
Abstract
Secretory carcinoma (SC), previously known as mammary analogue secretory carcinoma, is a rare salivary gland neoplasm that typically presents as a slow-growing painless lesion in the head and neck. SC occurs mainly in adults but has been described in children with the youngest reported patient diagnosed at five years of age. In children the gender distribution has been reported as female to male ratio of 1:1.2. SC is generally considered a low-grade malignancy with characteristic morphological features and immunological profile. SC also harbors ETV6-NTRK3 fusion (t(12;15)(p13:q25)). Surgical resection with or without lymph node dissection is the standard treatment, with generally favorable clinical outcomes. Here we present a single institution case series of six patients (ages 9-21) with SC and a review of the previously described pediatric cases. Our small series showed male predominance in pediatric patients with predominantly low-grade and stage tumors. All cases underwent complete surgical resections and when follow up is available there was no evidence of recurrences or metastases. To the best of our knowledge, this is the only SC case series comprised exclusively of pediatric and youth patients.
Introduction
Salivary gland malignancies are rare in the pediatric population, accounting for <5% of childhood malignancies. 1 Secretory carcinoma (SC) of the salivary gland, formerly known as mammary analogue secretory carcinoma, is a rare entity first described in 2010 and named due to the morphologic, genetic and immunophenotypic similarities to secretory carcinoma of the breast. 2 Secretory carcinoma of the salivary gland (SC) is most common in adult patients, but has been reported in children as young as 5 years. 3
The majority of SCs are slow growing and diagnosed after incidental discovery on physical exam.2,4,5 SC can arise in both major and minor salivary glands, with the parotid gland being the most common site. 6 Biopsy and fine needle aspiration (FNA) are two methods commonly used for preoperative diagnosis. The common cytologic features include cellular smears composed of cohesive sheets of neoplastic cells and occasional papillary structures. The cells have round-to-oval nuclei and vacuolated, eosinophilic or granular cytoplasm. 7
Histologically, SCs are usually circumscribed, non-encapsulated, lobular masses divided by fibrous septae and composed of microcystic, solid and tubular structures containing abundant extracellular material. The tumor cells have generally low-grade vesicular nuclei with finely granular chromatin, and central nucleoli, surrounded by pale eosinophilic granular or vacuolated cytoplasm. Cellular atypia is usually mild and mitotic figures are typically rare. Serous acinar differentiation is not seen. Rare cases demonstrate perineural and/or lymphovascular invasion. 8 , 9 SC has a distinctive immunohistochemical profile including strong and diffuse staining of mammaglobin, GATA-3, CK7, CK8, CK18, vimentin, S-100, and SOX-10 2 , 4 , 10 and negative DOG1. 11 The majority of cases are positive for gross cystic disease fluid protein (GCDFP-15), and epithelial membrane antigen (EMA). Basal cell/myoepithelial markers, such as p63, SMA, and CK5/6, are negative. 2 , 12
In addition to the morphologic and immunophenotypic similarities, SC of the salivary gland and breast share a common genetic alteration in ETV6. The most commonly described genetic alteration is t(12;15) (p13;q25), which encodes a chimeric tyrosine kinase ETV6-NTRK3, however other non NTRK3 fusions have been reported. 13 NTRK3 gene fusions have been described in other tumors including congenital mesoblastic nephroma, congenital infantile fibrosarcoma, gliomas, soft tissue sarcomas, and colon, cervical, lung and thyroid carcinomas. 12
SC is considered a low-grade malignancy and the majority of patients have long-term disease-free survival, although local recurrence, metastases and death have been reported.14,15
Here we present a case series of salivary gland SC in the pediatric population from a single institution, with review of the clinical presentation, pre-operative diagnostic material, histologic findings, genetic studies and clinical follow-up when available. To the best of our knowledge this is the largest case series of SC composed of patients under 21 years of age.
Case Series
With IRB approval, using a retrospective laboratory information system data search from 5/1/2010-11/30/2019, we identified six cases of SC in children and adolescents (age 9-21) with pathology reviewed at our institution, either in-house or through consultation. Our cases showed a male predominance, with a male-to-female ratio of 5:1. None of the patients had significant past medical history. Table 1 shows a summary of the clinical and pathologic findings.
Demographics, Clinical and Histologic Findings of Six Pediatric Patients With Secretory Carcinoma.
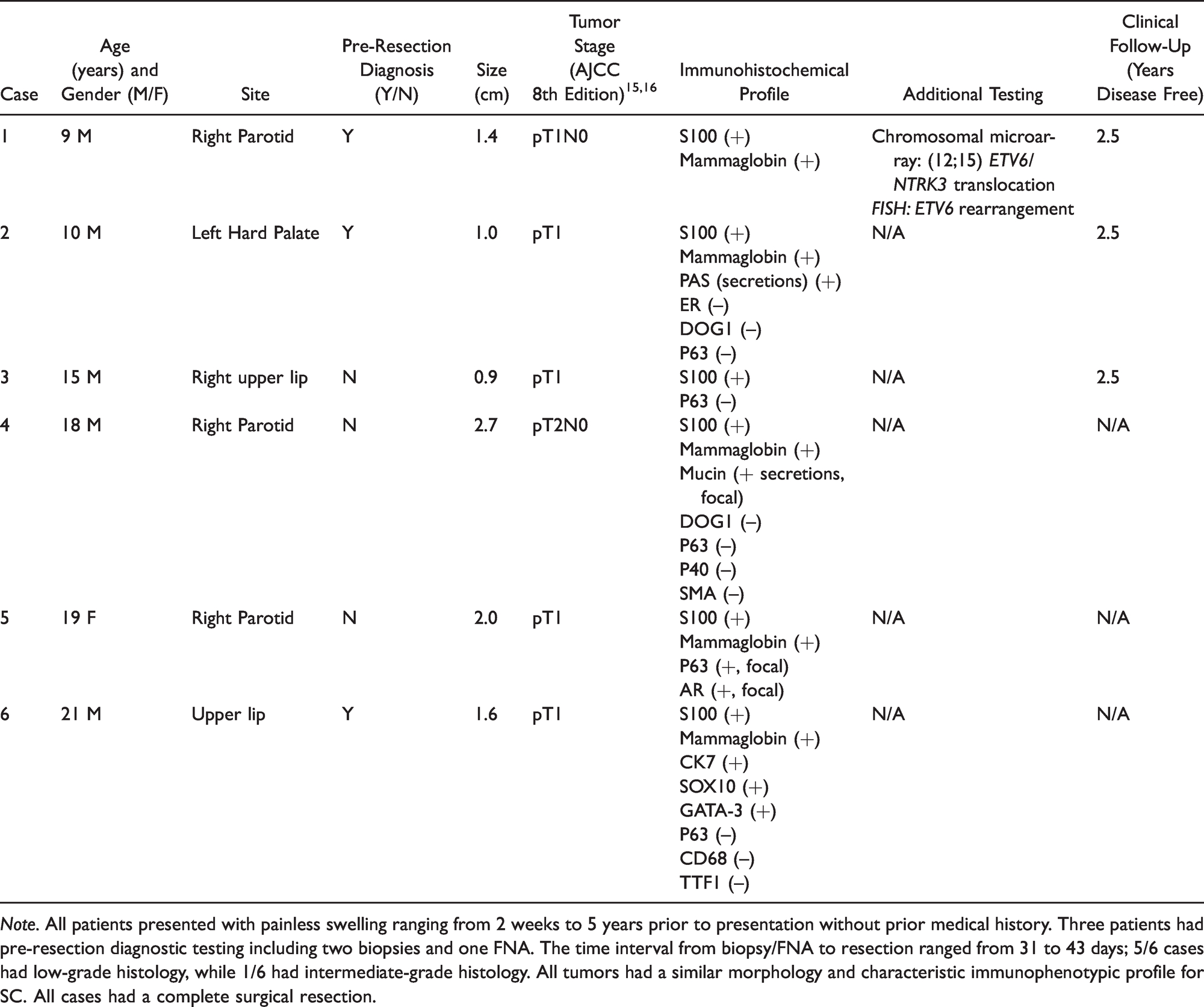
Note. All patients presented with painless swelling ranging from 2 weeks to 5 years prior to presentation without prior medical history. Three patients had pre-resection diagnostic testing including two biopsies and one FNA. The time interval from biopsy/FNA to resection ranged from 31 to 43 days; 5/6 cases had low-grade histology, while 1/6 had intermediate-grade histology. All tumors had a similar morphology and characteristic immunophenotypic profile for SC. All cases had a complete surgical resection.
Case 1
A 9-year-old male presented with a cheek lesion first noticed 2 weeks prior to evaluation. Radiographically, there was a nodular heterogeneously enhancing mass involving the anterior aspect of the right parotid gland. FNA showed low-grade carcinoma with features consistent with SC, including uniform cells arranged in solid sheets. The cells were epithelioid, cytologically bland, with occasional prominent nucleoli. The cytoplasm was eosinophilic with a subset of cells containing vacuoles (Figure 1). 43 days after FNA, the patient underwent superficial parotidectomy; a 1.4 cm SC tumor, was completely excised with negative margins. Histologically the tumor was morphologically and immunophenotypically consistent with the previous descriptions of SC, demonstrating tubular structures with eosinophilic luminal secretions and epithelial cells with eosinophilic cytoplasm. High power shows eosinophilic and vacuolated cytoplasm, slight nuclear pleomorphism and prominent nucleoli. The carcinoma is positive for mammaglobin and S100 immunostains, while it is negative for DOG-1 and P63 (Figure 2). Two lymph nodes were negative for carcinoma. Break-apart fluorescence in-situ hybridization (FISH) showed an ETV6 gene rearrangement, and chromosomal microarray showed a t(12;15)(p13;q25) ETV6/NTRK3 fusion. In 2.5 years of follow-up, there have been no recurrences or metastases.

Fine needle aspiration of secretory carcinoma. FNA shows sheets of monomorphic epitheloid neoplastic cells in both the DiffQuick (A [10×]) and PAP-stained (B [40×]) slides. Note the abundant eosinophilic cytoplasm and occasional vacuolization with small nucleoli (B). The cell block (C H&E [20×] shows clusters of neoplastic cells forming tubular structures with some eosinophilic secretions. Mammaglobin immunostain performed on the cell block (D [20×]) is diffusely positive in the neoplastic cells.

Morphologic and immunophenotypic features of secretory carcinoma. H&E(A [10×]) demonstrates tubular structures with eosinophilic luminal secretions and epithelial cells with eosinophilic cytoplasm. Medium power (B, H&E [20×]) shows some hobnailed appearance of the neoplastic cells. High power (C, H&E [40×]) shows eosinophilic and vacuolated cytoplasm, slight nuclear pleomorphism and prominent nucleoli. The carcinoma is positive for mammaglobin (D [20×]) and S100 (E [20×]) immunostains, while it is negative for DOG1 (F [20×]) and P63 (not included).
Case 2
An 11-year-old male presented with a hard palate lesion that had been present for 5 years. The posterior aspect of the left side of the hard palate showed bony erosion and mild thickening radiographically. A biopsy was positive for a low-grade salivary gland epithelial lesion. Two months after the biopsy, he underwent surgical resection and was diagnosed with SC at an outside institution. Tumor extended to all surgical margins. He subsequently underwent complete re-resection at our institution with negative margins. Histologically the tumor was composed of neoplastic cells with eosinophilic cytoplasm forming microtubular structures. The tumor was well circumscribed, but unencapsulated (Figure 3(A)). The tumor was positive (diffuse and strong) for mammaglobin and S100, while it was negative for ER, DOG-1 and P63. The secretions were positive for PAS without granular staining. In 2.5 years of follow-up there have been no recurrences or metastases.

Additional histologic features of secretory carcinoma. Low power shows lobules of tumor cells with eosinophilic cytoplasm forming microcystic structures (A H&E [10×]) that are well circumscribed by nonencapsulated. The tumor lobules are separated by thick fibrous septae. A common histologic finding includes eosinophilic secretions within the microtubular spaces (B H&E [20×]). One case of SC presented with a primarily cystic structure, with the epithelial lining composed of neoplastic cells (C H&E [20×]). Lowgrade neoplastic cells with tubular growth pattern and hobnail cells with microvesciular cytoplasm and some glands with pink eosinophilic secretions (D H&E [20×]).
Case 3
A 15-year-old male was incidentally noted to have right sided buccal swelling, which per patient was present for 6 months. MRI showed a gingival buccal sulcus lesion. No pre-resection diagnostic material was obtained. A 0.9 cm SC was completely excised. Microscopically the tumor was composed of nodules of low-grade cells with eosinophilic cytoplasm forming microtubules with intraluminal eosinophilic secretions (Figure 3(B)). The tumor cells were positive for S100 and negative for p63. In 2.5 years of follow-up there have been no recurrences or metastases.
Case 4
An 18-year-old male was found to have a 2.7 cm cystic parotid mass. This case was sent in for consultation. No other clinical information is known. Histologically a large mainly cystic mass, 2.7 cm, with epithelial lining showing foci of epithelial proliferation. Occasional epithelial projection within the cystic space and somewhat lobulated pattern is noted at the periphery is noted. The neoplastic cells have bland nuclei with vesicular chromatin and small nucleoli (Figure 3(C)). The tumor cells were diffusely positive for S100 and Mammaglobin. P40, smooth muscle myosin heavy chain, DOG-1 and P63 were negative. Focal mucin positive secretions were also noted. The tumor was completely excised. No follow up information is known.
Case 5
A 19-year-old female presented with a 2.0 cm parotid mass. This case was sent in for consultation. No other clinical information is known. The tumor was composed of low-grade cells forming cords, glands, and tubules of cells with variable amounts of eosinophilic-to-foamy cytoplasm. Scattered cells have large mucin vacuoles resembling mucinous cells. Several glands contain pink colloid-like material (Figure 3(D)). The neoplastic cells were positive for S100 and mammaglobin (focally). P63 and androgen receptor were also focally positive. The tumor was completely excised. No follow-up information is known.
Case 6
A 21-year-old male presented with a 1.6 cm lip lesion, and biopsy was positive for SC. 34 days after the biopsy, he underwent resection with negative surgical margins. Both the specimens were sent in for consultation and no additional clinical information is known. The biopsy and resection specimen showed similar morphologic features including intermediate-grade neoplastic cells with abundant vacuolated cytoplasm arranged in nests, cords and tubules. Within the tubules prominent eosinophilic secretions were noted. Occasional mitoses were seen. The tumor cells were diffusely positive for CK7, S100, SOX-10, Gata-3 with multifocal expression of Mammaglobin. The neoplastic cells were negative for p63, CD68 and TTF1. The tumor was completely excised. No perineural or angiolymphatic invasion was seen. No follow-up information is known.
Discussion
SC is a relatively newly-described variant of salivary gland carcinoma. While rare, this entity can be seen in the pediatric and adolescent populations. Most cases occur in children with no significant past medical history, as in our 6 cases. However, cases of secondary malignancy following radiation have been reported. 5 While the previous literature reports a slight male predominance in the pediatric population, 4 our case series has a male to female ratio of 5:1, which is likely explained by the rarity of SC in children and adolescents and small case numbers. Tumor sites included parotid gland (3) and minor salivary glands (1 hard palate and 2 upper lip). Where clinical history was known, lesions were present ranging from 2 weeks-5 years prior to evaluation. In 3 cases, pre-resection diagnostic material was available (2 biopsies and 1 FNA). All showed lesional tissue and diagnoses included a low-grade salivary gland carcinoma, low-grade salivary gland epithelial lesion, and SC. Tumor size upon resection ranged from 0.9 cm–2.7 cm and only one case had a stage 2 tumor.
Histologically all cases had classic features of SC, with relatively circumscribed, but non-encapsulated, masses divided by fibrous septa. Macrocystic, microcystic, solid, and papillary patterns were observed. Eosinophilic and mucinous secretions were present. The majority of cases (5/6) had low-grade nuclear features, while one demonstrated intermediate-grade nuclei. The immunohistochemical profile of these cases were consistent with SC.
Complete surgical resection with negative margins is the preferred treatment to date.14,15 Patients typically have a good prognosis with rare reports of recurrence in children. 7 All tumors in our series were resected with negative margins. Although the literature reports a subset of cases with lymphovascular and perineural invasion, 8 , 9 neither of these features were present in our samples. No lymph node metastases were seen in any of the cases where lymph nodes were evaluated. The three children with available follow-up information had no post-surgical complications and had no recurrences in two and a half years.
In the case where cytogenetic analysis was performed, an ETV6 rearrangement was present by FISH and microarray evaluation demonstrated the characteristic ETV6-NTRK3 t(12;15)(p13:q25). While ETV6-NTRK3 is the most common genetic alteration seen in SC, other gene partners have been recently described, including RET, MAML3, and MET. 13 ,16–19 The ETV6 gene partner can be important, not only for diagnosis, but also potentially as treatment targets. Recently developed NTRK inhibitors have been used in cases of locally advanced or metastatic disease. 12 None of our patients received NTRK inhibitor treatment.
Given SC is a rare salivary gland tumor in the children and adolescent population, it is important for pathologists to be aware of this entity. The differential diagnosis for SC includes other salivary gland neoplasms, including acinic cell carcinoma (ACC), mucoepidermoid carcinoma (MEC), cystadenocarinoma, and low-grade salivary duct carcinoma. 8 , 13 Some entities, like MEC, can be easily distinguished from SC on H&E sections. However, zymogen-poor acinic cell carcinoma can be challenging to differentiate from SC on H&E alone. Immunostains and molecular testing are important in determining the correct diagnosis.
In summary, our small case series emphasizes the important recognition of SC diagnostic category in salivary gland neoplasms in the pediatric population. It further supports the impression that SC is a low-grade malignancy and complete surgical resection was the treatment of choice. The vast majority of patients have an excellent prognosis and disease-free survival. Nonetheless, proper diagnosis of this neoplastic entity in pediatric patients is essential, especially for small biopsies and FNA while other than surgical treatment modalities can be explored.
Footnotes
Author Contributions
All authors contributed to the data collection, analysis and writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This project was conducted with institutional review board approval