
Abstract
Background
Absent submucosal ganglion cells in biopsies 1-3 cm above the pectinate line establishes the pathologic diagnosis of Hirschsprung Disease (HD). Calretinin stains both ganglion cells and their mucosal neurites and has gained importance in HD diagnosis. Absent calretinin positive mucosal neurites in biopsies at the appropriate level above the pectinate line is highly specific for HD. Whether this applies to lower biopsies is uncertain. To address this, we studied anorectal canal autopsy specimens from infants.
Methods
We performed an autopsy study of infant anorectal canal specimens to describe calretinin staining in this region. Calretinin staining was correlated with histologic and gross landmarks.
Results
In all 15 non-HD specimens, calretinin positive mucosal neurites were present in glandular mucosa up to the anorectal line where neurites rapidly diminished. Age range was preterm 26 weeks to 3 months.
Conclusions
Calretinin positive mucosal neurites are present in glandular mucosa up to the anorectal line in young infants. This is potentially important regarding neonatal HD biopsy level and diagnosis. Positive calretinin staining at the anorectal line favors normal innervation making HD unlikely. Absent calretinin positive neurites in glandular mucosa is worrisome for HD in young infants, regardless of location.
Background
Hirschsprung Disease incidence is 1/5000 to 1/10000 births per year. Surgical correction requires a major procedure while failure to diagnose can lead to significant morbidity and death. It results from deficient neuronal population of the gastrointestinal tract, which, in the vast majority of cases, produces a single segment of distal aganglionosis and dysmotility. Length of intestinal involvement is variable. Very short segment disease is less than 2cm. Short segment is limited to the rectosigmoid colon and is the most common type. Longer segments extend beyond the rectosigmoid colon, can involve the entire colon, and rarely involve the small intestine. 1 A typical case in infancy presents with abdominal distention, failure to pass meconium, and a contrast enema with transition zone and rectosigmoid ratio of less than one. In infants, the most common next step is suction rectal biopsy to confirm the diagnosis. Diagnostic criteria emphasize obtaining a 3mm biopsy that is 1–3cm above the pectinate line with enough submucosa to identify ganglion cells. A 1cm biopsy is more appropriate for newborns and young infants while higher biopsies are needed in older patients. Absent submucosal ganglion cells in an adequate biopsy is diagnostic of HD. Submucosal nerve hypertrophy supports HD with the caveats that this is not always present and is only useful in the infant age group. Absent calretinin positive neurites in the mucosa is also strong evidence if not pathognomonic for HD. For this reason calretinin immunohistochemical staining of biopsies has gained wide use. It is also relatively easy to perform and interpret on paraffin sections with few technical considerations.1–4 Acetylcholinesterase overexpression in mucosal neurites is often present, but this requires a difficult enzymatic staining technique on a separate frozen biopsy piece. Immunohistochemistry for choline transporter may be a substitute for acetylcholinesterase staining but both of these stains can be difficult to interpret. 1 Aganglionic segments of 4cm or less are particularly challenging because of the requirement to biopsy 1-2 cm above the pectinate line. Overly proximal biopsies risk false negative results, and overly distal biopsies risk false positive results. Recent reviews summarize and expand on the biopsy techniques and pitfalls.1,5
The suction rectal biopsy technique was established and validated by autopsy studies that mapped the distribution of ganglion cells in the submucosa of the anorectal canal in infants and children.6–8 The early study by Aldridge and Campbell 6 used the pectinate line as a reference point and defined the physiologic hypoganglionic zone as the distance between the pectinate line and the last submucosal ganglion cell on longitudinal section. By this definition, the hypoganglionic zone measured approximately 2cm. This meant biopsies within 2cm of the pectinate line would risk false positive diagnosis as submucosal ganglion cells could be missed. Myenteric ganglion cells extended farther than submucosal ganglion cells, meaning submucosal ganglion cells predicted myenteric ganglion cells and only submucosa needed to be sampled. Later studies and a more recent review indicate that biopsies in infants can be lower than 2cm with respect to the pectinate line if there is enough submucosa and serial sections are examined.1,8 Higher biopsies are necessary in older patients. Other current recommendations are that biopsies be completely covered by colonic glandular epithelium meaning biopsies with any transitional mucosa or squamous mucosa from the anorectal line should be considered inadequate. 1 In current practice, biopsies are localized 2-4cm from the anal verge and this approximates biopsies that are 1-3cm proximal to the pectinate line. Biopsying at multiple levels helps assure sampling that is neither too high nor too low. Equivocal findings, size of biopsy and uncertainty of biopsy level can result in re-biopsy rates of 30%. 9 The ability to interpret lower biopsies with less emphasis on required biopsy levels could potentially reduce the need for re-biopsy, increase diagnostic accuracy, and help identify shorter segment cases. Since negative calretinin mucosal staining is virtually diagnostic of HD in traditional biopsies taken 1-3cm above the pectinate line, we wondered if this could be applied to lower biopsies. To address this question, we decided to modify the previous autopsy studies by adding calretinin staining in order to describe the extent of calretinin positive mucosal neurites in the anorectal canal and physiologic hypoganglionic zone of infants.
Materials and Methods
Institutional review board approval was obtained for the study. Anorectal autopsy specimens were obtained from 16 sequential autopsies including preterm and term infants less than one year of age. Recorded patient information included patient gestational age at birth, age at death, and major clinical diagnoses. Postmortem interval at the time autopsy was estimated based on date and time of death and date of autopsy. Anorectal canal specimens included skin at the anal verge and at least 6cm of proximal colon. Specimens were opened, oriented, and photographed to allow correlation of histologic features with gross and surgical landmarks. Specimens were then rolled, pinned and fixed in formalin. Two longitudinal roll sections were prepared to include the entire length of the specimens. Paraffin embedded sections were stained with standard hematoxylin and eosin (HE), and a single strip was chosen for calretinin and smooth muscle actin immunohistochemistry and measurements. HE and smooth muscle actin were used to delineate the microscopic anatomy. HE and calretinin were used for ganglion cell mapping. Measurements were made using a digital camera. Mucosal calretinin staining was correlated with ganglion cell distribution and histologic landmarks. We used the original definition of Aldridge and Campbell and measured the hypoganglionic zone as the distance between the pectinate line and the last submucosal ganglion cell on longitudinal section. Immunohistochemical staining for calretinin and smooth muscle actin was performed using monoclonal primary ready to use antibodies with epitope retrieval (PH 9.0), DAB detection, and automated staining.
Results
The study included 15 non-HD infants and one HD infant. The non-HD infants included 11 infants born preterm and 4 infants born at term. After correcting for gestational age at death, eight cases remained in the preterm category while seven fell into the near and post term category. Average age in the corrected preterm category was 31 weeks (range 26–36 weeks). The near and post term category included one near term infant with corrected age of 39 weeks and six post term infants. Average age of the post term infants was 6 weeks with 3 infants less than one month of age and 3 infants greater than one month of age (range 1–12 weeks). The HD infant was 8 months of age.
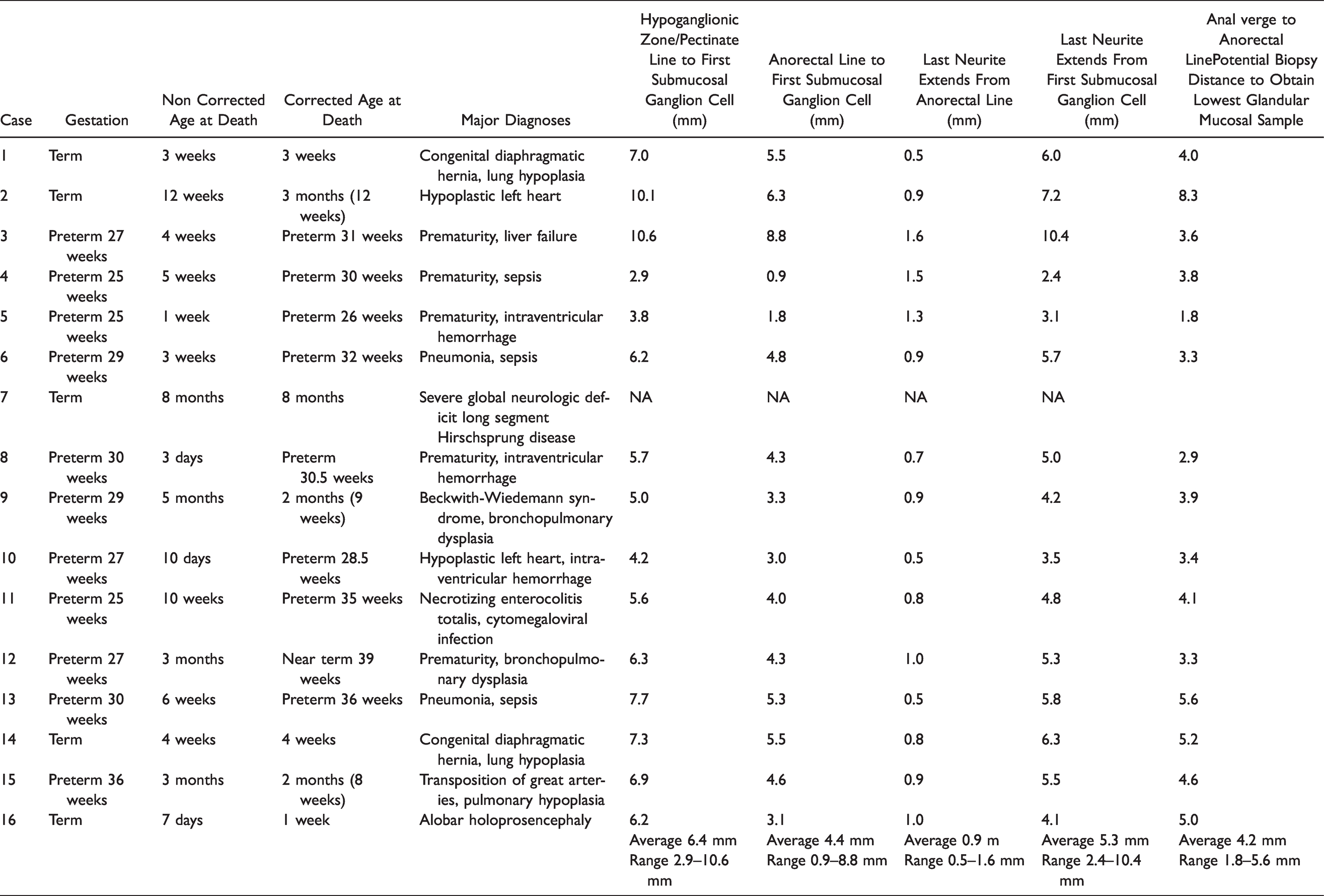
The skin to squamous junction just above the anal verge was the most prominent gross landmark. The pectinate line, anal columns, and anorectal line could be vaguely discerned but required correlation of gross and microscopic measurements (Figure 1). HE and smooth muscle actin staining allowed detailed evaluation of the microscopic anatomy. The glandular mucosa had mild to moderate autolysis. Calretinin staining was well-preserved and not affected by autolysis or postmortem interval, which ranged from 8–48 hours. Smooth muscle actin helped delineate the region of the anorectal line where a discreet muscularis mucosae broke up into dispersed muscle fibers and colonic glandular epithelium changed to non-glandular transitional mucosa. Smooth muscle actin also helped define the pectinate line, where subepithelial smooth muscle fibers stopped completely and transitional mucosa changed to squamous mucosa at the base of the anal valves. Figure 2 includes a longitudinal section stained with smooth muscle actin and a corresponding schematic from case 15. The schematic illustrates ganglion cell distribution on longitudinal section and adds the extent of calretinin positive mucosal neurites. This figure includes definitions and terminology for which comprehensive reviews are available.1,10 Ganglion cell distribution and measurements agreed with those of previous studies.6–8 Length of the hypoganglionic zone was variable and tended to increase with patient age (Figure 3). Patient information and measurements are listed in Table 1. Average length of the physiologic hypoganglionic zone was 6.4mm. The anorectal line was always distal to the last submucosal ganglion cell and within the hypoganglionic zone. Average length of the proximal portion of the hypoganglionic zone lined by glandular epithelium was 4.4mm. The average distance from the anal verge to the anorectal line was 4.2mm. Calretinin positive neurites were readily apparent and diffusely present in the lamina propria of the glandular epithelium and muscularis mucosae up to the anorectal line (Figure 4). In general they were more frequent in the muscularis mucosae than in the lamina propria. They were not diminished relative to the more proximal rectosigmoid mucosa. Neurites on longitudinal section were thin and beaded with granular staining. On cross section the neurites appear as dots or granules. Neurites could be readily seen at 100X but were best seen at 200–400X. The neurites abruptly diminished at the anorectal line where the glandular mucosa and muscularis mucosae stopped. Only a few sparse calretinin positive neurites, mostly in the form of granules and dots, were seen beyond the glandular mucosa in the upper portion of the anal columns. This staining extended on average 0.9 mm beneath the transitional epithelium. The average distance between the last submucosal ganglion cell and the last neurite was 5.3 mm. Ranges and average distances are listed in Table 1. Figure 5 is an en face longitudinal schematic of the submucosal ganglion cell distribution, measurements, and calretinin staining in relationship to histologic and anatomic landmarks for case 15.
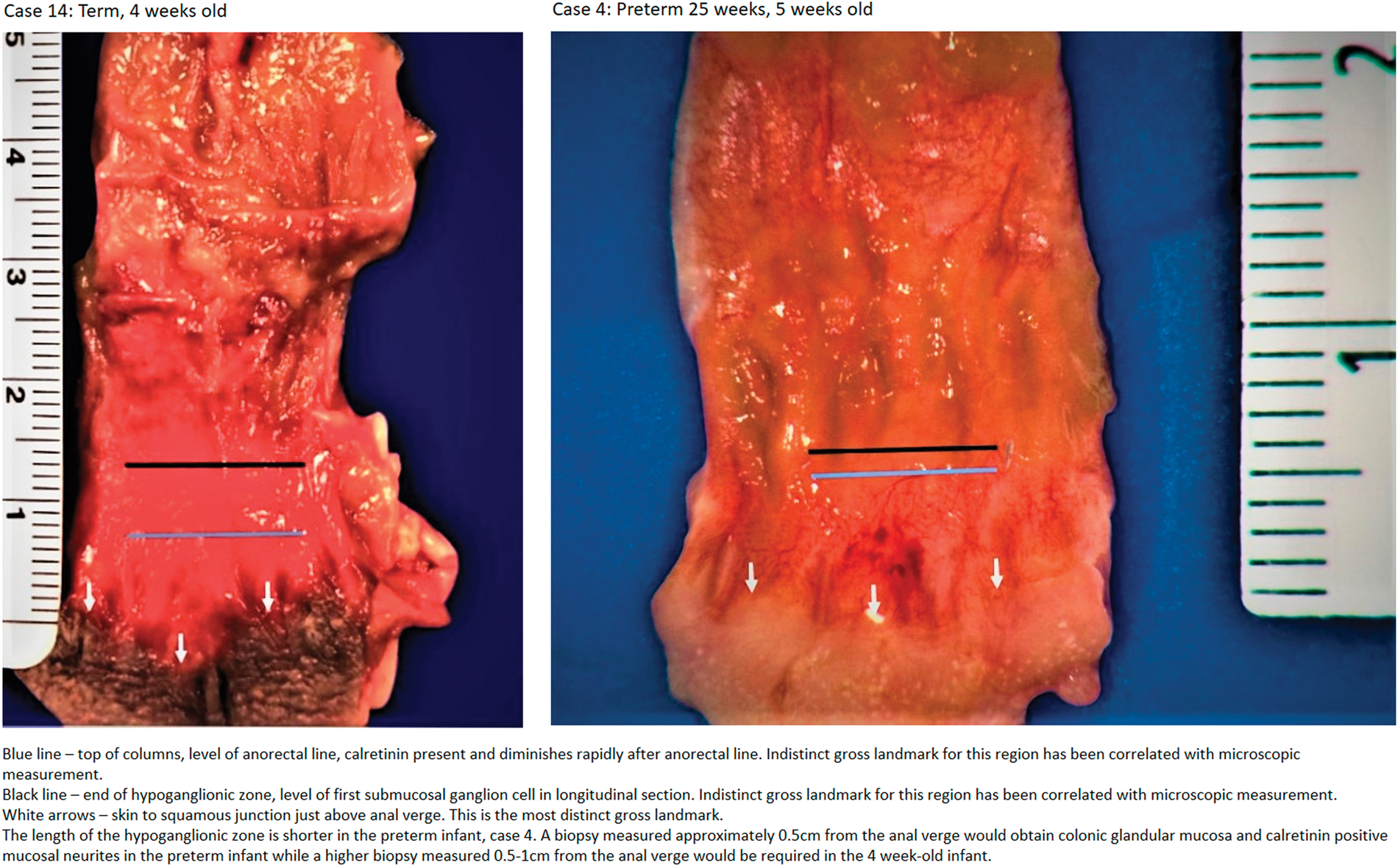
Microscopic to gross correlation for anorectal line, top of columns, and hypoganglionic zone.
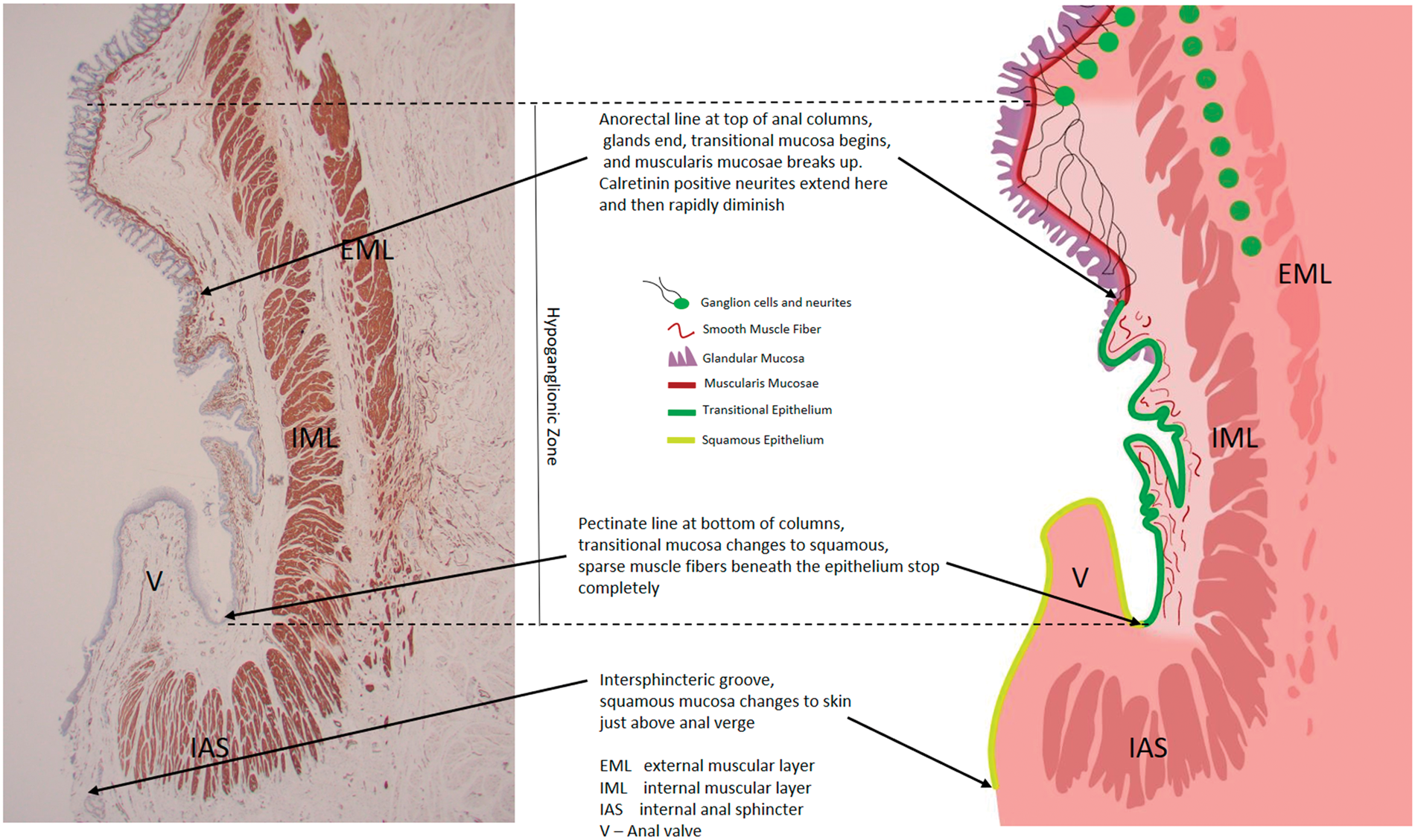
Case 15 smooth muscle actin with schematic longitudinal section.
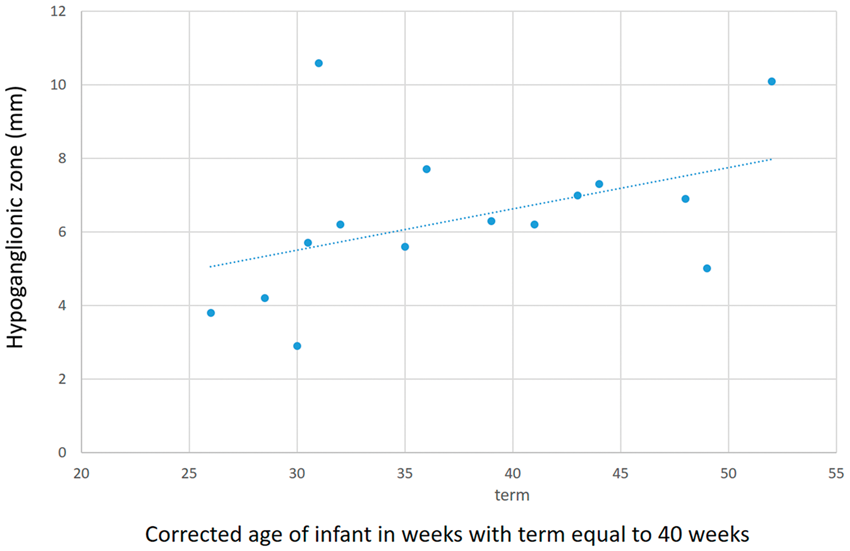
Trend of increasing length of hypoganglionic zone with corrected age.
Patient Data and Measurements of Extent of Calretinin Mucosal Neurites in Hypoganglionic Zone.
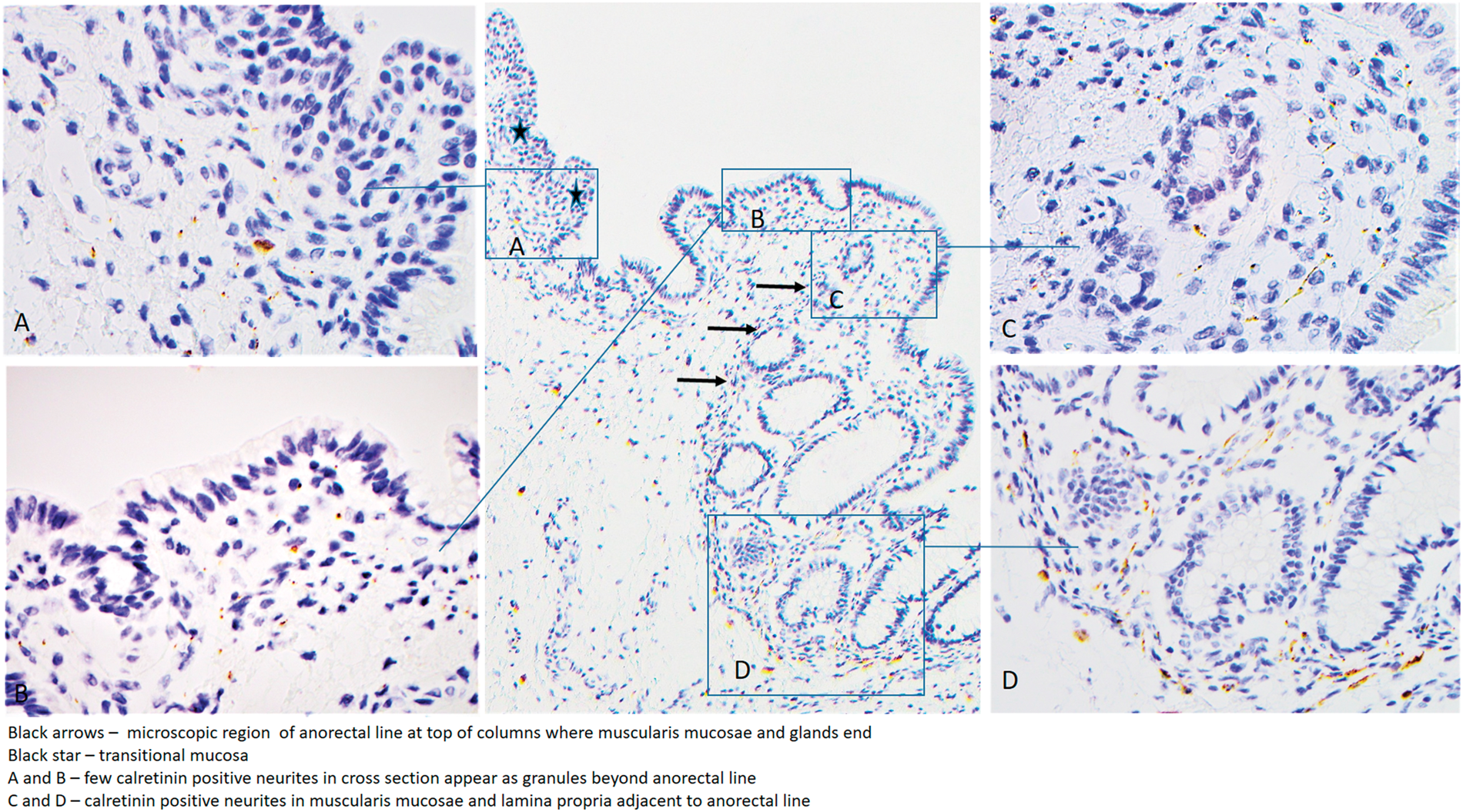
Calretinin staining in the region of anorectal line.
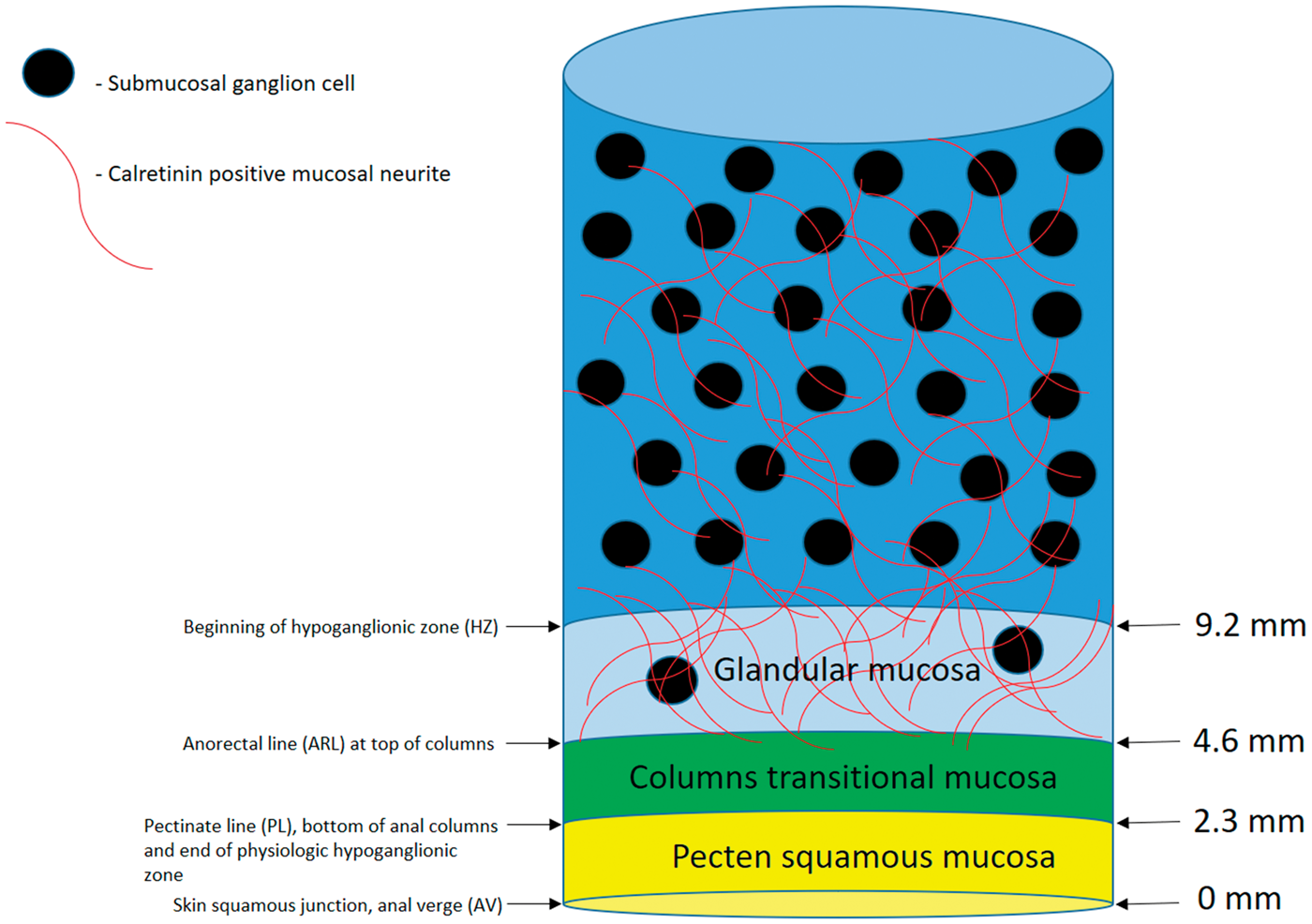
Schematic representation of neurites in relationship to gross and microscopic landmarks with measurements for case 15. The neurites are abundant in the glandular mucosa. Sparse neurites extend approximately 1mm beneath the transitional mucosa of the anal columns.
The single HD case was long segment HD with an aganglionic length of 20cm. This was an unsuspected and undiagnosed HD case without premortem biopsy. Calretinin was negative except for mast cells in this specimen.
Discussion
The major finding of our study, which includes only young infants, is the presence of calretinin positive mucosal neurites in all glandular mucosa up to the anorectal line at which point they rapidly diminish. This finding is consistent with previous studies, suggests a modified conceptual approach to rectal biopsy, and supports exploring the use of lower rectal biopsies in the diagnosis of HD. It is possible this finding might extend to older infants and children, but additional study of cases beyond the neonatal period are needed to confirm that. Therefore, the following discussion pertains to young infants within the neonatal age group (first month of life). Rectal biopsies are often done within the first week of life, in late preterm infants, and in near term infants, so this group is important.
With regard to previous studies, our finding is compatible with what is currently known about submucosal ganglion cells and their neurites. Analysis of HD resection specimens demonstrates that calretinin positive mucosal neurites extend 2cm from the last ganglion cell, 11 so neurites should have enough length to contribute to the most distal glandular mucosa at the anorectal line. In fact, in our specimens, the neurites would only have to span an average length of 4.4mm. Since the hypoganglionic zone contains a low density of submucosal ganglion cells, one would expect them to also contribute neurites to the mucosa of this region. In addition, research on the intrinsic enteric nervous system has confirmed that the neurites originate from the submucosal ganglion cells and they are an integral part of normal glandular mucosa. They target colonic glands, smooth muscle, and vessels and have secretory, sensory, and vasomotor functions. 12 Perhaps the neurites stop at the anorectal line because that is where the targets stop as their sole or main role is glandular mucosal innervation and signaling to the myenteric plexus. Finally, our finding helps explain why a small retrospective study found calretinin staining to be diagnostic in inadequate mucosal only biopsies and biopsies from the anorectal line with partial squamous or transitional mucosa. 13
With regard to the conceptual approach to rectal biopsy, there are two main issues. First, our finding may potentially alleviate concerns over false positive diagnoses related to low biopsies within the hypoganglionic zone. Calretinin staining is a highly sensitive way to detect the presence of nearby ganglion cells and likely much more sensitive than searching serial HE sections for ganglion cells in the submucosa. Since neurites appear to be present in all glandular mucosa, their absence in a 3mm sample of this mucosa could be diagnostic of HD regardless of location. Second, our finding suggests a way to more completely evaluate the extent of mucosal innervation, something not currently addressed due to the prohibition against low biopsies. The more distal the biopsy, the more significant is the presence of calretinin positive mucosal neurites. Their presence at the anorectal line is strong evidence that submucosal neuronal migration is sufficient enough to allow for complete mucosal innervation. In nearly all cases, this should assure intact submucosal and myenteric plexuses. This would leave only rare variant HD cases for exclusion such as very short segment HD, skip lesions, hypothetical transition zone variant, and myenteric hypoganglionosis. For diagnosis of these variants, other detection methods would be needed. 14
As to the possibility of including lower rectal biopsies in the diagnosis of HD, this could be particularly useful when paired with traditional higher biopsies. In our cohort this would mean biopsying 1 to 1.5cm lower than current practice. The lower biopsies would likely need to be mostly (at least one half) covered by glandular mucosa. Biopsies distal to the anorectal line and completely covered by squamous or transitional mucosa would be inadequate since calretinin positive neurites are so sparse immediately beyond the anorectal line. However, a biopsy with transitional or squamous mucosa in part of the biopsy piece could be advantageous since it would histologically localize the biopsy site. If it were possible to target the anorectal line, this could also eliminate the variability of biopsy requirements due to age of patient. Submucosa in all biopsies could still be evaluated for nerve hypertrophy and ganglion cells, although the absence of ganglion cells would remain much more significant in higher biopsies. Figure 6 shows how adding a low biopsy at the anorectal line could be diagnostic in the vast majority of cases and Figure 7 illustrates potential biopsy sites on a magnified study specimen. This could be especially useful in short segment disease of 2-4cm. A lower biopsy would decrease the risk of a false negative diagnosis due to an overly proximal biopsy and might help resolve equivocal findings in higher biopsies. Biopsy intent could be to obtain glandular mucosa at or as close to the anorectal line as possible. Perhaps superficial mucosal only biopsies at the anorectal line have diagnostic potential either as adjuncts or on their own.
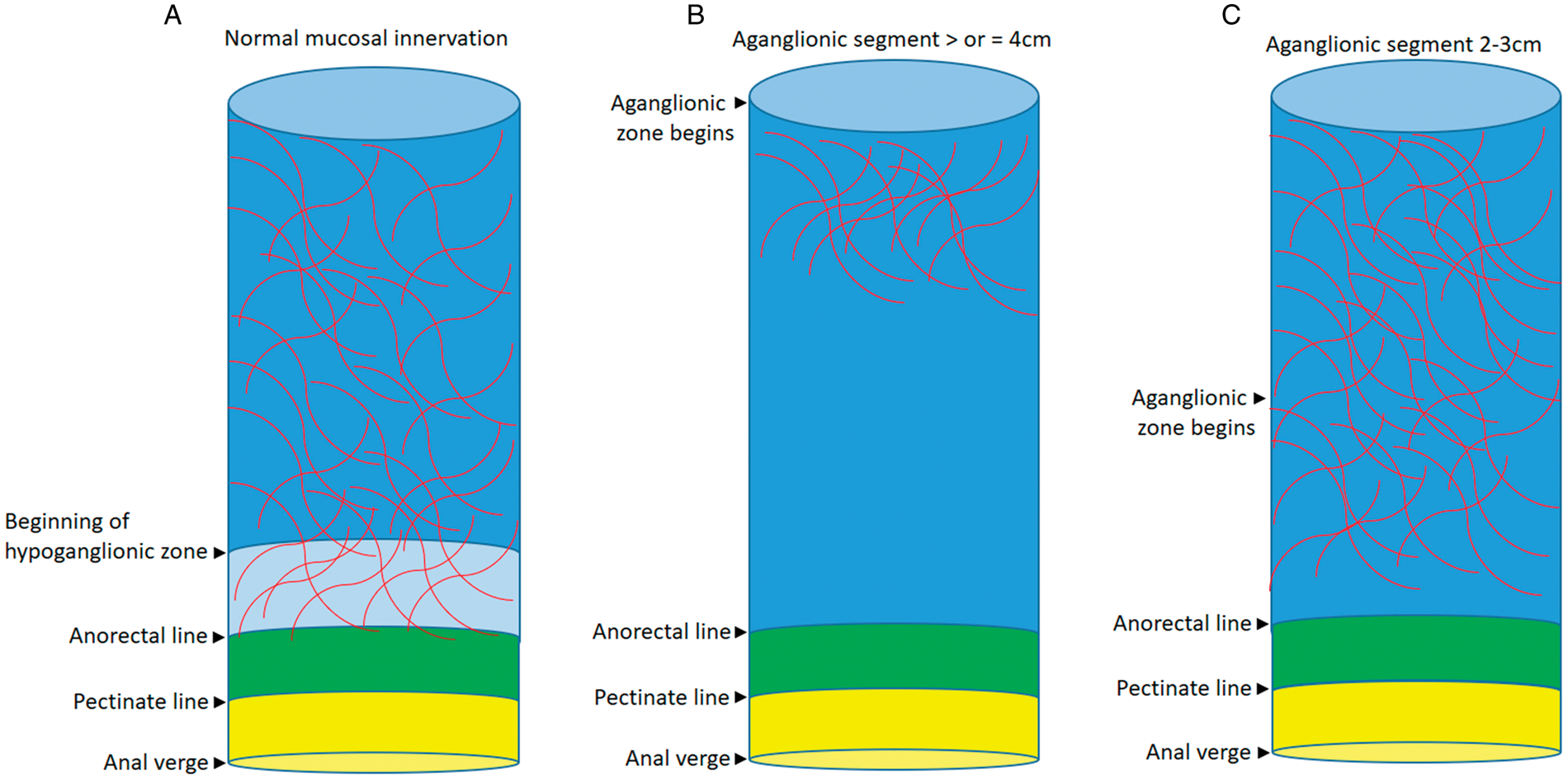
How low mucosal biopsies in the hypoganglionic zone at or above the anorectal line and including glandular mucosa can aid diagnosis in most cases of HD. A, Normal anorectal canal. All normal glandular mucosa should have calretinin positive neurites (red lines) extending to the anorectal line. A biopsy near the anorectal line will have neurites and rule out HD in most cases. B, HD greater than or equal to 4cm. Most cases of HD can be diagnosed with biopsies that contain glandular mucosa including those at the anorectal line because calretinin positive mucosal neurites will be absent. C, HD 2–3 cm. Low biopsies may be very useful for diagnosing short aganglionic segments of 2–3 cm, as the calretinin positive neurites may not reach the anorectal line.
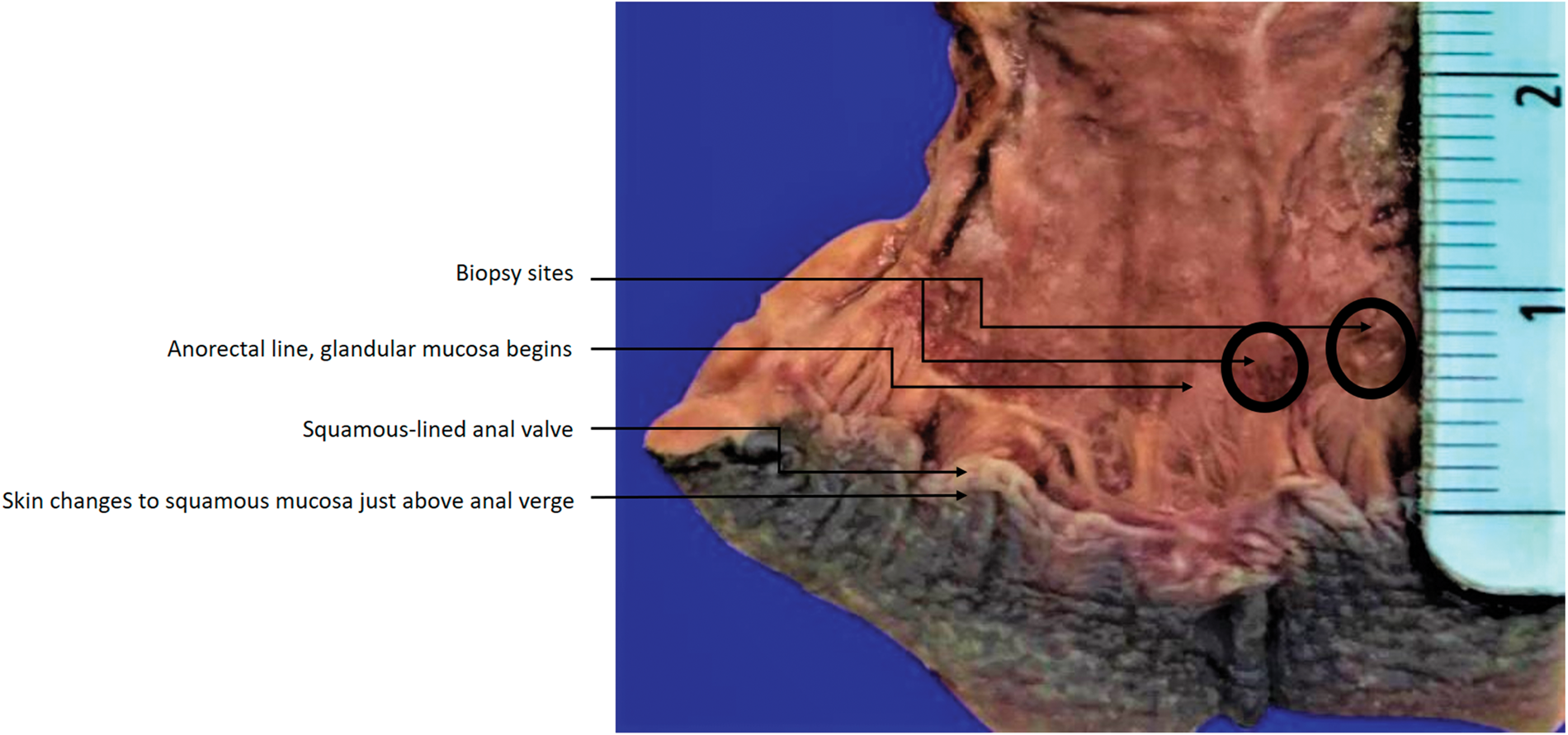
Potential biopsy sites at anorectal line on magnified specimen.
Limitations of our study should be recognized with regards to patient age, sampling of the anorectal canal, and clinical application. This is a small observational study of young infants including premature infants. How well these observations might hold up in the setting of small clinical biopsies in a wider age range is not certain. The density and staining intensity of neurites could either increase or decrease with increasing age. If the density were to decrease and this decrease be more pronounced in the hypoganglionic zone, then a small biopsy from an older infant or child at the anorectal line could be negative for calretinin positive mucosal neurites. Another limitation is the method of sampling which included two longitudinal strips, one of which was used for measurements. This sampling limits the confidence of the measurements since the anatomic zones and the leading edge of the enteric nervous system are irregular in the anorectal canal and hypoganglionic zone. This irregularity might also be a significant obstacle to localizing biopsies to the anorectal line. Expansion of this study to older infants and children, evaluation of a greater circumference of the anorectal canal, and more experience with low biopsies could address these issues.
Footnotes
Acknowledgements
The authors would like to thank the following for their dedication and help with this project. Minhui Ma, HTL, QIHC, for performing histology and immunohistochemistry, Charles Edward Love, FTS, FCMEO for autopsy assistance, Taylor-Nicole Boger, MHS, PA (ASCP) for image design and photo editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.