
Abstract
Methadone, an opioid agonist, is the recommended treatment for pregnant women with opioid use disorder (OUD). Fetal/neonatal autopsy findings as well as placental changes in the setting of maternal OUD or methadone maintenance therapy (MMT) are not well-characterized. Here we present a case of a neonate who had exposure to MMT while in utero and died shortly after birth and was subsequently found to have multifocal calcified renal vein thrombosis, a recent inferior vena cava thrombus, and placental features of fetal vascular malperfusion at autopsy.
Keywords
Introduction
Methadone, an opioid agonist, is the recommended treatment for pregnant women with opioid use disorder (OUD). It crosses the placenta and increases the risk of neonatal mortality and sudden infant death syndrome. 1 Methadone is metabolized in the liver and eliminated by the kidneys. In adults, opioid use can lead to acute kidney injury or result in acute glomerulonephritis. 2 How methadone affects fetal renal function is currently not well-understood. Higher susceptibility to thromboembolism among adult opioid abusers due to increased levels of platelets, hematocrit, fibrinogen, and C-reactive protein have been described. 3 It is unclear whether the same holds true for neonates who have been exposed to opioid agonist in utero.
Renal vein thrombosis (RVT), is an uncommon but well-known neonatal entity, often of low mortality but high morbidity. 4 , 5 It can occur spontaneously or as a complication of umbilical vein catheterization in otherwise healthy infants. In neonates, it is the most common noncatheter-related form of thromboembolism. 4 Some predisposing conditions include perinatal asphyxia, septicemia, dehydration, polycythemia, and inherited thrombophilic conditions. 5 Renal complications such as RVT at this stage of life, along with exposure to methadone, can increase the risk of opioid-induced respiratory distress. 6 OUD has also been associated with chorionic villi maldevelopment possibly resulting in fetal hypoxia. 1
Here, we present a case of neonatal demise occurring shortly after delivery with the neonate having been exposed to methadone maintenance therapy (MMT) throughout the gestation. This is the first account of neonatal RVT and inferior vena cava (IVC) thrombosis accompanied by features of fetal vascular malperfusion (FVM) occurring in the setting of maternal OUD/MMT.
Case Report
A term, male neonate was born to a 31-year-old G5P2 mother by emergent C-section (CS) at 40-1/7 weeks gestational age (GA) for terminal fetal bradycardia. Maternal history included opiate abuse, which started 9 years ago after a motor vehicle accident. She was initially treated with acetaminophen/oxycodone but later developed opioid dependence. After 7 years of usage, she went into recovery and has been on MMT for 2 years. Maternal history was also notable for a prior pregnancy while on MMT (the said offspring is alive and well), smoking, and obesity. No history of diabetes mellitus nor of thrombophilic disorders was noted. The paternal history was unknown.
Prenatal ultrasound at 30 and 34 weeks GA showed appropriate fetal growth, no anatomic fetal abnormalities, and the umbilical cord was within normal limits. At 40-1/7 weeks GA, the mother presented with decreased sensation of fetal movement. Further evaluation revealed decreased fetal heart rate in the 60's. Following emergent CS, the neonate emerged limp, blue, and without spontaneous respiratory effort. Appearance, Pulse, Grimace, Activity, and Respiration (APGAR) scores were 1 at both 1 and 5 minutes and his heart rate continued to decline. An umbilical vein catheter was placed. Despite maximal resuscitation, there was no clinical response. The neonate expired 19 minutes after birth. A urine drug screen was performed on the mother about 2 hours after delivery which showed elevated levels of morphine and fentanyl (administered in the hospital) and positivity for methadone and methadone metabolite. The neonate’s levels were not tested ante- or postmortem. The clinicians noted liver enlargement and requested an autopsy.
At autopsy, the external features and anthropometric measurements were consistent with >40 weeks GA. There were no external dysmorphic features. In situ examination revealed a prominent liver that was only slightly heavier than expected (liver weight: 167.8 g; expected: 130 ± 32 g). The IVC revealed a soft yellow-tan ovoid lesion focally attached to the vessel wall via a thin “thread-like” structure. The kidneys were red-tan and heavy (combined weight: 43.67 g; expected: 25.7 ± 7.5 g), with congested cut surfaces. The brain was dusky with convolutional pattern appropriate for GA. Coronal sections demonstrated accentuation of cortical pallor against the congested white matter (“ribbon effect”) indicating hypoxic–ischemic encephalopathy.
The placenta weighed 478 g (10th–25th percentile for GA). An eccentrically attached 3-vessel umbilical cord measured 15.0 cm long and 1.5 cm in average diameter, contained 3 coils (0.2 coils/cm) and a false knot distally. No additional segments of umbilical cord were submitted and the cross sections showed no thrombi within umbilical vessels. Fetal membranes were edematous. No parenchymal lesions were identified macroscopically.
Histologically, the kidneys showed calcified and organizing thrombi within several renal veins close to the hilum (Figure 1(A) to (G)). The lesion within the IVC was most consistent with a recent thrombus (Figure 1(H) to (J)). Thymic involutional changes were present. Extramedullary hematopoiesis (EMH) and circulating nucleated red blood cells (NRBCs) were seen in multiple organs. EMH was particularly increased in the liver with predominance of erythroid elements. The brain showed diffuse cortical edema, leptomeningeal and parenchymal congestion, and diffuse reactive astrogliosis of the white matter.

Renal vein and IVC thrombi: (A and D) Organized thrombi within large and medium-sized veins with evidence of calcification and recanalization (long arrows in A, C, and D) and extramedullary hematopoiesis surrounding the thrombus (arrow heads in D; H&E; 20×). B, Trichrome stain. C, CD34 stain highlights large vein wall and numerous minute capillaries within the thrombus, consistent with recanalization. E, Macroscopic image of the IVC with occluding thrombus beneath the probe. F, Low power view of recent IVC thrombus. (H&E; 20×). H&E, hematoxylin and eosin.
The placenta exhibited features consistent with FVM including multifocal large patches of enlarged hypovascular and avascular villi with prominent villous stromal–vascular karyorrhexis and stem villous obliteration. However, there were no histologic features suggestive of umbilical cord obstruction such as ectatic umbilical, chorionic plate, and stem villous vessels. There were areas of delayed villous maturation (DVM) and circulating fetal NRBCs (up to 15/10 high power field; Figure 2). Villous infarction, accelerated villous maturation, distal villous hypoplasia, decidual vascular lesions, and other features of maternal vascular malperfusion were absent.
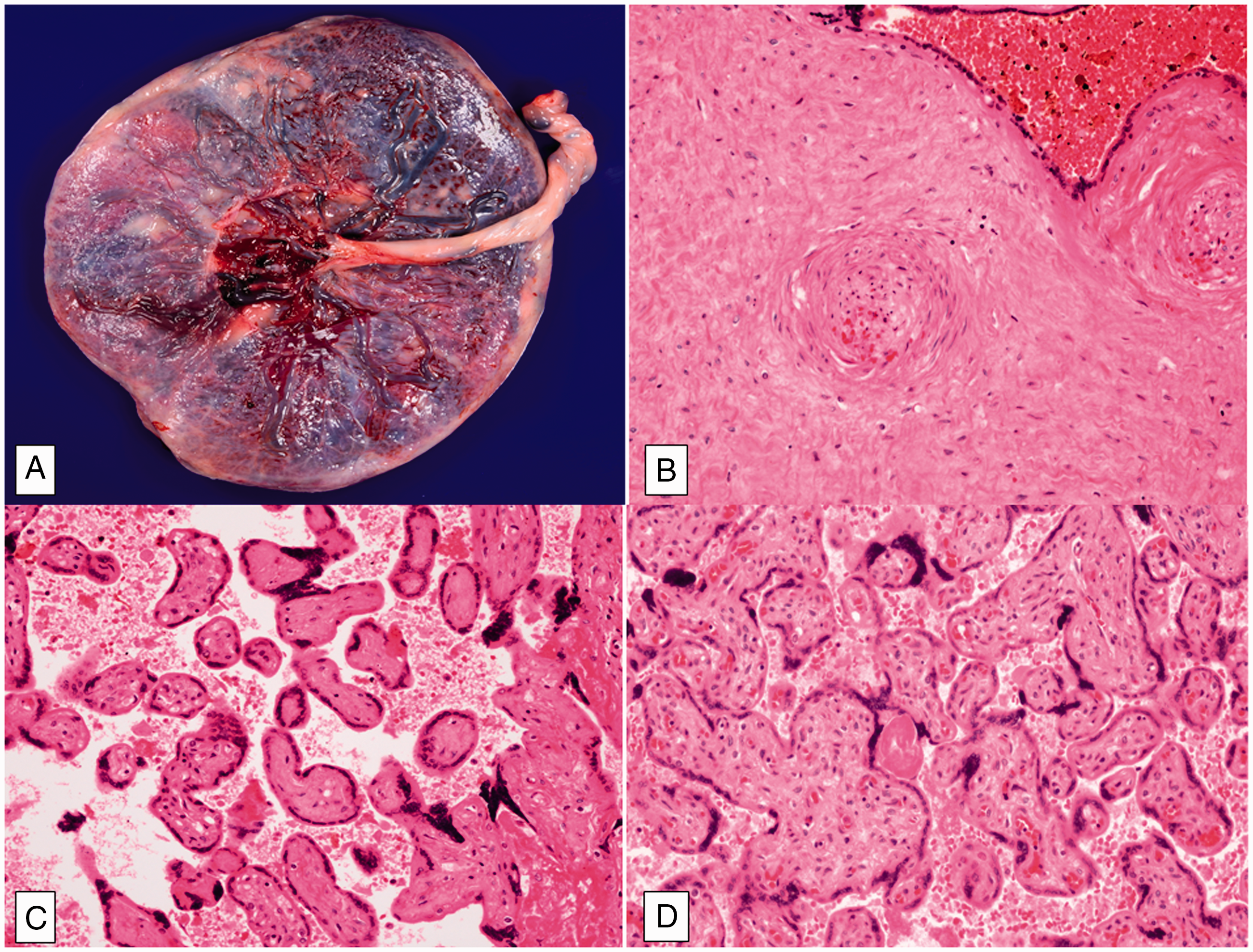
Placenta with microscopic features of fetal vascular malperfusion. A, Gross image of the placenta. B, Stem villous obliteration: thickening of the stem villous vessel wall with fibroblastic ingrowth and luminal obliteration (H&E; 40×). C, Cluster of avascular villi (H&E;40×). E, Representative focus of delayed villous maturation showing large bullous villi (H&E; 40×). H&E, hematoxylin and eosin.
Discussion
Fetal autopsy findings in the setting of maternal OUD or MMT are not well-characterized. It has been postulated that methadone use during pregnancy could be a direct or indirect contributory risk factor for sudden infant death syndrome. 7 One study showed the development of renal complications including RVT in a few pediatric patients who received morphine for pain management post elective surgeries and increased postsurgical respiratory depression. 6
In our case, the neonate was found to have multifocal RVT of the right kidney. There was evidence of global hypoxia, in utero stress-induced changes, as well as FVM in the placenta. At baseline, neonates are believed to be more prone to developing thromboembolic episodes due to their relatively lower levels of naturally occurring anticoagulants and fibrinolytic components when compared with older children and adults, low renal perfusion pressure, and double intracapillary network. In the presence of coexisting risk factors such as perinatal asphyxia, dehydration, hypovolemia, shock, or maternal diabetes mellitus, RVT may develop due to reduced renal perfusion which leads to vasoconstriction and decreased venous flow resulting in thrombosis. 4 , 8 Although most RVT cases are detected within the first few postnatal days or weeks of life, our case supports a prenatal onset given the presence of calcification and organization of the thrombi.
As stated earlier, renal complications may hamper the clearance of methadone and its by-products resulting in accumulation of active metabolites thereby augmenting the risk of opioid-induced respiratory distress. Depression of the ventilatory responses to hypoxia and hypercapnia and the lack of drive to breathe are known consequences of opioid exposure. 9 At birth, the neonate made no effort to breathe and even after intubation, minimal rising of the chest was noted. It was clear that the neonate was profoundly hypoxic and in respiratory failure. In addition, microscopic stress-induced changes such as EMH in various organs, involutional changes in the thymus, and circulating NRBCs corroborate prenatal hypoxic state.
Features of FVM in different stages of evolution (stem villous obliteration, villus stromal–vascular karyorrhexis, hypovascular, and avascular villi) are present, and the presence of avascular villi in the placenta indicates prolonged vascular occlusion. Complications of FVM have been linked to adverse perinatal outcomes, thromboembolic events, and intrauterine fetal demise. 10 Areas of DVM, also identified in the placenta, can be observed with FVM. Normally, the chorionic villi undergo maturation as the pregnancy progresses, and this is made evident by an increase in peripherally located thin-walled capillaries and formation of vasculo-syncytial membranes, which allow for a more efficient gas exchange between maternal and fetal circulations. 1 In DVM, the villi fail to mature and the vasculature remains centrally located within the villi, resulting in failure to eliminate the diffusion distance between maternal and fetal circulations thereby leading to intrauterine hypoxia. Serra et al. concluded that DVM was significantly more common in women treated with opioid maintenance therapy than the untreated group. 1
Interestingly, RVT and IVC thrombosis has been associated with FVM in 2 separate case reports 8 , 11 (see Table 1). Despite a more known association with maternal vascular malperfusion, some authors postulate that maternal diabetes may be an underrecognized risk factor for FVM. It has been suggested that a maternal diabetes environment may affect the fetal placental vascular system by inducing certain changes (increased angiogenesis, altered wall permeability, among others), which when combined with the innate hypercoagulable tendencies of the fetus, may trigger activation of coagulation factors. 11 Maternal diabetes mellitus is not present in the current case.
Summary of Reported Cases of RVT and IVC Thrombosis With Associated Placental FVM.
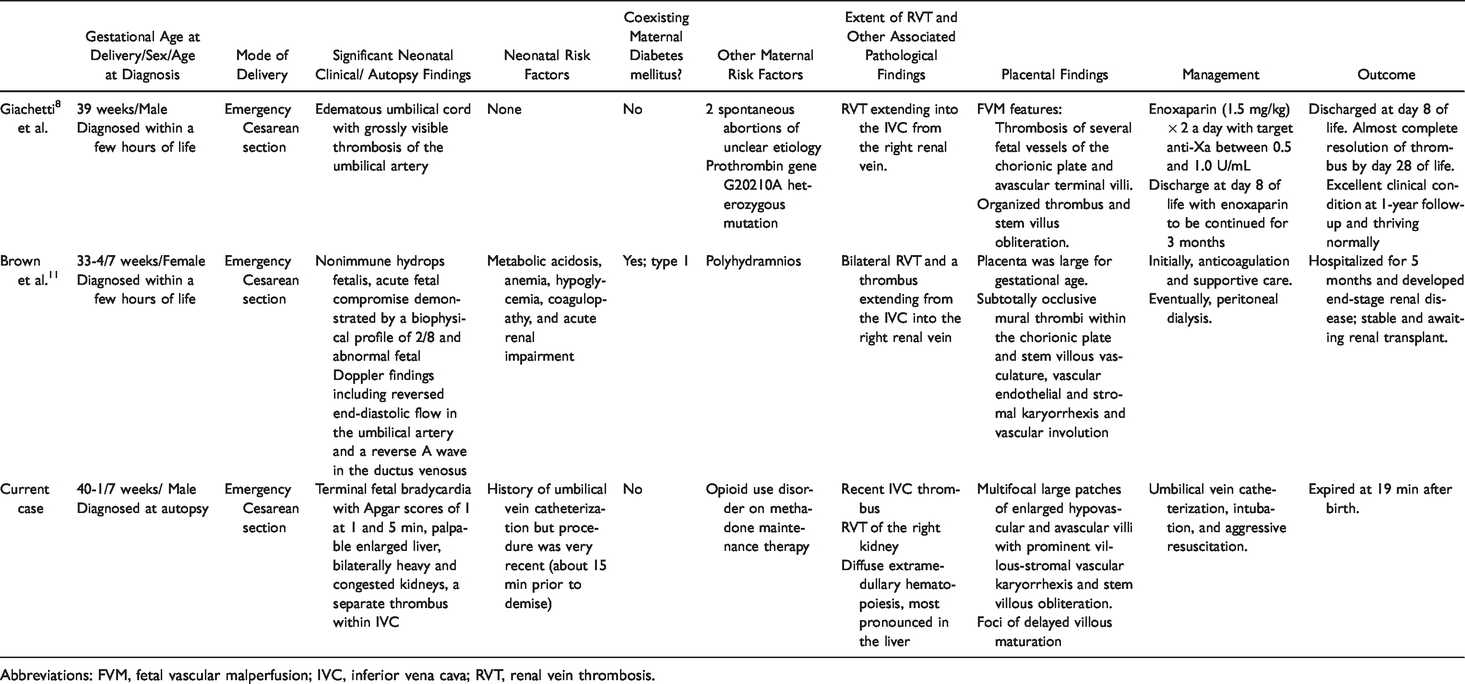
Abbreviations: FVM, fetal vascular malperfusion; IVC, inferior vena cava; RVT, renal vein thrombosis.
Overall, the autopsy and placental findings may be interconnected with “hypercoagulability” as the probable common denominator. It adds to the recently recognized association of fetal/neonatal thrombosis, most commonly affecting the renal vein and IVC, and FVM. The neonatal demise is likely related to respiratory complications of OUD/MMT, with the drug effects augmented by reduced drug elimination secondary to the coexisting RVT. It is possible that the MMT exposure not only resulted in respiratory function depression but also created a pro-thrombotic milieu, which in return exacerbated its own negative respiratory function effect. Other etiologies such as an inherited coagulation disorder cannot be entirely dismissed particularly with an unknown paternal history. FVM has not been previously described in placentas exposed to OUD or MMT. Better understanding of fetal/neonatal autopsy and placental findings in the setting of OUD or MMT is needed to make a more conclusive diagnosis of opioid-related neonatal demise.
Footnotes
Author Contributions
Joseph Kim and Chrystalle Katte Carreon performed the autopsy. Jessenia C. Guerrero, Joseph Kim, Mariarita Santi, Eduardo Ruchelli, and Chrystalle Katte Carreon drafted manuscript and reviewed microscopic findings. Mariarita Santi provided neuropathologic findings and performed brain dissection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval/Patient Consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human subject research and with the Helsinki Declaration of 1975, as revised in 2008, and in accordance with the publication policies on human subjects research of The Children’s Hospital of Philadelphia, Pennsylvania, USA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.