
Abstract
Background:
Colonic graft-versus-host disease (GVHD) is rare in children. The goal of this study was to evaluate the Lerner and the Farooq grade in pediatric patients.
Methods:
Retrospective multicenter study including all biopsies with a diagnosis of GVHD.
Results:
101 patients were included (median age: 8.9 years) with a male predominance (59%). 71% of patients had extracolonic GVHD. 98% and 54% of cases had apoptotic bodies and >6 apoptotic bodies, respectively. Crypt dropout was seen in 53% of cases and ulceration in 19%. Using the Lerner grade, 47% of cases were grade 1, 13% grade 2, 20% grade 3 and 20% grade 4; and using the Farooq grade, 35% were indeterminate for GVHD, 25% low, 27% intermediate and 14% high grade. There was moderate agreement (K = 0.47) between the system. 67% of the Lerner grade 1 cases were considered indeterminate for GVHD using the Farooq grade. No difference was seen with GVHD-related death and the grading systems. GVHD-related death was associated with extraintestinal involvement (P = .04), and with treatment response (P < .01).
Conclusions:
Although neither system was associated with GVHD-related death, given the more comprehensive approach, the authors suggest utilizing the Farooq grading system.
Keywords
Introduction
The cardinal histologic features of graft-versus-host disease (GVHD) include the presence of apoptotic bodies, crypt dropout, and ulceration.1-6 Pathologists play a vital role in the diagnosis of GVHD particularly in the exclusion of other conditions and current National Institute of Health (NIH) guideline advise the following categories based on the clinical and histologic findings: not GVHD, possible GVHD, and likely GVHD. 5 However, it still debatable what the minimum threshold for the diagnosis of GVHD is with the most common criterion used being the presence of 1–2 apoptotic bodies per biopsy fragment2,5,7 but a higher cutoff of 6 apoptotic bodies in 10 contiguous crypts have been proposed with a higher specificity, 3 and even a higher cutoff of 9 has been studied but had a suboptimal sensitivity. 1
Given the association of intestinal GVHD with non-relapse mortality,8-13 histologic grading systems have been developed with the most commonly used being the Lerner grade. 6 Although the Lerner grade is widely used it has several limitations including the lack of a definition for grade 1 cases, does not include the number of apoptotic bodies in its assessment, and, more importantly, does not correlate in current practices with clinical outcomes. In light of this, Farooq et al 1 developed a novel grading system which will be referred to in this manuscript as the Farooq grade. This system does provide clear and standardized instructions for the evaluation of the crypt apoptosis and crypt damage, hence, for the diagnosis of GVHD.
Unfortunately, most of the studies characterizing colonic GVHD are predominantly, if not entirely, composed of adult patients and pathologic characterization of colonic GVHD in cohorts composed exclusively of pediatric patients are lacking. Furthermore, the NIH consensus criteria was developed primarily from adult data and to the best of the authors’ knowledge has not been validated in pediatric patients. This is likely due to the rarity of hematopoietic stem cell transplant (HSCT) in this population accounting for less than 30% of all HSCT worldwide and due to the lower incidence of GVHD compared to adults patients. 14 Additionally, gastrointestinal involvement of GVHD is less common in pediatric patients compared to adult patients (40% vs 73%)14,15 with the most commonly involved organs by GVHD in pediatric patients being the skin, mouth, eyes, and lungs. 16 Worth noting, on the validation cohort of the Farooq grading system pediatric patients were included which was one of the main differences between the initial and validation cohort and potentially explaining the lack of the prognostic stratification on the validation cohort. 1
Given this, in current practice the pathologic assessment of colonic GVHD in the pediatric population is entirely based on extrapolation of the adults’ literature. Hence, the goal of this study was to provide a characterization of colonic GVHD in this patient population and to evaluate for the first time both the Lerner and the Farooq grading system in the pediatric population.
Materials and Methods
Prior to initiating the study, institutional review board (IRB) approval was obtained from Children’s Hospital of Philadelphia (IRB# 22-019872) and from Indiana University School of Medicine (IRB# 2022, 16082). In the remainder of the text, Children’s Hospital of Philadelphia will be referred as institution 1, and Indiana University School of Medicine as institution 2. A retrospective search was performed in both institutions for colonic biopsies for GVHD obtained from 2010 to 2021 from institution 1, and from 2005 to 2021 from institution 2. The electronic medical records at each center were queried for the clinical characteristics. All cases were included regardless of if the patients were treatment naïve or already receiving treatment for GVHD.
All biopsies were reviewed by a pediatric and gastrointestinal pathologist for the following histologic features: number of apoptotic bodies in 10 contiguous crypts (counted in the hotspot area), crypt dropout, and ulceration. Apoptotic bodies are commonly present in the regenerative component of the crypt and can show varying morphology from well-develop bodies characterize by clear vacuoles filled with nuclear dust and karyorrhectic debris, or as shrunken cells with a condense nuclei and an eosinophilic cytoplasm.2,5 Using the criteria of Farooq et al 1 crypt dropout when present was recorded as focal if present in 1 biopsy fragment, multifocal when in more than 1 fragment and as diffuse when seen in all the fragments. If more than 1 colonic biopsy specimen was received, the most abnormal biopsy part was used for the aggregate assessment.
A Lerner grade was assigned to all cases as previously defined: grade 1—crypt apoptosis without crypt dropout; grade 2—single crypt dropout; grade 3—contiguous crypt dropout; grade 4—diffuse crypt dropout with ulceration (Table 1).2,6 Additionally, all cases were graded according to the recently described histologic grading system proposed by Farooq et al, 1 referred in this text as the Farooq grade. This system evaluates for 2 main components: apoptotic bodies and crypt damage, with each component given a point according to the histologic features. For apoptotic bodies, if no apoptosis (0 points), 1–6 apoptotic bodies (1 point), and if >6 apoptotic bodies (2 points). This cut-off of 6 apoptotic bodies is an extrapolation of the criteria used for acute cellular rejection in intestinal allograft which has in prior studies has been used as a definitive feature of GVHD.3,7,17,18 In regard to the crypt damage, this is divided into no crypt dropout or ulceration (0 points), crypt dropout without ulceration (1 point), and ulceration (2 points). The aggregate points are added and according to the overall score cases are divided into indeterminate for GVHD (score 1), low grade (score 2), intermediate grade (score 3), and high grade (score 4) (Table 1). 1 Of note, the extend of crypt dropout (focal, multifocal, or diffuse) was not included in the original proposed Farooq grade as it did not significantly alter the performance of the grading system and simplified grading system was preferred by the authors. 1 A modified Lerner and modified Farooq grade was evaluated including the extend of crypt dropout (Supplemental Table 1).
Lerner and Farooq Grading Systems for Graft-versus-Host Disease (GVHD).
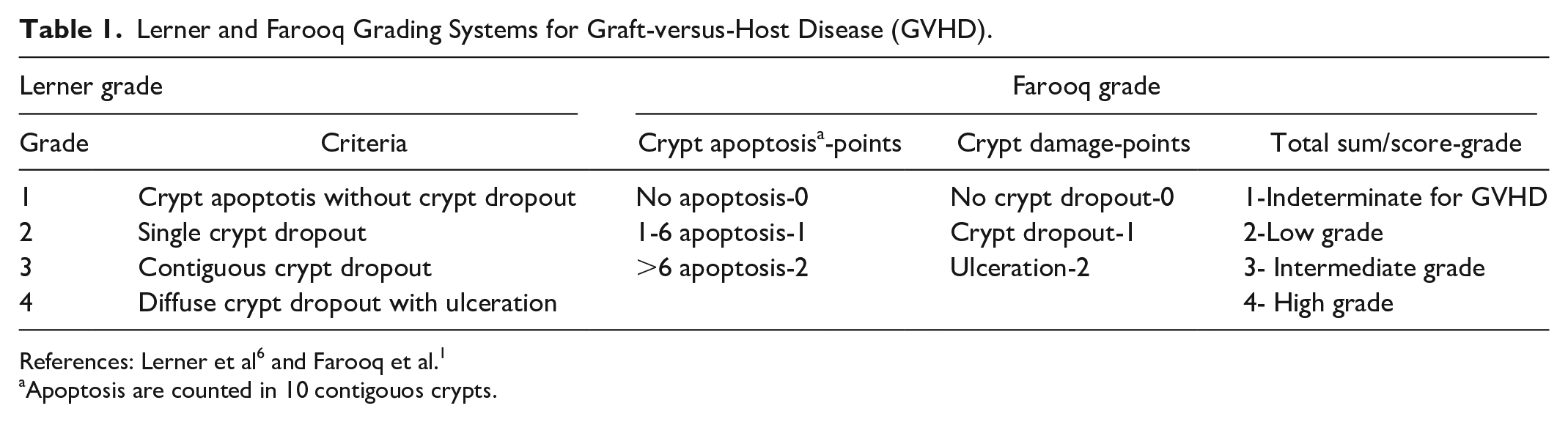
Apoptosis are counted in 10 contigouos crypts.
Statistical Analysis
Summary statistics were provided for the patient demographics, clinical characteristics, and histological findings for overall data and by institution. Comparisons between the institutions were provided using chi-square test for categorical variables and t-test for continuous variables. Summary statistics were also provided for patient characteristics by the Lerner system and the novel system, and comparisons were provided between the respective categories. Logistic regression was used to calculate the area under curve with GVHD related death as outcome for overall data and by institution. All analyses were done at a 5% significance level. SAS software 9.4 (Cary, NC) was used to perform all the analysis.
Results
A total of 101 colonic biopsies all from unique patients were included in the study, presenting with a median age of 8.9 years (IQR: 3.5–15.7) and predominantly in male patients (59.4%) (Table 2). The median time for HSCT to biopsy was 2 months (IQR: 1–6) with only 4 patients (4%) presenting within 21 days of transplantation. Most of the patients (76.3%) had a matched unrelated donor and the 2 most common sources for the stem cells were bone marrow (41.6%) and peripheral blood (39.6%). The indications for the SCT included acute lymphoblastic leukemia (28%), acute myeloid leukemia (19%), severe combined immunodeficiency (7%), sickle cell disease (5.0%), myelodysplastic syndrome (4.0%), juvenile myelomonocytic leukemia (4.0%), aplastic anemia (4.0%), chronic myeloid leukemia (3.0%), hemophagocytic lymphohistiocytosis (3.0%), non-Hodgkin lymphoma (2.0%), congenital bone marrow failure (2.0%), undifferentiated leukemia (2.0%), congenital neutropenia (2.0%), Diamond-Blackfan anemia (2.0%), acute erythroid leukemia (1.0%), adrenoleukodystrophy (1.0%), Ewing sarcoma (1.0%), chronic granulomatous disease (1.0%), congenital amegakaryocytic thrombocytopenia (1.0%), Hurler syndrome (1.0%), Evans syndrome (1.0%), and hyper-IgM syndrome (1.0%). For 1 patient the indication for SCT was not available.
Clinical Characteristics.
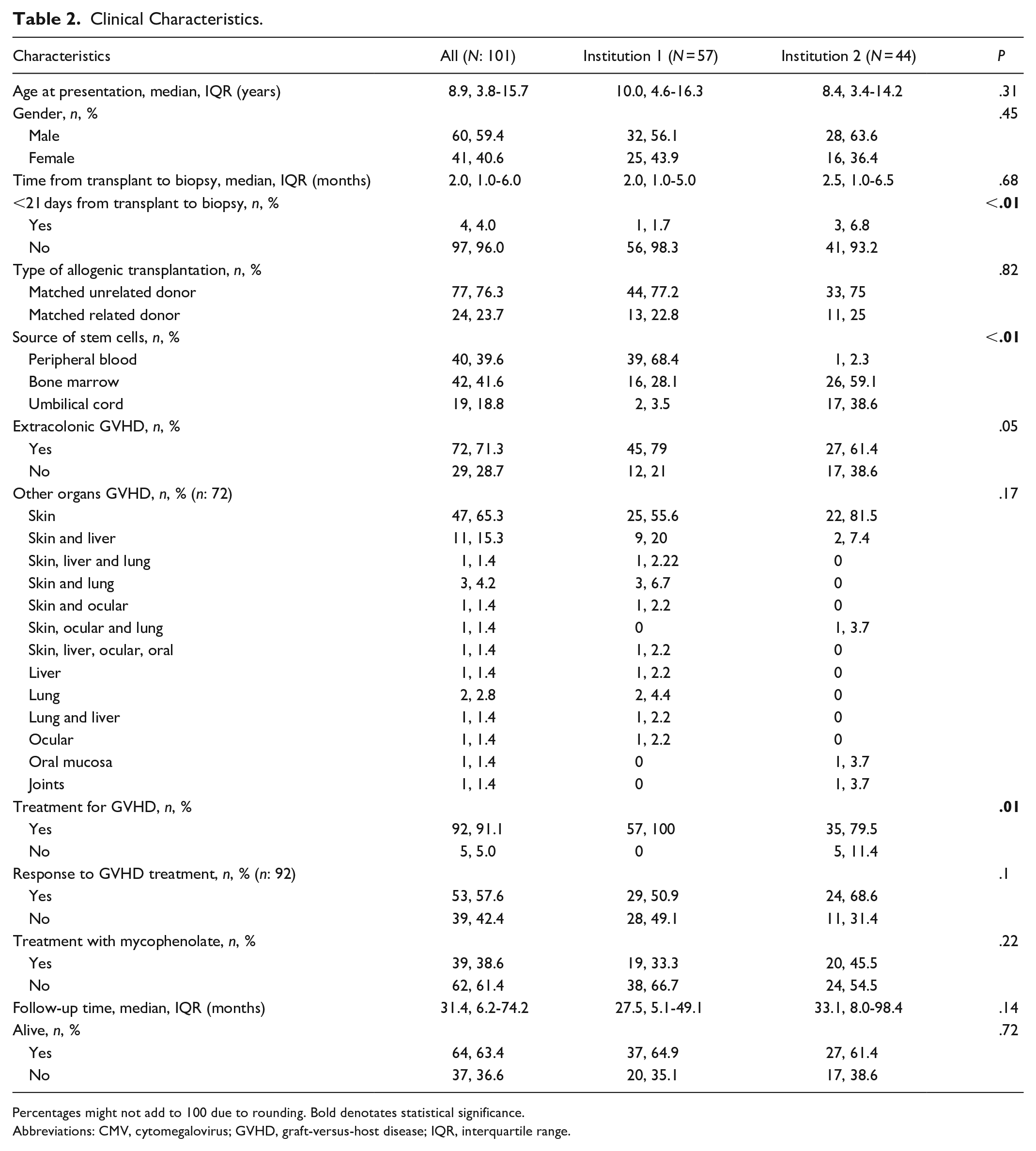
Percentages might not add to 100 due to rounding. Bold denotates statistical significance.
Abbreviations: CMV, cytomegalovirus; GVHD, graft-versus-host disease; IQR, interquartile range.
Apoptosis was found in almost all cases (98%) with a median number of 7 (range: 1–41) and of those, 53 cases (53.5%) had more than 6 apoptotic bodies in 10 contiguous crypts (Table 3, Figure 1). Crypt dropout was seen in half of the patients (52.5%) and was considered as focal in 18.8%, multifocal in 16.8%, and diffuse in 16.8%. Ulceration was seen in 18.8% of the cases. In 50 cases (49.5%) crypt dropout or ulceration were not seen, and in 32 cases (31.7%) there was crypt dropout but without ulceration. Of note, in 2 cases diffuse ulceration was seen and crypts were not available to assess for apoptosis or crypt damage. Using the Lerner grade, 47.5% of the cases were considered as grade 1, 12.9% as grade 2, 19.8% as grade 3, and 19.8% as grade 4. In contrast using the Farooq grade, 34.7% were indeterminate, 24.8% low grade, 26.7% intermediate grade, and 13.9% high grade.
Histologic Findings.
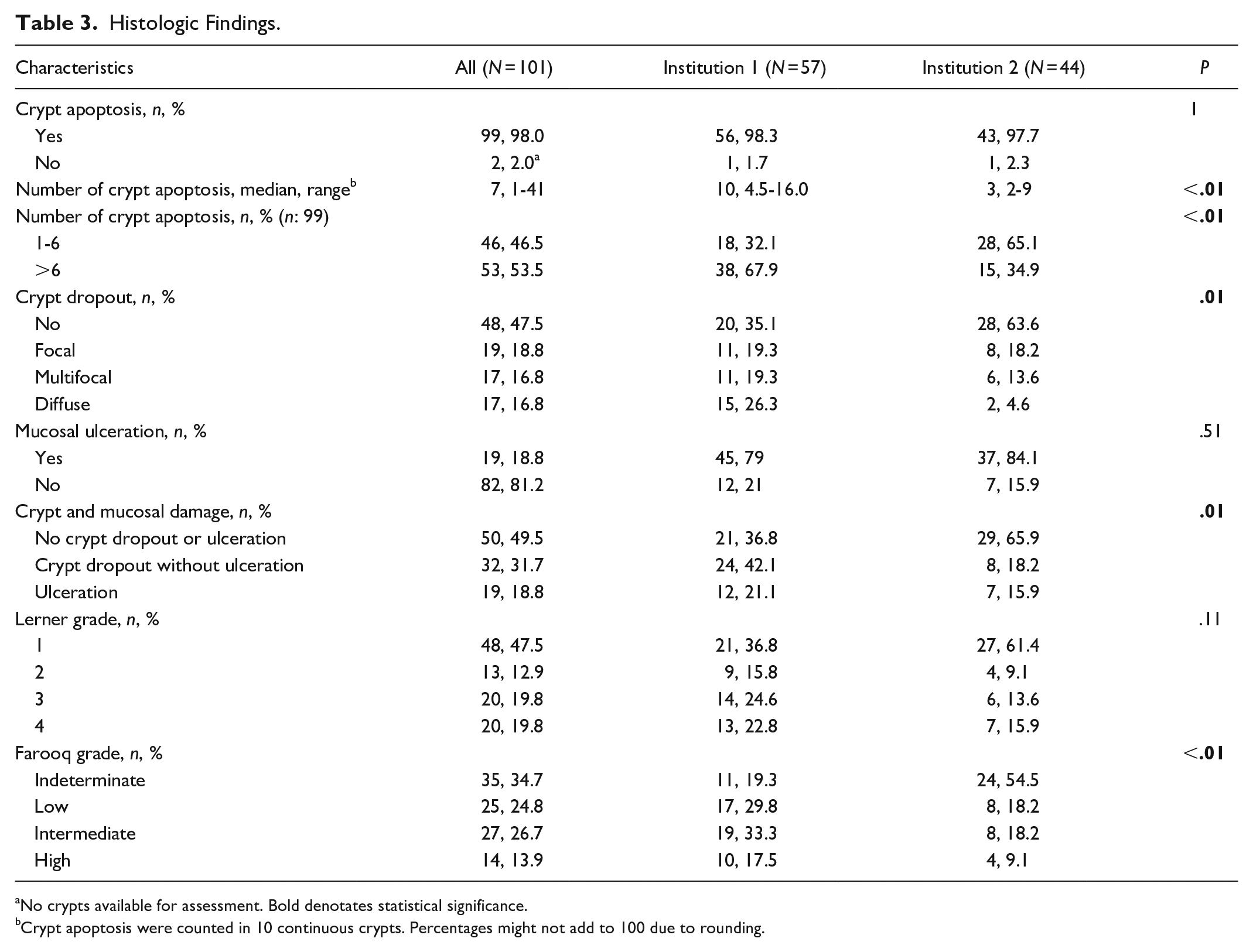
No crypts available for assessment. Bold denotates statistical significance.
Crypt apoptosis were counted in 10 continuous crypts. Percentages might not add to 100 due to rounding.
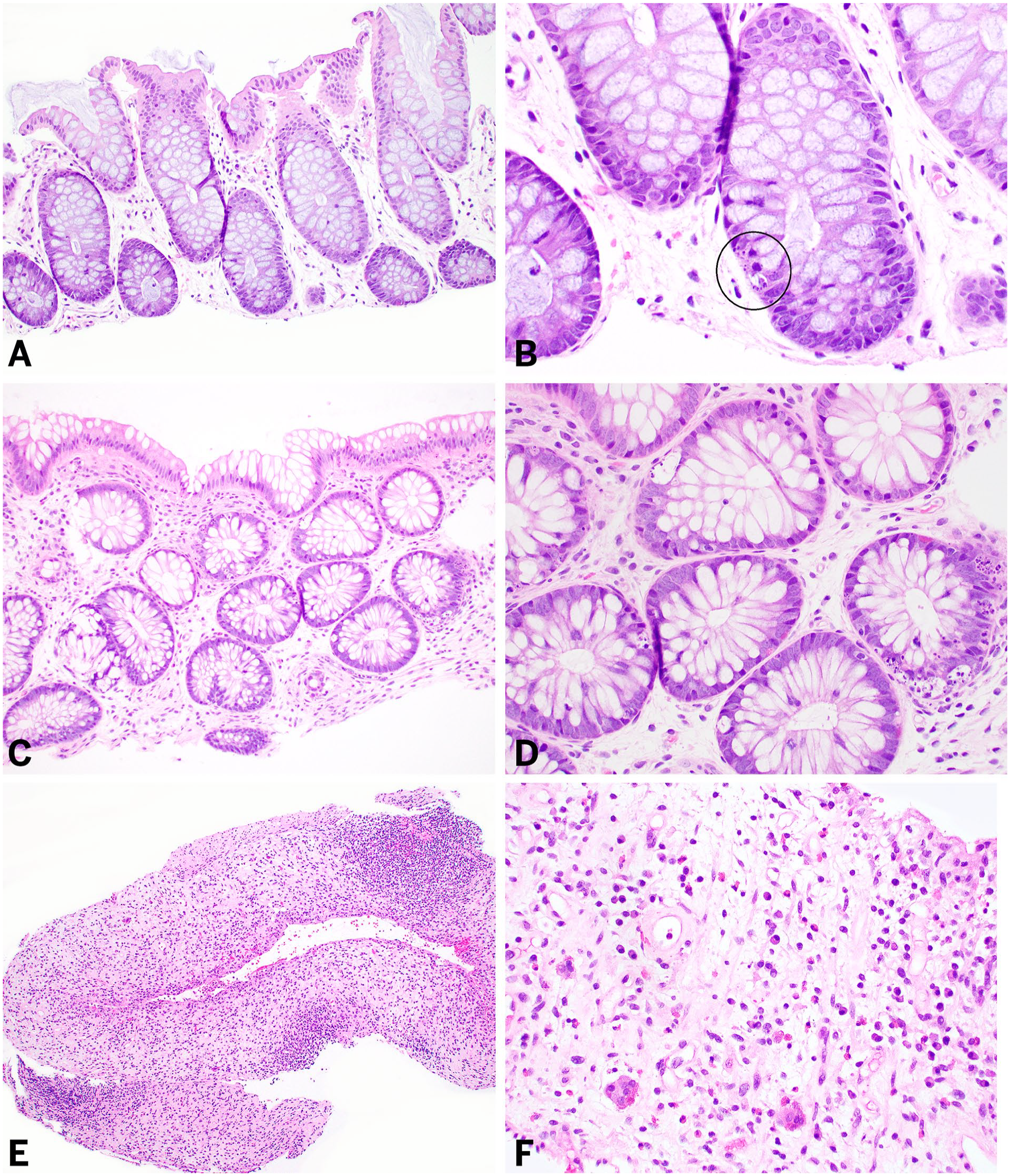
Selected cases of colonic GVHD. Case A-B and C-D show 2 cases with varying degrees of apoptotic bodies, but both considered as Lerner grade 1. When using the Farooq grade, case A-B is considered as indeterminate since there are only rare apoptotic bodies whereas the C-D case is considered as low-grade given the presence of more than 6 apoptotic bodies. Case E-F shows a completely ulcerated mucosa consistent with Lerner grade 4 but since crypts are unavailable for assessment of apoptotic bodies when using the Farooq grade is considered as low grade. All microphotographs are from hematoxylin and eosin-stained slides.
Most of the patients (71.3%) had evidence of extracolonic GVHD with the skin being the most common location (64.4%). Additionally, most patients received treatment for GVHD (91%) with just over half of them achieving treatment response (57.6%), and 39 patients (38.6%) received treatment with mycophenolate mofetil (MMF). Although 13 patients (12.9%) had positive cytomegalovirus (CMV) antibodies, none of the patients had an active CMV viremia.
Comparison of Clinicopathologic Characteristics Between Institutions
There was no difference in the age of presentation or gender assigned at birth between institutions (Table 2). Of the 4 cases presenting within 21 days of transplantation, 3 were from institution 2. No difference was seen in the type of allogenic transplantation between institutions, but the source of transplant was different with peripheral blood being the most common source in institution 1 (68%) compared to bone marrow in institution 2 (59%) (P < .01). No difference was seen in the presence of extracolonic GVHD nor the location of extracolonic GVHD. All patients received treatment for GVHD in institution 1 compared to 79.5% of patients from institution 2 (P = .01) but no difference was seen in response to treatment, use of MMF, and GVHD-related death.
Although no difference was seen in the presence of apoptotic bodies between institutions, a higher number of apoptotic bodies was seen in institution 1 (P < .01) (Table 3). Additionally, patients from institution 1 were more likely to have >6 apoptotic bodies compared to institution 2 (P < .01) and were more likely to have crypt dropout (P = .01). No difference was seen in the presence of ulceration across institutions. Although no difference was seen when using the Lerner grade across institutions, using the Farooq grade cases from institution 1 were more likely to be intermediate- and high-grade compared to institution 2 (P < .01).
Comparison of the Lerner Grade to Clinical Parameters
Table 4 summarizes the comparison of the Lerner grade with the different clinical parameters for the overall group and each institution. There was no difference between age at presentation, gender assigned at birth, time interval from transplant to presentation, or follow-up time and the Lerner grade. The Lerner grade was also not associated with evidence of extracolonic GVHD, treatment for GVHD, nor treatment response. Additionally, no difference was seen in GVHD-related death and the Lerner grade. A comparison of the modified Lerner grade and the clinical parameters is presented in the Supplemental Table 2.
Comparison of Lerner Grade With Clinical Variables.
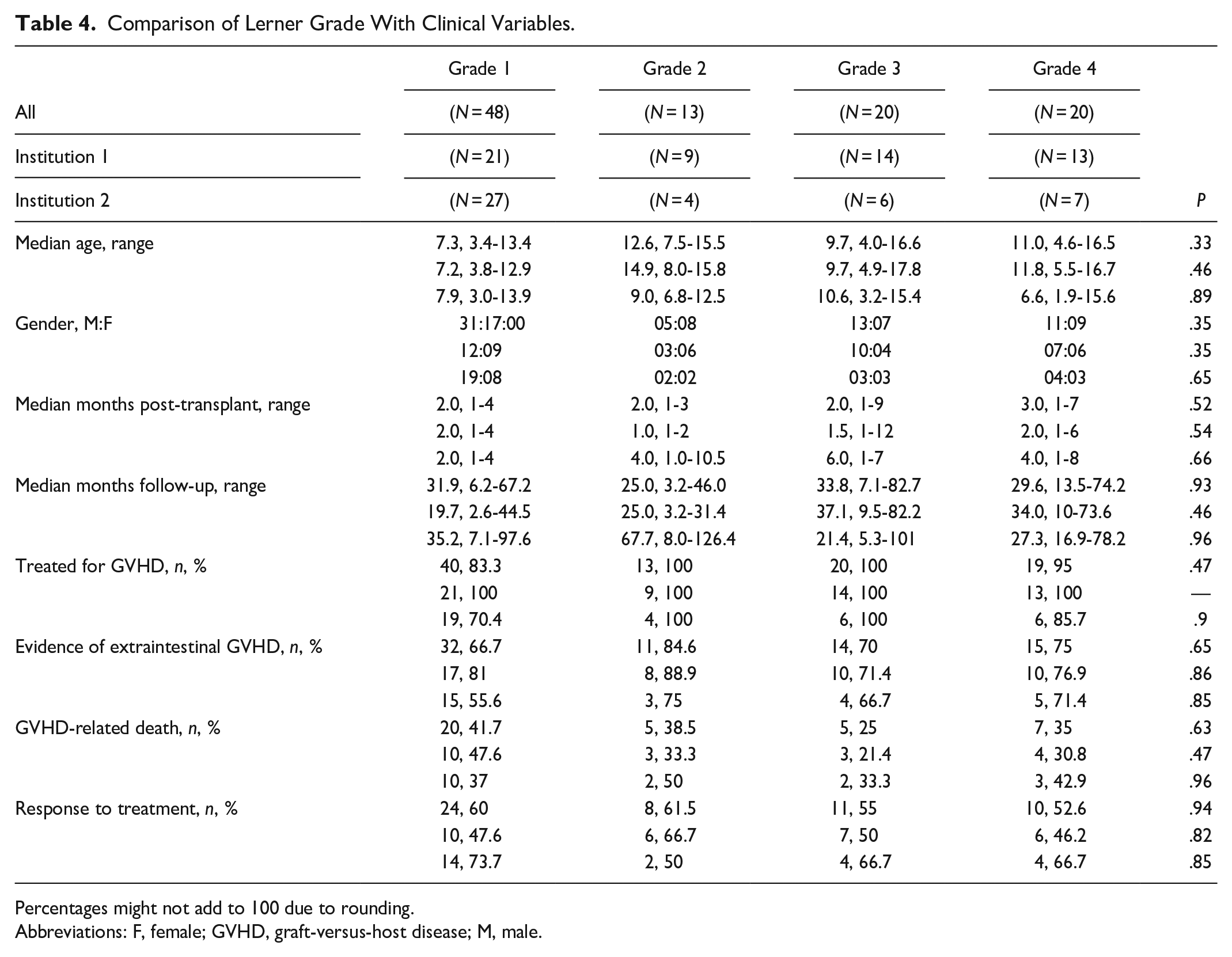
Percentages might not add to 100 due to rounding.
Abbreviations: F, female; GVHD, graft-versus-host disease; M, male.
Comparison of the Farooq Grade to Clinical Parameters
The Farooq grade was not associated with age at presentation, gender assigned at birth, time interval from transplant to presentation, or follow-up time (Table 5). No difference was seen between the Farooq grade and treatment for GVHD or treatment response. Although, the Farooq grade was not associated with extracolonic GVHD in the overall group, a difference was seen with cases from institution 2 (P = .03). No difference was seen in GVHD-related death and the Farooq grade. A comparison of the modified Farooq grade and the clinical parameters is presented in the Supplemental Table 3.
Comparison of the Farooq Grade With Clinical Variables.
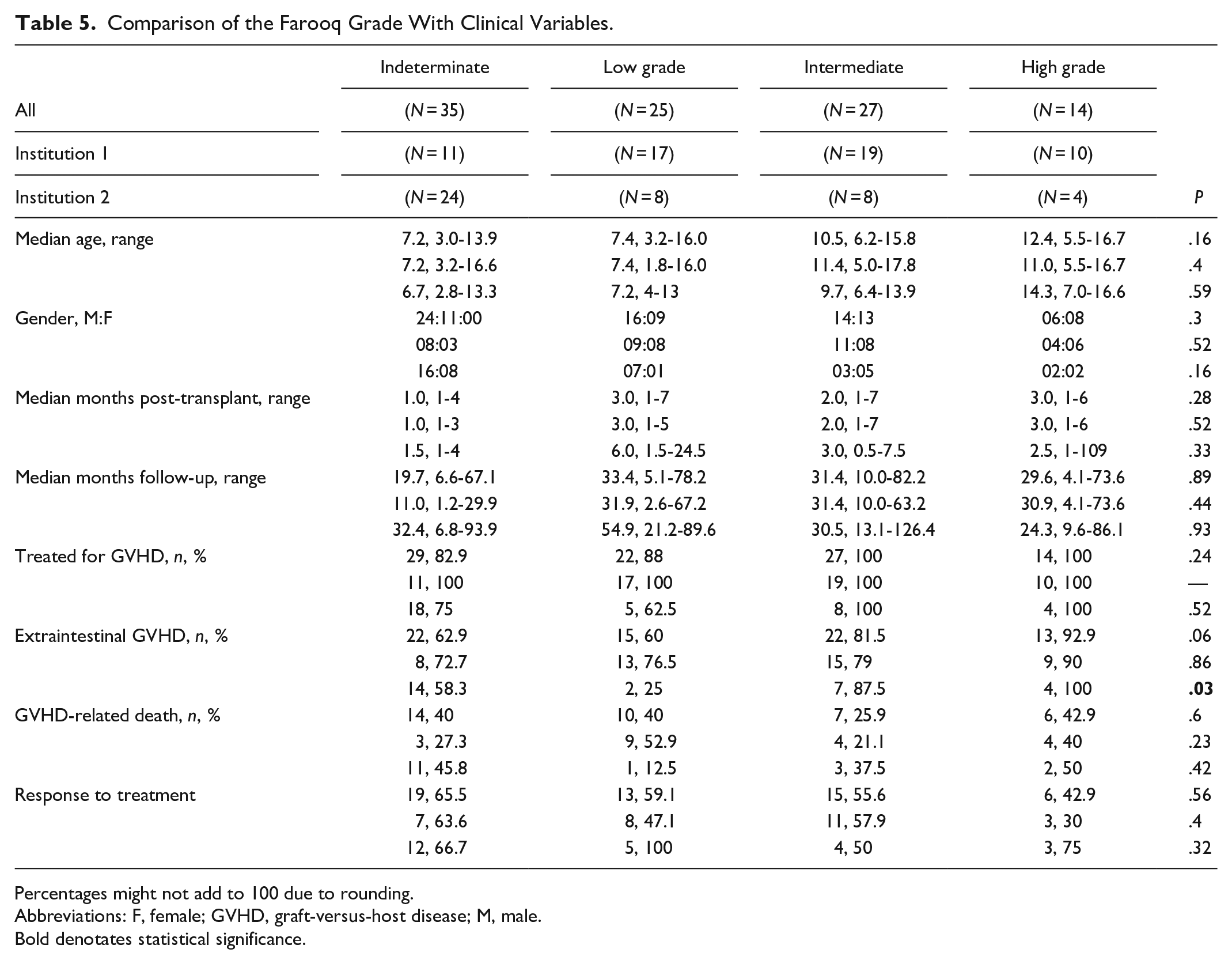
Percentages might not add to 100 due to rounding.
Abbreviations: F, female; GVHD, graft-versus-host disease; M, male.
Bold denotates statistical significance.
Grade Changes When Using the Lerner and Farooq Systems
When comparing the grade assigned using the Lerner system to the 1 with the Farooq system a moderate agreement was seen between the grades (K = 0.47, 95% CI: 0.34, 0.59). Most cases considered as Lerner grade 1 when using the Farooq grade were considered as indeterminate (32, 66.7%), with 16 cases (33.3%) of Lerner grade 1 considered as Farooq low-grade. Among the 13 cases considered as Lerner grade 2, 3 (23.1%) regraded as indeterminate, 1 (7.7%) as low grade and 9 (69.2%) as intermediate grade. Most of the cases with a Lerner grade 3 were considered as Farooq intermediate grade (15, 75%) with the remaining 5 cases (25%) considered as Farooq low grade. Similarly, most of the cases with a Lerner grade 4 were regarded as Farooq high grade (14, 70%) but 3 cases (15%) were considered as Farooq low grade and the remaining 3 cases (15%) as intermediate grade. Of note, all cases considered as Farooq high grade were Lerner grade 4.
Comparison of GVHD-Related Death and Grading Systems
After a median follow-up of 31.4 months (IQR: 6.2–74.2), 37 patients (36.6%) died due to GVHD-related causes. No difference was seen between the number of GVHD-related death across institutions (Table 2). There was no difference between apoptotic bodies using 6 and 9 as cutoffs, and crypt score with GVHD-related death (Table 6). Using the Lerner grade no difference was seen with GVHD-related death either in the overall group (P = .63; AUC = 0.57) or on each institution. Similarly, no difference was seen on GVHD-related death using the Farooq grade (P = .60; AUC = 0.57) but cases from institution 1 were marginally adequate (AUC = 0.66; 95% CI: 0.51, 0.81). Extraintestinal GVHD involvement was associated with GVHD-related death (P = .04; AUC = 0.6), and as expected response to treatment was also associated with GVHD-related death (P ≤ .01; AUC = 0.67). The GVHD-related death analysis using the modified Lerner and Farooq grading systems is presented in the Supplemental Table 4.
GVHD-related Death Across All Cases and Each Institution.
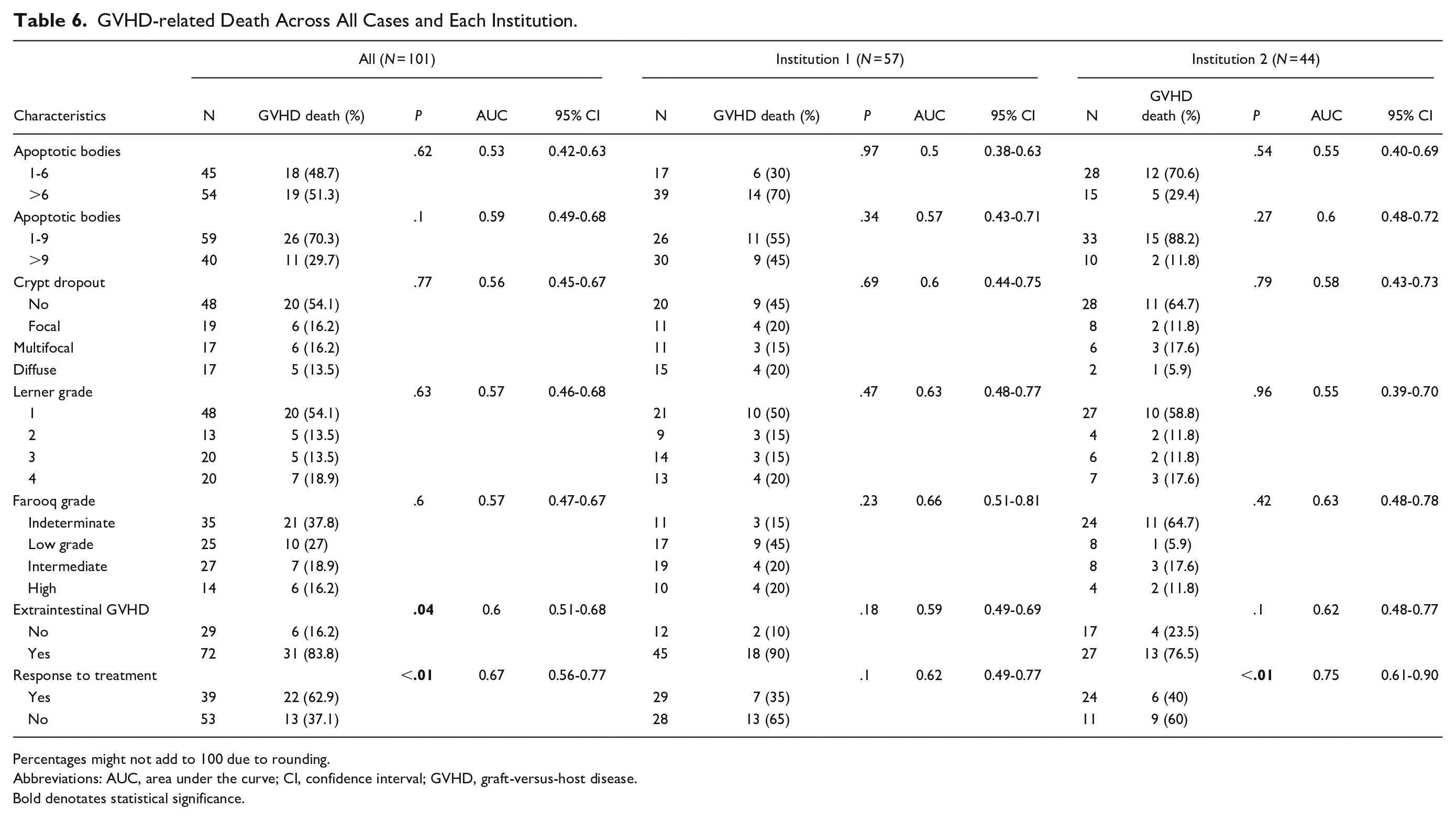
Percentages might not add to 100 due to rounding.
Abbreviations: AUC, area under the curve; CI, confidence interval; GVHD, graft-versus-host disease.
Bold denotates statistical significance.
Discussion
This study, to the best of the authors’ knowledge, presents for the first time a characterization of colonic GVHD in a cohort of patients entirely composed of pediatric patients from 2 pediatric centers. Additionally, it evaluated the commonly used Lerner grade in these cases as well as the recently proposed grading system, the Farooq grade. Unfortunately, in this cohort of pediatric patients, neither the Lerner or the Farooq grading systems correlated with GVHD-related deaths or with treatment response in the overall cohort. However, in institution 1 the Farooq grade was marginally adequate for GVHD-related deaths (AUC = 0.66; 95% CI: 0.51, 0.81). Additionally, the modify versions of the Lerner grade and the Farooq grade which includes the extent of crypt dropout did not yield any additional benefit hence given their added complexity is not recommended for clinical practice.
One of the key features of GVHD is apoptotic bodies which, as expected, was seen in all the cases apart from 2 cases without available crypts for assessment. When using the proposed cut-off of 6 apoptotic bodies in 10 contiguous crypts,1,3,7,18 54% of the cases met this criterion which is similar to the rate observed in the initial study proposing this criterion which was entirely composed of adult patients. 3 However, this rate was lower than the 1 seen in the study by Farooq et al, 1 in which 62% of cases met this threshold (P = .02); of note, this study included some pediatric patients in their validation cohort (median age of 50.7, range: 1.4–72.2). In terms of the presence of crypt dropout and ulceration, these features were seen at an equal rate compared to the study by Farooq et al. 1
The most widely used system for the histologic grading of GVHD is the Lerner grade proposed 50-years-ago. 6 As expected, significant changes in our treatment and understating of GVDH have occurred throughout these years warranting the evaluation of new models. One of the main limitations of the Lerner grade is the lack of clear guidelines for the diagnosis of grade 1 GVHD. Thus, it is still debatable what the minimal criteria to render a diagnosis of GVHD is with the most common threshold used being the presence of 1–2 apoptotic bodies per biopsy fragment.2,5,7 However, this threshold is nonspecific and a higher cutoff of 6 apoptotic bodies in 10 contiguous crypts is suggested by many as it imparts a higher specificity. 3 The Farooq grade attempted to fill this gap of the Lerner grade by including a clear demarcated threshold of 6 apoptotic bodies in their system. This results in a greater incidence of indeterminate cases which on Lerner would’ve been considered as grade 1 GVHD.
Considering this, it is not surprising to see only a moderate agreement when comparing the grade assigned with the Lerner system to the grade using the Farooq system (K = 0.47; 95% CI: 0.34–0.59). The largest difference in grading, as expected, was within the Lerner grade 1 given the lack of a minimal criteria for cases with only rare apoptotic bodies. When applying a cut-off of 6 apoptotic bodies, 32 cases (66.7%) considered as Lerner grade 1 cases were reassigned as indeterminate for GVHD using the Farooq grade. This highlights the need for standardized criteria and a minimal threshold for the diagnosis and grading of GVHD, and advocates in favor of using the Farooq system. One important limitation of the Farooq grade is when crypts are not available for evaluation as the authors acknowledge in their study. This rare scenario occurred in 2 cases in the current study, both having diffuse ulceration hence considered as Lerner grade 4 but with the Farooq system regarded as low grade.
Among the main differential diagnoses when evaluating biopsies for colonic GVHD includes MMF-induced colitis, CMV colitis, and conditioning regimens.2,19-23 Although a third of the patients were treated with MMF, the classic histologic features of MMF-induced colitis were not seen in any of the cases.19,22 Similarly, viral inclusions were not seen in any of the cases and none of the patients had ongoing CMV viremia. Conditioning regimens can present with similar features to GVHD, namely apoptotic bodies and crypt cell regeneration, however, these histologic features in the setting of conditioning regimen are found within the first 20 days of transplantation.2,23 In this study, only 4 cases presented within 21 days of transplantation and these cases did not show other histologic features suggestive of conditioning regimen such as epithelial atrophy and mucin depletion.
One of the limitations of this study is its retrospective nature which adds some inherent biases, particularly as the cohort extends over 15 years with different treatment and diagnostic approaches used across the years. Another potential difference are the several significant differences between the histologic features and the different institutions; however, the authors see this as an advantage of the study as it ensures a diverse patient population which is ideal when validating grading models developed with different patient populations. Additionally, although the study consists of significantly lower number of patients compared to studies in the adults’ literature, given the rarity of colonic GVHD in pediatric patients and the involvement of 2 centers, this study sample size is representative of the spectrum of colonic GVHD in this patient population.
In summary, this study presents the first comprehensive pathology characterization of colonic GVHD in the pediatric population. Crypt apoptosis was universally seen in almost all cases but with only half of them being greater than 6 apoptotic bodies. There was no difference in GVHD-related death or treatment response with either the Lerner grade or the Farooq grade. However, given the more objective quantification and assessment of crypt apoptotic and crypt damage, the authors suggest utilizing the Farooq grade in the pediatric population rather than the Lerner grade. Additionally, studies are needed to continue to characterize colonic GVHD in this patient population and to develop additional models that could potentially predict treatment response or GVHD-related deaths.
Supplemental Material
sj-xlsx-1-pdp-10.1177_10935266251330159 – Supplemental material for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population
Supplemental material, sj-xlsx-1-pdp-10.1177_10935266251330159 for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population by Ahmad Alkashash, Sruthi Bhamidipalli, Benjamin J. Wilkins, Omer A. Saeed and Iván A. González in Pediatric and Developmental Pathology
Supplemental Material
sj-xlsx-2-pdp-10.1177_10935266251330159 – Supplemental material for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population
Supplemental material, sj-xlsx-2-pdp-10.1177_10935266251330159 for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population by Ahmad Alkashash, Sruthi Bhamidipalli, Benjamin J. Wilkins, Omer A. Saeed and Iván A. González in Pediatric and Developmental Pathology
Supplemental Material
sj-xlsx-3-pdp-10.1177_10935266251330159 – Supplemental material for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population
Supplemental material, sj-xlsx-3-pdp-10.1177_10935266251330159 for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population by Ahmad Alkashash, Sruthi Bhamidipalli, Benjamin J. Wilkins, Omer A. Saeed and Iván A. González in Pediatric and Developmental Pathology
Supplemental Material
sj-xlsx-4-pdp-10.1177_10935266251330159 – Supplemental material for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population
Supplemental material, sj-xlsx-4-pdp-10.1177_10935266251330159 for Validation of a Recently Proposed Histologic Grading System (The Farooq Grade) for Colonic Graft-Versus-Host Disease in the Pediatric Population by Ahmad Alkashash, Sruthi Bhamidipalli, Benjamin J. Wilkins, Omer A. Saeed and Iván A. González in Pediatric and Developmental Pathology
Footnotes
Authors’ Note
Preliminary results of this study were presented as a platform presentation at the 2023 Society for Pediatric Pathology (SPP) spring annual meeting.
Authors’ Contribution
A.A., data acquisition, review and editing. S.B., statistical analysis, interpretation of data, review and editing. B.J.W. and O.A.S., analysis, review and editing. I.A.G., conceptualization, data acquisition, analysis, interpretation of data, writing of original draft, review and editing.
Data Availability
The datasets used during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The expenses of this project were covered by the Department of Pathology and Laboratory Medicine of Indiana University School of Medicine, Indiana, USA.
Ethics Approval
Indiana University School of Medicine and Children’s Hospital of Philadelphia institutional review board (IRB) were obtained prior initiation of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.