
Abstract
Digital imaging, including the use of artificial intelligence, has been increasingly applied to investigate the placenta and its related pathology. However, there has been no comprehensive review of this body of work to date. The aim of this study was to therefore review the literature regarding digital pathology of the placenta. A systematic literature search was conducted in several electronic databases. Studies involving the application of digital imaging and artificial intelligence techniques to human placental samples were retrieved and analyzed. Relevant articles were categorized by digital image technique and their relevance to studying normal and diseased placenta. Of 2008 retrieved articles, 279 were included. Digital imaging research related to the placenta was often coupled with immunohistochemistry, confocal microscopy, 3D reconstruction, and/or deep learning algorithms. By significantly increasing pathologists’ ability to recognize potentially prognostic relevant features and by lessening inter-observer variability, published data overall indicate that the application of digital pathology to placental and perinatal diseases, along with clinical and radiology correlation, has great potential to improve fetal and maternal health care including the selection of targeted therapy in high-risk pregnancy.
Introduction
The human placenta is a vital organ that allows for mutual exchange of nutrients, gasses, and waste products between the maternal and fetal circulation during pregnancy. 1 Placental abnormalities involving its structure and/or function may expose both the mother and fetus to acute and sometimes life-threatening health risks and long-term sequelae. 2 Gross and often microscopic examination of the placenta, correlated with clinical information, plays a key role not only in identifying pathological factors responsible for an acute poor pregnancy outcome but also in revealing which women are more likely to experience recurrent adverse events in future pregnancies and which babies may face long term developmental or metabolic diseases. 3 However, in hospitals with a huge number of deliveries many placentas tend to be discarded without being sent for microscopic evaluation, sometimes leading to misrecognition of pathological processes underlying high risk pregnancies.4,5 Additionally, since many residency training programs lack formal placental and perinatal pathology subspecialties, general pathologists graduating from these programs may not be proficient in this field. This ultimately leads to poor qualitative and quantitative reproducibility as well as standardization of placental pathological examination and reporting.6,7
Digital pathology has provided pathologists with new tools for making diagnoses, education, and performing research.8,9 For instance, whole slide imaging (WSI) has been approved by several regulatory bodies for rendering a primary diagnosis without having to examine glass slides using a light microscope, and is slowly being adopted in clinical practice in many countries.10,11 The development of global teleconsultation networks has also enabled pathologists to more easily share challenging cases with distant colleagues for second opinions.12-14 More recently, artificial intelligence (AI) has been successfully applied to whole slide images to help screen and triage cases, offer computer-aided diagnoses, and provide prognostic information directly from images of hematoxylin and eosin (H&E) stained tissue. The utility of WSI technology for clinical and non-clinical applications has been widely published for various surgical pathology and cytopathology specimens.15-23 Recently, digital pathology has also been leveraged to examine the placenta. However, a comprehensive review of this topic has to date not yet been performed.
The aim of this study was to thus systematically review the published literature regarding the application of digital imaging techniques involving the human placenta and to objectively evaluate how these innovative imaging techniques have augmented the field of placental and perinatal pathology.
Materials and Methods
Literature Search and Article Screening
A systematic review without language restrictions was conducted according to standard methods and reporting in accordance with appropriate guidelines, Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 24 and Meta-Analysis of Observational Studies in Epidemiology (MOOSE). 25 The databases Pubmed and Embase were systematically searched until October 2022 to identify any study regarding the placenta and digital pathology. The search strategy comprised a combination of terms including “placenta,” “automated digital image analysis,” “deep learning,” “machine learning,” “quantitative immunohistochemistry,” and “artificial intelligence” and their spelling variations. The complete search strategy of these databases is shown in Supplemental Table S1.
Three authors (SM, IG, and AE) independently reviewed all article titles and abstracts with the aid of Rayyan QCRI reference manager web application. 26 Inclusion criteria encompassed the application of any kind of digital pathology technique to study the human placenta. Abstracts with adequate study details were included. Full texts of the articles fulfilling the initial screening criteria were acquired and reviewed. Any disagreement with respect to inclusion of a particular article was resolved by consensus.
Data Extraction
Two investigators (SM, IG) independently extracted data from the included studies with a standardized form. Data extracted included: author(s) and publication year, country of origin for the research, type of paper (full article or abstract), total number of patients, type of digital pathology technique employed, study results, and limitations of the study.
Results
Literature Search Findings
A flow diagram of the screening and exclusion of all articles is shown in Figure 1. Of the 2008 publications retrieved after removal of duplicates, 1701 were excluded after title and abstract screening. The remaining 307 publications were identified as potentially relevant to the study. After full text assessment, 28 of these articles were excluded for the following reasons: 14 were only review articles, 12 papers represented duplication of data, and 2 studies lacked sufficient detailed information about the application of digital pathology specifically to the placenta. Thus, 279 final studies were included in this review. They included 185 full text articles and 94 abstracts.
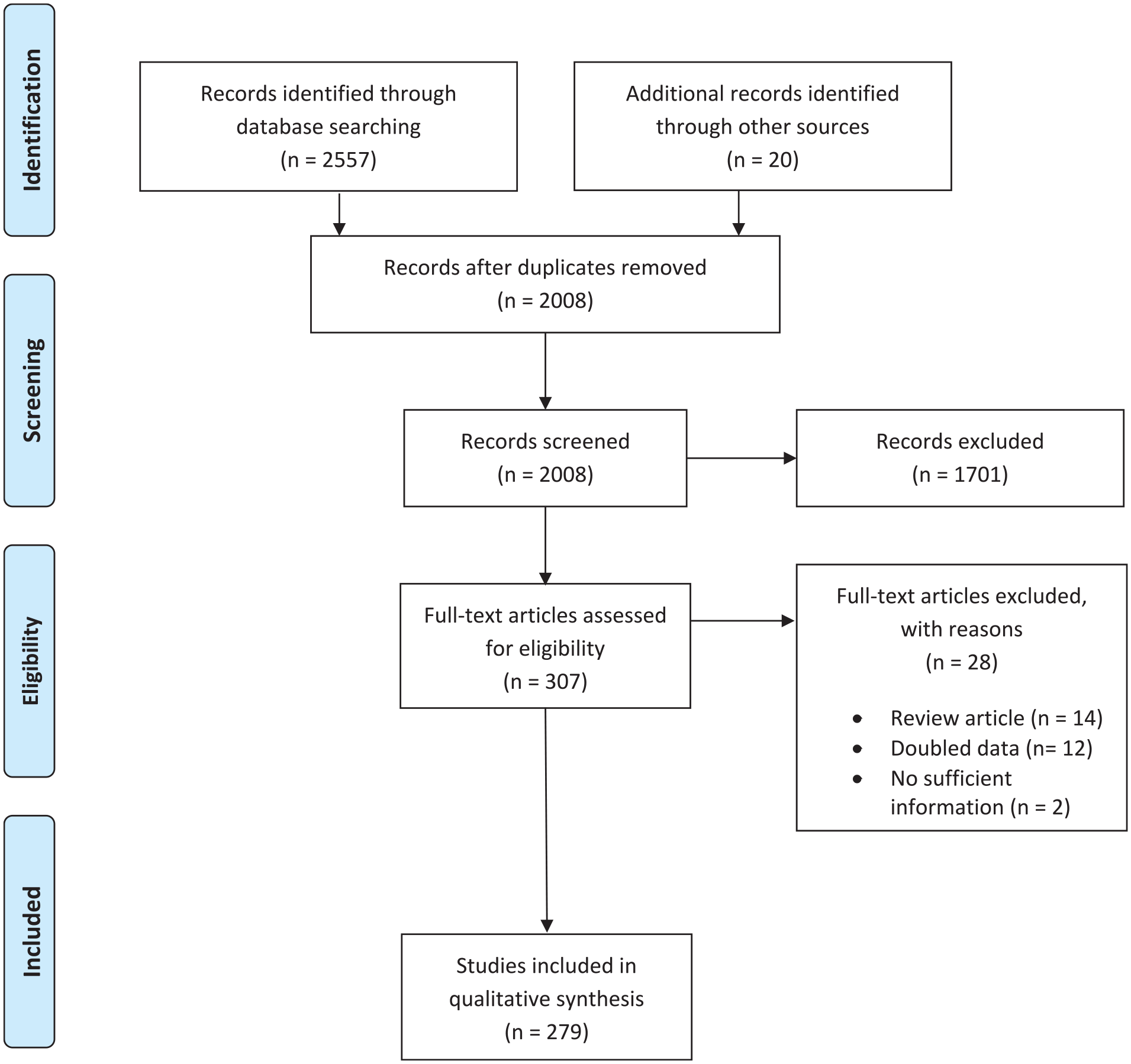
Search flow diagram.
The included studies were published over a time span (1978–2022) of 4 decades and were geographically distributed as follows: 148 (53%) from Europe, 54 (19%) from North America, 49 (17.5%) from Asia, 13 (4.5%) from Africa, 9 (3%) from Oceania, and 5 (2%) from South America. These studies involved a total of 12,080 patients, with the number of subjects per study ranging from 1 to 871.
Characteristics of Digital Imaging Techniques
An overview of the included studies is provided in Table 1. Given that some studies utilized more than 1 technique of AI, the retrieved studies were divided into 3 methods: (i) immunohistochemistry (IHC) coupled with AI (112 papers including 39 abstracts, involving 6687 total specimens), (ii) confocal microscopy (68 papers including 16 abstracts, involving 1438 patients), and (iii) 3D imaging analysis (124 studies encompassing 39 abstracts, involving 5692 placentas). There were 25 papers (16 with full text and 9 abstracts) concerning placenta alterations related to abortion and recurrent miscarriage, involving 1088 subjects (Supplemental Table S2). Gestational diabetes was discussed in 15 publications (Supplemental Table S3), while a total of 64 articles (Supplemental Table S4) focused on the use of digital pathology in the context of preeclampsia and gestational hypertension, and intrauterine growth restriction (IUGR) was the main topic in 28 articles (Supplemental Table S5). The remaining studies addressed miscellaneous entities (Supplemental Table S6) including molar pregnancy/trophoblastic disease, preterm or prolonged pregnancy, infections or inflammatory conditions occurring during pregnancy, smoking-related damage to the placenta and fetus, anemia or obesity in pregnancy, ectopic pregnancy, twin-to-twin transfusion syndrome, and placenta increta among. Digital imaging and AI were also applied to study normal anatomy and physiology of the human placenta (Supplemental Table S7).
Overview of the Included Studies.
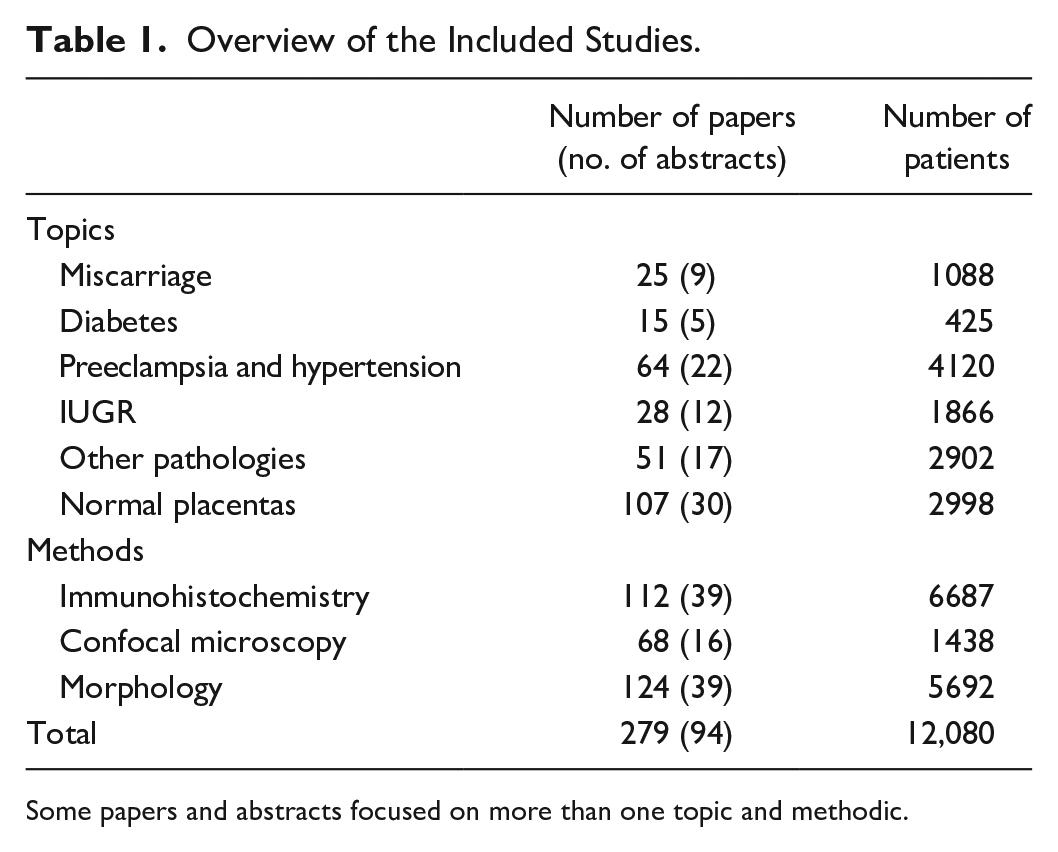
Some papers and abstracts focused on more than one topic and methodic.
Discussion
The application of digital imaging tools has improved the interpretation of the placenta. Computer-guided techniques have been employed to quantify the immunohistochemical expression of tissue markers in placenta, develop machine learning algorithms for assisting pathologists rendering diagnoses, and 3D imaging reconstruction systems have been leveraged to study specific morphologic features of the human placenta.
Immunohistochemistry Quantification
Quantitative digital/computer-assisted immunoreactive scoring systems using image analysis methods have been tested in a wide range of placental and perinatal pathological processes. In 2003, Kontron Systems 300 software was used to characterize decidual trophoblast cell invasion by quantifying anti-MNF116 immunohistochemical staining in placental bed biopsies from normal and preeclampsia pregnancies. These Authors found restricted invasion of trophoblastic cells in preeclampsia, which may influence vascular remodeling required for delivering adequate volumes of maternal blood to the placenta. 27 With regard to preeclampsia, semi-quantitative digital image analysis has also been used in several studies to quantify and correlate levels of different proteins within placental cells with maternal serum levels: among them was syndecan-1 evaluated with MembraneQuant software, which was found to be increased in syncytiotrophoblast cells in both early and late preeclampsia, suggesting a potential association with maternal anti-angiogenic and pro-inflammatory states. 28 Moreover, in 2006 a semi-quantitative scoring scale was used to compare HLA-G and HLA-E immunohistochemical staining between cases of recurrent miscarriage and elective terminations, but no differences were observed in either spatial localization or quantification. 29 In 2011, investigators employed ImageJ to demonstrate that alterations in decidual macrophage distribution and phenotype may contribute to the pathogenesis of preeclampsia. 30 Furthermore, in 2018 image analysis using the Aperio ImageScope Positive Pixel Count algorithm to score angiogenic factors like VEGF, Flt-1, PlGF, and KDR was performed on placentas with preeclampsia, IUGR, and healthy controls. In doing so, these authors detected a significantly reduced expression of angiogenic factors in IUGR pregnancies compared with normal and preeclamptic ones, suggesting a putative explanation for the loss of vasculature and villous architecture in IUGR. 31 Speaking of preeclampsia, in 2020 morphometric image analysis of histone 2A (H2A) immunohistochemical expression was employed for studying the specific distribution of mature (H2A+) and differentiating (H2A−) chorionic syncytiotrophoblasts in preeclamptic and normotensive patients, with a special focus on their HIV status. The Authors found not only a lower expression of H2A in the preeclampsia group compared to the normotensive group, but they also showed reduced staining of such a molecule in the villi of HIV+ compared to HIV- placentas. 32 These findings led the investigators to speculate on a putative protective role of H2A expression against the process of HIV-1 vertical transmission.
Regarding IUGR, other researchers when using a dual-labeling strategy combined with Image Pro software, reported increased IGFBP-1 phosphorylation in decidualized mesenchymal cells in placentas associated with IUGR compared to appropriate for gestational age controls, suggesting that specific phosphorylated sites on IGFBP-1 may be important for regulating cellular growth and development, as well as limiting trophoblast invasion and migration. 33 In the last decade, quantitative immunohistochemical analysis has also been applied to placenta increta cases, where a combination of high-resolution virtual imaging, IHC, and computer-assisted image analysis revealed larger vessel dimensions with greater heterogeneous distribution than controls, partially explaining the severe hemorrhages observed during placenta-increta deliverie. 34 Finally, using Image Pro Plus software investigators were able to analyze the number of syncytial knots per villous area, Ki67 proliferation index, villous vascularity (CD31), and number of leukocytes (CD45) in placentas associated with stillbirths. They applied this morphometry signature based analysis to stillborn cases of unknown cause and thereby reduced the number of unexplained stillbirths. 35 Of note, similar image analysis methods had been previously used by the same group to characterize placenta morphology after maternal perception of reduced fetal movement, 36 and to assess placental storage conditions. 37
Machine and Deep Learning Algorithms
Automatic analysis of histopathology images involves image classification and image segmentation. To date, several studies have reported the development of deep learning algorithms applied to placental histopathology, especially for characterizing villous morphology and detecting vascular pathology. The first report on this topic dates back to 2005 when computerized morphometric analysis with a light microscope and WinScanArray 3 software was used to isolate blood vessel lumens. This technique was performed to examine differences in villous vascular volume between normal placentas and those from pregnancies complicated by preeclampsia or pre-gestational diabetes. Significant quantitative changes were found in the villous vascular tree in pre-gestational diabetes, that were not detectable by conventional light microscopy, suggesting that morphometric analysis of the capillary tree may have diagnostic importance in this entity. 38 More recently, KS300 Kontron-Zeiss software was employed for comparing placental vascular morphology at term between women with normal and an altered Doppler exam during pregnancy. This study showed a greater number and width of stem, intermediary, and terminal villi vessels in the placentas of patients with Doppler exam alterations, even without clinically relevant placental pathologies. 39 Additionally, automated image analysis systems have been developed for the evaluation of villous morphology in recurrent miscarriage, 40 delayed or accelerated villous maturation, 41 and distal villous hypoplasia (DVH), achieving respectable and reproducible results. In 2016, fractal dimension (a mathematical calculation of image complexity) was compared to the inter-observer agreement among 5 pathologists regarding DVH, a hallmark of IUGR, demonstrating that artificial intelligence has the potential to increase objectivity in reporting a clinically useful lesion. 42 Deep learning has also been applied to the identification of decidual vasculopathy (DV), a placental lesion characterized by hypertrophy of decidual arterioles often found in cases of preeclampsia or in otherwise healthy patients with a higher risk of developing such disease in subsequent pregnancies. Researchers have developed a hierarchical machine learning approach for the detection and classification of DV lesions in WSI placenta slides. 43 Their proposed method would allow many more placentas to be automatically screened by fewer pathologists, thereby potentially increasing the detection of mothers who are at risk for preeclampsia in subsequent pregnancies with direct therapeutic application. Today, women at high risk of recurrent preeclampsia are given regular doses of aspirin during the first trimester in order to prevent this disease. 43 Interestingly, recently a deep learning model (GestAltNet) has been applied to estimate the gestational age of scanned placenta slides. A mean absolute error of about 1 week was achieved, comparable to human pathologists’ evaluation, suggesting a potential application of this method to study abnormalities of villous maturation, like those occurring in preeclampsia and gestational diabetes. 44
3D Imaging
The two major methodologies of 3D imaging used to interrogate the human placenta are stereology and serial section reconstruction. These methods can be used in combination.
Stereology mainly deals with applying random sampling schemes to specimens and creating image slices that are measured by reproducible geometrical features (area, test points, volumes, and lines) for calculating volumes, surfaces, and lengths. 45 Stereology, although time-consuming, has been broadly used to study normal and abnormal human placentas. The strengths of this technology include unbiased sampling, simplicity, relatively cheap cost, and its potential application to multiple examination levels from macro- to microscopic levels. While this 3D imaging tool was initially used to explore placenta physiology, such as diffusing capacity for oxygen, 46 more recently it has been exploited for studying a wide range of pathological conditions such as preeclampsia, diabetes, 47 smoking-related damages, 48 placenta previa, 49 systemic lupus erythematosus, 50 and infections, 51 among other entities. Preeclampsia is the field that witnessed the widest application of stereological approaches, where villi architecture has been variously compared with IUGR pregnancies. For example, in this setting clinical measurements and umbilical cord physical parameters lead to interesting results, among which were: (i) observation of different villous content, weights, and volumes in pregnancies with idiopathic IUGR and in cases with both IUGR and preeclampsia, with different patterns in early and late onset scenarios, suggesting that idiopathic IUGR and IUGR in preeclampsia have a separate etiology 52 and that early- and late-onset preeclampsia should be treated differently 53 ; (ii) association of first-trimester serum pregnancy associated plasma protein-A (PAPP-A) levels with abnormal placental morphometry at delivery in pregnancies with preeclampsia and IUGR, which might explain the link between adverse pregnancy outcomes and first-trimester PAPP-A levels 54 ; (iii) finding a significant increase in placental volumetric parameters (volume of total villi, volume of intervillous vessels, etc.) in preeclampsia patients compared to other groups. 55 Finally, the literature contains reports of attempts to combine stereology with digital analysis of IHC staining in physiological and pathological settings. For example, in 2009 a novel double immuno-labeling protocol was developed to selectively identify proliferating villous cytotrophoblast cells using thick paraffin sections suitable for stereological quantification. 56 In addition, results from a 2015 study demonstrated that when IHC and stereology were combined structural differences between mild and severe pre-eclampsia were noted and hypothesized to be attributed to growth factors like VEGF and PIGF. 57
The other main strategy for generating three-dimensional reconstructions of the human placenta is serial sectioning either from physical slices or optical sectioning. 45 As for the former, in 2016 a software-based “sequential slice-to-slice” technique was successfully used to reconstruct villous microanatomy and, comparing placentas from healthy controls with those from pregnancies complicated by pre-eclampsia, growth restriction, and gestational diabetes, marked differences across normal and pathological pregnancies in terms of size, distribution, and branching patterns of stem villi were found. 58 On the other hand, for years confocal microscopy has been the most employed method for 3D reconstruction from optical sectioning and successfully used to study trophoblast caspase-mediated apoptosis, 59 terminal villous diffusion capacity, 60 and capillary-bed spatial arrangement. 61 In 2008, a confocal microscopy-based study elegantly outlined asymmetric placental capillary bifurcations and suggested that microrheological phenomena, in particular the so-called “plasma skimming” effect, are likely present in the fetoplacental microcirculation and may have effects on local blood flow, contributing to the higher efficiency of hemoglobin oxygenation in the placenta. 62 However, confocal microscopy examination carries several intrinsic limitations, the most challenging probably represented by an imaging depth resolution of only 100 µm due to scattering of light by refractive index mismatches of tissue components. Recently, different methods have been proposed for overcoming this drawback, including a method based on a combination of immunolabeling, rapid tissue clarification, and laser scanning confocal microscopy, allowing analysis of complex villous structures and capillary networks at the order of 1 mm3 in a few hours. 63 Future prospective methods include super-resolution microscopy and light sheet microscopy, which have been applied to different organs but not yet to the placenta.
Limitations
Several of the included articles have intrinsic limitations. Many articles lack properly matched control groups. Moreover, potential case selection or sampling biases might have influenced the results of some works.
Conclusion
This review demonstrates that as imaging technology advanced, numerous groups of investigators have successfully leveraged these tools to investigate the normal and abnormal human placenta. Digital analysis techniques and 3D imaging have been employed for researching a wide variety of perinatal diseases, including preeclampsia, gestational diabetes, IUGR, and miscarriage, among others. Preliminary work has verified that artificial intelligence algorithms applied to whole slide images of the placenta can be trained to detect specific lesions such as DV. This creates potential for automating and standardizing the microscopic examination of human placentas. Further innovation in this field is anticipated along with improvements in diagnosis, prognostication, and discovery of the human placenta.
Supplemental Material
sj-docx-1-pdp-10.1177_10935266221137953 – Supplemental material for Application of Digital Imaging and Artificial Intelligence to Pathology of the Placenta
Supplemental material, sj-docx-1-pdp-10.1177_10935266221137953 for Application of Digital Imaging and Artificial Intelligence to Pathology of the Placenta by Stefano Marletta, Liron Pantanowitz, Nicola Santonicco, Alessandro Caputo, Emma Bragantini, Matteo Brunelli, Ilaria Girolami and Albino Eccher in Pediatric and Developmental Pathology
Footnotes
Authors’ Note
The author Ilaria Girolami is now affiliated with Division of Pathology, Central Hospital Bolzano, Bolzano, Italy.
And the author Liron Pantanowitz now affiliated with Department of Pathology & Clinical Labs, University of Michigan, Ann Arbor, MI, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No ethical issues are raised by systematic reviews.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.