
Abstract
We report a rare case of gestational alloimmune liver disease (GALD) and congenital athymia in a 3-week-old premature male neonate, born via in vitro fertilization (IVF) surrogacy. The neonate initially presented with disseminated intravascular coagulation and septic shock, and subsequently developed liver failure. Despite aggressive treatment, he succumbed. Autopsy confirmed GALD, congenital athymia, splenomegaly, and extensive hemorrhage in the gastrointestinal mucosa and brain. Congenital athymia, characterized by a lack of functional T cells, might impair immune regulation or tolerance mechanisms and reduce the neonate’s capacity to recover from GALD-induced liver injury. The additional context of an IVF surrogate pregnancy further complicates the immunologic landscape. This case highlights the need for further investigation into potential causal or synergistic relationships among these conditions to optimize management strategies for affected neonates.
Keywords
Introduction
Gestational alloimmune liver disease (GALD) and congenital athymia are both rare and severe conditions,1,2 and their concurrent occurrence has not been previously reported. This case report describes a premature neonate, born via in vitro fertilization (IVF) surrogacy, who was diagnosed with both GALD and congenital athymia. The neonate presented with severe systemic manifestations, including disseminated intravascular coagulation, septic shock, and liver failure. Despite aggressive medical interventions, the neonate succumbed to complications. This case aims to raise awareness of a potential causal or synergistic relationship between GALD and congenital athymia.
Case Report
Clinical Summary
A 3-week-old male neonate, born prematurely at 34 weeks and 5 days via cesarean section due to a low biophysical profile, was initially admitted to the NICU at an outside facility for prematurity. He was started on trophic feedings but became NPO after developing coffee-ground emesis. On day 2 of life, the neonate developed disseminated intravascular coagulation (DIC), septic shock, and renal failure, requiring pressor support and multiple blood transfusions. A sepsis evaluation was performed, and the neonate was treated with broad-spectrum antibiotics for culture-negative sepsis and acyclovir.
On day 11 of life, the neonate was transferred to our institution for management of liver failure, with suboptimal imaging suspicious for extra-hepatic hemosiderosis, suggesting GALD. He also developed upper gastrointestinal hemorrhage and had hypothyroidism, managed with Synthroid.
Further imaging confirmed a diagnosis of GALD. The neonate subsequently underwent 2 double-volume exchange transfusions followed by intravenous immunoglobulin (IVIG) administration on days 15 and 16 of life, respectively; however, liver function showed no improvement. Persistent coagulopathy, hyperammonemia, and declining alpha-fetoprotein (AFP) levels (30 100 ng/mL on day 15 and 10 300 ng/mL on day 19 of life) were indicative of impaired hepatic regeneration. Additionally, brain imaging revealed deep medullary vein thrombosis and extensive cerebellar hemorrhage. After in-depth discussions with the family regarding the poor neurological prognosis, the decision was made to shift the focus of care. Compassionate extubation was performed, and the neonate passed away shortly thereafter.
This is a surrogate pregnancy conceived via IVF with embryo transfer. The biologic mother (oocyte source) had no prior pregnancies (G0P0), and the surrogate mother was a healthy 24-year-old, G2P1102. The prenatal course was largely unremarkable, with no clinical or radiologic suspicion of hepatic dysfunction. The neonate was born with a birth weight of 1785 g and length of 41.5 cm, both between the 3rd and 10th percentiles, and had Apgar scores of 8 at both 1 and 5 minutes. The prenatal course was largely unremarkable, with no documentation of oligohydramnios or ascites. Blood type testing revealed that the neonate was B positive and the surrogate mother was O positive; the direct antiglobulin test (DAT) was negative. A comprehensive workup for TORCH infections, metabolic disorders, and mitochondrial diseases was performed and yielded negative results. The placenta was not available for examination due to delivery at an outside institution.
Autopsy Findings
The major autopsy findings included GALD with submassive confluent hepatic necrosis with loss of reticulin framework, extensive bile ductular proliferation, cholestasis, and cirrhosis, and siderosis in multiple organs, including liver, pancreas, thyroid, and myocardium (Figure 1), athymia and extensive hemorrhage in the gastrointestinal mucosa and brain. Additional abnormal findings include a 3-lobe left lung, a hypoplastic thyroid gland, and splenomegaly.
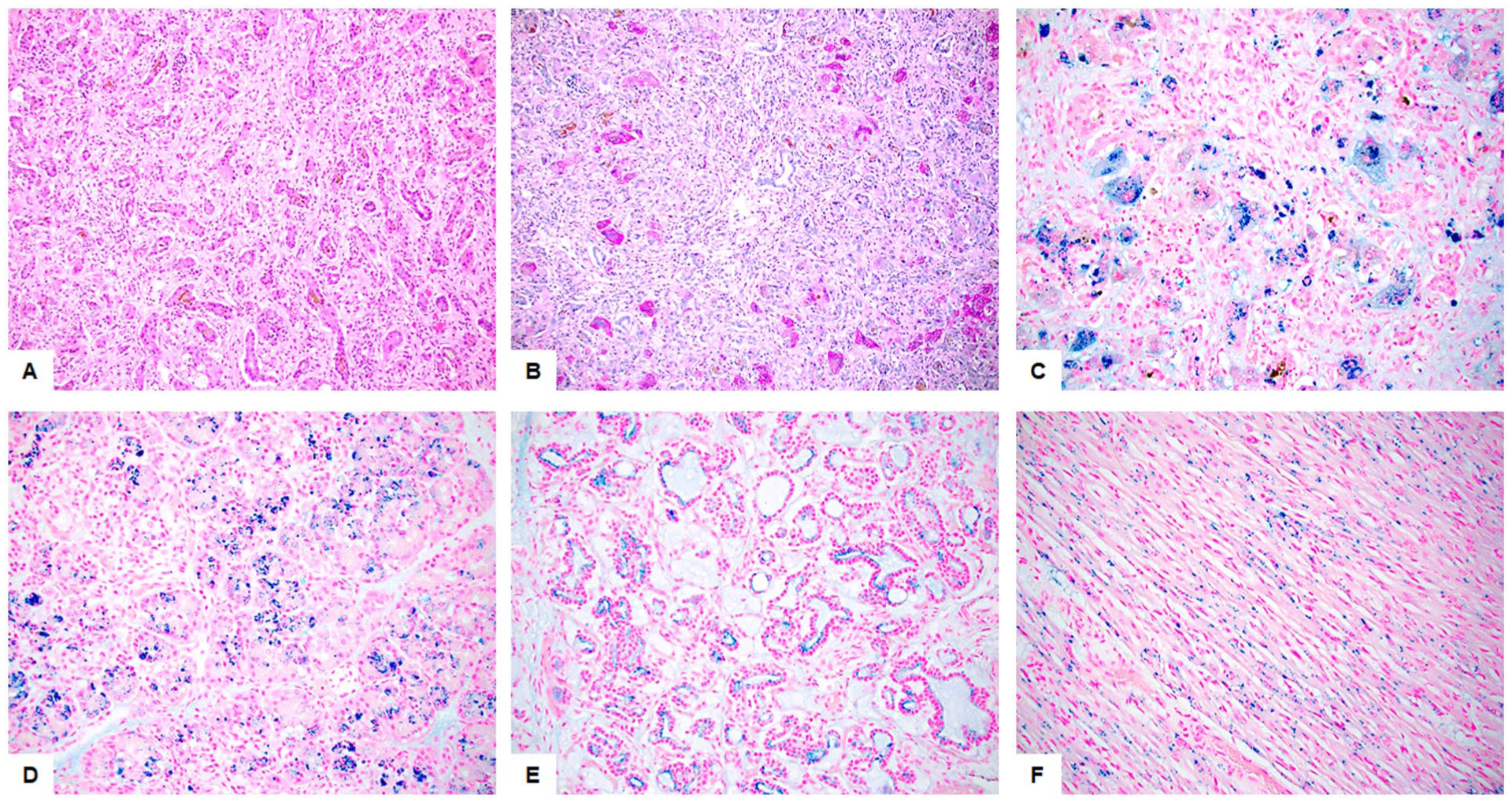
(A) H&E staining of the liver reveals submassive confluent necrosis of the hepatic parenchyma, with the damaged areas being replaced by extensive ductular proliferation, cholestasis, and fibrosis. (B) PAS staining highlights scattered preserved hepatocytes within the liver. (C-F) Perl’s Prussian blue staining demonstrates excessive iron deposits in the liver (C, mainly Kupffer cells), pancreas (D), thyroid (E), and myocardium (F). Original magnifications: 100× for A and B, 200× for C to F.
Molecular Findings
Clinical exome sequencing at our institution of both the decedent and his biologic mother revealed no clearly established clinically significant variants.
Discussion
We present a rare case of GALD and congenital athymia in a premature neonate born via an IVF surrogate pregnancy, which ultimately resulted in a fatal outcome.
The true mechanism of GALD remains theoretical, with the alloimmune hypothesis being the most widely accepted.3,4According to this hypothesis, an antigen expressed in the fetal liver is not recognized by the maternal immune system as “self.” The mother (in this case, the surrogate mother) produces immunoglobulin G (IgG) antibodies, which are transported across the placenta beginning around the 12th week of gestation. These antibodies bind to fetal hepatocytes, activate the terminal complement cascade, and cause varying degrees of hepatocyte injury. The lack of genetic relevancy between the surrogate mother and the fetus could theoretically increase the risk of GALD, as the surrogate’s immune system may be more prone to mount an immune response against the fetal liver cells. However, there is currently no evidence in the literature to support an increased risk of GALD associated with surrogacy.
GALD is a leading cause of neonatal liver failure, accounting for 60% to 90% of cases. 5 Despite its significance, diagnosing GALD remains challenging due to its variable clinical presentations, which can range from asymptomatic to acute liver failure. Neonates with liver failure due to GALD typically present with hypoglycemia, coagulopathy, hypoalbuminemia, jaundice, and edema. Laboratory findings often include marked hyperbilirubinemia, significantly elevated AFP, and high serum ferritin levels. Extrahepatic siderosis is a hallmark feature that distinguishes GALD from secondary hemochromatosis and can be detected by imaging, such as MRI, or by minor salivary gland biopsy. The definitive diagnosis in our case was delayed, in part due to the initial suboptimal imaging quality and a limited biopsy specimen obtained at an outside institution. While liver biopsy is not the definitive diagnostic tool for GALD, it may be used to assess the severity of liver damage and look for specific immune markers like C5b-9 deposition, which can support the diagnosis.
The treatment of GALD typically involves a combination of double-volume exchange transfusion to remove existing reactive antibodies, followed by IVIG to block antibody-induced complement activation. 6 Our patient received 2 double-volume exchange transfusions followed by IVIG 2 weeks later; however, liver function did not recover. Due to size constraints and the presence of severe comorbidities, liver transplantation was not a option in this case.
Congenital athymia is a severe immunodeficiency disorder characterized by the absence or underdevelopment of the thymus, an organ essential for the development of T-lymphocytes and proper immune function. 2 Patients with congenital athymia typically present with a complete absence of T cells but normal numbers of B cells and natural killer (NK) cells, resulting in a T−B+NK+ immunophenotype, similar to that observed in severe combined immunodeficiency (SCID). Consequently, congenital athymia is often identified during newborn screening for SCID. 7 Neonates with congenital athymia are highly susceptible to infections and have an increased risk of developing autologous graft-versus-host disease (GVHD) and autoimmune disorders. 2 In this case, the neonate developed hypothyroidism, a well-documented complication of congenital athymia. The absence of functional T cells in this neonate might impair immune regulatory mechanisms relevant to GALD pathogenesis and limit the ability to modulate alloimmune injury. Consequently, this could contribute to a more severe or prolonged maternal alloimmune response against fetal hepatocytes and diminish the neonate’s capacity for hepatic repair and regeneration.
The traditional management of congenital athymia has focused on supportive care to prevent and manage infections. The only potential curative option currently available is allogeneic thymus transplantation.7,8 However, the presence of GALD in this case added an additional layer of complexity to management. Moreover, the premature birth of this neonate further complicated the clinical course.
In conclusion, this is the first reported case of concurrent GALD and congenital athymia resulting in a fatal outcome. Congenital athymia, characterized by a lack of functional T cells, might impair immune regulation or tolerance mechanisms and reduce the neonate’s capacity to recover from GALD-induced liver injury. The additional context of an IVF surrogate pregnancy further complicates the immunologic landscape. This case highlights the need for further investigation into potential causal or synergistic relationships among these conditions to optimize management strategies for affected neonates.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.