of histiocytes. Histiocyte clustering was reported as a helpful histological feature when maternal space involvement was low (ie, Rota grade 1; Figure 1).
Clustering of histiocytes together in the intervillous space was identified as a useful low to moderate power feature of CIUE. Pathologist Criteria for the Diagnosis and Grading of CIUE. Universal criteria” were applied by all pathologists prior to review. “Variable criteria” differed between pathologists prior to review. “Consensus criteria” were agreed upon following group review of the cases in round 1 and were applied to the cases in round 2.
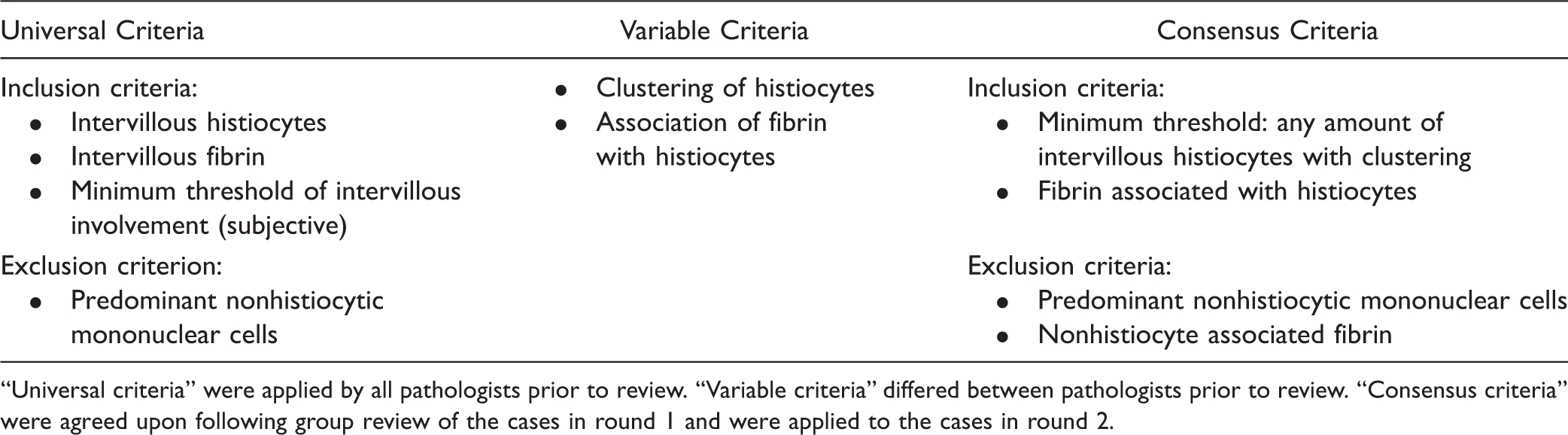
All pathologists included intervillous fibrin when assessing grade, although some reviewers included all intervillous fibrin while others included only intervillous fibrin associated with areas of intervillous histiocytes. For those including only histiocyte-associated fibrin, there was uncertainty over the criteria for distinguishing histiocyte associated and nonassociated fibrin (Figure 2).
Fibrin without associated clustered intervillous histiocytes (black arrows) can contribute to interobserver variability in grading of CIUE.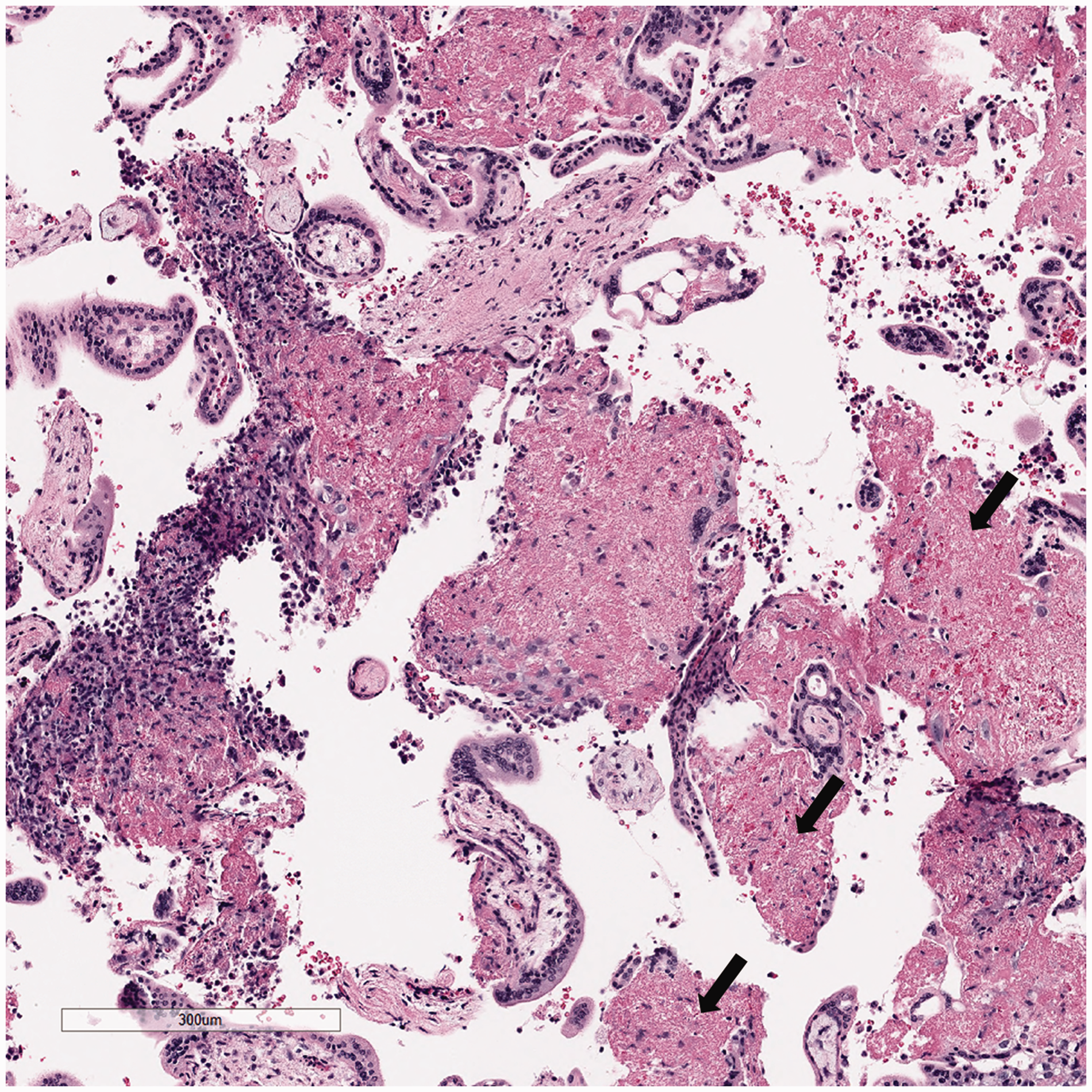
All pathologists excluded cases where there the majority of intervillous mononuclear cells were nonhistiocytic. No pathologists excluded cases with chronic villitis or other pathological lesions present in the slides examined.
After rereview of the first-round cases using the mutually agreed diagnostic inclusion (any amount of intervillous histiocytes with clustering, intervillous histiocyte-associated fibrin) and exclusion (predominant nonhistiocytic mononuclear cells) criteria, 2 cases were reclassified as negative. One case had increased intervillous fibrin but no clustered intervillous histiocytic component and the other was comprised primarily of a neutrophilic intervillous infiltrate. Disagreement between Rota grades 0/1 and 1/2 was considered the most significant factor in interobserver variability.
Round 2 Individual Pathologist Scores and Consensus Scores.
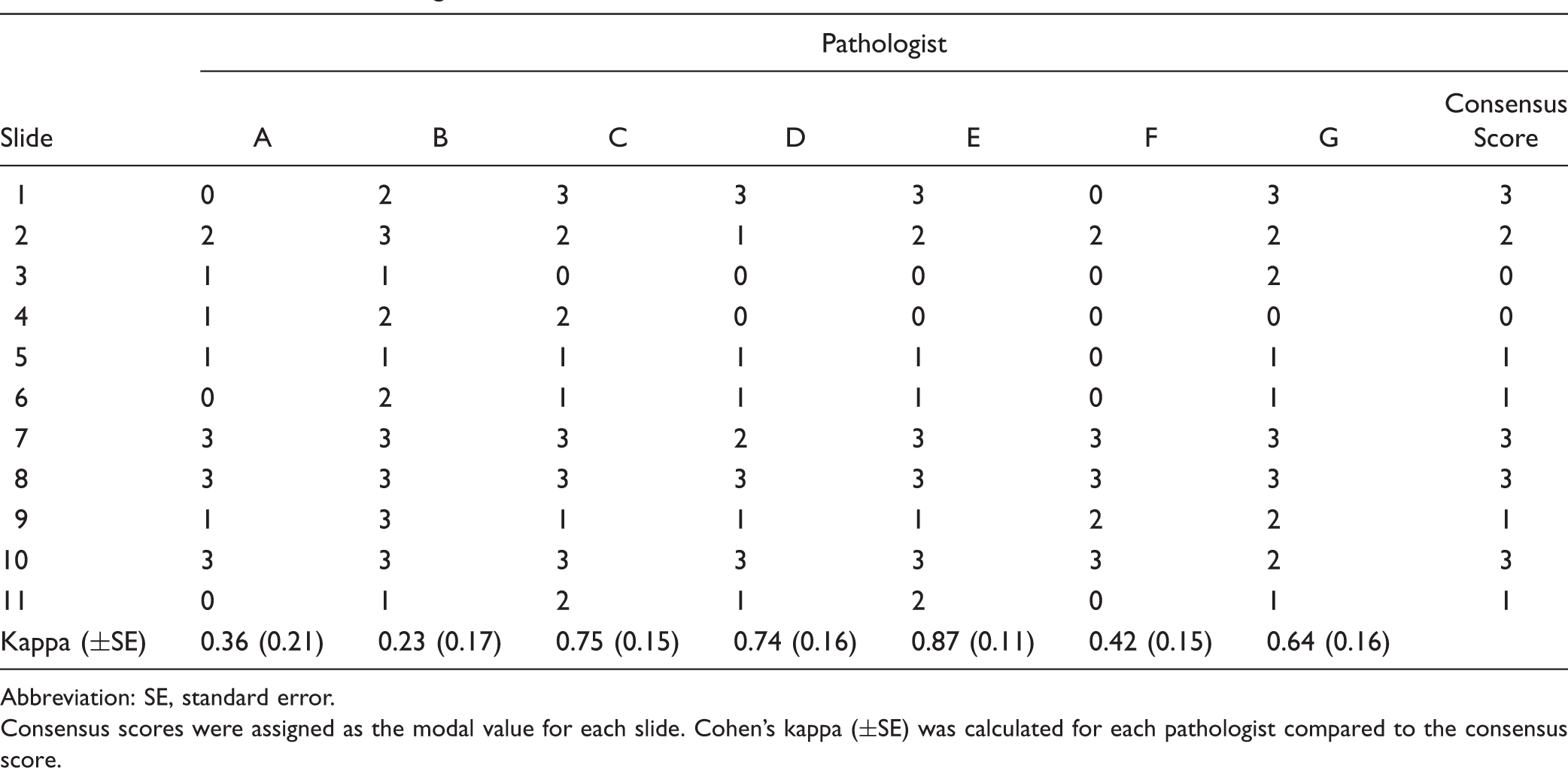
Abbreviation: SE, standard error.
Consensus scores were assigned as the modal value for each slide. Cohen’s kappa (±SE) was calculated for each pathologist compared to the consensus score.
Discussion
The definition and nomenclature of CIUE has been variable which has led to diagnostic confusion and difficulty in studying this process in a standardized fashion. The recent review of CIUE by Bos et al., 11 published after this study was completed, provides an excellent overview of variability of diagnostic criteria of CIUE in the literature.
Overall, diagnostic accuracy was high and agreement on Rota grade was moderate. Uncertainty over the distinction between Rota grades 1 and 2 and the extent of intervillous fibrin to include in grading were significant factors in interobserver variability. Group review did not improve accuracy and agreement, but this may be due to a higher proportion of Rota grade 0/1/2 slides in round 2. Simplifying CIUE grading to a low-grade/high-grade scheme (<50% or ≥50%) might improve grading reproducibility.
All pathologists involved in this review considered intervillous histiocytosis as a necessary feature of CIUE. The threshold criterion for diagnosis was the subjective impression of abnormal intervillous histiocytic aggregation. Studies demonstrating poorer outcome with higher grade CIUE suggest that a higher minimal threshold may be more specific, but there is little data to support this suggestion and adoption of a higher threshold risks missing more subtle correlations of CIUE grade with clinical outcome. Bos et al. have recently proposed diagnostic criteria for CIUE that includes a minimum of 5% maternal space involvement, which would be more inclusive and facilitate subsequent studies to determine the correlation of CIUE grade to outcomes. As a caveat, this proposed threshold is based on a case series by Traeder et al., 6 where its use as an inclusion criterion was not supported by evidence; further studies are required to further define the minimal threshold of histiocytic intervillous space involvement for CIUE diagnosis.
The inclusion of fibrin in grading was variable in our review due to uncertainty over the classification of histiocyte-associated versus histiocyte-unassociated fibrin. This uncertainty was likely the primary cause of interobserver variability, particularly in distinguishing between Rota grades 1 and 2. Omission of fibrin in CIUE grading might significantly improve interobserver variability. However, it is possible that the impact of fibrin on outcome is independent of histiocyte density; this distinction would be lost if fibrin was not included. Simplification of the Rota grading scheme to less than 50% or more than 50% maternal space involvement may mitigate the effect of variable inclusion of fibrin on interobserver agreement.
Exclusion criteria are less well-defined in the diagnosis of CIUE. In our review, features of an infectious process were considered exclusionary criteria and included a predominance of neutrophils within the histiocytic clusters and cooccurrence of acute chorioamnionitis or acute villitis. Cooccurrence of chronic villitis or other placental lesions has been used as an exclusionary criterion by others but was not regarded as such by the pathologists involved in this study.
Although not used in this study, CD68 immunohistochemistry was identified as a useful adjunct in identification of histiocytes where cytological features were less definitive, particularly in the setting of abundant fibrin or blood. Bos et al. include a requirement for approximately 80% of the intervillous mononuclear cells to be CD68 positive in their proposed CIUE diagnostic criteria. In our experience, CD68 immunohistochemistry is valuable for estimating the percentage of intervillous space involvement but not required in all cases to differentiate histiocytes from other circulating mononuclear cells.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.