
Abstract
Background and Aims:
Langerhans cell histiocytosis (LCH) commonly affects children. The histological distinction of hepatic LCH from its mimickers is challenging and often requires judicious use of immunohistochemistry in the correct clinical and radiological context. We described the patterns of hepatic LCH and applied an ensemble transfer-learning model to predict and distinguish hepatic Langerhans cell infiltration from histological mimics.
Materials and Methods:
Clinical, histological, and immunophenotypic data from 6 pediatric LCH cases with liver biopsies were retrieved from the archives. The histological patterns were reviewed. Histological images were obtained from all cases of hepatic LCH with histologically overt Langerhans cell infiltration, as well as from cases with histological mimickers. A soft-voting-based ensemble transfer learning model was applied to the images after splitting them into training, validation, and test sets. The performance metrics were evaluated.
Results:
All cases were multisystem LCH (MS-LCH). The hepatic histomorphology showed sclerosing cholangiopathy with/without Langerhans cell infiltration as the most common pattern. Bile extravasation and cystic dilatation were noted in a single case. Eosinophilic microabscesses, cholangiopathy, and portal-based aggregates are the important histological clues. The ensemble learning model had an area under the curve (receiver operating characteristic) of 0.99, with sensitivities, specificities, and accuracies of 33.3%, 100%, and 75%, respectively.
Conclusion:
Sclerosing cholangiopathy with or without Langerhans cells is the most common pattern of hepatic LCH. An ensemble transfer learning model can serve as a valuable screening tool for histopathologists to predict and diagnose hepatic LCH.
Keywords
Introduction
Langerhans cell histiocytosis (LCH) is a clonal neoplasm of myeloid dendritic cells depicting characteristic histomorphology and immunophenotype.1,2 It commonly affects the pediatric population and can involve single or multiple organ systems. The involvement of the liver in the pediatric population is not uncommon, although it is a high-risk feature. The diagnosis of hepatic LCH seldom requires a liver biopsy, and histomorphology can exhibit multiple overlapping patterns, leading to diverse differential diagnoses.
A convolutional neural network (CNN) is a deep learning (DL) model that performs complex tasks, such as image recognition, by extracting feature maps directly from images, with high predictive accuracy. 3 The transfer learning models are pre-trained CNN models. An ensemble transfer learning model combines features from multiple transfer learning models and reduces individual bias, achieving greater predictive accuracy than any single model.
We have 2 distinct objectives in this study. The first is to describe the patterns of hepatic LCH in pediatric liver biopsies from our center, a tertiary institute in North India. The second is the application of an ensemble transfer learning model to distinguish the histological images of hepatic LCH infiltration from its histological mimickers. This study, to the best of our knowledge, appears to be the first of its kind to apply an ensemble transfer learning model to histological images of hepatic LCH.
Materials and Methods
Evaluation of the Clinical and Histological Spectrum
All pediatric liver biopsies performed for Langerhans cell histiocytosis (LCH) over the last 7 years (2019-2025) were reviewed, along with their clinical data (n = 6). The histological patterns of these cases, immunohistochemistry results, and follow-up data, where available, were noted.
Histological Image Acquisition and Selection
The hematoxylin and eosin (H&E)-stained slides of 3 pediatric cases (Cases 1, 2, and 3) showing overt infiltration by LCH were chosen for microphotography (The tissue for performing BRAF V600E immunostain was scant in Case 2, but there was adequate tissue in the H&E-stained slide for photography). Two previously published cases of adult hepatic LCH with overt LCH infiltration were also included. 4 The pediatric liver biopsies with no/subtle infiltration (Cases 4, 5, and 6) were excluded from image acquisition and selection to maintain high-quality training data. Four pathologists (DB, SM, RL, and NK) reviewed the slides, and representative photomicrographs depicting the characteristic histomorphology of LCH infiltration from each case were obtained using an Olympus microscope (Olympus BX53) with cellSens software version 4.3.1 (total 52 images; 10.4 images per case; 12, 8, 9, 13, and 10 images, respectively). Images obtained at both 20× and 40× objectives were collected from each case for appraisal of tissue architecture and cytomorphology. Representative photomicrographs of various other age-matched non-LCH cases depicting sclerosing cholangiopathy and/or eosinophilic microabscesses were also obtained from primary sclerosing cholangitis (n = 2), secondary sclerosing cholangitis (hepatolithiasis, IgG4-related disease, benign biliary stricture; n = 4), progressive familial intrahepatic cholestasis type 3 (PFIC3) with biliary fibrosis (n = 2), and eosinophilic abscesses (n = 2). A total of 91 images were obtained from these 10 cases (9.1 images per case; 8, 9, 13, 10, 8, 9, 10, 10, 7, 7 images, respectively). These non-LCH cases can histologically simulate the patterns of hepatic LCH. The cases of hepatolithiasis and progressive familial intrahepatic cholestasis type 3 were part of 2 previous publications. 5,6
Application of the Ensemble Transfer Learning Model
All images (n = 143) obtained from the hepatic LCH and non-LCH cases were split into training (n = 99 [69%]; 36 LCH, 63 non-LCH), validation (n = 20 [14%]; 7 LCH, 13 non-LCH), and testing sets (n = 24 [17%]; 9 LCH, 15 non-LCH) using a nearly 70:15:15 stratified ratio to maintain class balance. The dataset splitting was performed programmatically using the split-folders Python library. Images were randomly shuffled and split, maintaining the original class-wise directory structure, ensuring that images belonging to each histological class were proportionally distributed across the 3 subsets. A fixed random seed (seed = 42) was used to ensure reproducibility of the dataset partitioning. The testing dataset remained completely independent and was not used during model training or validation. All images were then resized to 224 × 224 pixels and normalized using a rescaling factor of 1/255. No data augmentation was performed to preserve the histomorphological features and avoid artificial artifacts in a small dataset involving uncommon diseases. The Langerhans cells were not annotated by the pathologists at the time of training. Three convolutional neural network (CNN) architectures, including EfficientNetB0, ResNet50, and InceptionV3, initialized with ImageNet pretraining weights, were used as base feature extractors. The convolutional backbone was frozen during training to prevent overfitting on the relatively small dataset. A custom classification head comprised a GlobalAveragePooling2D layer, a 128-unit ReLU dense layer, and a single sigmoid output neuron attached to each network. Models were trained for 5 epochs using the Adam optimizer, binary cross-entropy loss, and accuracy as the evaluation metric, with a batch size of 16. A soft-voting ensemble was implemented for final prediction, assigning weights of 0.2, 0.2, and 0.6 to EfficientNetB0, ResNet50, and InceptionV3, respectively, based on validation performance. Ensemble probabilities were thresholded at 0.5 to generate binary predictions. Three different CNN architectures were employed to leverage their complementary strengths. Performance was assessed on the independent test set. A confusion matrix was generated to count true positives, true negatives, false positives, and false negatives.
Additionally, discriminatory capability was assessed using the receiver operating characteristic (ROC) curve and its corresponding area under the curve (AUC). A classification report was generated that included sensitivity (recall/true-positive rate), specificity (true-negative rate), positive predictive value (precision), negative predictive value, accuracy, and F1 score for each class. To facilitate error analysis, all misclassified images were automatically exported and stored in a designated directory, with filenames annotated with their predicted and true labels. All experiments were implemented using Python 3.12 (TensorFlow/Keras) within the Jupyter Notebook environment (version 7.4.3). The study adhered to the norms of the Helsinki Accord, and written informed consent was obtained from the guardians of all patients at the time of biopsy. Informed consent was also obtained from the guardians of all patients under regular follow-up at the time the manuscript was drafted. Only retrospective archival material was used, maintaining the patients’ anonymity.
Results
Clinical and Histopathological Features
The authors identified 6 cases of pediatric LCH for which liver biopsies were performed in the last 7 years. All cases belonged to multisystemic LCH (MS-LCH). The liver biopsies were diagnostic for 4 cases showing infiltration by LCH, while they were performed following the induction chemotherapy in 2 other cases.
The mean age of the 4 cases with hepatic infiltration by LCH was 2.2 years (range: 0.8-5 years). All were male children. The presentations in all cases were characterized by features of cholestasis or pruritus, accompanied by hepatomegaly or hepatosplenomegaly. All 4 cases exhibited skin rashes (all biopsy-proven for LCH) and 2 cases showed cystic lung lesions (1 biopsy-proven for LCH). The mean serum total bilirubin, conjugated bilirubin, AST, ALT, ALP, GGT, total protein, albumin, and INR values were 3.3 mg/dL (range: 0.7-5.6 mg/dL), 1.8 mg/dL (range: 0.2-3.3 mg/dL), 110.7 IU/L (range: 98-123 IU/L), 59.3 IU/L (range: 49-71 IU/L), 1783.7 IU/L (range: 563-2670 IU/L), 1142.3 IU/L (range: 510-1615 IU/L), 6.5 g/dL (range: 6-7.2 g/dL), 2.9 g/dL (range: 2.5-3.5 g/dL), and 1.5 (range: 0.9-2.6), respectively. Their mean hemoglobin, total leukocyte count, and platelet count were 9.2 g/dL (range: 9.2-9.2 g/dL), 13 000/µL (range: 12 000-15 000/µL), and 2 71 000/µL (range: 1 89 000-3 14 000/µL), respectively. The mean age of both post-chemotherapy cases was 4.5 years, with a male and a female child. The biopsies in these 2 cases were performed due to persistent hepatomegaly and elevated liver enzymes. Besides, 1 case showed an intrahepatic cystic lesion. The mean serum total bilirubin, conjugated bilirubin, AST, ALT, ALP, GGT, total protein, albumin, and INR values were 0.5 mg/dL, 0.1 mg/dL, 90.5 IU/L, 105.5 IU/L, 632.5 IU/L, 563.5 IU/L, 6.2 g/dL, 3.8 g/dL, and 0.9, respectively. Their mean hemoglobin, total leukocyte count, and platelet count were 9.1 g/dL, 9000/µL, and 2 62 000/µL, respectively (Table 1).
Details of the Clinical, Hematological, Biochemical, Histological, and Immunohistochemical Details.
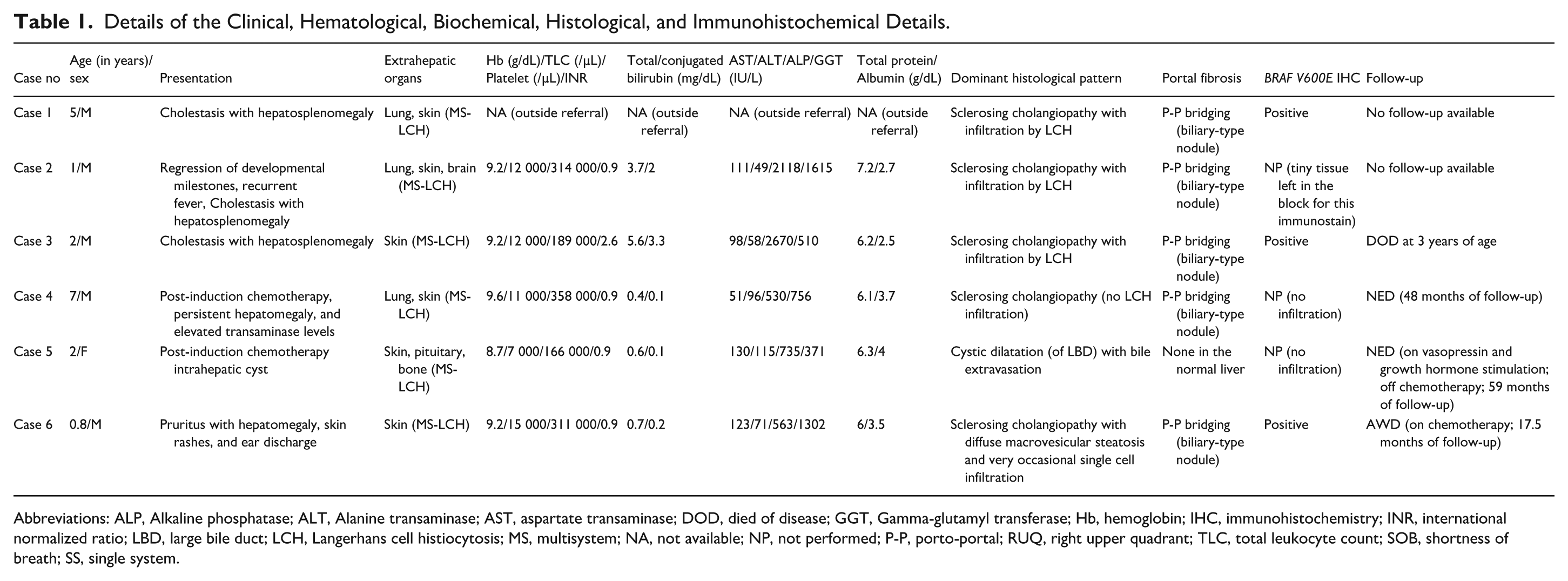
Abbreviations: ALP, Alkaline phosphatase; ALT, Alanine transaminase; AST, aspartate transaminase; DOD, died of disease; GGT, Gamma-glutamyl transferase; Hb, hemoglobin; IHC, immunohistochemistry; INR, international normalized ratio; LBD, large bile duct; LCH, Langerhans cell histiocytosis; MS, multisystem; NA, not available; NP, not performed; P-P, porto-portal; RUQ, right upper quadrant; TLC, total leukocyte count; SOB, shortness of breath; SS, single system.
The histopathology of all 3 cases with overt infiltration of LCH (Cases 1, 2, and 3) showed portal-based nodules, aggregates, and singly scattered atypical histiocytes. These atypical histiocytes showed grooved reniform nuclei, pale chromatin, inconspicuous nucleoli, and abundant eosinophilic cytoplasm and were associated with an eosinophil-rich inflammatory milieu. The eosinophils formed eosinophilic microabscesses at places and showed admixture with lymphocytes and occasional neutrophils. The portal tracts in all cases showed marked expansion, accompanied by porto-portal bridging fibrosis and the formation of biliary-type nodules. All cases exhibited characteristic cholangiopathic changes, characterized by the infiltration and destruction of interlobular bile ducts by atypical histiocytes. Occasional lymphocytic cholangitis was also noted. All cases showed moderate ductular reaction, especially in the lesional portal tracts. The portal tracts not involved by the lesion also showed mild portal fibrosis, moderate ductular reaction, and mild inflammatory infiltrate comprising lymphocytes and scattered eosinophils. None of these cases showed portal plasmacytosis or interface hepatitis. The hepatic lobules showed bilirubinostasis in 2 cases. However, there was no copper retention, lobular microgranuloma, or steatosis in any of the cases. Moderate biliary metaplasia was noted in 3 cases in which CK7 immunostaining was performed. Only an occasional case showed focal lobular inflammation and focal Kupffer cell hyperplasia. Occasional intrasinusoidal eosinophils were also noted. Langerhans cells in all cases with overt infiltration were identified by diffuse strong membranocytoplasmic immunopositivity for CD1a, and Langerin (CD207). Tissue for BRAF V600E immunohistochemistry was available in 2 cases with LCH infiltration, and both were positive for BRAF V600E (Figure 1, Table 2).
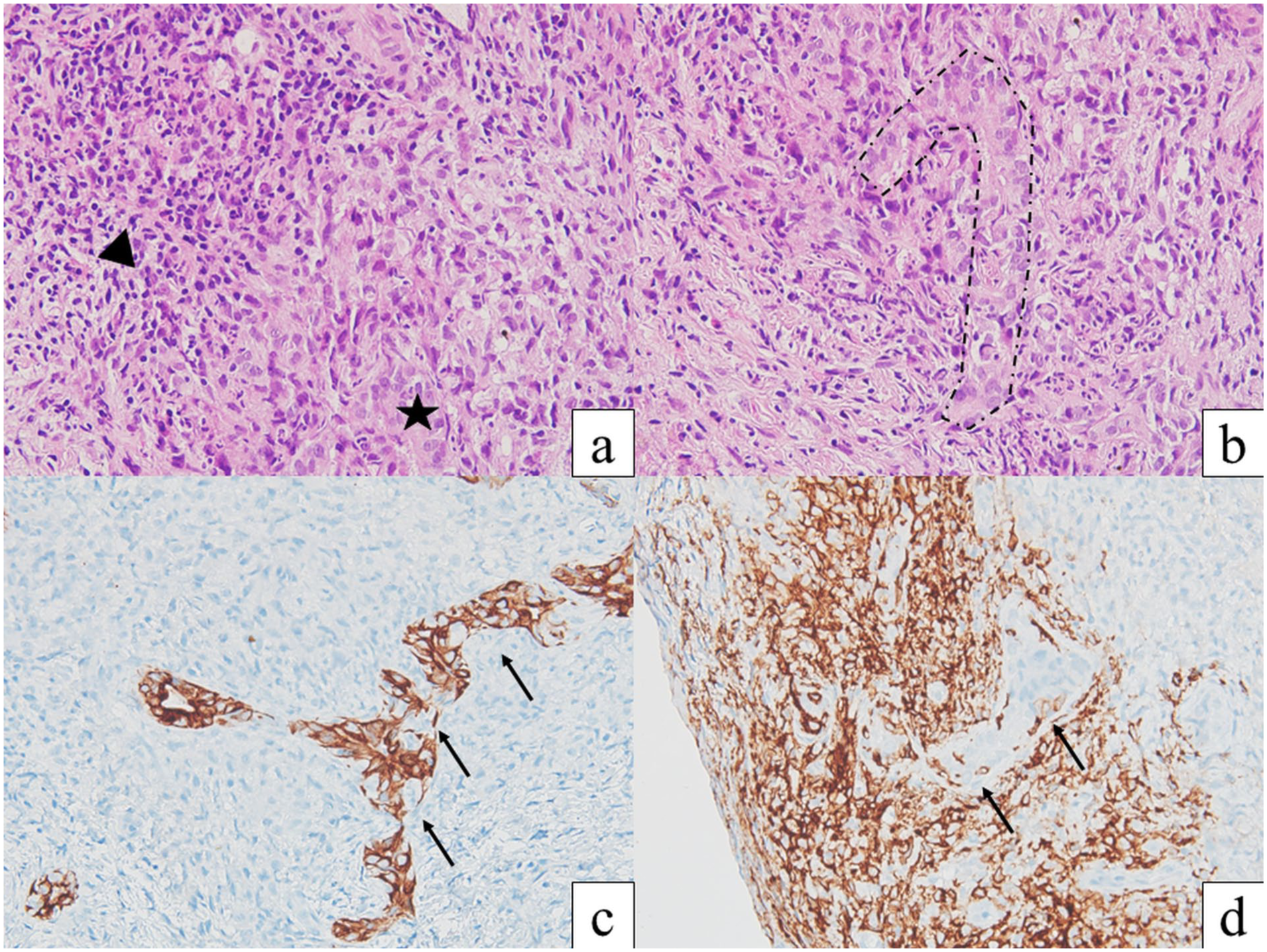
Histopathology of hepatic infiltration by Langerhans cell histiocytosis in Case 2; Portal-based aggregates of Langerhans cells at the bottom right corner (black star) admixed with aggregates of neutrophils, lymphocytes, and eosinophils (black arrowhead; a, hematoxylin and eosin, 400×); The Langerhans cells infiltrating and destroying interlobular bile duct (black dots; b, hematoxylin and eosin, 400×); CK7 immunostain highlighting destruction of the bile duct by the infiltrating Langerhans cells (black arrows). The unstained area also showed aggregates of Langerhans cells (c, 400×); Langerin immunostain highlighted portal-based aggregates with duct infiltration (black arrows; d, 400×).
Table Depicting Detailed Histological Features in the Liver Biopsies.
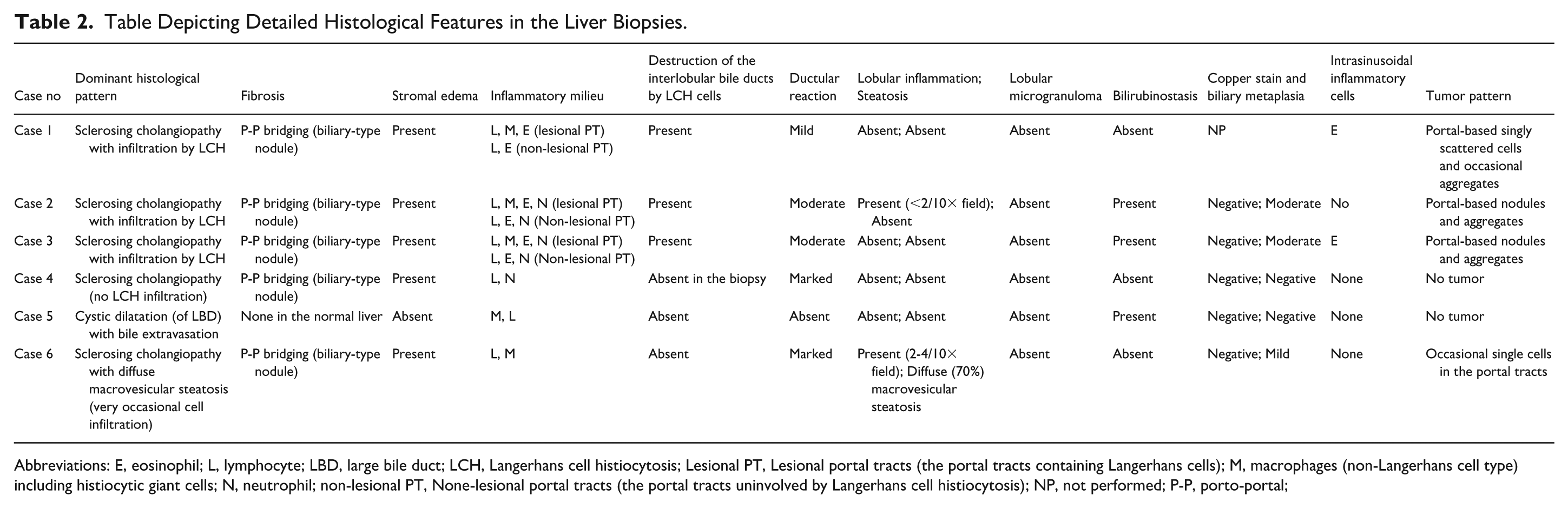
Abbreviations: E, eosinophil; L, lymphocyte; LBD, large bile duct; LCH, Langerhans cell histiocytosis; Lesional PT, Lesional portal tracts (the portal tracts containing Langerhans cells); M, macrophages (non-Langerhans cell type) including histiocytic giant cells; N, neutrophil; non-lesional PT, None-lesional portal tracts (the portal tracts uninvolved by Langerhans cell histiocytosis); NP, not performed; P-P, porto-portal;
The liver histology in a post-chemotherapy case (Case 4) showed sclerosing cholangiopathy with porto-portal bridging fibrosis, biliary-type nodule formation, exuberant ductular reaction, and occasional periductal collagen condensation. No bilirubinostasis, copper retention, or infiltration by LCH was noted. The other case (Case 5) presented a cystic lesion containing bile, along with foreign body giant cells, biliophages, and foamy macrophages within its fibrocollagenous wall. This lesion did not show any lining epithelium (possibly denuded). The liver parenchyma away from the cystic lesion appeared to be normal (Figure 2; Table 2). This lesion could result from a ruptured cyst/dilated bile duct with extravasated bile. Radiological evaluation revealed strictures in the larger bile ducts, accompanied by intrahepatic biliary radicle dilatation, in the first case.
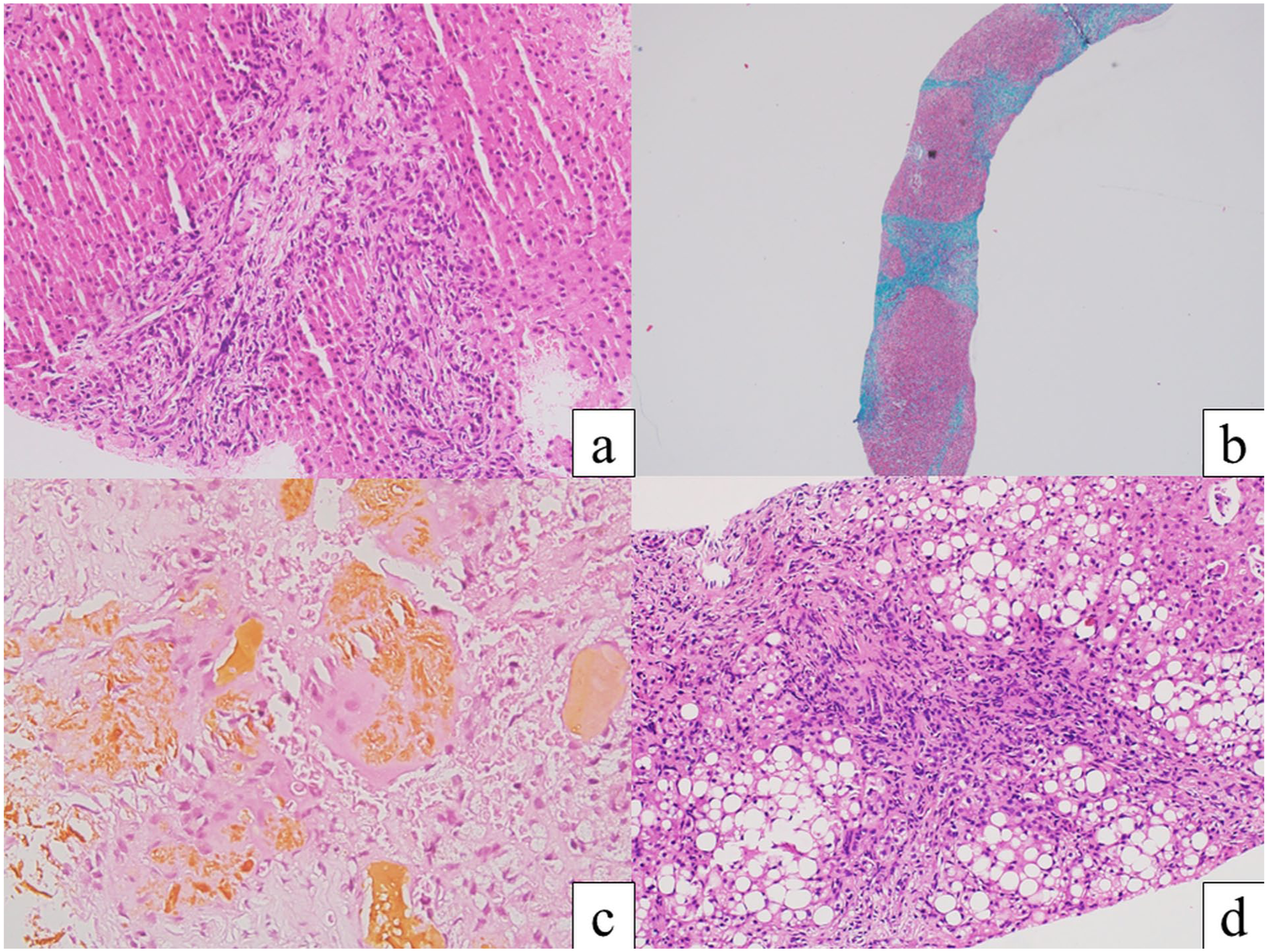
Histopathology of hepatic Langerhans cell histiocytosis without overt infiltration; Portal fibrosis, edema, and ductular reaction suggesting a sclerosing cholangiopathy pattern (Case 4; a, hematoxylin and eosin, 100×); Masson trichrome stain highlighting biliary-type nodule formation due to porto-portal bridging fibrosis (Case 4; b, 20×); Foreign body giant cell reaction and histiocyte collection against extravasated bile (Case 5; c, hematoxylin and eosin, 400×); Sclerosing cholangiopathy pattern with macrovesicular steatosis (Case 6; d, hematoxylin and eosin, 100×).
One case with subtle hepatic infiltration (Case 6) exhibited a sclerosing cholangiopathy pattern similar to that of Case 4. There were occasional singly scattered Langerhans cells in the portal tracts, highlighted by CD1a and Langerin. The hepatic lobules in this case showed diffuse macrovesicular steatosis (Figure 2). Intrahepatic biliary radicle dilatation was identified on radiological evaluation.
Artificial Intelligence (AI)-Assisted Distinction Between Hepatic LCH and Other Non-LCH Mimickers
The major histological differentials of hepatic LCH include diverse pediatric causes of non-LCH cholangiopathies (sclerosing cholangiopathy, PFIC3) and eosinophilic microabscesses. Therefore, we selected 10 archival non-LCH cases to distinguish them from 5 cases of hepatic LCH with overt infiltration (3 pediatric and 2 adult) by using an ensemble of 3 CNN models and to assess its predictive accuracy.
The model demonstrated an area under the curve receiver operating characteristic (AUCROC) of 0.99, with low sensitivity (33.3%) and high specificity (100%). The confusion matrix, AUCROC, and other performance metrics are depicted in Figure 3 and Table 3, respectively.
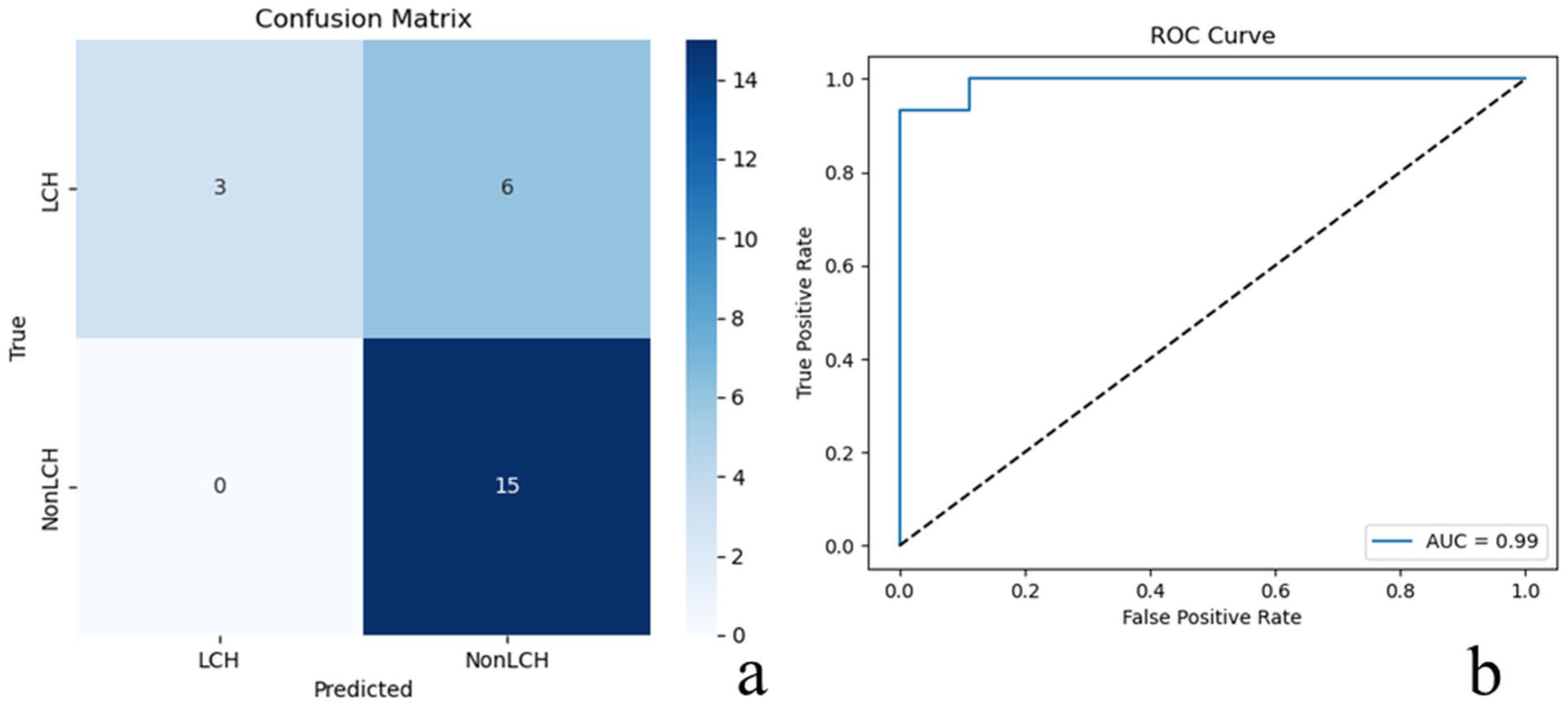
The confusion matrix (a) and AUCROC (b) of the ensemble model.
Performance Metrics of the Ensemble Transfer Learning in Convolutional Neural Network Models.
The falsely predicted LCH images were reviewed. They belong to 3 cases (An adult case, Case 1, and Case 2; 2 images each). The first 3 falsely predicted images (adult case [n = 2] and Case 2 [n = 1]) depicted periductal collections of Langerhans cells admixed with many lymphocytes, nuclear debris, and background ductular reaction, while the other 3 images (Case 1 [n = 2] and Case 2 [n = 1]) highlighted eosinophil-rich abscesses and portal-based granulomata rich in Langerhans cells. These images/patterns did not show any unique/non-classical histology, and similar histological findings were noted in other cases. Thus, the exact reason for the false prediction was difficult to explain (Figure 4).
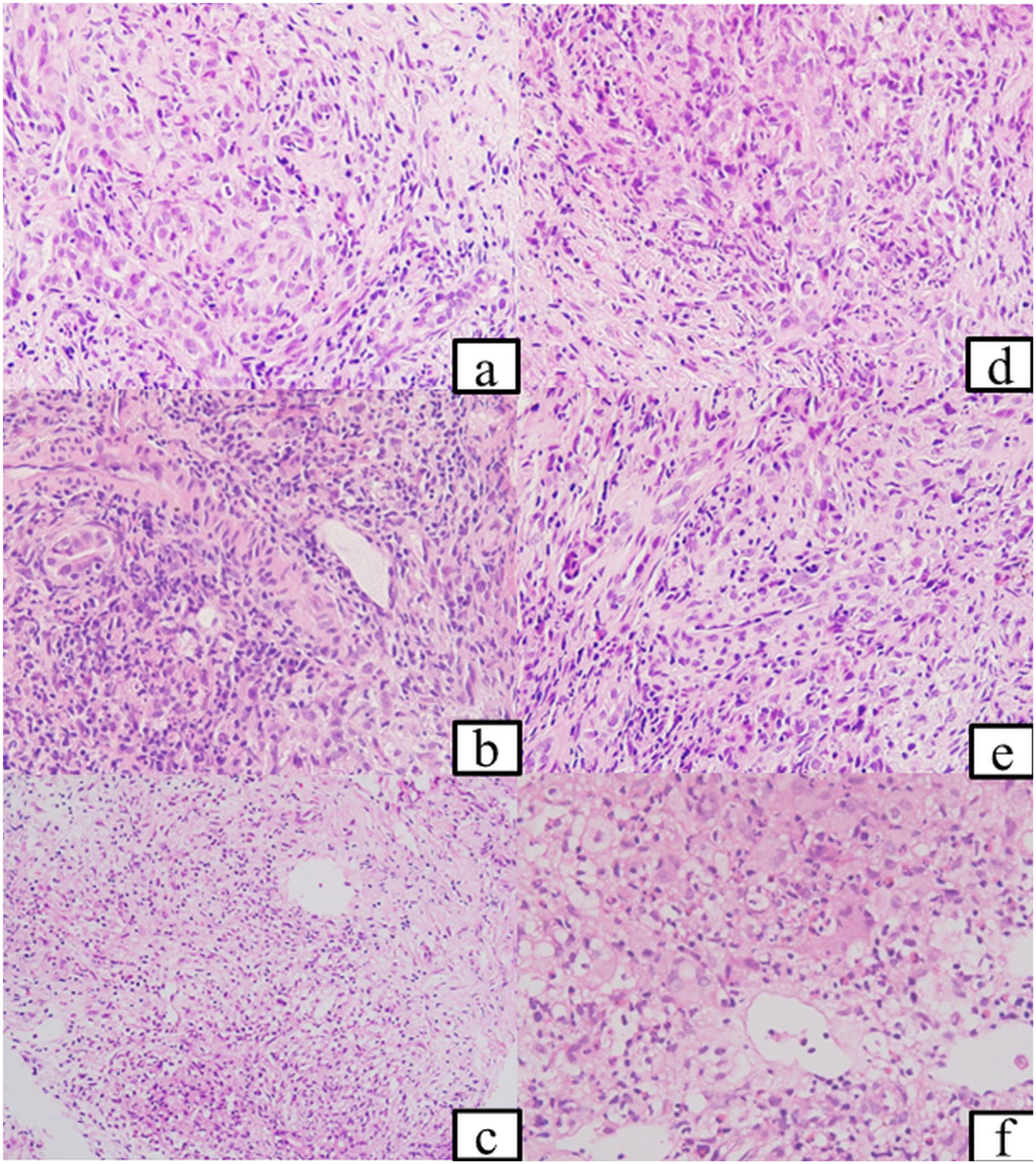
A comparison between the falsely predicted images (left-hand panel [a-c]) and corresponding correctly-predicted/training images (right-hand panel [d-f]) with nearly similar histological findings: The falsely predicted images showing clusters of Langerhans cells admixed with many lymphocytes, nuclear debris, and background ductular reaction (a and b) and eosinophil-rich abscesses and portal-based granulomata rich in Langerhans cells (c; hematoxylin and eosin, 400×). The right-hand panel (d-f) depicts similar histological findings across different sets of images, some of which were used in the training set and others were not, with false predictions (hematoxylin and eosin, 400×).
Discussion
Langerhans cell histiocytosis (LCH) is a clonal neoplasm of myeloid dendritic cells.1,2 The disease affects the pediatric population 5 times more commonly than adults. It can involve a single system (SS-LCH) or multiple (more than one) organ systems (multisystem; MS-LCH), with the most common organs being bone, skin, and pituitary. Involvement of the liver (Hepatic LCH) is usually considered “high-risk” with an unfavorable outcome. Hepatic LCH is typically a component of MS-LCH and affects 15% to 60% of pediatric LCH and 16% to 27% of adult LCH.7-11 The diagnosis of hepatic LCH is often presumed based on clinical, biochemical, and radiological features in cases of biopsy-proven LCH in another organ system, with characteristic histomorphology and immunohistochemical features. Although histopathology and immunohistochemistry are the mainstays of diagnosis, liver biopsies are performed in only a small subset of LCH cases. Rarely, the liver is the first or only organ to be involved and/or biopsied. We aimed to decipher the histological spectrum of hepatic LCH in the pediatric liver biopsies. Besides, we attempted to apply an ensemble transfer learning model to identify the pattern of hepatic LCH infiltration.
The histological diagnosis of hepatic LCH depends on the cholestatic clinical profile with/without visceromegaly, identification of an appropriate clinical context, such as skin rashes, bone lesions, lymphadenopathy, or cystic lung disease, and characteristic histomorphology and immunohistochemistry. The histomorphology depicts (a) infiltration by the atypical histiocytes with grooved nuclei (Langerhans cells) usually showing evidence of duct infiltration and duct damage, (b) a typical inflammatory milieu, and/or (c) a histological pattern. Langerhans cells usually occur as portal-based aggregates, clusters, and single-cell infiltrates. Occasional lobular aggregates are also noted. They usually elicit dense portal-based fibrosis and an inflammatory milieu rich in macrophages, giant cells, and numerous eosinophils with occasional eosinophilic microabscesses. Langerhans cells are typically positive for S100 (nucleocytoplasmic), CD68, CD1a, and langerin (CD207), the latter considered to represent the ultrastructural Birbeck granules. Bilirubinostasis and a variable degree of chronic cholestasis can be observed, similar to the index series. 12
The histological patterns of hepatic LCH can be divided into 3 major categories.7,9,12 The majority of cases exhibit a sclerosing cholangiopathy pattern, with or without the presence of Langerhans cells. 5 of the 6 cases in the index series showed this pattern, and 4 cases showed Langerhans cells in the biopsy. Only 1 case did not show Langerhans cells despite demonstrating sclerosing cholangiopathy on the post-induction liver biopsy. This pattern occurs because Langerhans cells have a propensity to infiltrate and destroy small bile ducts. Three biopsy cases with Langerhans cells showed infiltration, destruction, and partial replacement of interlobular bile ducts by Langerhans cells. The infiltration is often patchy, and the biopsy may merely show sclerosing cholangiopathy, simulating other causes of primary/secondary sclerosing cholangitis, as seen in 2 cases of the index series. In fact, Case 6 merely showed a very occasional single-cell infiltrate and a dominant sclerosing cholangiopathy pattern. These single cells may be overlooked/missed if not suspected and can be challenging to interpret. Thus, a possibility of hepatic LCH should be ruled out in case of sclerosing cholangiopathy in a child below 5 years of age. The sclerosing cholangiopathy may portend to biliary cirrhosis with ductopenia requiring liver transplantation.7-14 The coexistence of sclerosing cholangiopathy pattern with occasional infiltrating Langerhans cells in the liver biopsy also highlights the fact that an intermediate stage exists between the traditionally described early-infiltrative and late-sclerosing patterns. 15 The second pattern of infiltration is cystic dilatation and bile extravasation due to destructive cholangitis of the large bile ducts. This pattern, comparatively rarer, was seen in a single case in this series. Langerhans cells tend to infiltrate the ducts, and the predominant ductal involvement determines the pattern. Thus, a sclerosing cholangiopathy pattern resulting from small-duct involvement is the most common, followed by large-duct involvement. Uncommonly, a liver biopsy can show a combinatorial feature of sclerosing cholangiopathy with large duct damage. 4 Another uncommon pattern in the liver biopsy is the mass-like lesions/granulomatoid foci. 12 None of the cases in the index series showed this pattern, although portal-based granulomata were noted. According to the corresponding author’s experience, this pattern is more commonly detected in autopsies or explants. An uncommon primary biliary cholangitis (PBC)-like pattern of hepatic LCH with granulomatous cholangitis has also been described. 7 The presence of steatosis in the liver biopsy in a single case (case 6) is difficult to explain and could be multifactorial in origin (malnutrition, drugs, etc.). However, hepatic steatosis in hepatic LCH liver biopsies is not uncommon, as reported by Abdallah et al. (n = 5/13; 38.5%). 16
Most cases of LCH are caused by mutations in genes encoding mitogen-activated protein kinase (MAPK) pathway proteins. The BRAF p.V600E mutation is the most common (19%-28%), typically associated with MS-LCH, and is associated with a poor prognosis, characterized by poor 3-year overall and event-free survival rates.17-20 The mutation can be detected by molecular methods (real-time polymerase chain reaction, Sanger sequencing, and next-generation sequencing). Mutation-specific immunohistochemistry (using the anti-BRAF VE1 antibody clone) is available and provides reliable results upon validation. Immunohistochemistry was positive in both cases, with adequate tissue available for testing.
The histomorphology of hepatic LCH, with infiltration of Langerhans cells, can have multiple differential diagnoses. The differential comprises primary and secondary sclerosing cholangitis, PFIC3, and various causes of eosinophilic abscesses. Thus, we aimed to evaluate the predictive ability of transfer learning models to distinguish hepatic LCH with Langerhans cell infiltration from other patterns simulating LCH. As we had only 3 cases of pediatric hepatic LCH with overt hepatic Langerhans cell infiltration, we included 2 more (adult) cases to assess predictive ability. We excluded cases with a sclerosing cholangiopathy pattern and no/subtle infiltration by Langerhans cells to maintain the high quality and accuracy of the training data. A transfer learning model utilizes pre-trained models, and an ensemble transfer learning model merges multiple transfer learning models. An ensemble transfer learning model provides more stable predictions and reduces the bias of individual models by combining their predictions. The final prediction in the ensemble model is usually decided by voting, stacking, or averaging. Thus, we applied an ensemble of 3 commonly used transfer-learning CNN models with soft voting to obtain the final output. This study is the first to implement this strategy for distinguishing hepatic LCH from its histological differentials. A similar model had previously been successfully employed in cytology.21,22
Our results indicate high specificity and precision of the model, although sensitivity was suboptimal. In simple terms, the model accurately predicted all non-LCH images, but incorrectly classified 6 LCH images as non-LCH. The wrongly categorized images showed portal-based collections of Langerhans cells, granulomatous reactions/histiocytic aggregates, and eosinophilic abscesses, histological features that are not unique to the training, validation, or testing datasets. Thus, the exact reason for such a false prediction was difficult to elucidate. Such false predictions may be obviated in the future by using a larger sample size for such a rare disease, training and validation with variant histology, and removing class imbalance. 3 These are the typical constraints in the AI-based pediatric hepatopathology research. The application of whole-slide imaging (WSI) could have been a better alternative. The absence of the WSI application from the index study, due to its temporary unavailability at our institute, is a limitation of this study. The massive size, requiring significant storage, computational power, and complex patching strategies, was a significant constraint for WSI. Additionally, we applied the model only to images/cases with histological evidence of hepatic Langerhans cell infiltration. The CNN architectures can often detect supra-visual/sub-visual characteristics of an image without any annotation. Short of WSI, the purpose of training images containing microphotographs captured under both 20× and 40× objectives was to elucidate both architectural (20×) and cytological features (40×). Thus, the ensemble's false predictions possibly underscore the importance of future annotation of Langerhans cells on a larger dataset.
The occurrence of the sclerosing cholangiopathy pattern in the liver biopsy, without/with minimal infiltration of Langerhans cells, cannot be distinguished from primary and secondary sclerosing cholangitis based on histomorphology alone. Therefore, we did not apply the model to cases of sclerosing cholangiopathy without/with minimal histological evidence of Langerhans cells. Despite these limitations, AI was able to distinguish the cytoarchitectural changes of hepatic LCH, including the cholangiopathic features, to a fair extent. Thus, this model in its present form should be best positioned as a screening, triage, or decision-support tool. Future improvements require larger multicenter datasets, external validation in a larger cohort, threshold optimization to achieve higher sensitivity, and more versatile integration with radiological and clinical information.
Conclusion
We described various patterns of hepatic LCH and successfully applied an ensemble transfer learning model to distinguish hepatic Langerhans cell infiltration patterns from their histological differentials. Despite its limitations, the predictive model’s results were encouraging and require a larger dataset and external validation.
Footnotes
Author Contributions
DiB, SM, RL, and NK were involved in histological analysis and interpretation. RL and AB provided academic inputs. RL and NK critically reviewed the manuscript. AB, CT, DeB, and SL were involved in the clinical management, data collection, and critical review of the manuscript. PD prepared the code for the AI model, interpreted the AI data, and critically reviewed the manuscript. DiB collected the data, prepared the first draft of the manuscript, and ran the AI model. SM conceptualized and finalized the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.