
Abstract
Introduction:
Anterior cutaneous nerve entrapment syndrome (ACNES) is an underdiagnosed, but common, cause of abdominal pain in children. It is unknown if the involved nerves are normal or are pathologic and should be divided or released and retained. We present the pathology findings of resected nerves in children with ACNES.
Methods:
Operative reports, pathology reports, and clinical notes of consecutive patients who underwent anterior neurectomy from December 2011 to September 2023 were reviewed.
Results:
One hundred and three pathology specimens from 78 patients were evaluated. Twenty-nine of the 103 specimens were from re-operative cases. Of the 103 pathology specimens, 71 (69%) had pathologic findings in the form of: myxomatous change (49, 69%), myelin vacuolar degeneration (22, 31%), perineural fibrosis (15, 21%), traumatic neuroma-like changes (2, 3%), and possible axonal injury (1, 1%). Four specimens (4%) did not have an identifiable nerve.
Conclusion:
The majority of nerve specimens from patients with ACNES were found to have changes consistent with chronic nerve damage distal to the location of presumed entrapment. Resection of these cutaneous nerves, rather than release and retention, seems prudent.
Level of evidence:
III
Introduction
Abdominal cutaneous nerve entrapment syndrome (ACNES) is an increasingly recognized source of abdominal pain. Siawash et al. found a prevalence of 13% in a single center when further examining patients being managed for chronic abdominal pain of unknown etiology over a 2-year time period. 1 Once the diagnosis is made by physical exam and the patient’s history, patients often undergo a nerve block for both diagnostic and therapeutic purposes. While the nerve block may be repeated multiple times with variable amounts of success, some patients require further escalation to surgical intervention by resection of the affected nerves. 2
Studies on the pathology of resected nerves from ACNES are sparse. There have been multiple proposed etiologies of ACNES including infection, inflammation, or trauma to the nerve. 3 Only more recently has the etiology been suggested to be due to the compression of the nerve rather than infection or inflammation.2,4
This study reports the pathology findings of resected nerves in a large cohort of children with ACNES.
Methods
This is a retrospective study that evaluated a total of 103 specimens that were obtained from anterior neurectomies performed on 78 pediatric patients from December 2011 to September 2023. Patients who underwent fascial release without a specimen obtained from the intervention were excluded from this review (19 patients). Patients were diagnosed with ACNES based upon history and clinical exam in the pediatric surgery clinic and underwent a diagnostic/therapeutic local nerve block prior to any operation. The operations were completed by a single pediatric surgeon at Boston Children’s Hospital. The surgery was performed as detailed in the article by Mooney, which included preoperative marking of the abdomen at the area of maximal pain, dissection to the anterior rectus sheath with division and resection of any encountered nerves coursing through the investing fascia in the area of discomfort. 5 Operative and pathology reports were reviewed, and histopathological examination was conducted by various anatomic pathologists and confirmed with central review by a neuropathologist.
Results
One hundred and three specimens from 78 patients who underwent anterior neurectomy were available for review. Patients were majority female (76%), with a mean age of 16 years (range 10-29, Table 1). Four (4%) specimens did not contain identifiable nervous tissue, 28 (27%) did not have significant pathologic changes and 71 (69%) showed pathologic changes (Figure 1). Pathologic changes included: myxomatous change of the nerve in 49 (69%), myelin vacuolar degeneration in 22 (31%), perineural fibrosis in 15 (21%), traumatic neuroma-like changes in 2 (3%), and possible axonal injury in 1 (1%) patient (Figure 2).
Patient Demographics.
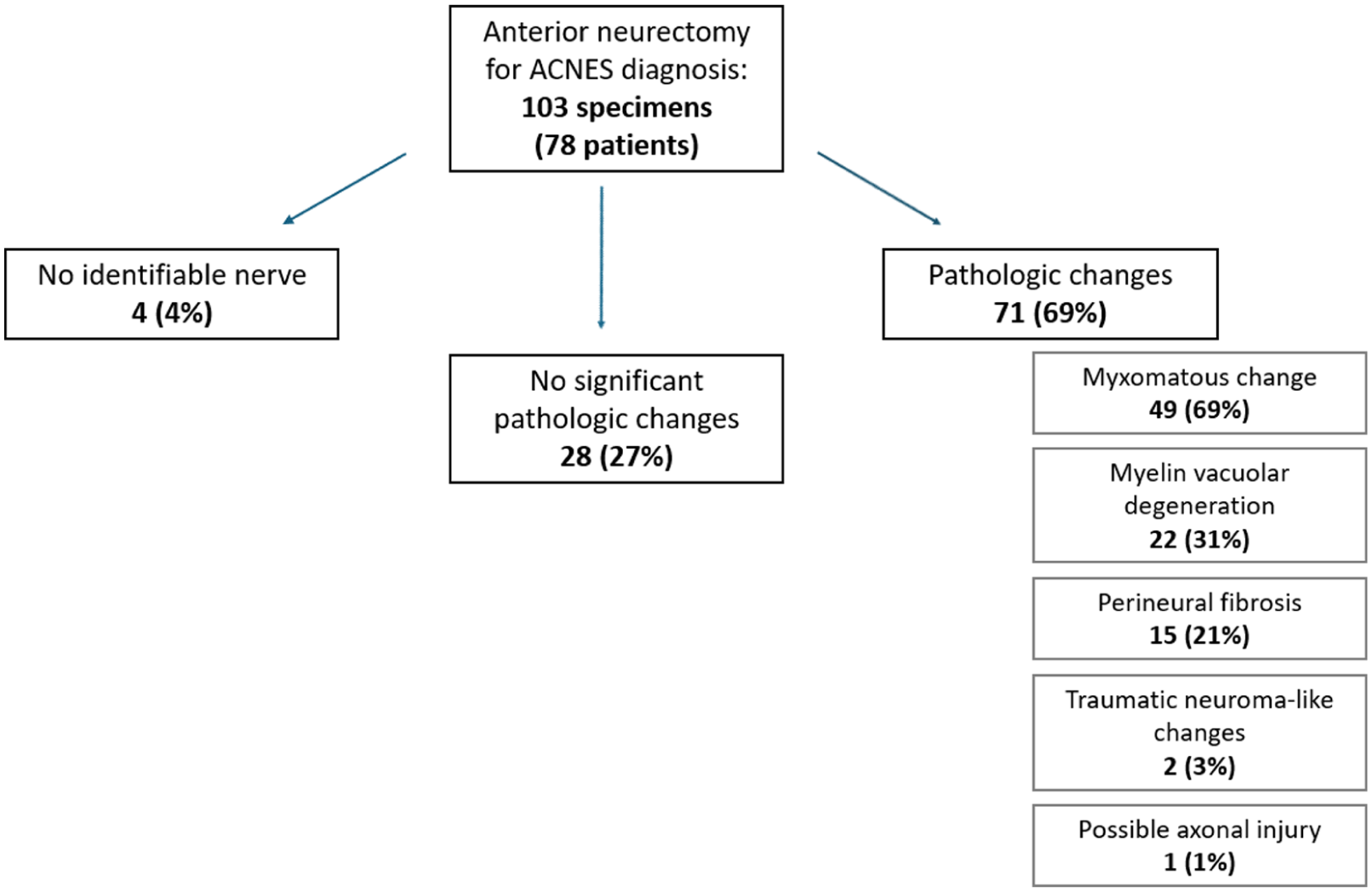
Pathology outcomes of ACNES specimens.
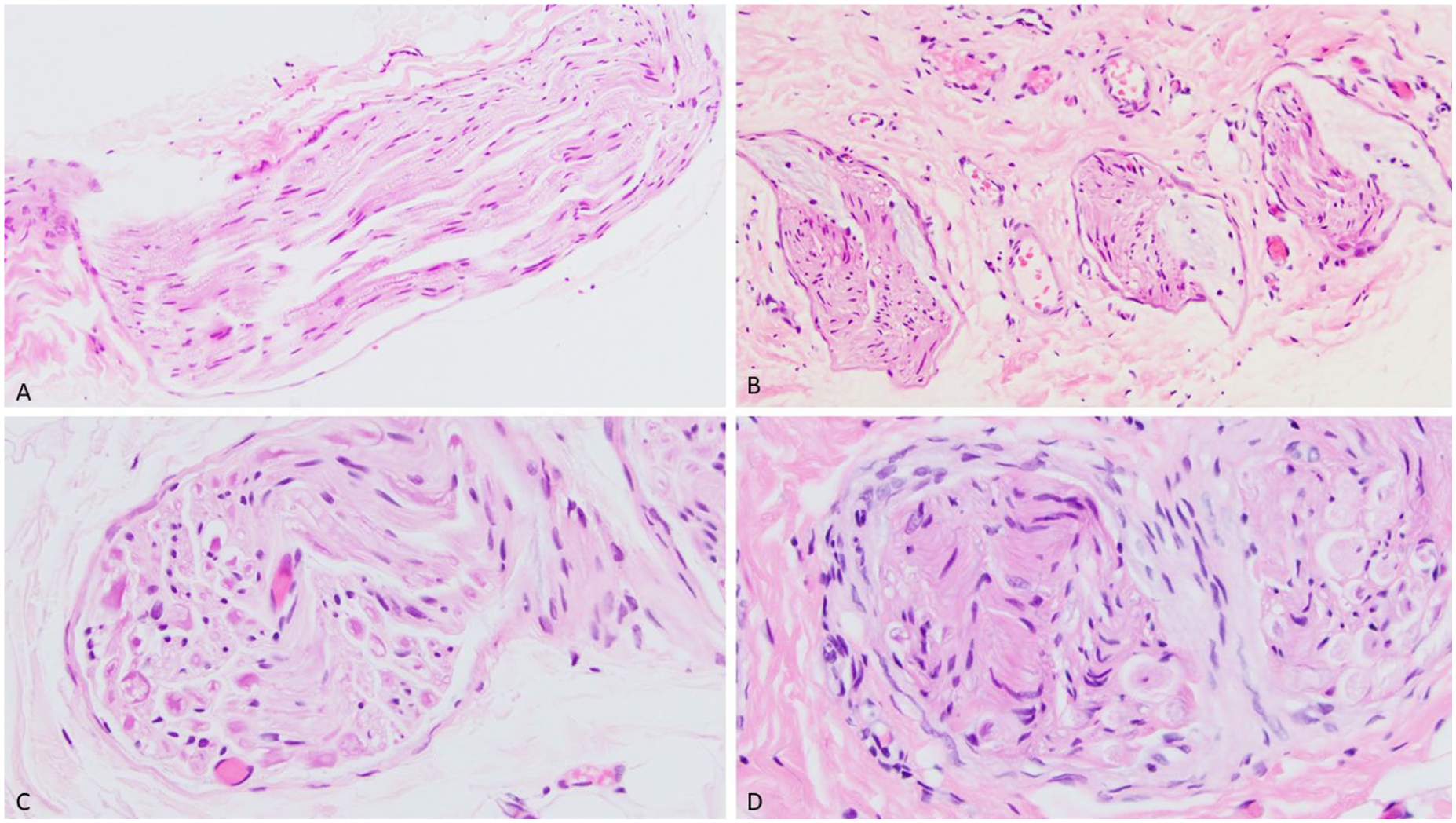
Histological findings in ACNES, hematoxylin-eosin stain. (A) A nerve from a case with no significant pathologic findings; the axons, myelin sheath, Schwann cells and perineurial cells are generally unremarkable. (B) Nerves with myxoid stroma accumulation. (C) Cross section of a nerve with myelin clumps and axons of variable thickness. (D) The hyperplastic perineurium seen in a subset of ACNES resection specimens.
Forty-eight patients (62%) achieved pain relief. Of those patients, 38 had pain relief after 1 operation and 10 patients required 2 or more operations. Thirteen patients (17%) did not achieve pain relief after operative intervention and 17 (21%) patients were lost to follow up.
Discussion
ACNES remains an under-diagnosed cause of abdominal pain. Given the infrequency of its diagnosis, the optimal management strategy remains unclear. The involved nerve may be released or resected, the selection of which method hinges in part on whether the nerve is normal or not. This study evaluated the histology of nerves resected for ACNES and identified chronic nerve damage in the majority of specimens, consistent with what would be expected in nerves distal to an area of chronic compression. The identification of pathologic nerve findings supports an etiology of compression for ACNES and supports the resection of the involved cutaneous nerve branches, rather than their release and retention.
The patients without long-term pain relief, in the majority still had abnormal pathology of the resected nerves (7 of 13 patients). Interestingly, one of the patients required 4 operations for pain that “recurred” but in a different location each time, and their final operation was the only 1 with pathologic changes of the nerve. It is unclear why these patients did not achieve long-term pain relief when the apparent culprit nerve was resected and further investigation into the etiology of ACNES may help in answering this.
The rate of pathologic change in the nerve specimens was 69%. The surgical technique of anterior neurectomy includes exploration along the rectus sheath and resection of the offending nerve along with any other peripheral nerves that are encountered in the area of pain, in case that they are the true pain culprit. Thus, it is not unexpected to have nerve specimens without pathologic findings.
There are limited studies that describe the pathology findings of the nerves obtained from a neurectomy in ACNES patients. In a study by Markus et al., they evaluated the histology of a small cohort of patients who underwent anterior neurectomy for ACNES. 4 They found the nerve specimens to be consistent with degenerative changes without signs of inflammation and thus concluded the etiology of ACNES to be consistent with nerve compression. Our study found various degenerative changes in the majority of specimens and is consistent with this previous work, which we believe further supports the etiology of direct compression of the nerve.
A limitation of this study includes the loss to follow up of 17 patients or approximately 21% of the study group. This is not surprising as this operation is not widely available and some patients travelled from across the country or occasionally, internationally for this treatment. Additionally, our average patient age is 16 years old, which is approaching the time that patients “age out” of pediatric care and may continue care elsewhere. In 26 of the 29 specimens from re-operative cases, the indication was for a recurrence at the previous site – we acknowledge that for that group of specimens, there may be some effect on the tissue as the specimen is resected from a previously operated in field and may affect the pathology results. Additionally, as this was a retrospective review of a cohort of patients who had pathological tissue available for exam, we cannot compare the pathology of normal nerves in such a study and the results should be interpreted within that context.
Conclusion
The findings of trauma with histological abnormalities consistent with chronic damage, supporting their resection rather than release and retention.
Footnotes
Author Note
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.