
Abstract
Fetal urinoma is defined as an encapsulated accumulation of extravasated urine within the perirenal space or retroperitoneum. It is an uncommon finding in prenatal practice, and the vast majority of known cases are strongly associated with the existence of a urinary obstruction, such as posterior urethral valves, ureteropelvic junction obstruction, or ureterocele. We report a unique case of prenatally detected fetal bladder urinoma that occurred in the absence of an apparent obstructive uropathy, but was associated with extensive ischemic necrosis and calcifications of adjacent bladder wall, coexistent with signs of vascular supply decompensation.
Introduction
Urinoma is a cystic mass formed by extravasated urine encapsulated in the perirenal fascia or retroperitoneum. 1 The formation of an urinoma requires a urine-producing kidney and leaking collecting system. The proposed etiologies of leakage include different types of urinary tract obstruction, neoplastic or iatrogenic causes. 2 However, there are no published cases of urine leakage resulting from bladder wall ischemic necrosis in fetuses.
The differential diagnosis of a cystic mass located between the kidney and the spine apart from urinoma includes: neuroblastoma, lymphangioma, extralobar pulmonary sequestration, congenital adrenal hyperplasia, partial multicystic dysplastic kidney, renal duplication, gastric duplication cyst, splenic cyst, bronchogenic cyst 3 and the differential diagnosis of paravesical cyst includes diverticulum of the bladder, duplication cyst and seminal vesicle cyst. 4
Case Report
A 31-year-old woman G2P1 with uneventful medical history and pregnancy was admitted to the Department of Obstetrics and Gynecology at Rabin Medical Center with preterm uterine contractions and suspected fetal hydrops on 25 + 5 weeks gestation. Ultrasonographic examination revealed a male fetus with massive ascites. Additionally, an enlarged urinary bladder with thick partially contracting walls and non-vascularized septate cystic mass measuring 39 mm adjacent to its right posterior wall was noticed (Figure 1(A) and (B)). There were no signs of urinary obstruction, generalized hydrops or other fetal anomalies. Middle cerebral artery peak systolic velocity and cardiac functions were normal, therefore fetal hydrops and fetal anemia were ruled out. The patient underwent fetal abdominal paracentesis and 100 cc of clear and slightly reddish fluid was aspirated. Peritoneal fluid biochemistry analysis confirmed the urinary origin. The fetal ascites recurred on the next day, and the patient opted for termination of pregnancy.
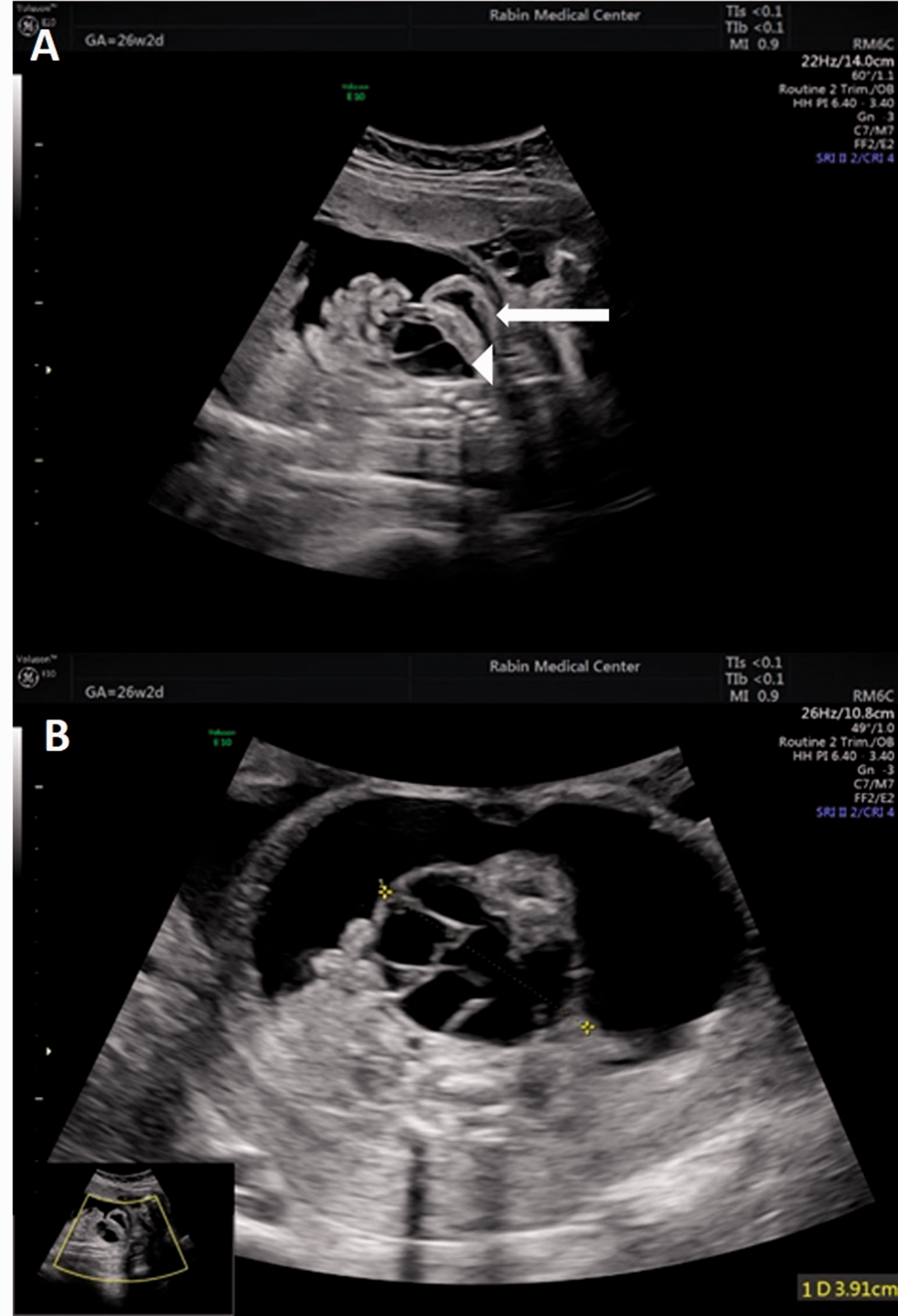
Fetal ultrasonographic findings. A, Sagittal view demonstrating ascites, thick urinary bladder (arrow) with cystic mass adjacent to its posterior wall (arrowhead). B, Axial view demonstrating a septate cystic mass measuring 39 mm adjacent to posterior wall of the urinary bladder, embedded in clear abdominal fluid.
At autopsy, a male fetus, 26 weeks of gestation, weighing 1,078 gr appeared appropriate to gestational age with mild maceration and autolysis. On external examination the abdomen was markedly dilated. No other abnormalities were noted. Internal examination disclosed 50 cc of transparent fluid in the abdominal cavity, enlarged urinary bladder with thick firm wall, and cystic mass adjacent to the bladder wall. The cystic mass was adherent to the right posterior wall of the bladder and separated from all other abdominal organs and viscera. The lungs weighed 15.3 gr, with a lung/body weight ratio of 0.014, that was consistent with mild hypoplasia. 5 In addition the right umbilical artery was displaced anteriorly (Figure 2).
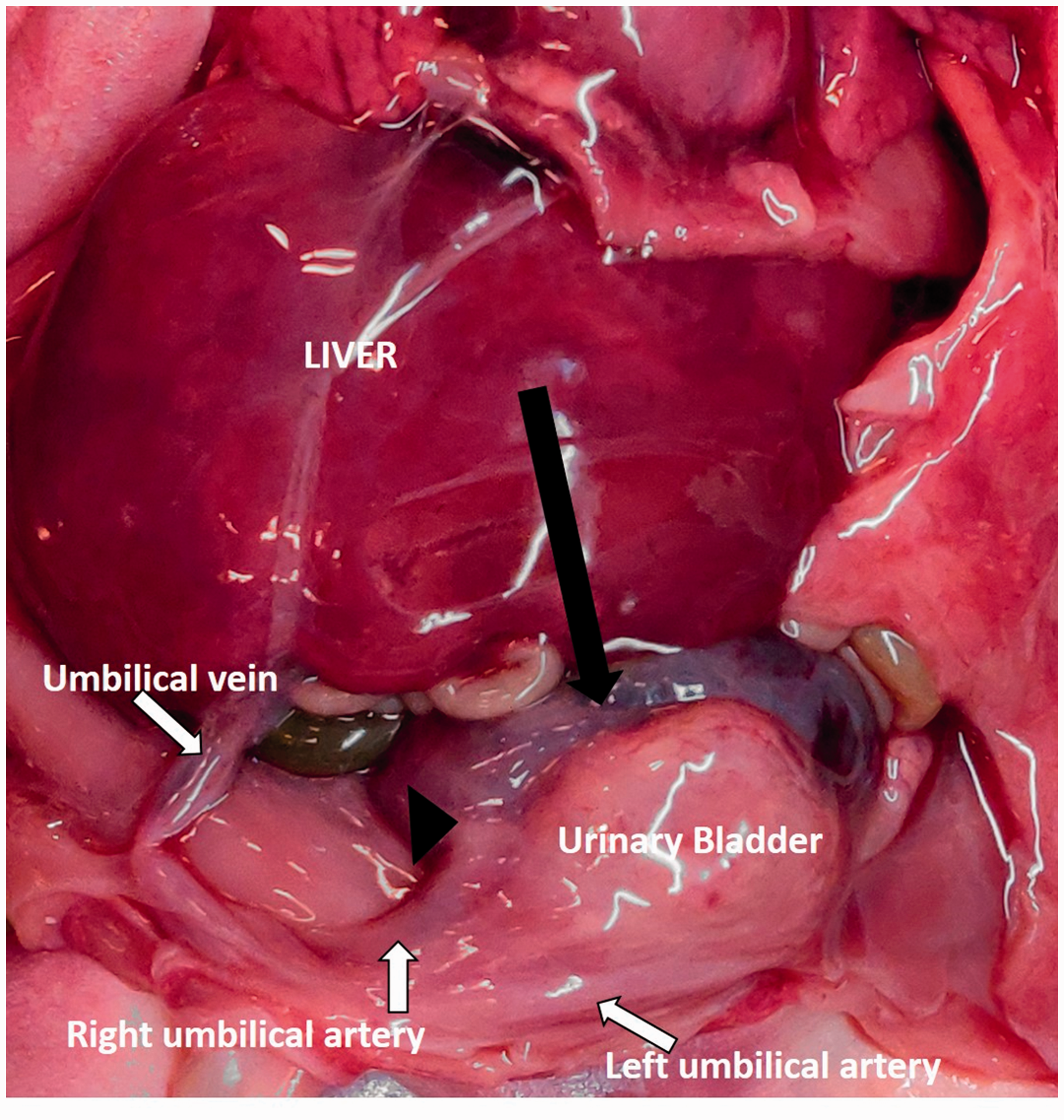
Abdominal and pelvic organs at autopsy: urinoma adjacent to the posterior wall of the bladder (black arrow), anteriorly displaced umbilical artery (black arrowhead).
On histologic sections, the right posterior bladder wall was almost fully necrotized with extensive calcifications (Figure 3(A)). At the level of bladder neck, the necrosis was transmural and involved the entire circumference of bladder. (Figure 3(B)). Blood vessels filled with thrombotic material were seen (Figure 3(C)). Immunostaining for iron and CD61 was performed to confirm the findings (Figure 3(D)).

Histologic features of urinary bladder. A, Transmural necrosis with calcifications throughout the bladder wall (Arrows: asterix = lumen of bladder, double asterix = lumen of urinoma) (H&E, ×20). B, Discontinuity in detrusor muscle of bladder wall due to necrosis, demonstrated by Desmin immunostain (Arrows: asterix = lumen of bladder, double asterix = lumen of urinoma) (X40). C, Arrow: blood vessels filled with thrombotic material and calcifications (H&E, ×100). D, Thrombi in venules of bladder. The thrombi are rich platelets, demonstrated by CD61 immunostain (Arrows: CD61 immunostain, ×100).
The cystic mass was unilocular, with thin strands of fibrin-like material floating in its cavity, most probably consistent with septa noted on ultrasonographic examination (Figure 4(B)). The wall was composed of loose fibrous tissue devoid of endothelial or epithelial lining. Immunostaining for CD31, D2-40, P63, and pan-cytokeratin keratin failed to show any lining (Figure 4(C)) and supported the diagnosis of urinoma. No signs of bladder neck obstruction were identified.
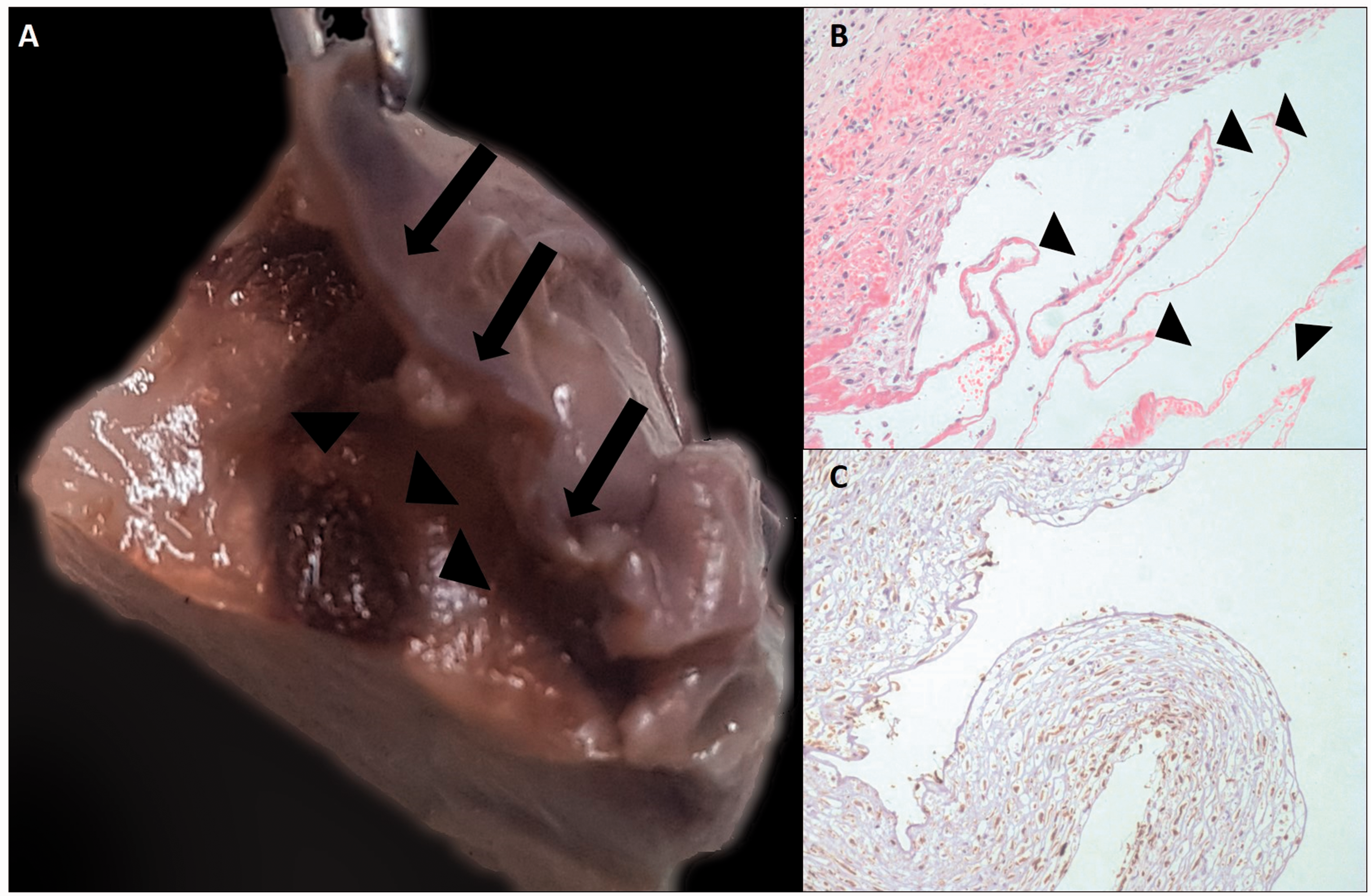
Features of urinoma. A, Arrows: urinoma adjacent to posterior wall of bladder (arrowheads), which is partially necrotic. B, wall of the urinoma, composed of loose fibrous tissue with thin threads of fibrin- like material (arrowheads) (H&E, ×100). C, Wall of urinoma, lacking any epithelial lining (Pan-cytokeratin immunostain, ×100).
Term placenta (weight on the 90th percentile for 26 weeks of gestation) showed changes compatible with fetal death in utero with no other abnormalities.
Discussion
Here we present a rare case of isolated fetal ascites and urinoma adjacent to the necrotic bladder wall. Various mechanisms might lead to isolated fetal ascites (i.e., without other signs of hydrops), including abnormal lymphatic drainage, obstruction of venous return (as observed in space-occupying lesions in the thorax), cardiac failure, decreased plasma oncotic pressure (i.e., fetal anemia), hepatic insufficiency (e.g., storage diseases), congenital nephrosis, urinary tract obstruction, or meconial peritonitis. 6 Furthermore, infections such as congenital syphilis, cytomegalovirus (CMV), varicella, toxoplasmosis, and hepatitis A can cause fetal ascites in rare cases. 7 While the prevalence of fetal hydrops ranges from 1/800 to 1/3500 live births, the true prevalence of isolated fetal ascites is unknown. 8
Fetal urinoma is such an uncommon finding in prenatal practice that it is described mainly in case reports. It can result from traumatic amniocentesis; 9 however, most reported cases are associated with obstructive uropathy, usually secondary to posterior urethral valves, or ureteropelvic junction obstruction.2,10
Increased pressure secondary to the obstruction leads to extravasation of urine into the perirenal fat, followed by lipolysis and inflammatory reaction with the consequent formation of a fibrous sac around the collected urine. 11 The extravasated urine can be presented in the form of a localized collection such as urinoma or generalized, e.g., ascites or rarely pleural effusion. 12 It can be assumed that the amount of urine is responsible for the formation of either urinoma, in cases of slow leakage, or ascites in cases of simultaneous release of large amounts of urine. Moreover, there are several reported cases of urinary ascites secondary to urinary bladder rupture in premature neonates. 13 There was the histological appearance of an ischemic injury to the bladder in one case, described as a necrotic area showing a calcified healing area of ischemic muscle without signs of bladder rupture and inflammatory change, apart from a thick coat of fibrin on the peritoneal surface of the bladder and other intraperitoneal organs. 14
Although the abovementioned cases were described in premature neonates that seem to be more susceptible to ischemic injury than fetuses, 15 the present case was compounded by the anterior displacement of right umbilical artery. The umbilical artery gives rise to the superior vesical arteries (their number varies from one to five) and its distortion could lead to vascular compromise with resulting ischemic necrosis in bladder wall.
In consideration of the forgoing evidence, the urinoma could be a localized presentation of slow urine outflow due to bladder wall defect resulting from ischemic necrosis. Hence, the larger volume of urine in the peritoneal cavity because of defect's persistence or bladder rupture is responsible for the consequent development of urinary ascites.
We described the first case of fetal urinoma associated with bladder wall ischemic necrosis. Distorted umbilical artery is likely to be associated with vascular compromise followed by ischemic necrosis. Slow extravasation of urine throughout the necrotic wall resulted in the formation of urinoma, and subsequently in ascites.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.