
Abstract
Background
The incidence of umbilical cord or placental parenchyma abnormalities associated with mortality or morbidity of term infants is lacking.
Methods
Placentas of 55 antepartum stillbirths (APD), 21 intrapartum stillbirths (IPD), 12 neonatal deaths (ND), and 80 admissions to a level 3 neonatal intensive care unit (NS) were studied and compared with 439 placentas from neonates from normal term pregnancies and normal outcome after vaginal delivery (NPVD) and with 105 placentas after an elective caesarian sections (NPEC).
Results
NPVD and NPEC placentas showed no or one abnormality in 70% and placentas from stillbirth showed two or more abnormalities in 80% of cases. APD placentas more frequently had a low weight and less formation of terminal villi. Hypercoiling was more often present in all study groups. Severe chronic villitis was almost exclusively present in APD placentas. Chorioamnionitis was significantly more frequent in APD, IPD and NS placentas and funisitis was more often observed in IPD and NS placentas.
Conclusion
Multiple placental abnormalities are significantly more frequent in placentas from term neonates with severe perinatal morbidity and mortality. These placental abnormalities are thought to be associated with disturbed oxygen transfer or with inflammation.
Introduction
The placenta is essential for intra-uterine growth and development of the fetus. It connects mother and fetus, delivers oxygen and nutrients to and removes waste products from the fetus. Oxygen delivery is one of the main functions of the placenta and, if reduced, is an important cause of perinatal mortality and morbidity.1,2 The study of the placenta is essential to gain more insight into the different causes of perinatal morbidity and mortality and can have implications for future pregnancies.3–5 Abnormalities in the placenta may also indicate increased risk of chronic disease later in life.6,7 To date, few studies have examined the relation between neonatal outcome and placenta pathology. The incidence of placental pathology in normal placentas is almost lacking and in most papers only placenta pathology in adverse outcome is studied.4,8–14 In this paper we describe the pathology in placentas from cases of NICU admittance (survivors and patients that died at the NICU), from term neonates that died intrapartum and from term antepartum death cases and compared these findings with the pathology observed in placentas from normal healthy neonates born at term after an uncomplicated pregnancy. These infants were either born vaginally or by elective caesarian section. The placentas were studied with special attention for the anatomy and pathological lesions in the umbilical cord (e.g. cord coiling), fetal vessels and placental parenchyma, all known to have an effect on the fetal circulation and linked to fetal hypoxia and/or inflammation.15–17
Methods
Population
In 2007 and 2008 a prospective cohort study on severe morbidity and mortality of term fetuses or neonates without congenital anomalies, called ATNICID (Admission of Term Neonates to Intensive Care or Intrauterine Death), was performed in the middle of the Netherlands in an area situated around the University Hospital and neonatal intensive care unit (NICU) of Utrecht. The study has already been extensively described.18,19 Data on all antepartum stillbirths, intrapartum stillbirths, neonatal deaths, and admissions to a level 3 NICU of term infants within the first seven days of life were collected. Placentas from multiple pregnancies were excluded from this study. Antepartum stillbirth was defined as the death of a fetus prior to the onset of labour and intrapartum death was defined as the death of the fetus after the onset of labour but before birth. The control placentas were obtained between January 2006 and November 2007 from a prospective birth cohort of healthy children born after at least 37 weeks of gestation with an uncomplicated pregnancy and a spontaneous vaginal delivery or an elective CS because of a previous CS or breech presentation. We classified the weight of the newborns below the 10th or above the 90th percentile according to the Dutch reference curves. 20 Mortality was classified according to the Tulip classification system. 21
Placenta study
All control placentas were sent fresh to the pathology department. During the study period obstetricians and midwives were asked to send placentas from infants that died before birth as soon as possible and preferably fresh to the pathology department of the university hospital as well as the placentas from the cases that were admitted to the NICU. All placentas were examined by one pathologist (PGJN). If the placenta was sent to the local pathologist the slides and remaining formalin fixed material were reviewed and additional sampling of the placenta parenchyma, membranes and umbilical cord was done according to our protocol. From 16 of the 80 NS placentas only slides were available and from 2 of the 80 NS placentas the placenta was received on formalin. From 16 of the 55 APD placentas only slides were available and two of the 55 APD placentas were received on formalin. From 1 of the 21 IPD placentas only slides were available and 1 of the IPD placentas was received on formalin. From 4 of the 12 ND placentas only slides were available and 1 of the ND placentas was received on formalin. From the cases were only histology was available, a slide from the umbilical cord, membranes and at least two slides from normal parenchyma and additional slides from macroscopically observed abnormalities were available in all cases.
Macroscopical examination
The cord coiling index was determined fresh in all placentas by measuring the number of complete coils of 360° of the arteries divided by the total length of umbilical cord in cm. Hypocoiling was considered as an index below 0.1 and hypercoiling as an index above 0.3. 22 Cords with a length over 80 cm were classified as excessive long. Placentas were weighed without membranes and umbilical cord and weight for gestational age percentiles were used from Pinar and colleagues. 23 A weight below the 10th and above the 90th percentile was classified as abnormal.
Histology
For histology two sections of umbilical cord, at the fetal and placental side, a membrane roll, one sample from the umbilical cord insertion, and three slides of normal placental parenchyma, including both decidua and chorionic plate, were collected and stained with standard haematoxylin and eosin. Additional samples were taken from macroscopically abnormal parenchyma. The histological evaluation was done before the 2016 Amsterdam consensus conference. 24 The terminology used was comparable with the statements of the conference or slightly modified based on the author’s previous publications.16,19
Chorioamnionitis was diagnosed as the presence of neutrophils in the chorionic plate or the extraplacental membranes. Funisitis was diagnosed as the presence of neutrophils in the wall of the umbilical vein or arteries with or without extension in Wharton’s jelly. Chronic villitis or villitis of unknown etiology (VUE) was diagnosed as an infiltrate of lymphocytes and macrophages in groups of at least 5 placental villi. In addition to the presence of chorioamnionitis, funisitis or chronic villitis, the severity of inflammation was graded mild, moderate or severe, with slight modifications comparable to the staging and grading system used in the Amsterdam consensus conference statement. 24 Our grade 1 VUE was comparable with low grade focal VUE and our grade 3 was comparable with high grade diffuse VUE. Grade 2 were both low grade diffuse and high grade focal VUE of the 2016 Amsterdam consensus conference. 24 Delay in the formation of syncytiocapillary membranes (SCM) in terminal villi was determined as previously described. 16 A SCM was defined as a dilated capillary in broad contact with the thin trophoblastic cover, without presence of a nucleus in the contact area according to Stallmach and others. 25 Formation of SCM or maturation was classified as abnormal if in at least one slide the mean of SCM was less than 0.25 SCM/villus in the 10 smallest villi in 10 fields. Fetal thrombosis was determined as groups of at least 5 avascular fibrotic villi, thrombosis in a vessel of the umbilical cord, chorionic plate or stemvillus, haemorrhagic endovasculitis, or intramural deposition of fibrin in a vessel of the umbilical cord, chorionic plate or stemvillus.24,26 The presence of nucleated red blood cells (NRBC) were documented and graded as mild with the occasional presence of NRBC in umbilical cord blood, and as moderate or severe based on the occasional or abundant presence of NRBC in terminal villi respectively. Only moderate and severe presence of NRBC was used for this study. The different items associated with maternal vascular malperfusion that were scored in these term placenta’s were low weight (a weight below the 10th percentile) and presence of infarcts. Accelerated villous maturation was not present/scored in these term placentas and there were no cases with distal villous hypoplasia in our study or control group. Decidual arteriopathy was not scored during the study period. There were two cases with the clinical diagnosis of placental abruption in the antepartum stillbirth group, two cases in the intrapartum death group and three cases in the NICU admitted neonates. Ischemic changes/increased occurrence of syncytial knots was not scored according to the 2016 Amsterdam consensus conference in the study group (more than 1/3 of affected villi per slide).
Statistical Analysis
In all analyses, placentas from the NPVD group were used as the reference category. The associations between the multinomial outcome and the placental characteristics were assessed by calculating an odds ratio (OR) with 95% confidence interval (95% CI). The OR was determined using a logistic regression model or multinomial logistic regression model depending on the placental characteristic being dichotomous or categorical, respectively. An OR and its 95% CI not including one, i.e. a p-value < 0.05 was considered to be statistically significant. All statistical analysis were conducted in R for Windows (version 2.10.0).
Results
Obstetrical details from all groups are presented in Table 1. Six placentas from multiple-gestation pregnancies were excluded from this study. Percentages of the placentas available for the study are presented in Figure 1. From the 206 neonates admitted to the NICU, 98 infants were admitted because of asphyxia of which 13 neonates died. Thirty-two neonates were admitted because of an infection, of which four died. The other NICU survivors were admitted because of meconium aspiration syndrome (n = 10), respiratory distress (n = 24) and other reasons (n = 42). Four hundred and thirty-nine control placentas were collected after a vaginal delivery and 105 placentas after an elective CS. Odds ratios, (95% confidence intervals and p values are presented in Table 2.
Obstetrical Characteristics of the Total Study Population.
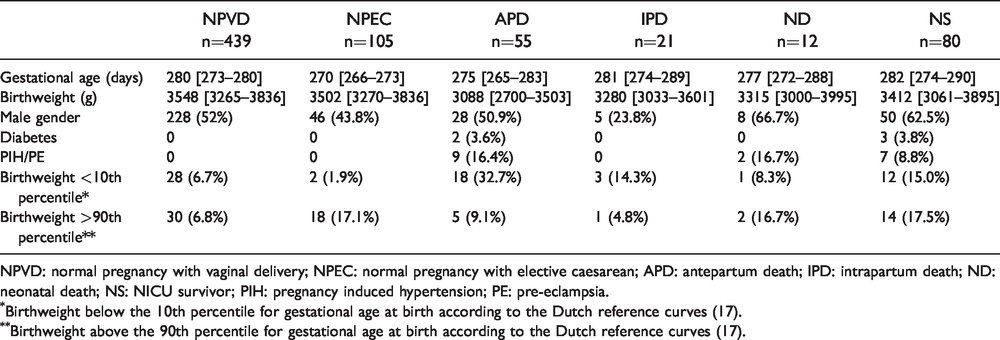
NPVD: normal pregnancy with vaginal delivery; NPEC: normal pregnancy with elective caesarean; APD: antepartum death; IPD: intrapartum death; ND: neonatal death; NS: NICU survivor; PIH: pregnancy induced hypertension; PE: pre-eclampsia.
Birthweight below the 10th percentile for gestational age at birth according to the Dutch reference curves (17).
Birthweight above the 90th percentile for gestational age at birth according to the Dutch reference curves (17).
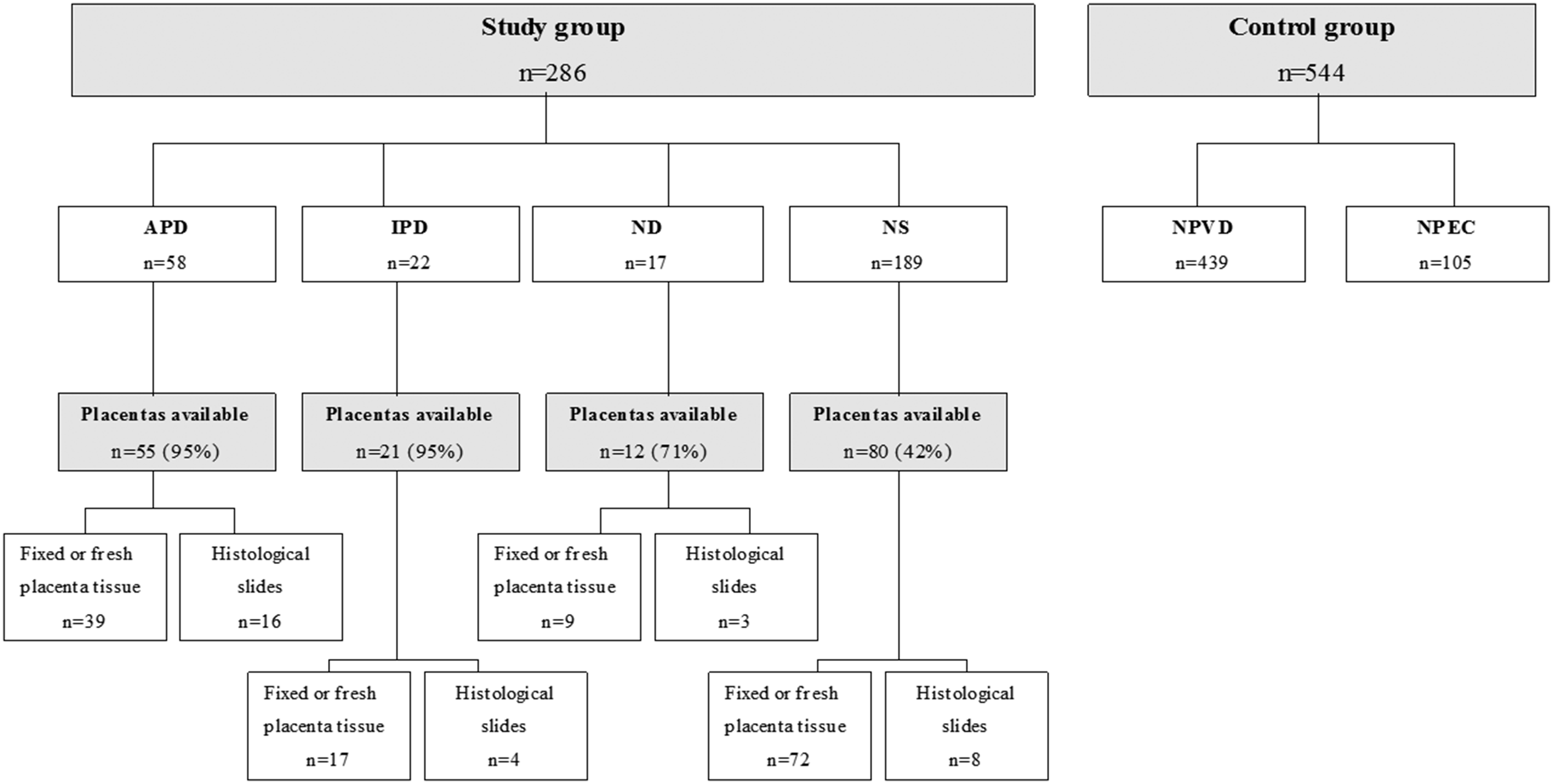
Total number of placentas per study group. APD: antepartum death; IPD: intrapartum death; ND: neonatal death; NS: NICU survivor; NPVD: normal pregnancy with vaginal delivery; NPEC: normal pregnancy with elective caesarean.
Odds Ratios and Confidence Intervals With P Values of the Different Abnormalities in the Placenta Per Study Group.
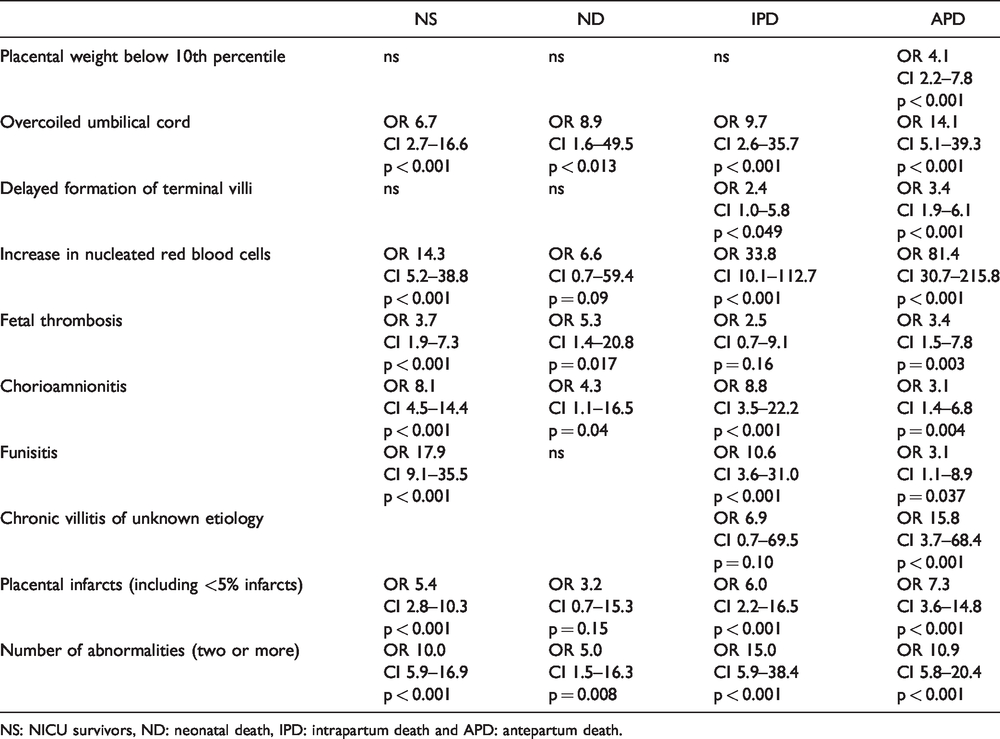
NS: NICU survivors, ND: neonatal death, IPD: intrapartum death and APD: antepartum death.
Placental weight
Low weight placentas were overrepresented in the APD cases. Fifty five percent of APD placentas had a weight below 10th percentile (Figure 2(A)). The incidence of placentas with a weight above the 90th percentile was highest in the NS placentas (OR 4.3 (CI 2.2 – 7.9, p < 0.001) and the NPEC placentas (OR 2.9; CI 1.6–5.1, p < 0.001).
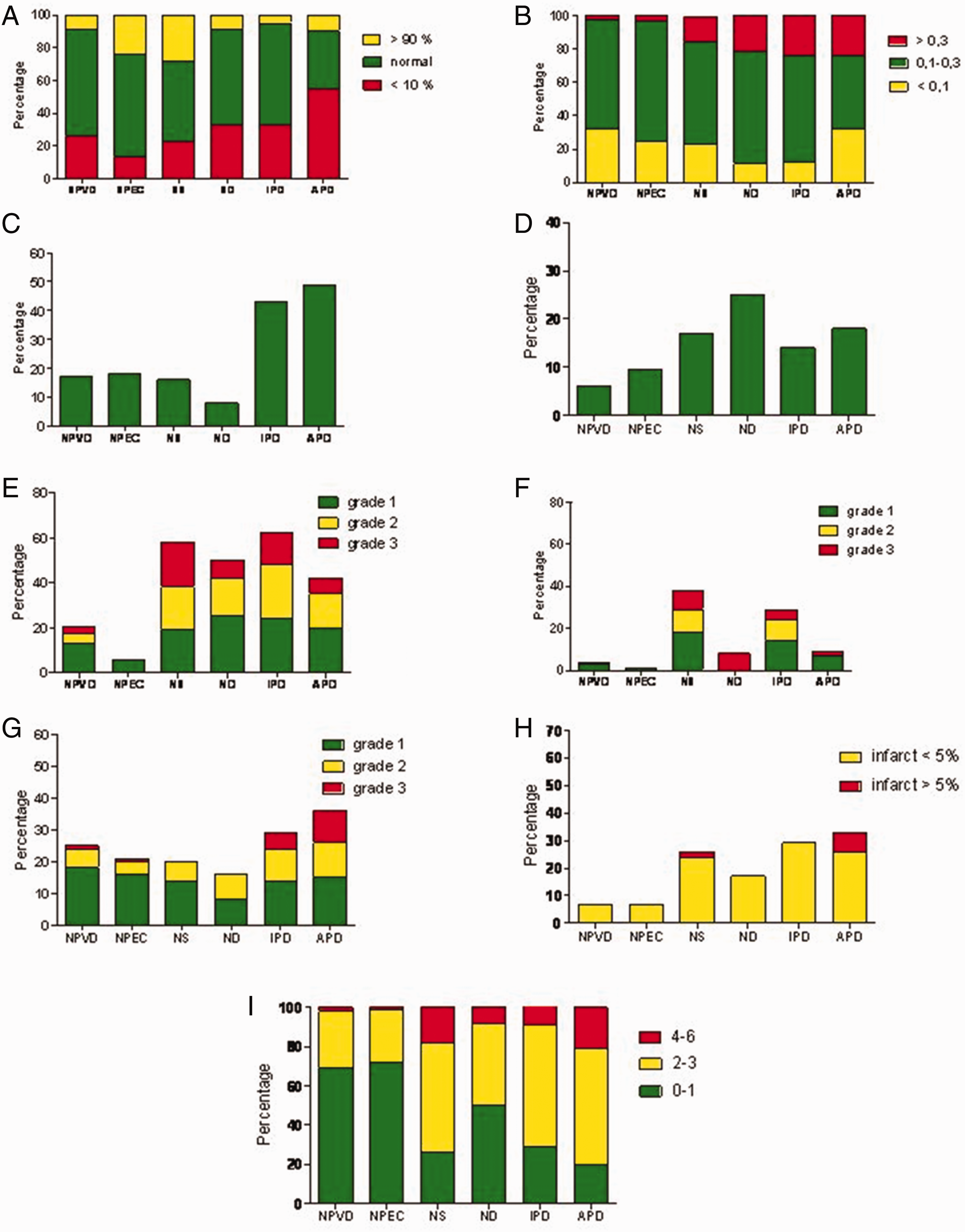
Placental abnormalities per study group. A: Placental weight; B: Cord coiling index; C:Diminished formation of terminal villi; D: Thrombosis; E: Chorioamnionitis, F: Funisitis; G: chronic villitis; H: placental infarcts; I: Total number of abnormalities per placenta.
Placental infarcts
In the study groups infarcts were not often present and in most cases only less than 5% of the placental parenchyma was involved. More than 5% involved parenchyma was seen in 7% of APD placentas and in 3% of NS placentas; in the other groups more than 5% infarcted parenchyma was not observed (Figure 2(H)). Infarcts of less than 5% parenchymal volume were seen in 6-7% of NPVD and NPEC placentas. The incidence of less than 5% infarcts was 31%, 27%, 17% and 25% in the APD, IPD, ND and NS placentas respectively. In 30% of the low and normal weight placentas from the APD cases infarcts could be found. In IPD and ND cases the incidence of finding infarcts was 30% only in the low weight placentas and in normal weight placentas it was 10%. In placentas with a weight above the 90th percentile no infarcts were observed in control or study group (data not shown).
Maturation or formation of terminal villi
The placentas from the APD and IPD cases had the highest incidence of diminished formation of terminal villi 49 and 43% of cases respectively (Figure 2(C)). The two other groups (ND and NS) showed a diminished formation of terminal villi in 8-16% of cases. The NPVD and NPEC placentas showed a diminished maturation in 17-18% of cases. In these two groups with normal neonatal outcome a diminished formation of terminal villi was more often observed in the placentas with a weight above the 90th percentile. In low weight placentas it was 10%, in normal weight placenta’s it was 21% and in the placentas with a weight above the 90th percentile it was 34% (data not shown). There were no cases with distal villous hypoplasia. Accelerated villous maturation was not present/scored in these term placentas.
Villitis of unknown etiology
Grade 3 chronic villitis of unknown etiology (high grade diffuse VUE) was almost exclusively found in APD placentas (10% of cases) and in IPD placentas (5% of cases) (see Figure 2(G)). A grade 1 chronic villitis (low grade focal VUE) was present in 8-18% of placentas from all groups. Chronic villitis was more often observed in low weight placentas, in both control groups the incidence of VUE was 32%, 22% and 14% in respectively placentas with a weight below the 10th percentile, with normal weight or a weight above the 90th percentile. In all study groups combined these percentages were 33%, 22% and 21% respectively.
Umbilical cord pathology
The placentas from all infants that died (APD, IPD and ND cases) had an incidence of 23 - 24% of hypercoiled umbilical cords (Figure 2(B)). The incidence of hypercoiling in placentas from neonates admitted to the NICU was 15% and for the NPVD group 2% and for the NPEC group 6%. Undercoiling was not associated with adverse outcome at term. In the IPD and ND group no abnormal long cords were present and in the other four groups (NPVD, NPEC, APD and NS) the incidence was between 2 and 8%.
Thrombosis
Thrombosis was observed in 14-25% of cases in the study groups with the highest incidence in the ND placentas (Figure 2(D)). In the NPVD and NPEC placentas it was observed in 6.1 and 9.5% of cases respectively.
Acute inflammation
The lowest incidence of chorioamnionitis was found in NPEC placentas (5.7% of cases with grade 1 and none with grade 2 or 3) (Figure 2(E)). In NPVD placentas it was 20.4% of cases (12.9% of cases with grade 1 and 7.5% of cases with grade 2 or 3). A fetal response was rarely present in NPVD or NPEC placentas. The placentas from the study groups showed chorioamnionitis in 43–62% of cases. A fetal response (grade 1 funisitis or more) was observed in 29% and 38% of IPD and NS cases respectively.
Nucleated red blood cells
A moderate increase in NRBC was occasionally seen in the NPVD and NPEC groups (1% moderate and none severe). In the study groups a moderate or severe increase in NRBC was seen in the APD group in 49% of cases, in the IPD group in 32% of cases, the ND group in 25% of cases and in the NS group in 17% of cases.
Total number of abnormalities per placenta and cause of death
More than 70% of the placentas of the APD, IPD and NS group showed two or more of the above mentioned placental abnormalities and the ND group placentas showed two or more abnormalities in 50% of cases (Figure 2(I)). The NPVD and NPEC placentas showed none or only one abnormality per placenta in 70% and 73% of cases respectively. The most common combination of abnormalities was delayed formation of terminal villi and low placental weight (present in 38% of APD cases and 11% of cases in the NPVD group). The second most common combination was low weight and the presence of infarcts (31% of cases in APD placentas and 27% of cases in NPVD placentas). The cause of death of the neonates that died after NICU admittance, died during birth or in the antepartum period (19, 19 and 53 respectively) was classified according to the Tulip classification system. Placental bed pathology (as single entity) was found in 19% of cases, other placenta pathology (as single entity) was found in 13%, umbilical cord pathology in 10%, multiple placental pathology in 30%, infectious disease in 5% and unknown in 23%. In the latter group important information (clinical and/or pathological) was missing e.g. in almost half of these cases the placenta was not available for study.
Discussion
This study describes placental pathology in term pregnancies with a normal or adverse outcome e.g. NICU admittance or death before birth, during delivery or within the first week after birth. It is shown that abnormalities that are thought to be associated with a disturbed oxygen delivery - low placental weight, delayed villous maturation, umbilical cord abnormalities, placental infarcts and destructive chronic villitis - are significantly more often present in the placentas from children with an adverse outcome. Furthermore, multiple abnormalities are also significantly more often present in placentas from these cases compared to placentas from term neonates with normal outcome. We know of no other study in which placental pathology is directly linked to perinatal outcome of term infants and compared with cases with a favorable outcome. The strength of this study is that we prospectively collected the placentas and compared a large group of placentas from term born neonates with an adverse outcome with a large group of placentas from term born neonates with a normal outcome. All placentas were histologically examined by the same person (PGJN). A limitation of the study is that not all placentas were available. This may have introduced a bias because infants with severe asphyxia admitted immediately after birth, are over represented in our study.
The frequency of lesions found in the placentas from neonates with normal outcome are comparable with published series.14,27 The incidence of acute inflammation (both maternal and fetal response) in the placentas from a normal vaginal delivery were lower as described by Romero et al. 14 The lower incidence of acute inflammation in the placentas after an elective CS is comparable with their observation of a lower incidence in placentas from women that delivered without labor. The incidence of VUE was similar with and also the observation that in general only mild or low grade lesions are found in these placentas is comparable. 14 The difference in incidence of acute inflammation might be due to the different composition of the population studied. The observation that in most cases with normal outcome no or only one lesion is found is similar with their observation. 14 This is in contrast with the 5–15 × higher risk of adverse outcome with the occurrence of multiple lesions (2 or more).
Maternal vascular malperfusion or placental bed pathology, results in low placental weight, accelerated maturation and ischemic changes of the placental villi as well as infarcts. This study was performed before 2016 and ischemic changes were not scored according to the Amsterdam consensus conference. 24 Placental infarcts were more often observed in the study groups but in most cases the percentage of infarcted placental volume was less than 5%. In term placentas lesions of maternal vascular malperfusion (MVM), aside from low placental weight, were not an important cause of death as was published before. 28 As a single cause of death MVM was observed in 19% of cases. In 30% of cases there were multiple lesions present in the placenta as cause of death. In addition in cases with ante partum death a low placental weight present in 50% of cases was in almost 80% of these cases combined with other lesions (e.g. an overcoiled cord or VUE) that might have contributed to fetal death (data not shown). Lesions of maternal vascular malperfusion are important but as a single cause of death more often observed in the second and early third trimester but not in late third trimester. 4
The most important feature of maturation of the placenta is the formation of terminal villi. In this process the size of the villi decreases and syncytio-capillary membranes are formed, thus decreasing the diffusion distance between maternal and fetal blood. In the last weeks of pregnancy the placenta hardly increases in weight but the oxygen demand of the fast growing fetus is increasing and this maturation of the placenta is essential for increasing the oxygen supply to the fetus. Only in a few papers is diffusion distance mentioned as an important feature of the maturing placenta.1,2,29,30 In several studies this delay in formation of terminal villi was associated with perinatal mortality.16,25,31 This decrease in the distance between maternal and fetal blood in the last weeks of pregnancy has a profound effect on the oxygen levels in the fetal blood and it was recently demonstrated that this was associated with higher concentrations of amniotic fluid erythropoietin levels. 1 We observed a higher incidence of delayed villous maturation in all groups as compared with other studies, most likely due to our definition used and scoring milder cases or cases with focal occurrence as well as was described in a previous paper. 16 The incidence in our papers is also higher as compared with a study using CD15 immunohistochemistry. 30 In our study we also demonstrated that an absent or delayed formation of syncytio-capillary membranes was significantly associated with antepartum death. A remarkable finding was that in 38% of APD placentas delayed formation of the syncytio-capillary membranes (delayed maturation) was combined with a low weight placenta. This is in contrast with the observation that in placentas from neonates with normal outcome a diminished formation of terminal villi was associated with a higher weight of the placenta.
Villitis of unknown etiology (VUE) might be due to a maternal allograft rejection and maternal anti-fetal graft-versus-host disease as was recently suggested. 32 VUE can be graded as mild, moderate or severe or grade 1–3 depending on the amount of villi affected by the destructive chronic inflammation. The incidence of mild or grade 1 VUE in our population was between 8–18% in all groups without significant differences and this is comparable with or slightly higher with previous data and this might be due to relative increased sampling of placental parenchyma used in our study.14,33–36 The presence of grade 1 VUE was not associated with an adverse outcome. A moderate or grade 2 VUE was more common in the IPD and APD placentas and high grade diffuse (grade 3 in our study) VUE was almost exclusively seen in these two groups. It is likely that this loss of parenchyma is enough to explain intra-uterine mortality or mortality during birth. The diagnosis of severe VUE is important because of to the high recurrence rate in following pregnancies. 37
In this study we found that increased coiling, i.e. a coiling index of more than 0.3, is significantly associated with adverse outcome. The presence of an hypercoiled cord is 9-14 times more often present in the ND, IPD and APD groups and almost 7 times more present in the NS group. These data are in concordance with previous studies although in most studies risk ratios were not mentioned.15,22,38,39 The precise mechanism as to why hypercoiling is associated with an adverse outcome is unknown but may be due to increased hemodynamic forces with detrimental effect on the neonatal heart.40–42
Acute inflammatory lesions could be due to an infection but especially at term in many cases it is a non-infectious reaction.14,43,44 Both chorioamnionitis (maternal response) and funisitis (fetal response) was observed more often in the study groups. The highest incidence of a fetal response was observed in the IPD and NS group. In the NPEC group the lowest incidence of chorioamnionitis was found and there was almost no fetal response present as was described before. 45
Most of the placental abnormalities observed are supposed to result in a diminished oxygen supply to the fetus. The significantly increased number of NRBC in the fetal circulation of the study groups point to this diminished oxygen supply as well. Each single abnormality mentioned above may, in some cases, explain the adverse outcome. However, more than 70% of the placentas of the APD, IPD and NS group and 50% of the placentas of the ND group, showed two or more of the above mentioned placental abnormalities that could be hold responsible for the adverse outcome. Using the Tulip classification this was highlighted as well, in 30% of cases multiple placenta pathology was used to classify death of the neonates. In contrast, two or more abnormalities were only observed in 17-20% of the NPVD and NPEC placentas. Furthermore, when a combination of abnormalities was found in the control groups it was usually a combination of minor abnormalities like a grade 1 villitis or chorioamnionitis with a low weight placenta or infarction of less than 5%. It could be speculated that senescence of the placenta results in accumulation of several abnormalities hampering oxygen delivery to the fetus and that this combination of abnormalities is responsible for the adverse outcome. The most frequently encountered combination of abnormalities was delayed formation of terminal villi and a low weight placenta (present in 38% of APD cases and in 11% in the NPVD group). Both entities are able to hamper oxygen delivery. The second most frequently found combination both in APD placentas and NPVD placentas was the maternal malperfusion combination of a low weight placenta and the presence of infarcts in respectively 31 and 27%.
In summary: placentas including the umbilical cord of term infants with perinatal mortality or severe morbidity show a diversity of pathological entities. With the exception of acute intrauterine inflammation all other pathology are thought to result in a decreased oxygen exchange between mother and fetus thus explaining the adverse outcome. In the majority of cases a combination of two or more pathological entities is found and this combination results in an even greater decrease in oxygen exchange. Investigation of the placenta in case of an adverse outcome is of the utmost importance. First; it gives valuable information on the cause of adverse outcome for both parents and clinicians. Secondly; it can have implications for a next pregnancy for instance if a severe VUE was diagnosed with its associated high risk of recurrence. Thirdly; it contributes to an understanding of the epidemiology of perinatal morbidity and mortality and fourthly it may stimulate research in finding markers or other clinical signs to predict placental function at term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.